
Association between Systemic Immune Inflammation Index and Cognitive Impairment after Acute Ischemic Stroke

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample
2.2. Baseline Data Collection
2.3. Assessment of Cognitive Function
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Prevalence and Risk Factors of PSCI
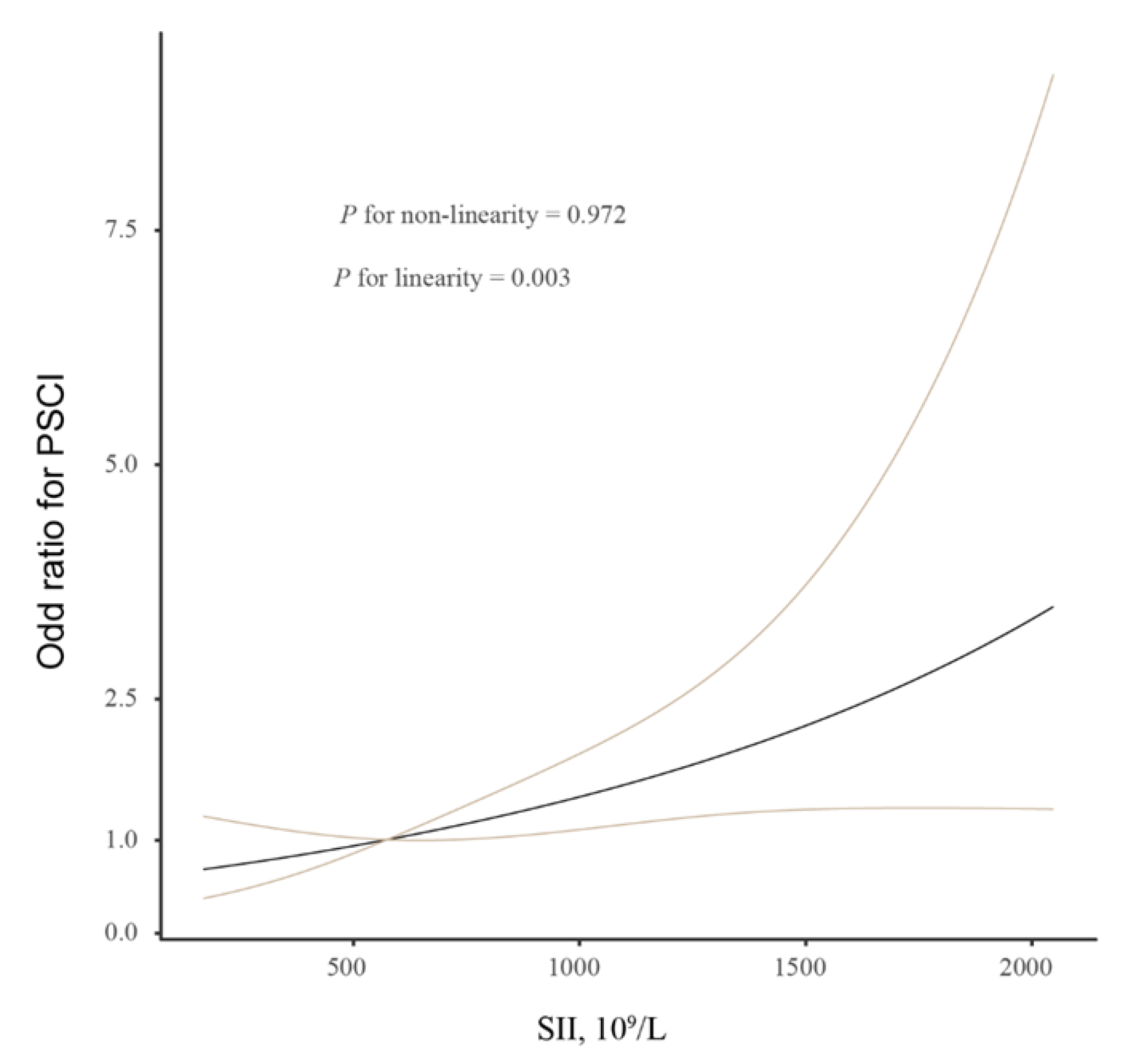
3.3. Logistic Regression Analysis for the Relationship between the SII Index and PSCI
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, Y.J.; Li, Z.X.; Gu, H.Q.; Zhai, Y.; Jiang, Y.; Zhao, X.Q.; Zhao, J.Z. China Stroke Statistics 2019: A Report from the National Center for Healthcare Quality Management in Neurological Diseases, China National Clinical Research Center for Neurological Diseases, the Chinese Stroke Association, National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention and Institute for Global Neuroscience and Stroke Collaborations. Stroke Vasc. Neurol. 2020, 5, 211–239. [Google Scholar]
- GBD 2016 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar] [CrossRef] [Green Version]
- Wu, S.; Wu, B.O.; Liu, M.; Chen, Z.; Wang, W.; Anderson, C.S.; Zhang, S. Stroke in China: Advances and challenges in epidemiology, prevention, and management. Lancet Neurol. 2019, 18, 394–405. [Google Scholar] [CrossRef]
- Soto-Camara, R.; Gonzalez-Santos, J.; González-Berna, J.; Trejo-Gabriel-Galan, J.M. Factors associated with a rapid call for assistance for patients with ischemic stroke. Emergencias 2020, 32, 33–39. [Google Scholar]
- Tu, W.J.; Hua, Y.; Yan, F.; Bian, H.; Yang, Y.; Lou, M.; Wang, L. Prevalence of stroke in China, 2013–2019: A population-based study. Lancet Reg. Health W. Pac. 2022, 28, 100550. [Google Scholar] [CrossRef]
- Sun, J.; Tan, L.; Yu, J. Post-stroke cognitive impairment: Epidemiology, mechanisms and management. Ann. Transl. Med. 2014, 2, 80. [Google Scholar]
- Pendlebury, S.; Rothwell, P. Prevalence, incidence, and factors associated with pre-stroke and post-stroke dementia: A systematic review and meta-analysis. Lancet Neurol. 2009, 8, 1006–1018. [Google Scholar] [CrossRef]
- Pendlebury, S.; Rothwell, P. Incidence and prevalence of dementia associated with transient ischaemic attack and stroke: Analysis of the population-based Oxford Vascular Study. Lancet Neurol. 2019, 18, 248–258. [Google Scholar] [CrossRef] [Green Version]
- Brainin, M.; Tuomilehto, J.; Heiss, W.D.; Bornstein, N.M.; Bath, P.M.; Teuschl, Y. Post Stroke Cognition Study Group. Post-stroke cognitive decline: An update and perspectives for clinical research. Eur. J. Neurol. 2015, 22, 229-e16. [Google Scholar] [CrossRef]
- Kim, J.Y.; Kawabori, M.; Yenari, M.A. Innate inflammatory responses in stroke: Mechanisms and potential therapeutic targets. Curr. Med. Chem. 2014, 21, 2076–2097. [Google Scholar] [CrossRef] [Green Version]
- Pagram, H.; Bivard, A.; Lincz, L.F.; Levi, C. Peripheral Immune Cell Counts and Advanced Imaging as Biomarkers of Stroke Outcome. Cerebrovasc. Dis. Extra. 2016, 6, 120–128. [Google Scholar] [CrossRef]
- Kim, J.; Park, J.; Chang, J.; Kim, S.; Lee, J. Inflammation after Ischemic Stroke: The Role of Leukocytes and Glial Cells. Exp. Neurobiol. 2016, 25, 241–251. [Google Scholar] [CrossRef] [Green Version]
- Chamorro, Á.; Meisel, A.; Planas, A.; Urra, X.; Van de Beek, D.; Veltkamp, R. The immunology of acute stroke. Nat. Rev. Neurol. 2012, 8, 401–410. [Google Scholar] [CrossRef]
- Chen, G.; Nuñez, G. Sterile inflammation: Sensing and reacting to damage. Nat. Rev. Immunol. 2010, 10, 826–837. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Bi, X. Post-Stroke Cognitive Impairment: A Review Focusing on Molecular Biomarkers. J. Mol. Neurosci. 2020, 70, 1244–1254. [Google Scholar] [CrossRef]
- Hu, B.; Yang, X.R.; Xu, Y.; Sun, Y.F.; Sun, C.; Guo, W.; Fan, J. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin. Cancer Res. 2014, 20, 6212–6622. [Google Scholar] [CrossRef] [Green Version]
- Wang, B.L.; Tian, L.; Gao, X.H.; Ma, X.L.; Wu, J.; Zhang, C.Y.; Yang, X.R. Dynamic change of the systemic immune inflammation index predicts the prognosis of patients with hepatocellular carcinoma after curative resection. Clin. Chem. Lab. Med. 2016, 54, 1963–1969. [Google Scholar] [CrossRef]
- Zhang, B.; Yao, W. Prognostic role of the systemic immune-inflammation index in biliary tract cancers: A meta-analysis of 3515 patients. World J. Surg. Oncol. 2022, 20, 320. [Google Scholar] [CrossRef]
- Liang, R.; Chen, N.; Li, M.; Wang, X.; Mao, Q.; Liu, Y. Significance of systemic immune-inflammation index in the differential diagnosis of high- and low-grade gliomas. Clin. Neurol. Neurosurg. 2018, 164, 50–52. [Google Scholar] [CrossRef]
- Hu, J.; Wang, L.; Fan, K.; Ren, W.; Wang, Q.; Ruan, Y.; He, J. The Association Between Systemic Inflammatory Markers and Post-Stroke Depression: A Prospective Stroke Cohort. Clin. Interv./Aging. 2021, 16, 1231–1239. [Google Scholar] [CrossRef]
- Çırakoğlu, Ö.; Yılmaz, A. Systemic immune-inflammation index is associated with increased carotid intima-media thickness in hypertensive patients. Clin. Exp. Hypertens. 2021, 43, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Weng, Y.; Zeng, T.; Huang, H.; Ren, J.; Wang, J.; Yang, C.; Chen, G. Systemic Immune-Inflammation Index Predicts 3-Month Functional Outcome in Acute Ischemic Stroke Patients Treated with Intravenous Thrombolysis. Clin. Interv. Aging. 2021, 16, 877–886. [Google Scholar] [CrossRef] [PubMed]
- Yi, H.J.; Sung, J.H.; Lee, D.H. Systemic Inflammation Response Index and Systemic Immune-Inflammation Index Are Associated with Clinical Outcomes in Patients Treated with Mechanical Thrombectomy for Large Artery Occlusion. World Neurosurg. 2021, 153, e282–e289. [Google Scholar] [CrossRef] [PubMed]
- Muir, K.; Weir, C.; Murray, G.; Povey, C.; Lees, K. Comparison of neurological scales and scoring systems for acute stroke prognosis. Stroke 1996, 27, 1817–1820. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.J.; Bendixen, B.; Kappelle, L.; Biller, J.; Love, B.; Gordon, D. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, F.; Li, Y.; Zhao, Y.; Sun, M.; He, Q.; Wen, R.; Xie, Z. Systemic immune-inflammation index predicts the outcome after aneurysmal subarachnoid hemorrhage. Neurosurg. Rev. 2022, 45, 1607–1615. [Google Scholar] [CrossRef] [PubMed]
- Xu, M.; Chen, R.; Liu, L.; Liu, X.; Hou, J.; Liao, J.; Hu, P. Systemic immune-inflammation index and incident cardiovascular diseases among middle-aged and elderly Chinese adults: The Dongfeng-Tongji cohort study. Atherosclerosis 2021, 323, 20–29. [Google Scholar] [CrossRef]
- Nasreddine, Z.; Phillips, N.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Webb, A.; Pendlebury, S.; Li, L. Validation of the Montreal cognitive assessment versus mini-mental state examination against hypertension and hypertensive arteriopathy after transient ischemic attack or minor stroke. Stroke 2014, 45, 3337–3342. [Google Scholar] [CrossRef] [Green Version]
- Zhong, C.; Bu, X.; Xu, T.; Guo, L.; Wang, X.; Zhang, J.; He, J. Serum Matrix Metalloproteinase-9 and Cognitive Impairment After Acute Ischemic Stroke. J. Am. Heart Assoc. 2018, 7, e007776. [Google Scholar] [CrossRef] [Green Version]
- Alves, H.C.; Treurniet, K.M.; Dutra, B.G.; Jansen, I.G.; Boers, A.M.; Santos, E.M.; Majoie, C.B. Associations Between Collateral Status and Thrombus Characteristics and Their Impact in Anterior Circulation Stroke. Stroke 2018, 49, 391–396. [Google Scholar] [CrossRef]
- Mohd, Z.M.; Ghazali, S.; Che, D.N.; Singh, D.; Subramaniam, P. A Review of Risk Factors for Cognitive Impairment in Stroke Survivors. Sci. World J. 2016, 2016, 3456943. [Google Scholar]
- Duda, B.; Puente, A.; Miller, L. Cognitive reserve moderates relation between global cognition and functional status in older adults. J. Clin. Exp. Neuropsychol. 2014, 36, 368–378. [Google Scholar] [CrossRef]
- Ahmad, W. Overlapped metabolic and therapeutic links between Alzheimer and diabetes. Mol. Neurobiol. 2013, 47, 399–424. [Google Scholar] [CrossRef] [PubMed]
- Yun, S.; Yi, H.; Lee, D.; Sung, J. Systemic Inflammation Response Index and Systemic Immune-inflammation Index for Predicting the Prognosis of Patients with Aneurysmal Subarachnoid Hemorrhage. J. Stroke Cerebrovasc. Dis. 2021, 30, 105861. [Google Scholar] [CrossRef] [PubMed]
- Swardfager, W.; Winer, D.; Herrmann, N.; Winer, S.; Lanctôt, K. Interleukin-17 in post-stroke neurodegeneration. Neurosci. Biobehav. Rev. 2013, 37, 436–447. [Google Scholar] [CrossRef] [PubMed]
- Ong, C.W.; Pabisiak, P.J.; Brilha, S.; Singh, P.; Roncaroli, F.; Elkington, P.T.; Friedland, J.S. Complex regulation of neutrophil-derived MMP-9 secretion in central nervous system tuberculosis. J. Neuroinflammation. 2017, 14, 31. [Google Scholar] [CrossRef] [Green Version]
- Winterbourn, C.; Kettle, A.; Hampton, M. Reactive Oxygen Species and Neutrophil Function. Annu. Rev. Biochem. 2016, 85, 765–792. [Google Scholar] [CrossRef]
- Gill, D.; Veltkamp, R. Dynamics of T cell responses after stroke. Curr. Opin. Pharmacol. 2016, 26, 26–32. [Google Scholar] [CrossRef]
- Rosenberg, G.; Sullivan, N.; Esiri, M. White matter damage is associated with matrix metalloproteinases in vascular dementia. Stroke 2001, 32, 1162–1168. [Google Scholar] [CrossRef] [Green Version]
- Maugeri, N.; Rovere-Querini, P.; Evangelista, V.; Covino, C.; Capobianco, A.; Bertilaccio, M.T.; Manfredi, A.A. Neutrophils phagocytose activated platelets in vivo: A phosphatidylserine, P-selectin, and {beta}2 integrin-dependent cell clearance program. Blood 2009, 113, 5254–5265. [Google Scholar] [CrossRef] [PubMed]
- Miranda, M.; Morici, J.; Zanoni, M.; Bekinschtein, P. Brain-Derived Neurotrophic Factor: A Key Molecule for Memory in the Healthy and the Pathological Brain. Front. Cell. Neurosci. 2019, 13, 363. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | SII Index | ||||
|---|---|---|---|---|---|
| First Quartile, n = 64 | Second Quartile, n = 64 | Third Quartile, n = 63 | Fourth Quartile, n = 63 | p-Value | |
| Demographic characteristic | |||||
| Age, year | 63.0 ± 9.8 | 65.7 ± 9.5 | 64.9 ± 11.9 | 68.6 ± 8.8 | 0.019 |
| Male, % | 41 (64.1) | 28 (43.8) | 40 (63.5) | 34 (54.0) | 0.108 |
| Vascular risk factors, % | |||||
| Hypertension | 48 (75.0) | 42 (65.6) | 40 (63.5) | 44 (69.8) | 0.516 |
| Diabetes | 20 (31.3) | 18 (28.1) | 20 (31.7) | 12 (19.0) | 0.350 |
| Hyperlipidemia | 7 (10.9) | 10 (15.6) | 9 (14.3) | 12 (19.0) | 0.640 |
| Coronary heart disease | 8 (12.5) | 10 (15.6) | 12 (19.0) | 12 (19.0) | 0.713 |
| Current smoking | 30 (46.9) | 23 (35.9) | 20 (31.7) | 25 (39.7) | 0.345 |
| Current drinking | 22 (34.4) | 23 (35.9) | 29 (46.0) | 24 (38.1) | 0.542 |
| Clinical data | |||||
| Onset-to-blood drawing time, day | 2.0 (1.0, 3.0) | 2.0 (1.0, 3.0) | 2.0 (1.0, 3.0) | 2.0 (2.0, 3.0) | 0.335 |
| Educational status, years | 9.0 (6.0, 12.0) | 9.0 (6.0, 9.0) | 8.0 (6.0, 9.0) | 9.0 (7.0, 12.0) | 0.341 |
| Systolic blood pressure, mmHg | 137.3 ± 17.0 | 139.7 ± 16.1 | 133.9 ± 18.4 | 137.1 ± 18.7 | 0.324 |
| Diastolic blood pressure, mmHg | 80.1 ± 8.6 | 81.9 ± 9.9 | 77.5 ± 10.0 | 83.7 ± 11.0 | 0.004 |
| Baseline NIHSS, score | 3.0 (2.0, 4.0) | 3.0 (2.0, 4.0) | 4.0 (2.0, 6.0) | 4.0 (2.0, 5.0) | 0.285 |
| Previous antiplatelet, % | 23 (35.9) | 18 (28.1) | 15 (23.8) | 15 (23.8) | 0.376 |
| Previous statin, % | 21 (32.8) | 15 (23.4) | 20 (31.7) | 13 (20.6) | 0.320 |
| PSCI, % | 28 (43.8) | 25 (39.1) | 30 (47.6) | 47 (74.6) | 0.001 |
| Stroke subtypes, % | 0.143 | ||||
| Large artery atherosclerosis | 20 (31.3) | 30 (46.9) | 30 (47.6) | 26 (41.3) | |
| Cardioembolism | 20 (31.3) | 11 (17.2) | 12 (19.0) | 10 (15.9) | |
| Small artery occlusion | 23 (35.9) | 20 (31.3) | 16 (5.4) | 20 (31.7) | |
| Others | 1 (1.6) | 3 (4.7) | 5 (7.9) | 7 (11.1) | |
| Laboratory data | |||||
| Total cholesterol, mmol/L | 4.0 ± 1.1 | 3.9 ± 1.1 | 3.9 ± 0.9 | 4.0 ± 1.0 | 0.972 |
| Triglyceride, mmol/L | 1.5 ± 0.7 | 1.6 ± 0.7 | 1.5 ± 0.8 | 1.4 ± 0.6 | 0.434 |
| Low-density lipoprotein, mmol/L | 2.4 ± 0.8 | 2.4 ± 0.9 | 2.5 ± 0.6 | 2.5 ± 0.9 | 0.706 |
| High-density lipoprotein, mmol/L | 1.1 ± 0.3 | 1.1 ± 0.2 | 1.1 ± 0.3 | 1.1 ± 0.2 | 0.588 |
| Hs-CRP, mg/L | 4.8 (2.3, 8.1) | 4.2 (2.2, 7.8) | 5.8 (3.3, 9.1) | 7.2 (3.3, 14.0) | 0.049 |
| Fasting blood glucose, mmol/L | 6.3 ± 2.7 | 6.0 ± 2.5 | 6.5 ± 3.0 | 5.5 ± 2.5 | 0.174 |
| Variables | With PSCI, n = 130 | Without PSCI, n = 124 | p Value |
|---|---|---|---|
| Demographic characteristic | |||
| Age, year | 67.3 ± 8.9 | 63.4 ± 11.1 | 0.004 |
| Male, % | 70 (53.8) | 73 (58.9) | 0.420 |
| Vascular risk factors, % | |||
| Hypertension | 97 (74.6) | 77 (62.1) | 0.032 |
| Diabetes | 44 (33.8) | 26 (21.0) | 0.022 |
| Hyperlipidemia | 19 (14.6) | 19 (15.3) | 0.874 |
| Coronary heart disease | 22 (16.9) | 20 (16.1) | 0.865 |
| Current smoking | 48 (36.9) | 50 (40.3) | 0.578 |
| Current drinking | 49 (37.7) | 49 (39.5) | 0.765 |
| Clinical data | |||
| Onset-to-blood drawing time, day | 2.0 (1.0, 3.0) | 2.0 (1.0, 3.0) | 0.812 |
| Educational status, years | 9.0 (6.0, 9.0) | 9.0 (7.0, 12.0) | 0.039 |
| Systolic blood pressure, mmHg | 136.7 ± 17.0 | 137.3 ± 18.3 | 0.806 |
| Diastolic blood pressure, mmHg | 81.1 ± 10.0 | 80.5 ± 10.0 | 0.637 |
| Baseline NIHSS, score | 4.0 (2.0, 6.0) | 3.0 (2.0, 4.0) | 0.001 |
| Previous antiplatelet, % | 38 (29.2) | 33 (26.6) | 0.642 |
| Previous statin, % | 37 (28.5) | 32 (25.8) | 0.634 |
| Stroke subtypes, % | 0.035 | ||
| Large artery atherosclerosis | 63 (48.5) | 43 (34.7) | |
| Cardioembolism | 28 (21.5) | 25 (20.2) | |
| Small artery occlusion | 30 (23.1) | 49 (39.5) | |
| Others | 9 (6.9) | 7 (5.6) | |
| Laboratory data | |||
| Total cholesterol, mmol/L | 3.9 ± 1.0 | 4.0 ± 1.0 | 0.374 |
| Triglyceride, mmol/L | 1.5 ± 0.6 | 1.5 ± 0.8 | 0.968 |
| Low-density lipoprotein, mmol/L | 2.3 ± 0.8 | 2.5 ± 0.8 | 0.134 |
| High-density lipoprotein, mmol/L | 1.1 ± 0.3 | 1.1 ± 0.2 | 0.363 |
| Hs-CRP, mg/L | 6.8 (2.9, 10.0) | 4.5 (2.6, 7.8) | 0.031 |
| Fasting blood glucose, mmol/L | 6.1 ± 2.6 | 6.1 ± 2.8 | 0.983 |
| SII index, ×109/L | 653.9 (352.7, 1117.9) | 493.1 (300.5, 745.1) | 0.001 |
| SII quartile, % | 0.001 | ||
| First | 28 (21.5) | 36 (29.0) | |
| Second | 25 (19.2) | 39 (31.5) | |
| Third | 30 (23.1) | 33 (26.6) | |
| Fourth | 47 (36.2) | 16 (12.9) |
| Variables | PSCI | PSCI Severity | ||
|---|---|---|---|---|
| OR (95%CI) | p Value | OR (95%CI) | p Value | |
| Crude model | ||||
| SII index (per-SD increase) | 2.191 (1.437–3.338) | 0.001 | 1.791 (1.301–2.480) | 0.001 |
| SII quartile | ||||
| First | Reference | Reference | ||
| Second | 0.820 (0.408–1.667) | 0.590 | 2.630 (1.362–5.078) | 0.004 |
| Third | 1.169 (0.581–2.351) | 0.662 | 3.504 (1.787–6.862) | 0.001 |
| Fourth | 3.777 (1.780–8.013) | 0.001 | 2.669 (1.379–5.170) | 0.003 |
| Model 1 | ||||
| SII index (per-SD increase) | 2.045 (1.347–3.106) | 0.001 | 1.726 (1.270–2.347) | 0.001 |
| SII quartile | ||||
| First | Reference | Reference | ||
| Second | 0.726 (0.352–1.496) | 0.385 | 2.326 (1.189–4.549) | 0.014 |
| Third | 1.106 (0.543–2.251) | 0.781 | 3.340 (1.696–6.573) | 0.001 |
| Fourth | 3.201 (1.486–6.894) | 0.001 | 2.522 (1.291–4.918) | 0.001 |
| Model 2 | ||||
| SII index (per-SD increase) | 2.341 (1.439–3.809) | 0.001 | 1.879 (1.324–2.537) | 0.001 |
| SII quartile | ||||
| First | Reference | Reference | ||
| Second | 0.644 (0.292–1.421) | 0.276 | 2.927 (1.398–6.134) | 0.004 |
| Third | 0.943 (0.432–2.059) | 0.882 | 4.473 (2.145–9.319) | 0.001 |
| Fourth | 3.993 (1.685–9.462) | 0.002 | 3.435 (1.665–7.085) | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bao, Y.; Wang, L.; Du, C.; Ji, Y.; Dai, Y.; Jiang, W. Association between Systemic Immune Inflammation Index and Cognitive Impairment after Acute Ischemic Stroke. Brain Sci. 2023, 13, 464. https://doi.org/10.3390/brainsci13030464
Bao Y, Wang L, Du C, Ji Y, Dai Y, Jiang W. Association between Systemic Immune Inflammation Index and Cognitive Impairment after Acute Ischemic Stroke. Brain Sciences. 2023; 13(3):464. https://doi.org/10.3390/brainsci13030464
Chicago/Turabian StyleBao, Yuanfei, Lingling Wang, Chaopin Du, Yan Ji, Yiwei Dai, and Wei Jiang. 2023. "Association between Systemic Immune Inflammation Index and Cognitive Impairment after Acute Ischemic Stroke" Brain Sciences 13, no. 3: 464. https://doi.org/10.3390/brainsci13030464