
Remotely Programmable Deep Brain Stimulator Combined with an Invasive Blood Pressure Monitoring System for a Non-Tethered Rat Model in Hypertension Research
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
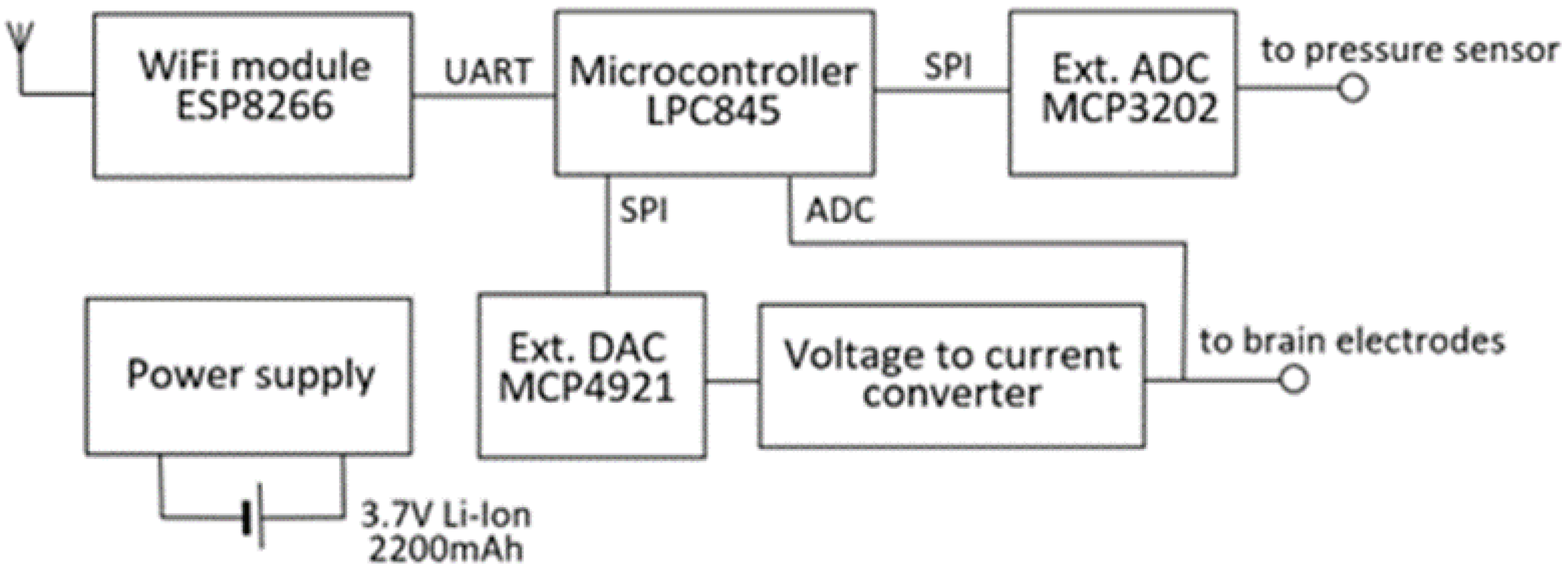
2.1. Design of the Device
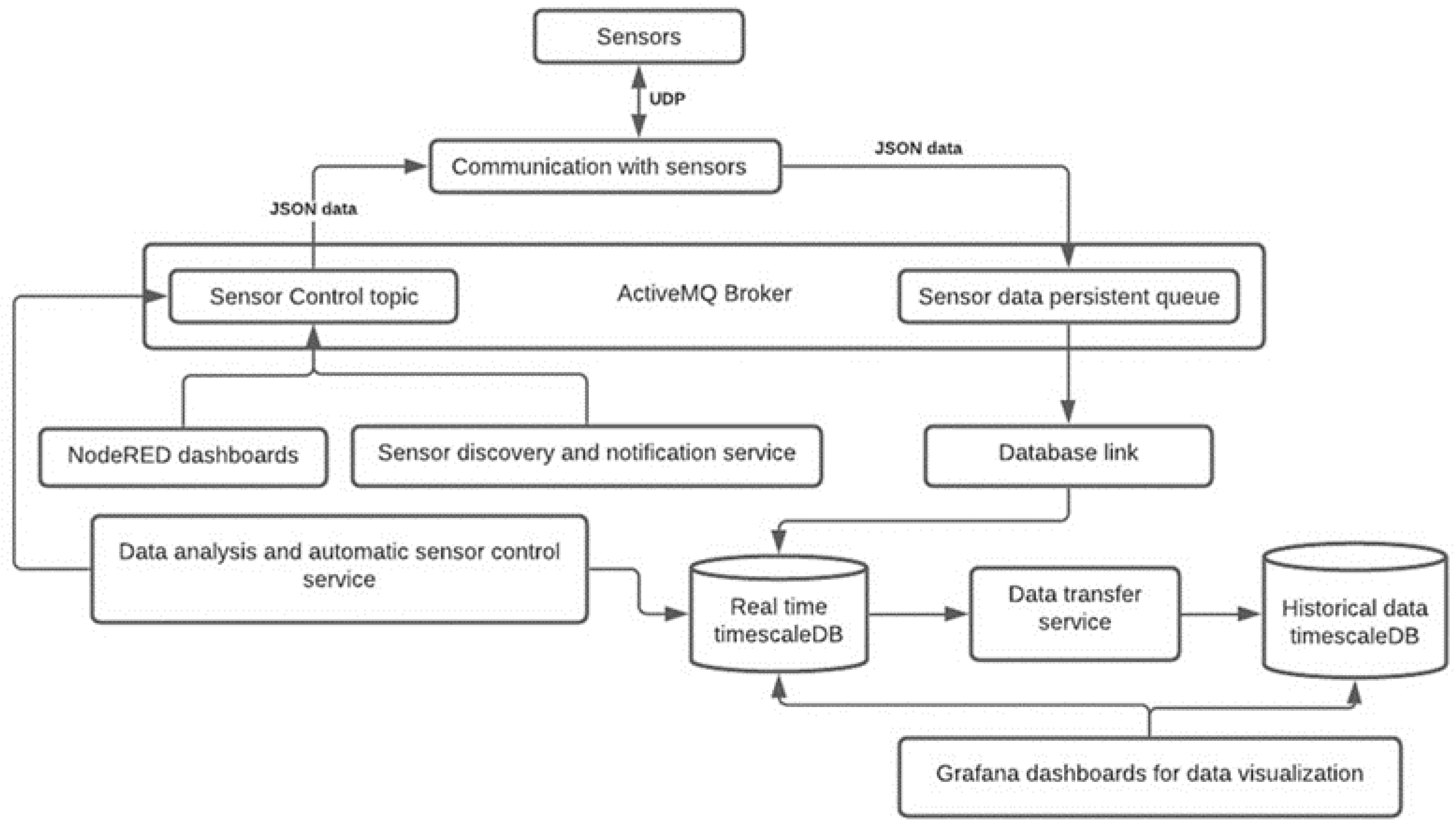
2.2. Data Recording and Analysis
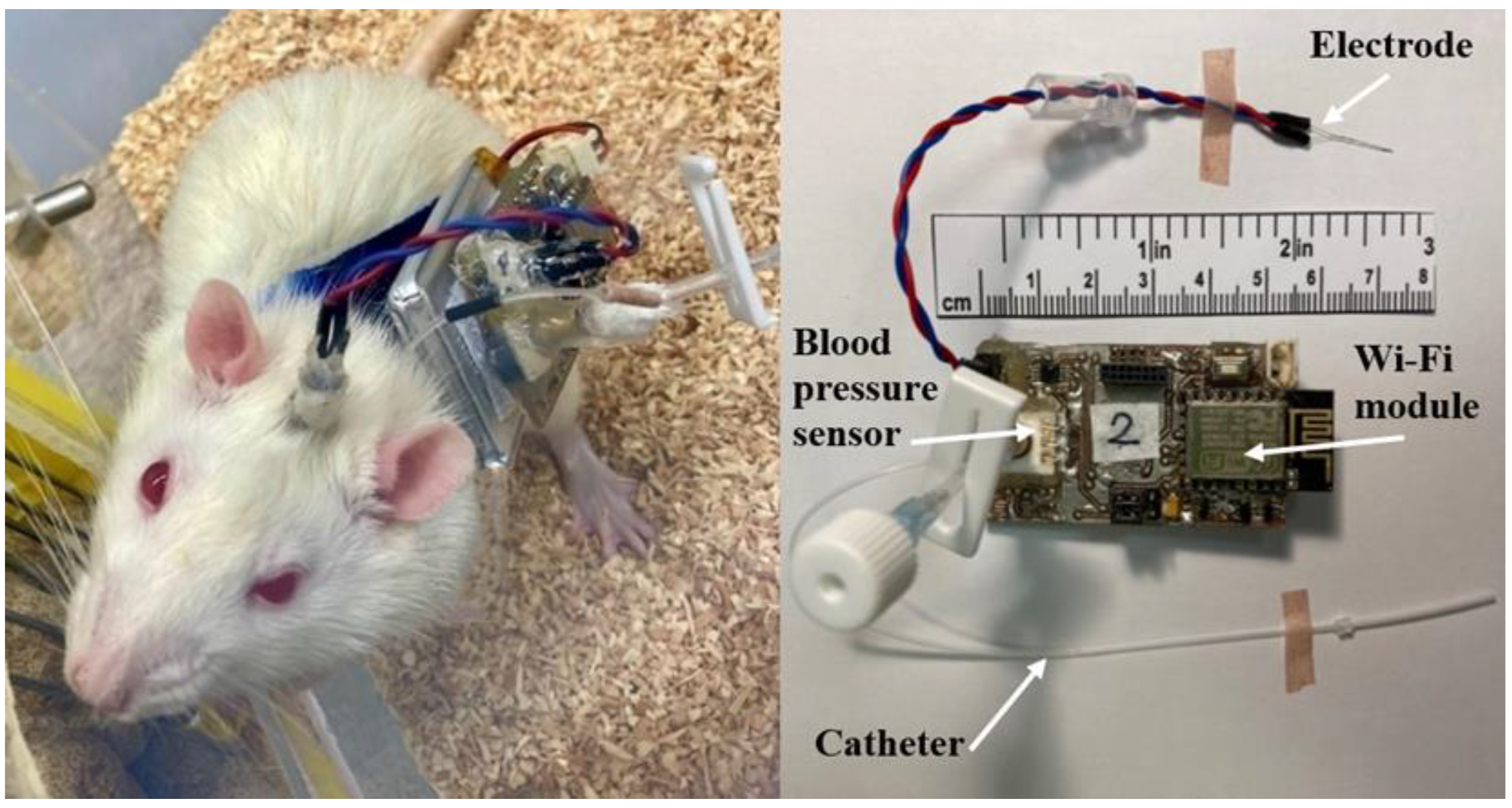
2.3. Device Peripherals
2.4. Procedure
2.5. Postoperative Period
2.6. Data Analysis
3. Results
3.1. Survivability and Neurological Compromise
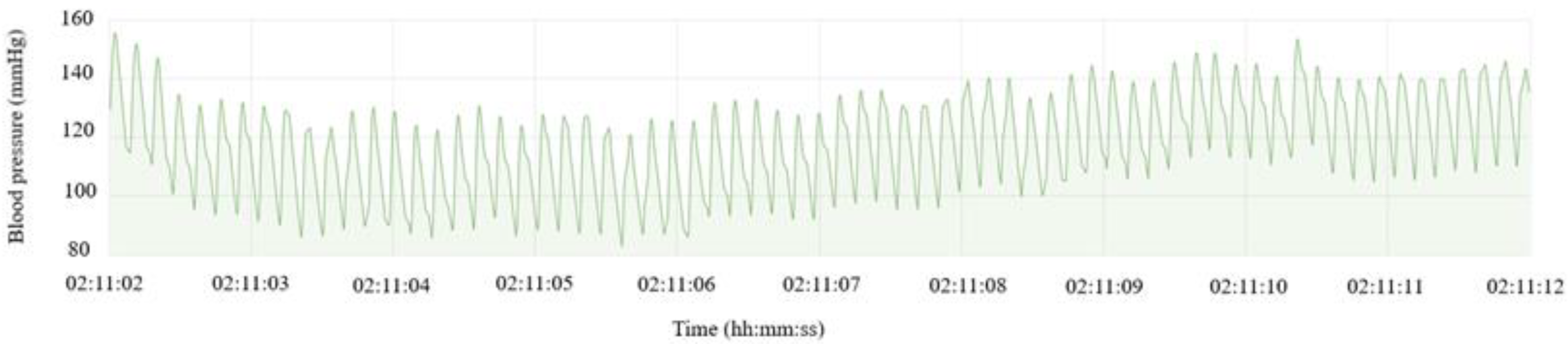
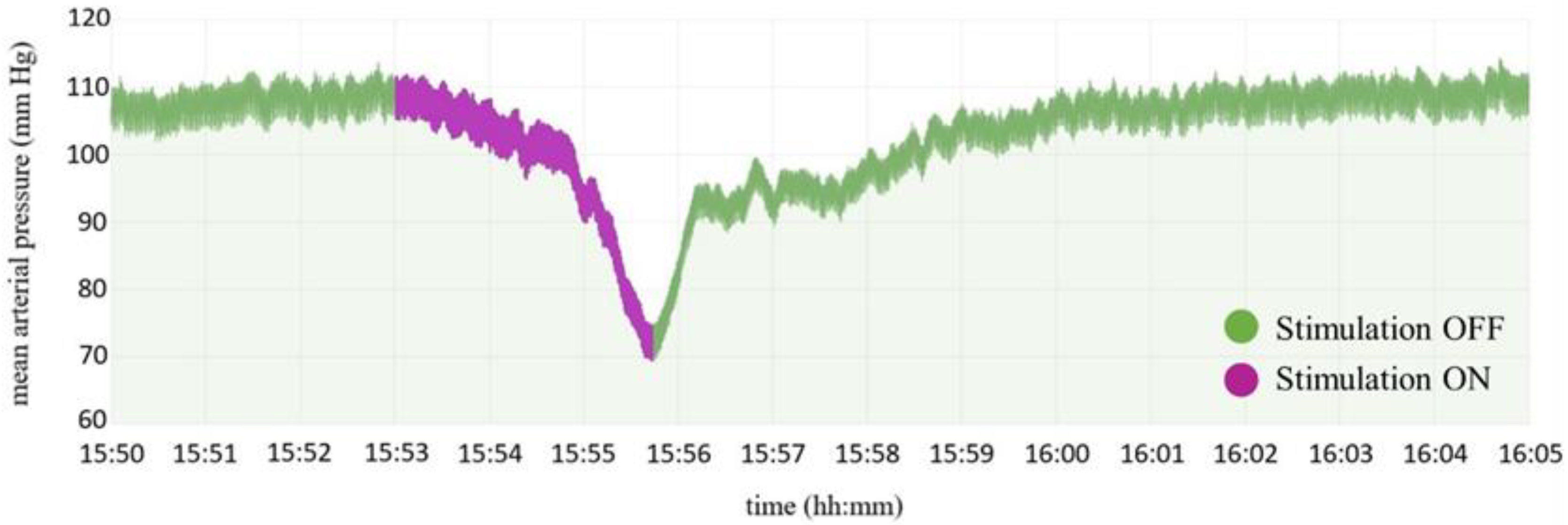
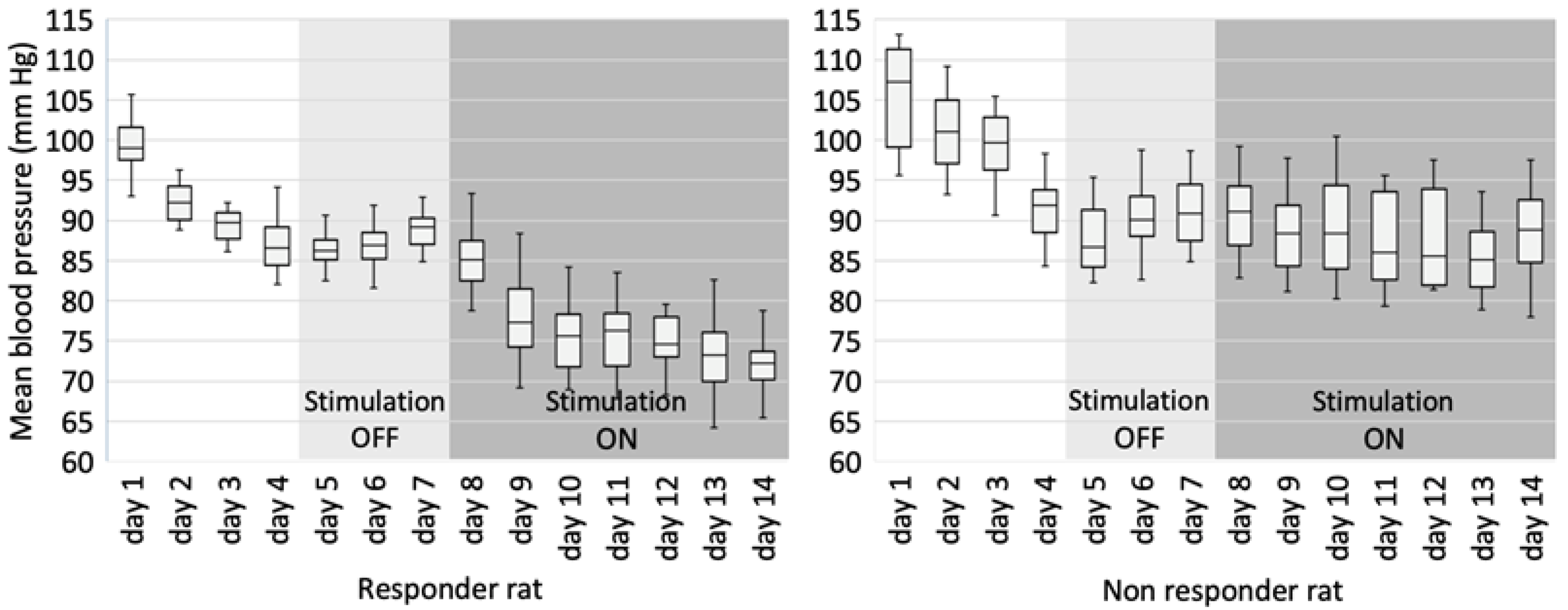
3.2. Blood Pressure Recording
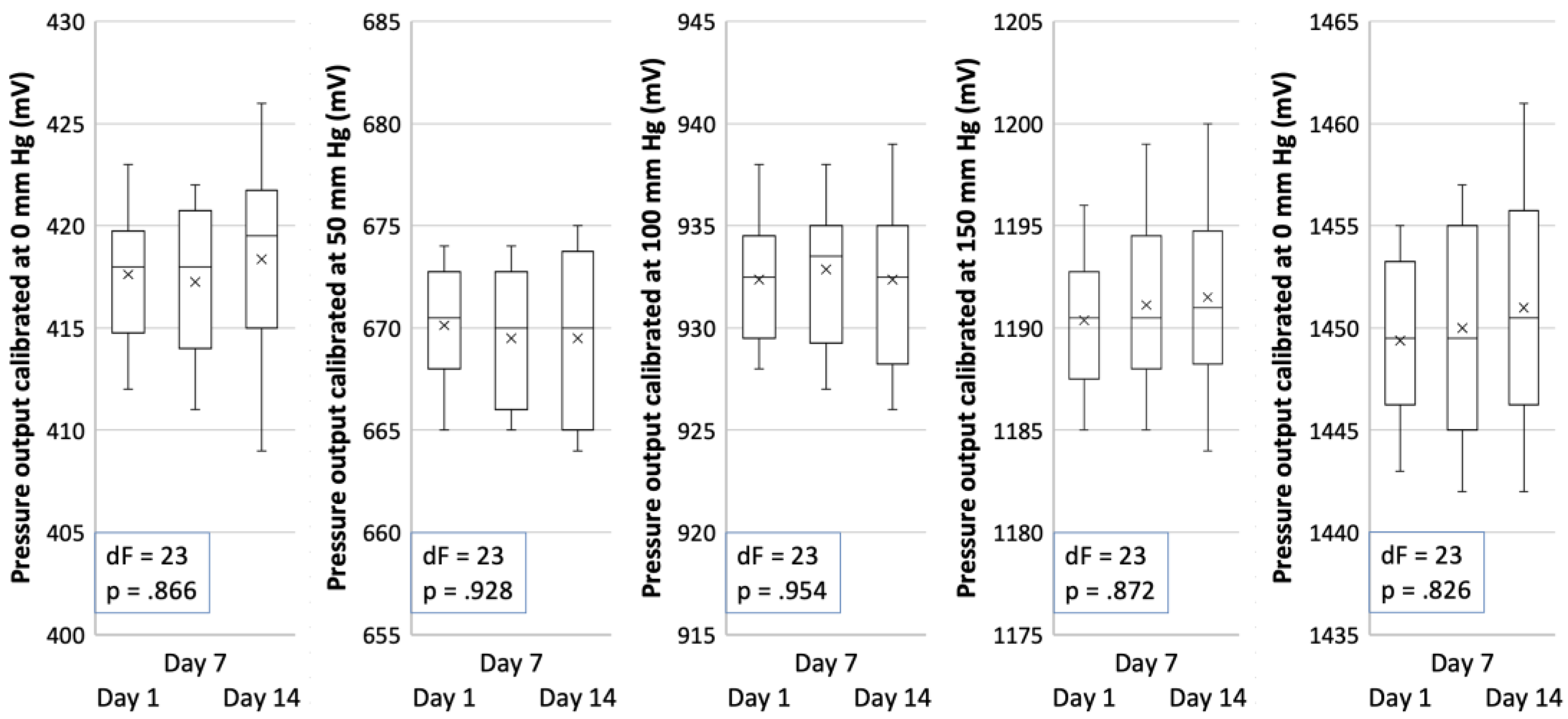
3.3. Zero and Sensitivity Drift
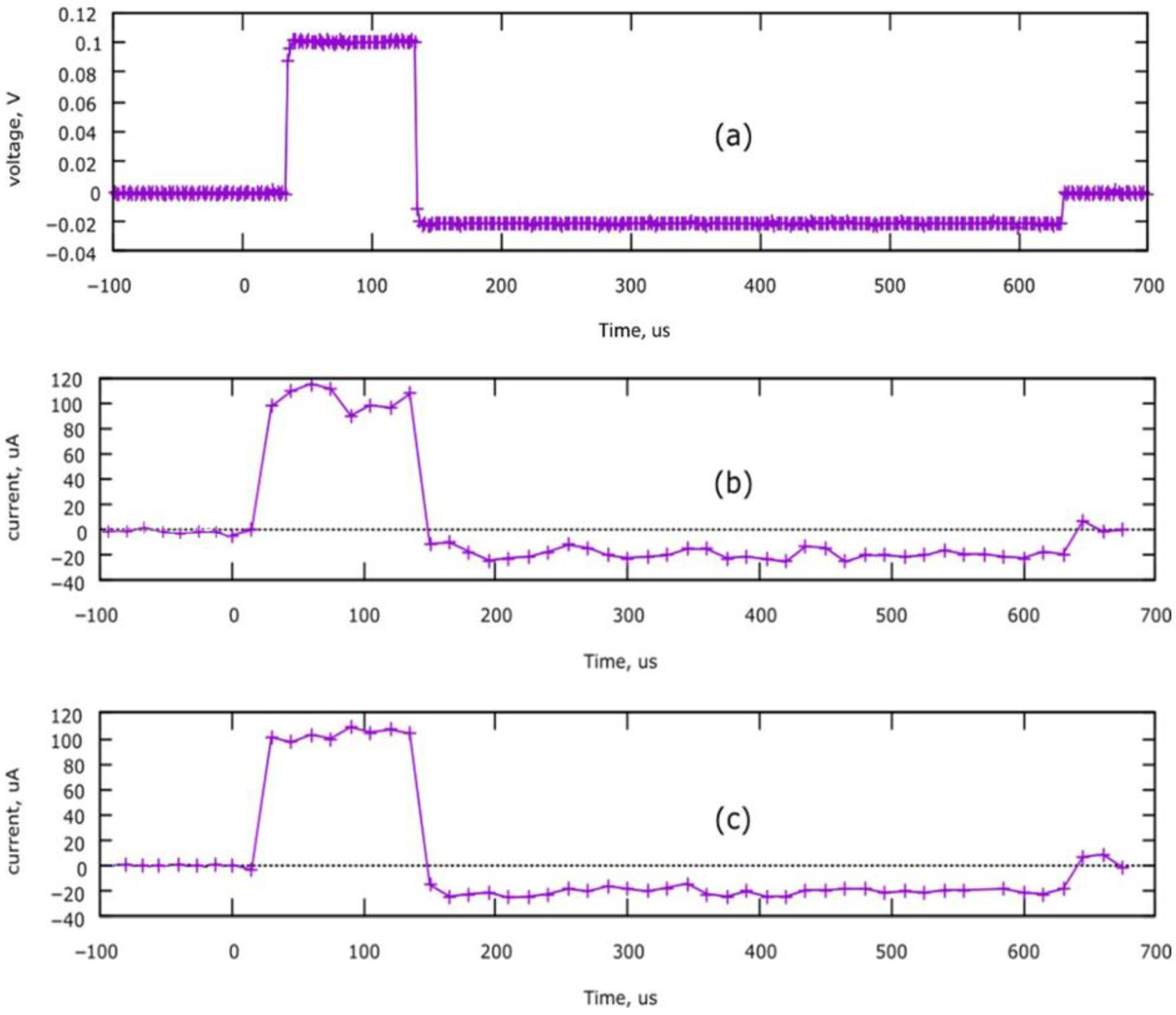
3.4. Device Performance
3.5. Catheter Patency Rates
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, J.; Chen, Z. Neuromodulation for Pain Management. Adv. Exp. Med. Biol. 2019, 1101, 207–223. [Google Scholar] [CrossRef] [PubMed]
- Deer, T.R.; Pope, J.E.; Hanes, M.C.; McDowell, G.C. Intrathecal Therapy for Chronic Pain: A Review of Morphine and Ziconotide as Firstline Options. Pain Med. 2019, 20, 784–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burke, M.J.; Fried, P.J.; Pascual-Leone, A. Transcranial magnetic stimulation: Neurophysiological and clinical applications. Handb. Clin. Neurol. 2019, 163, 73–92. [Google Scholar] [CrossRef] [PubMed]
- Borgomaneri, S.; Battaglia, S.; Garofalo, S.; Tortora, F.; Avenanti, A.; di Pellegrino, G. State-Dependent TMS over Prefrontal Cortex Disrupts Fear-Memory Reconsolidation and Prevents the Return of Fear. Curr. Biol. 2020, 30, 3672–3679. [Google Scholar] [CrossRef] [PubMed]
- Kalanithi, P.S.; Henderson, J.M. Optogenetic neuromodulation. Int. Rev. Neurobiol. 2012, 107, 185–205. [Google Scholar] [CrossRef]
- Krauss, J.K.; Lipsman, N.; Aziz, T.; Boutet, A.; Brown, P.; Chang, J.W.; Davidson, B.; Grill, W.M.; Hariz, M.I.; Horn, A.; et al. Technology of deep brain stimulation: Current status and future directions. Nat. Rev. Neurol. 2021, 17, 75–87. [Google Scholar] [CrossRef]
- Rock, A.K.; Truong, H.; Park, Y.L.; Pilitsis, J.G. Spinal Cord Stimulation. Neurosurg. Clin. N. Am. 2019, 30, 169–194. [Google Scholar] [CrossRef] [PubMed]
- González, H.F.J.; Yengo-Kahn, A.; Englot, D.J. Vagus Nerve Stimulation for the Treatment of Epilepsy. Neurosurg. Clin. N. Am. 2019, 30, 219–230. [Google Scholar] [CrossRef] [PubMed]
- Erosa, S.C.; Moheimani, R.S.; Oswald, J.C.; Castellanos, J.P.; Abraham, M.E.; Schuster, N.M. Peripheral Nerve Stimulation for Chronic Pain and Migraine: A Review. Phys. Med. Rehabil. Clin. N. Am. 2022, 33, 379–407. [Google Scholar] [CrossRef]
- Tronnier, V.; Rasche, D. Epidural and subdural stimulation. Handb. Clin. Neurol. 2013, 116, 343–351. [Google Scholar] [CrossRef]
- Limousin, P.; Pollak, P.; Benazzouz, A.; Hoffmann, D.; Le Bas, J.F.; Broussolle, E.; Perret, J.E.; Benabid, A.L. Effect of parkinsonian signs and symptoms of bilateral subthalamic nucleus stimulation. Lancet 1995, 345, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Steigerwald, F.; Matthies, C.; Volkmann, J. Directional Deep Brain Stimulation. Neurotherapeutics 2019, 16, 100–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiken, S.; Nambu, A. Mechanism of Deep Brain Stimulation: Inhibition, Excitation, or Disruption? Neuroscientist 2016, 22, 313–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mallet, L.; Polosan, M.; Jaafari, N.; Baup, N.; Welter, M.L.; Fontaine, D.; du Montcel, S.T.; Yelnik, J.; Chéreau, I.; Arbus, C.; et al. Subthalamic nucleus stimulation in severe obsessive-compulsive disorder. N. Engl. J. Med. 2008, 359, 2121–2134. [Google Scholar] [CrossRef] [Green Version]
- Halpern, C.H.; Wolf, J.A.; Bale, T.L.; Stunkard, A.J.; Danish, S.F.; Grossman, M.; Jaggi, J.L.; Grady, M.S.; Baltuch, G.H. Deep brain stimulation in the treatment of obesity. J. Neurosurg. 2008, 109, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Malone, D.A.; Dougherty, D.D.; Rezai, A.R.; Carpenter, L.L.; Friehs, G.M.; Eskandar, E.N.; Rauch, S.L.; Rasmussen, S.A.; Machado, A.G.; Kubu, C.S.; et al. Deep brain stimulation of the ventral capsule/ventral striatum for treatment-resistant depression. Biol. Psychiatry 2009, 65, 267–275. [Google Scholar] [CrossRef] [Green Version]
- Breit, S.; Lessmann, L.; Benazzouz, A.; Schulz, J.B. Unilateral lesion of the pedunculopontine nucleus induces hyperactivity in the subthalamic nucleus and substantia nigra in the rat. Eur. J. Neurosci. 2005, 22, 2283–2294. [Google Scholar] [CrossRef]
- Sani, S.; Jobe, K.; Smith, A.; Kordower, J.H.; Bakay, R.A. Deep brain stimulation for treatment of obesity in rats. J. Neurosurg. 2007, 107, 809–813. [Google Scholar] [CrossRef]
- Oterdoom, D.L.M.; Lok, R.; van Beek, A.P.; den Dunnen, W.F.A.; Emous, M.; van Dijk, J.M.C.; van Dijk, G. Deep Brain Stimulation in the Nucleus Accumbens for Binge Eating Disorder: A Study in Rats. Obes. Surg. 2020, 30, 4145–4148. [Google Scholar] [CrossRef]
- O’Callaghan, E.L.; Hart, E.C.; Sims-Williams, H.; Javed, S.; Burchell, A.E.; Papouchado, M.; Tank, J.; Heusser, K.; Jordan, J.; Menne, J.; et al. Chronic Deep Brain Stimulation Decreases Blood Pressure and Sympathetic Nerve Activity in a Drug- and Device-Resistant Hypertensive Patient. Hypertension 2017, 69, 522–528. [Google Scholar] [CrossRef]
- Ems, R.; Garg, A.; Ostergard, T.A.; Miller, J.P. Potential Deep Brain Stimulation Targets for the Management of Refractory Hypertension. Front. Neurosci. 2019, 13, 93. [Google Scholar] [CrossRef] [PubMed]
- Formolo, D.A.; Gaspar, J.M.; Melo, H.M.; Eichwald, T.; Zepeda, R.J.; Latini, A.; Okun, M.S.; Walz, R. Deep Brain Stimulation for Obesity: A Review and Future Directions. Front. Neurosci. 2019, 13, 323. [Google Scholar] [CrossRef] [PubMed]
- Hsu, T.I.; Nguyen, A.; Gupta, N.; Godbole, N.; Perisetla, N.; Hatter, M.J.; Beyer, R.S.; Bui, N.E.; Jagan, J.; Yang, C.; et al. Effectiveness of Deep Brain Stimulation in Treatment of Anorexia Nervosa and Obesity: A Systematic Review. World Neurosurg. 2022, 168, 179–189. [Google Scholar] [CrossRef]
- World Health Organization. Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks, 1st ed.; World Health Organization: Geneva, Switzerland, 2009; p. V. [Google Scholar]
- Zhou, B.; Bentham, J.; Di Cesare, M.; Bixby, H.; Danaei, G.; Cowan, M.J.; Paciorek, C.J.; Singh, G.; Hajifathalian, K.; Bennett, J.E.; et al. Worldwide trends in blood pressure from 1975 to 2015: A pooled analysis of 1479 population-based measurement studies with 19.1 million participants. Lancet 2017, 389, 37–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; Amann, M.; Anderson, H.R.; Andrews, K.G.; Aryee, M.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef] [Green Version]
- Yoruk, A.; Bisognano, J.D.; Gassler, J.P. Baroreceptor Stimulation for Resistant Hypertension. Am. J. Hypertens. 2016, 29, 1319–1324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denker, M.G.; Cohen, D.L. Resistant Hypertension and Renal Nerve Denervation. Methodist Debakey Cardiovasc. J. 2015, 11, 240–244. [Google Scholar] [CrossRef] [Green Version]
- Mann, S.J. Neurogenic hypertension: Pathophysiology, diagnosis and management. Clin. Auton. Res. 2018, 28, 363–374. [Google Scholar] [CrossRef]
- King, A.J.; Novotny, M.; Swain, G.M.; Fink, G.D. Whole body norepinephrine kinetics in ANG II-salt hypertension in the rat. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2008, 294, 1262–1267. [Google Scholar] [CrossRef] [Green Version]
- Osborn, J.W.; Fink, G.D. Region-specific changes in sympathetic nerve activity in angiotensin II-salt hypertension in the rat. Exp. Physiol. 2010, 95, 61–68. [Google Scholar] [CrossRef] [Green Version]
- Armitage, J.A.; Burke, S.L.; Prior, L.J.; Barzel, B.; Eikelis, N.; Lim, K.; Head, G.A. Rapid onset of renal sympathetic nerve activation in rabbits fed a high-fat diet. Hypertension 2012, 60, 163–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grassi, G. Sympathomodulatory Effects of Antihypertensive Drug Treatment. Am. J. Hypertens. 2016, 29, 665–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DiBona, G.F.; Esler, M. Translational medicine: The antihypertensive effect of renal denervation. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2010, 298, 245–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahfoud, F.; Schlaich, M.P.; Lobo, M.D. Device Therapy of Hypertension. Circ. Res. 2021, 128, 1080–1099. [Google Scholar] [CrossRef] [PubMed]
- Blessing, W.W.; Reis, D.J. Inhibitory cardiovascular function of neurons in the caudal ventrolateral medulla of the rabbit: Relationship to the area containing A1 noradrenergic cells. Brain Res. 1982, 253, 161–171. [Google Scholar] [CrossRef]
- Guyenet, P.G.; Stornetta, R.L.; Souza, G.M.P.R.; Abbott, S.B.G.; Brooks, V.L. Neuronal Networks in Hypertension: Recent Advances. Hypertension 2020, 76, 300–311. [Google Scholar] [CrossRef]
- Mayorov, D.N.; Head, G.A. Influence of rostral ventrolateral medulla on renal sympathetic baroreflex in conscious rabbits. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2001, 280, 577–587. [Google Scholar] [CrossRef]
- Kawase, T. Light up the “no-man’s land” on the brain stem. Keio J. Med. 1995, 44, 133–139. [Google Scholar] [CrossRef] [Green Version]
- Bourns.com. Available online: https://www.bourns.com/docs/product-datasheets/bps130.pdf (accessed on 29 December 2021).
- Paxinos, G.; Watson, C. The Rat Brain in Stereotaxic Coordinates, 6th ed.; Elsevier: Amsterdam, The Netherlands, 2009. [Google Scholar]
- Goodchild, A.K.; Moon, E.A. Maps of cardiovascular and respiratory regions of rat ventral medulla: Focus on the caudal medulla. J. Chem. Neuroanat. 2009, 38, 209–221. [Google Scholar] [CrossRef]
- Sved, A.F.; Blessing, W.W.; Reis, D.J. Caudal ventrolateral medulla can alter vasopressin and arterial pressure. Brain Res. Bull. 1985, 14, 227–232. [Google Scholar] [CrossRef]
- Bradley, D.J.; Pascoe, J.P.; Paton, J.F.; Spyer, K.M. Cardiovascular and respiratory responses evoked from the posterior cerebellar cortex and fastigial nucleus in the cat. J. Physiol. 1987, 393, 107–121. [Google Scholar] [CrossRef] [Green Version]
- O’Callaghan, E.L.; McBryde, F.D.; Patel, N.K.; Paton, J.F.R. Examination of the periaqueductal gray as a site for controlling arterial pressure in the conscious spontaneously hypertensive rat. Auton. Neurosci. 2022, 240, 102984. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Panneton, W.M. The caudal pressor area of the rat: Its precise location and projections to the ventrolateral medulla. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2002, 283, 768–778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciriello, J. Caudal ventrolateral medulla mediates baroreceptor afferent inputs to subfornical organ angiotensin II responsive neurons. Brain Res. 2013, 1491, 127–135. [Google Scholar] [CrossRef]
- Cooper, C.M.; Farrand, A.Q.; Andresen, M.C.; Beaumont, E. Vagus nerve stimulation activates nucleus of solitary tract neurons via supramedullary pathways. J. Physiol. 2021, 599, 5261–5279. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.Y.; Kuo, T.B.; Hsieh, I.T.; Yang, C.C. Electrical stimulation of the rostral ventrolateral medulla promotes wakefulness in rats. Sleep Med. 2013, 14, 1076–1084. [Google Scholar] [CrossRef] [PubMed]
- Lertwittayanon, W.; Devinsky, O.; Carlen, P.L. Cardiorespiratory depression from brainstem seizure activity in freely moving rats. Neurobiol. Dis. 2020, 134, 104628. [Google Scholar] [CrossRef]
- Robinson, T.E. Electrical Stimulation of the Brain Stem in Freely Moving Rats: I. Effects on Behavior, Physiology & Behavior; Elsevier: London, ON, Canada, 1978; pp. 223–231. [Google Scholar]
- Feinstein, B.; Gleason, C.A.; Libet, B. Stimulation of locus coeruleus in man. Preliminary trials for spasticity and epilepsy. Stereotact. Funct. Neurosurg. 1989, 52, 26–41. [Google Scholar] [CrossRef]
- Young, R.F.; Tronnier, V.; Rinaldi, P.C. Chronic stimulation of the Kölliker-Fuse nucleus region for relief of intractable pain in humans. J. Neurosurg. 1992, 76, 979–985. [Google Scholar] [CrossRef] [Green Version]
- Elias, G.J.B.; Loh, A.; Gwun, D.; Pancholi, A.; Boutet, A.; Neudorfer, C.; Germann, J.; Namasivayam, A.; Gramer, R.; Paff, M.; et al. Deep brain stimulation of the brainstem. Brain 2021, 144, 712–723. [Google Scholar] [CrossRef]
- Green, A.L.; Hyam, J.A.; Williams, C.; Wang, S.; Shlugman, D.; Stein, J.F.; Paterson, D.J.; Aziz, T.Z. Intra-operative deep brain stimulation of the periaqueductal grey matter modulates blood pressure and heart rate variability in humans. Neuromodulation 2010, 13, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Green, A.L.; Wang, S.; Owen, S.L.; Xie, K.; Liu, X.; Paterson, D.J.; Stein, J.F.; Bain, P.G.; Aziz, T.Z. Deep brain stimulation can regulate arterial blood pressure in awake humans. Neuroreport 2005, 16, 1741–1745. [Google Scholar] [CrossRef]
- Green, A.L.; Wang, S.; Bittar, R.G.; Owen, S.L.; Paterson, D.J.; Stein, J.F.; Bain, P.G.; Shlugman, D.; Aziz, T.Z. Deep brain stimulation: A new treatment for hypertension? J. Clin. Neurosci. 2007, 14, 592–595. [Google Scholar] [CrossRef] [PubMed]
- DeLalio, L.J.; Sved, A.F.; Stocker, S.D. Sympathetic Nervous System Contributions to Hypertension: Updates and Therapeutic Relevance. Can. J. Cardiol. 2020, 36, 712–720. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, T.; Griffin, K.; Bidani, A.; Davisson, R.; Hall, J. Recommendations for Blood Pressure Measurement in Humans and Experimental Animals. Hypertension 2005, 45, 299–310. [Google Scholar] [CrossRef] [Green Version]
- Ewing, S.G.; Lipski, W.J.; Grace, A.A.; Winter, C. An inexpensive, charge-balanced rodent deep brain stimulation device: A step-by-step guide to its procurement and construction. J. Neurosci. Methods 2013, 219, 324–330. [Google Scholar] [CrossRef] [Green Version]
- Fluri, F.; Mützel, T.; Schuhmann, M.K.; Krstić, M.; Endres, H.; Volkmann, J. Development of a head-mounted wireless microstimulator for deep brain stimulation in rats. J. Neurosci. Methods 2017, 291, 249–256. [Google Scholar] [CrossRef]
- Forni, C.; Mainard, O.; Melon, C.; Goguenheim, D.; Kerkerian-Le Goff, L.; Salin, P. Portable microstimulator for chronic deep brain stimulation in freely moving rats. J. Neurosci. Methods 2012, 209, 50–57. [Google Scholar] [CrossRef]
- Luo, Y.S.; Luo, Y.L.; Ashford, E.B.; Morin, R.R.; White, W.J.; Fisher, T.F. Comparison of catheter lock solutions in rats. In Proceedings of the 51st Annual Meeting of the American Association for Laboratory Animal Science, San Diego, CA, USA, 6 November 2000. [Google Scholar]
- Wang, Y.; Cong, Y.; Li, J.; Li, X.; Li, B.; Qi, S. Comparison of invasive blood pressure measurements from the caudal ventral artery and the femoral artery in male adult SD and Wistar rats. PLoS ONE 2013, 8, e60625. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pulse amplitude | 0–140 µA, steps of 1 µA |
| Pulse duration | 40–300 µs, steps of 1 µs |
| Pulse repetition period (frequency) | 2–500 ms (2–500 Hz), steps of 1 ms |
| Weight (with jacket, case and battery) | 55 g |
| Dimensions (with case) | 5.5 × 3 × 2 cm |
| Operation time with one battery | 20 h with continuous stimulation parameters: 100 μA, 50 Hz, 0.1 ms, and continuous data measurement and transmission |
| Programmable periodical sleep cycles for energy saving. In sleep mode, the WiFi module is not operational and blood pressure is not measured, while brain stimulation is always on. | |
| The pressure measurement period is software configurable and can be as little as 4 ms. | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chomanskis, Ž.; Jonkus, V.; Danielius, T.; Paulauskas, T.; Orvydaitė, M.; Melaika, K.; Rukšėnas, O.; Hendrixson, V.; Ročka, S. Remotely Programmable Deep Brain Stimulator Combined with an Invasive Blood Pressure Monitoring System for a Non-Tethered Rat Model in Hypertension Research. Brain Sci. 2023, 13, 504. https://doi.org/10.3390/brainsci13030504
Chomanskis Ž, Jonkus V, Danielius T, Paulauskas T, Orvydaitė M, Melaika K, Rukšėnas O, Hendrixson V, Ročka S. Remotely Programmable Deep Brain Stimulator Combined with an Invasive Blood Pressure Monitoring System for a Non-Tethered Rat Model in Hypertension Research. Brain Sciences. 2023; 13(3):504. https://doi.org/10.3390/brainsci13030504
Chicago/Turabian StyleChomanskis, Žilvinas, Vytautas Jonkus, Tadas Danielius, Tomas Paulauskas, Monika Orvydaitė, Kazimieras Melaika, Osvaldas Rukšėnas, Vaiva Hendrixson, and Saulius Ročka. 2023. "Remotely Programmable Deep Brain Stimulator Combined with an Invasive Blood Pressure Monitoring System for a Non-Tethered Rat Model in Hypertension Research" Brain Sciences 13, no. 3: 504. https://doi.org/10.3390/brainsci13030504