
Retinal Alterations as Potential Biomarkers of Structural Brain Changes in Alzheimer’s Disease Spectrum Patients
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
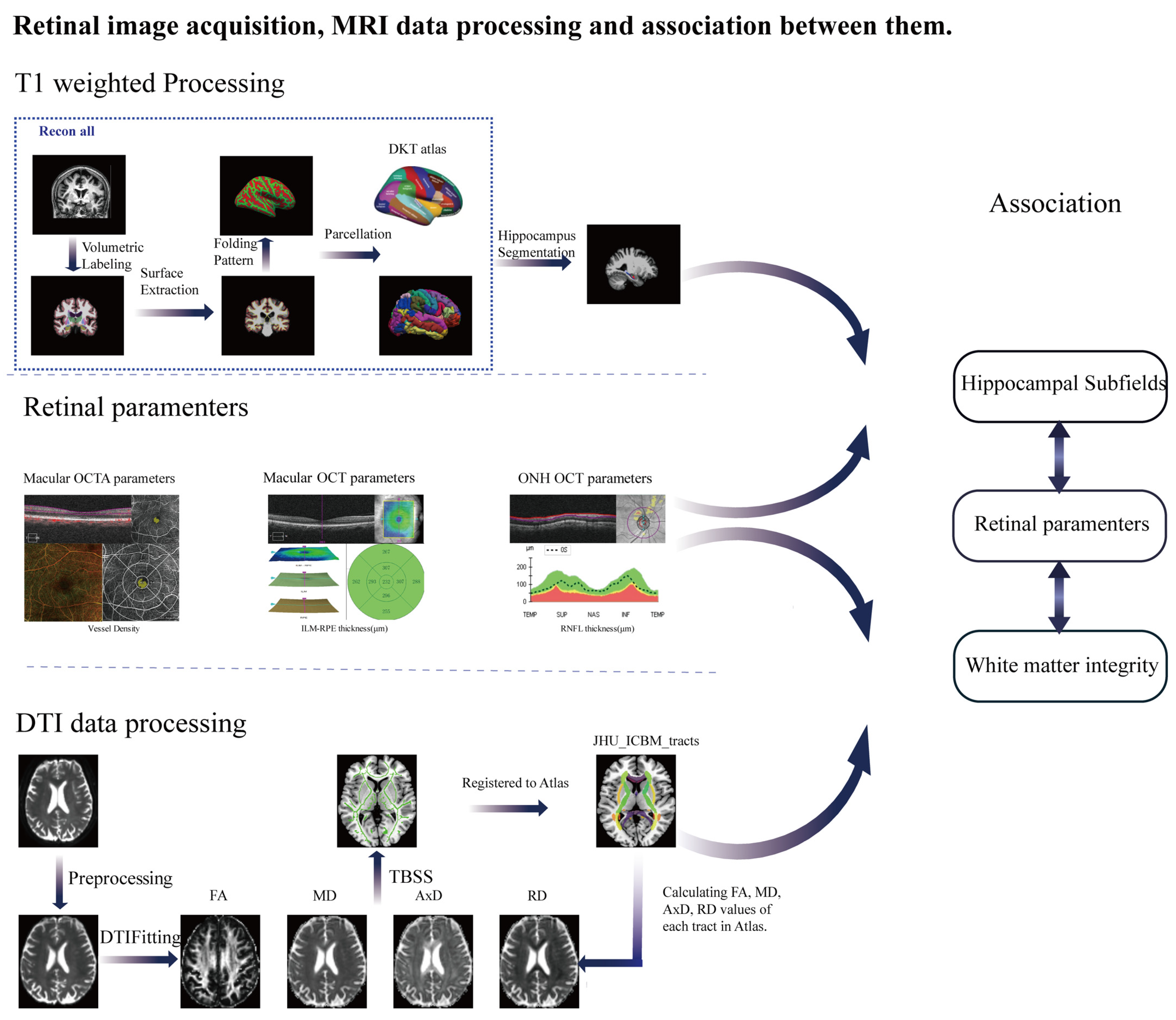
2.2. MRI Data Acquisition
2.3. MRI Analysis
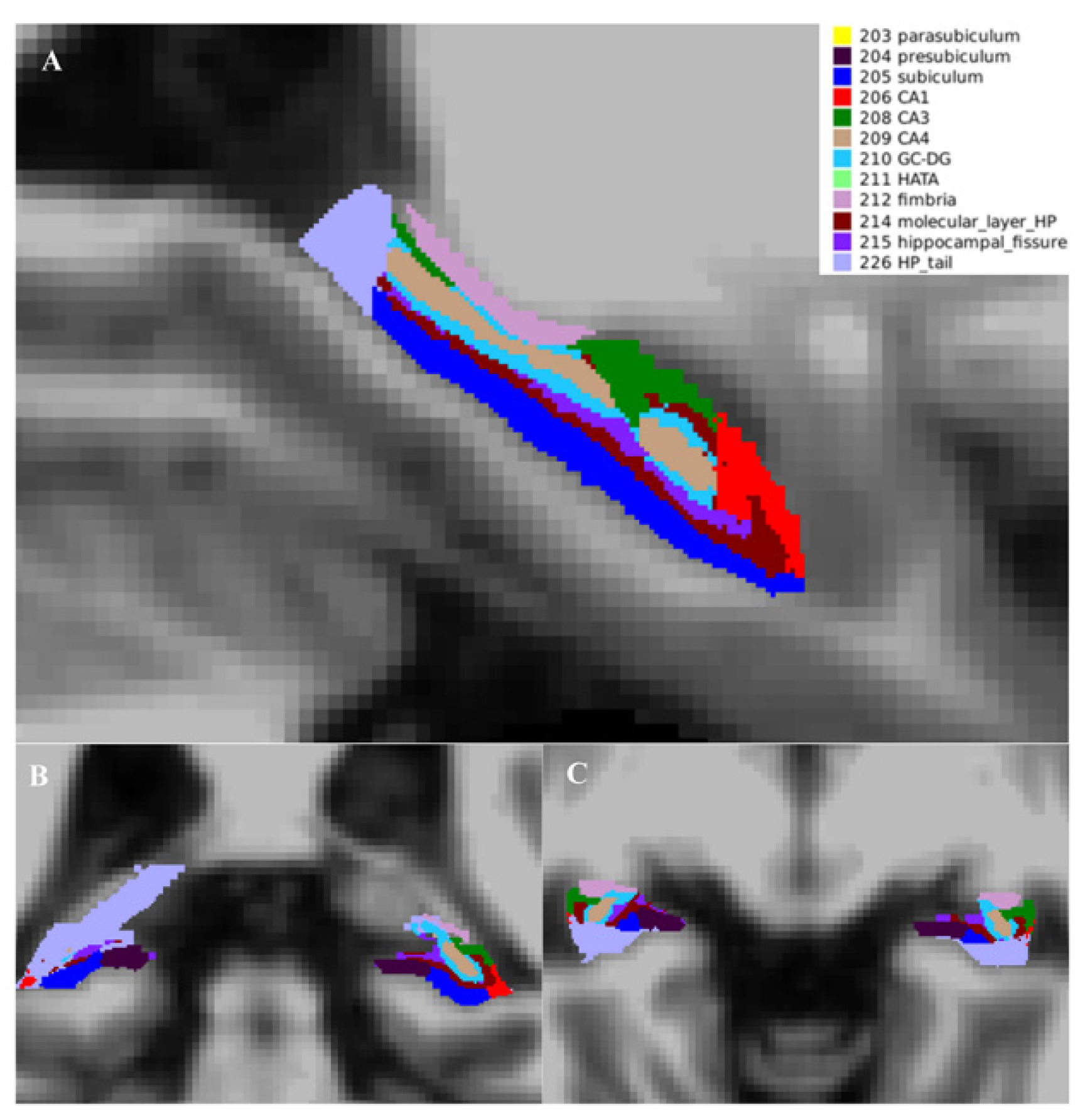
2.3.1. Hippocampal Subfield Acquisition
2.3.2. DTI Processing
2.4. Retinal Image Acquisition
2.5. Statistical Analysis
3. Results
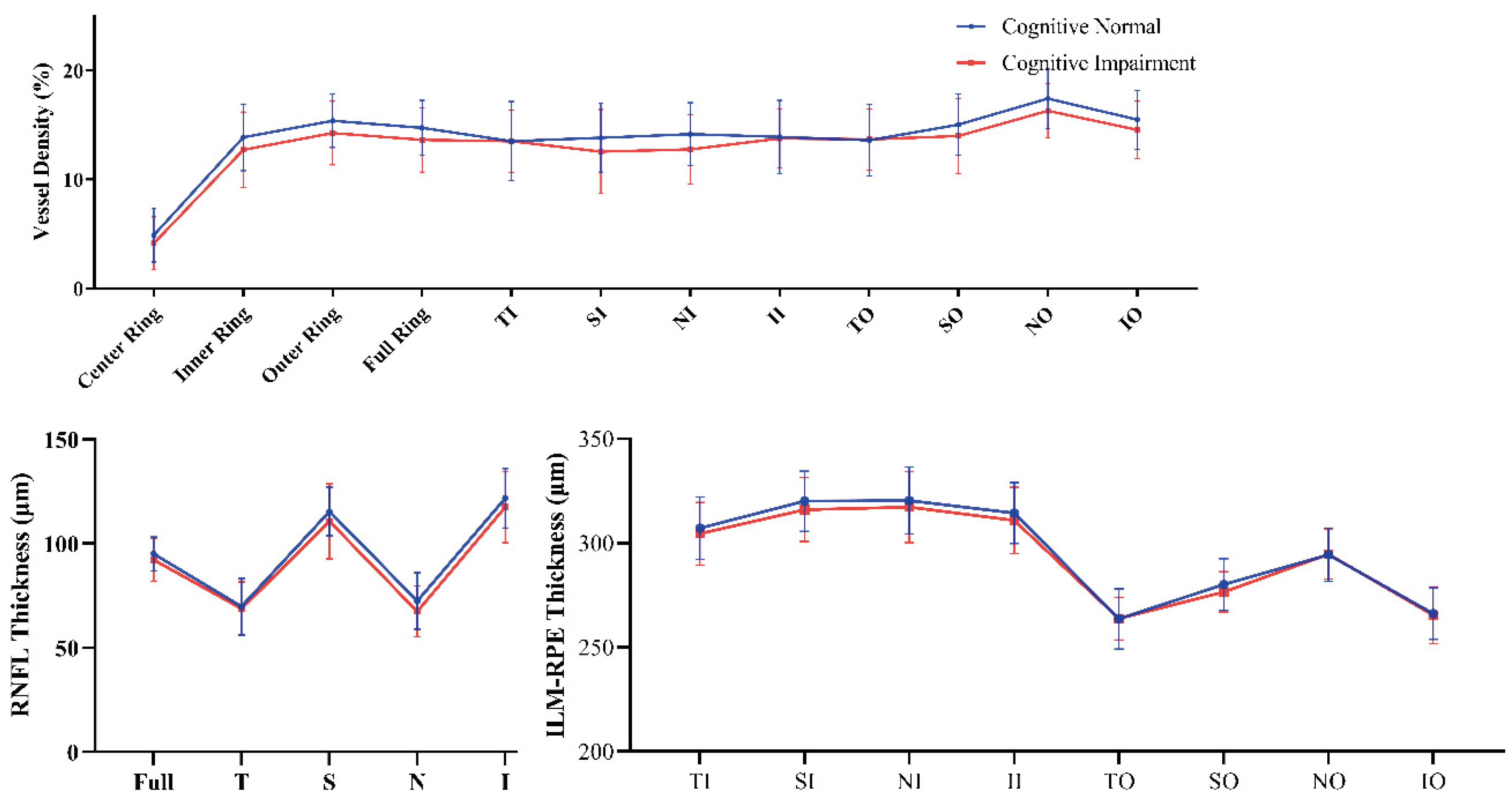
3.1. Demographic, Neuropsychological Characteristics and Retinal Measures
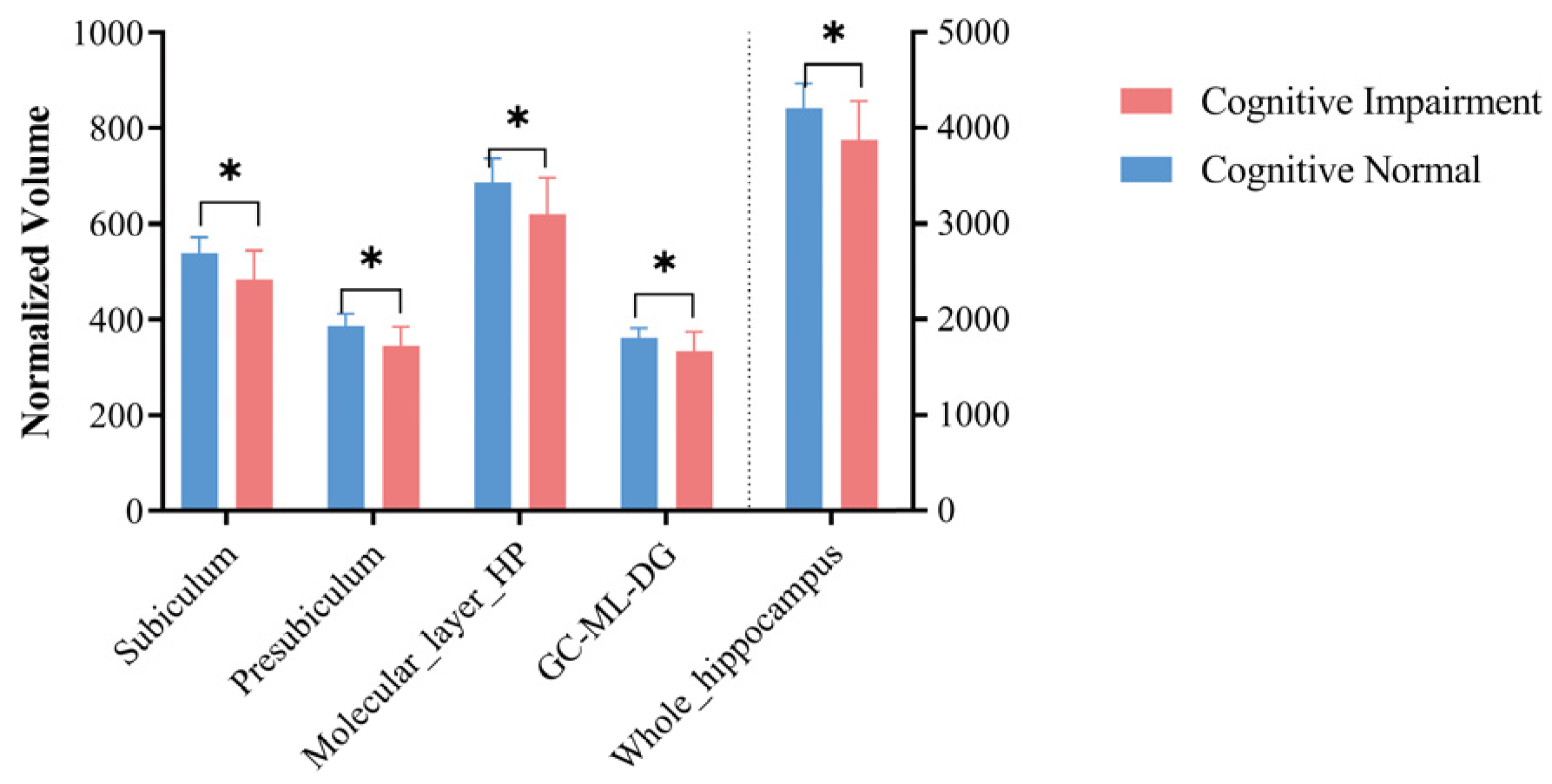
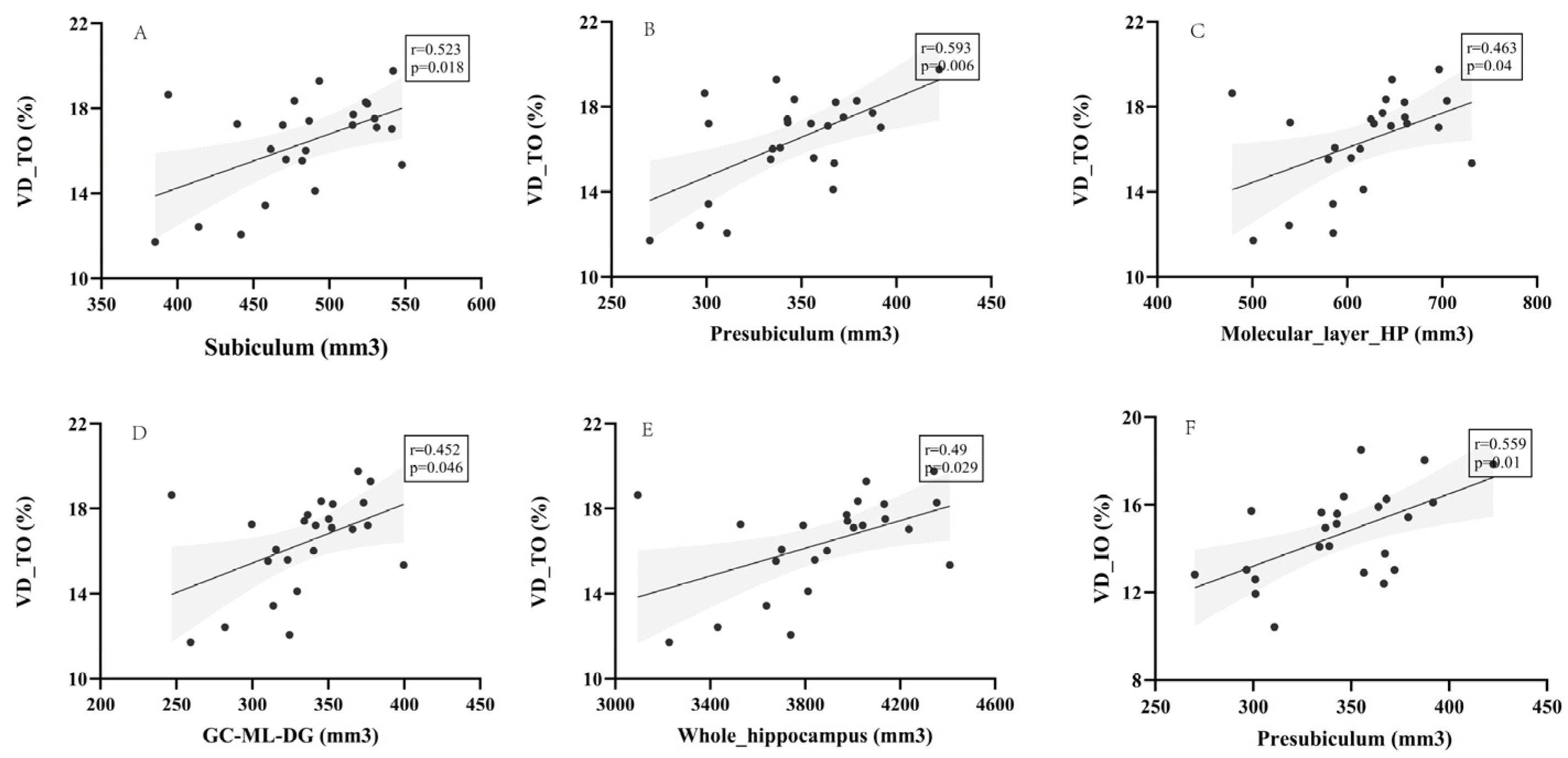
3.2. Hippocampal Volume and Its Association with Retinal Measures
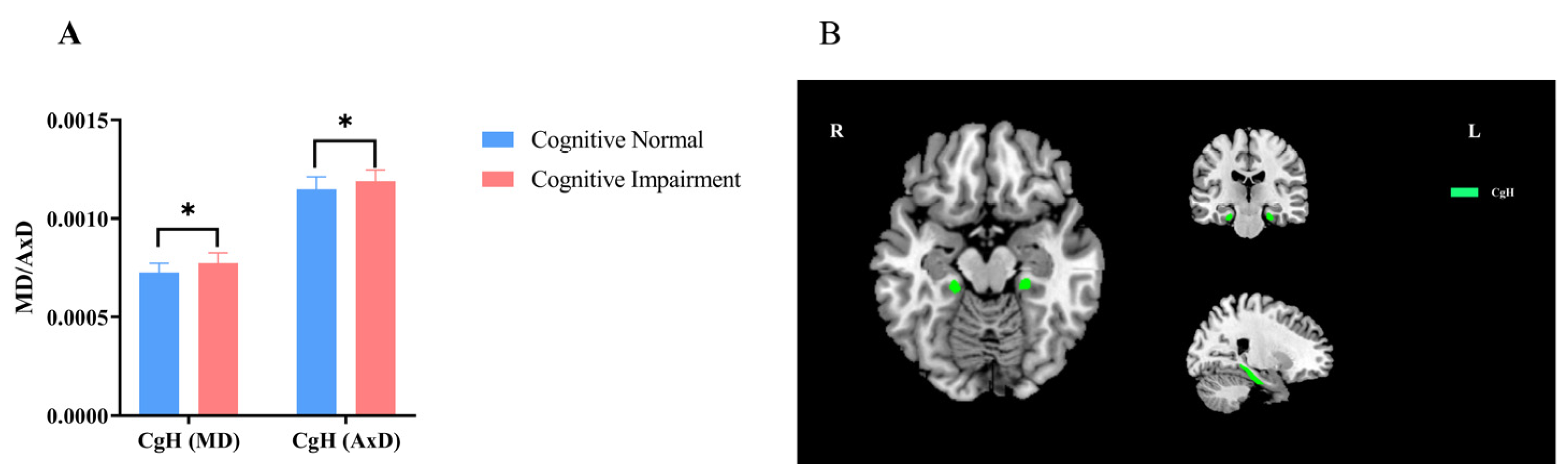
3.3. WM Integrity and Its Association with Retinal Measures
4. Discussion
4.1. Volumetric Comparisons of the Hippocampal Subfield Volumes and Correlations with Retinal OCTA Parameters
4.2. Microstructural Comparisons of WM Integrity and Correlations with Retinal OCTA Parameters
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hodson, R. Alzheimer’s disease. Nature 2018, 559, S1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vega, J.N.; Newhouse, P.A. Mild cognitive impairment: Diagnosis, longitudinal course, and emerging treatments. Curr. Psychiatry Rep. 2014, 16, 490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Márquez, F.; Yassa, M.A. Neuroimaging Biomarkers for Alzheimer’s Disease. Mol. Neurodegener. 2019, 14, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- London, A.; Benhar, I.; Schwartz, M. The retina as a window to the brain-from eye research to CNS disorders. Nat. Rev. Neurol. 2013, 9, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Gasparini, L.; Crowther, R.A.; Martin, K.R.; Berg, N.; Coleman, M.; Goedert, M.; Spillantini, M.G. Tau inclusions in retinal ganglion cells of human P301S tau transgenic mice: Effects on axonal viability. Neurobiol. Aging 2011, 32, 419–433. [Google Scholar] [CrossRef]
- Koronyo-Hamaoui, M.; Koronyo, Y.; Ljubimov, A.V.; Miller, C.A.; Ko, M.K.; Black, K.L.; Schwartz, M.; Farkas, D.L. Identification of amyloid plaques in retinas from Alzheimer’s patients and noninvasive in vivo optical imaging of retinal plaques in a mouse model. NeuroImage 2011, 54 (Suppl. 1), S204–S217. [Google Scholar] [CrossRef] [Green Version]
- La Morgia, C.; Ross-Cisneros, F.N.; Koronyo, Y.; Hannibal, J.; Gallassi, R.; Cantalupo, G.; Sambati, L.; Pan, B.X.; Tozer, K.R.; Barboni, P.; et al. Melanopsin retinal ganglion cell loss in Alzheimer disease. Ann. Neurol. 2016, 79, 90–109. [Google Scholar] [CrossRef]
- Schön, C.; Hoffmann, N.A.; Ochs, S.M.; Burgold, S.; Filser, S.; Steinbach, S.; Seeliger, M.W.; Arzberger, T.; Goedert, M.; Kretzschmar, H.A.; et al. Long-term in vivo imaging of fibrillar tau in the retina of P301S transgenic mice. PLoS ONE 2012, 7, e53547. [Google Scholar] [CrossRef]
- Tsuruma, K.; Tanaka, Y.; Shimazawa, M.; Hara, H. Induction of amyloid precursor protein by the neurotoxic peptide, amyloid-beta 25–35, causes retinal ganglion cell death. J. Neurochem. 2010, 113, 1545–1554. [Google Scholar] [CrossRef]
- Cao, L.; Wang, H.; Wang, F.; Xu, D.; Liu, F.; Liu, C. Aβ-induced senescent retinal pigment epithelial cells create a proinflammatory microenvironment in AMD. Investig. Ophthalmol. Vis. Sci. 2013, 54, 3738–3750. [Google Scholar] [CrossRef] [Green Version]
- Hinton, D.R.; Sadun, A.A.; Blanks, J.C.; Miller, C.A. Optic-nerve degeneration in Alzheimer’s disease. N. Engl. J. Med. 1986, 315, 485–487. [Google Scholar] [CrossRef] [PubMed]
- Perez, S.E.; Lumayag, S.; Kovacs, B.; Mufson, E.J.; Xu, S. Beta-amyloid deposition and functional impairment in the retina of the APPswe/PS1DeltaE9 transgenic mouse model of Alzheimer’s disease. Investig. Ophthalmol. Vis. Sci. 2009, 50, 793–800. [Google Scholar] [CrossRef] [PubMed]
- Ning, A.; Cui, J.; To, E.; Ashe, K.H.; Matsubara, J. Amyloid-beta deposits lead to retinal degeneration in a mouse model of Alzheimer disease. Investig. Ophthalmol. Vis. Sci. 2008, 49, 5136–5143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, H.; Koronyo, Y.; Fuchs, D.-T.; Sheyn, J.; Wawrowsky, K.; Lahiri, S.; Black, K.L.; Koronyo-Hamaoui, M. Retinal capillary degeneration and blood-retinal barrier disruption in murine models of Alzheimer’s disease. Acta Neuropathol. Commun. 2020, 8, 202. [Google Scholar] [CrossRef]
- Shi, H.; Koronyo, Y.; Rentsendorj, A.; Regis, G.C.; Sheyn, J.; Fuchs, D.-T.; Kramerov, A.A.; Ljubimov, A.V.; Dumitrascu, O.M.; Rodriguez, A.R.; et al. Identification of early pericyte loss and vascular amyloidosis in Alzheimer’s disease retina. Acta Neuropathol. 2020, 139, 813–836. [Google Scholar] [CrossRef] [Green Version]
- Tadokoro, K.; Yamashita, T.; Kimura, S.; Nomura, E.; Ohta, Y.; Omote, Y.; Takemoto, M.; Hishikawa, N.; Morihara, R.; Morizane, Y.; et al. Retinal Amyloid Imaging for Screening Alzheimer’s Disease. J. Alzheimer’s Dis. JAD 2021, 83, 927–934. [Google Scholar] [CrossRef]
- Dumitrascu, O.M.; Lyden, P.D.; Torbati, T.; Sheyn, J.; Sherzai, A.; Sherzai, D.; Sherman, D.S.; Rosenberry, R.; Cheng, S.; Johnson, K.O.; et al. Sectoral segmentation of retinal amyloid imaging in subjects with cognitive decline. Alzheimers Dement. 2020, 12, e12109. [Google Scholar] [CrossRef]
- Koronyo, Y.; Rentsendorj, A.; Mirzaei, N.; Regis, G.C.; Sheyn, J.; Shi, H.; Barron, E.; Cook-Wiens, G.; Rodriguez, A.R.; Medeiros, R.; et al. Retinal pathological features and proteome signatures of Alzheimer’s disease. Acta Neuropathol. 2023. [Google Scholar] [CrossRef]
- Meleppat, R.K.; Fortenbach, C.R.; Jian, Y.; Martinez, E.S.; Wagner, K.; Modjtahedi, B.S.; Motta, M.J.; Ramamurthy, D.L.; Schwab, I.R.; Zawadzki, R.J. In Vivo Imaging of Retinal and Choroidal Morphology and Vascular Plexuses of Vertebrates Using Swept-Source Optical Coherence Tomography. Transl. Vis. Sci. Technol. 2022, 11, 11. [Google Scholar] [CrossRef]
- Meleppat, R.K.; Ronning, K.E.; Karlen, S.J.; Burns, M.E.; Pugh, E.N.; Zawadzki, R.J. In vivo multimodal retinal imaging of disease-related pigmentary changes in retinal pigment epithelium. Sci. Rep. 2021, 11, 16252. [Google Scholar] [CrossRef]
- De Carlo, T.E.; Romano, A.; Waheed, N.K.; Duker, J.S. A review of optical coherence tomography angiography (OCTA). Int. J. Retin. Vitr. 2015, 1, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, C.Y.; Mok, V.; Foster, P.J.; Trucco, E.; Chen, C.; Wong, T.Y. Retinal imaging in Alzheimer’s disease. J. Neurol. Neurosurg. Psychiatry 2021, 92, 983–994. [Google Scholar] [CrossRef] [PubMed]
- Ge, Y.-J.; Xu, W.; Ou, Y.-N.; Qu, Y.; Ma, Y.-H.; Huang, Y.-Y.; Shen, X.-N.; Chen, S.-D.; Tan, L.; Zhao, Q.-H.; et al. Retinal biomarkers in Alzheimer’s disease and mild cognitive impairment: A systematic review and meta-analysis. Ageing Res. Rev. 2021, 69, 101361. [Google Scholar] [CrossRef]
- Gupta, V.B.; Chitranshi, N.; den Haan, J.; Mirzaei, M.; You, Y.; Lim, J.K.; Basavarajappa, D.; Godinez, A.; Di Angelantonio, S.; Sachdev, P.; et al. Retinal changes in Alzheimer’s disease-integrated prospects of imaging, functional and molecular advances. Prog. Retin. Eye Res. 2021, 82, 100899. [Google Scholar] [CrossRef]
- Bulut, M.; Kurtuluş, F.; Gözkaya, O.; Erol, M.K.; Cengiz, A.; Akıdan, M.; Yaman, A. Evaluation of optical coherence tomography angiographic findings in Alzheimer’s type dementia. Br. J. Ophthalmol. 2018, 102, 233–237. [Google Scholar] [CrossRef]
- Yoon, S.P.; Grewal, D.S.; Thompson, A.C.; Polascik, B.W.; Dunn, C.; Burke, J.R.; Fekrat, S. Retinal Microvascular and Neurodegenerative Changes in Alzheimer’s Disease and Mild Cognitive Impairment Compared with Control Participants. Ophthalmol. Retin. 2019, 3, 489–499. [Google Scholar] [CrossRef] [PubMed]
- Ko, F.; Muthy, Z.A.; Gallacher, J.; Sudlow, C.; Rees, G.; Yang, Q.; Keane, P.A.; Petzold, A.; Khaw, P.T.; Reisman, C.; et al. Association of Retinal Nerve Fiber Layer Thinning with Current and Future Cognitive Decline: A Study Using Optical Coherence Tomography. JAMA Neurol. 2018, 75, 1198–1205. [Google Scholar] [CrossRef]
- Almeida, A.L.M.; Pires, L.A.; Figueiredo, E.A.; Costa-Cunha, L.V.F.; Zacharias, L.C.; Preti, R.C.; Monteiro, M.L.R.; Cunha, L.P. Correlation between cognitive impairment and retinal neural loss assessed by swept-source optical coherence tomography in patients with mild cognitive impairment. Alzheimers Dement. 2019, 11, 659–669. [Google Scholar] [CrossRef]
- Cunha, L.P.; Lopes, L.C.; Costa-Cunha, L.V.F.; Costa, C.F.; Pires, L.A.; Almeida, A.L.M.; Monteiro, M.L.R. Macular Thickness Measurements with Frequency Domain-OCT for Quantification of Retinal Neural Loss and its Correlation with Cognitive Impairment in Alzheimer’s Disease. PLoS ONE 2016, 11, e0153830. [Google Scholar] [CrossRef] [Green Version]
- Den Haan, J.; van de Kreeke, J.A.; Konijnenberg, E.; ten Kate, M.; den Braber, A.; Barkhof, F.; van Berckel, B.N.; Teunissen, C.E.; Scheltens, P.; Visser, P.J.; et al. Retinal thickness as a potential biomarker in patients with amyloid-proven early- and late-onset Alzheimer’s disease. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2019, 11, 463–471. [Google Scholar]
- Den Haan, J.; Janssen, S.F.; van de Kreeke, J.A.; Scheltens, P.; Verbraak, F.D.; Bouwman, F.H. Retinal thickness correlates with parietal cortical atrophy in early-onset Alzheimer’s disease and controls. Alzheimers Dement. 2018, 10, 49–55. [Google Scholar]
- Mendez-Gomez, J.L.; Pelletier, A.; Rougier, M.-B.; Korobelnik, J.-F.; Schweitzer, C.; Delyfer, M.-N.; Catheline, G.; Monferme, S.; Dartigues, J.-F.; Delcourt, C.; et al. Association of Retinal Nerve Fiber Layer Thickness with Brain Alterations in the Visual and Limbic Networks in Elderly Adults without Dementia. JAMA Netw. Open 2018, 1, e184406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, Z.; Zheng, H.; Hu, J.; Jiang, L.; Cao, X.; Chen, Y.; Mei, X.; Li, C.; Shen, Y. Retinal Nerve Fiber Layer Thinning Is Associated with Brain Atrophy: A Longitudinal Study in Nondemented Older Adults. Front. Aging Neurosci. 2019, 11, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, Z.; Cao, X.; Hu, J.; Jiang, L.; Mei, X.; Zheng, H.; Chen, Y.; Wang, M.; Cao, J.; Li, W.; et al. Retinal nerve fiber layer thickness is associated with hippocampus and lingual gyrus volumes in nondemented older adults. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2020, 99, 109824. [Google Scholar] [CrossRef]
- Sergott, R.C.; Raji, A.; Kost, J.; Sur, C.; Jackson, S.; Locco, A.; Patel, A.; Furtek, C.; Mattson, B.; Egan, M.F. Retinal Optical Coherence Tomography Metrics Are Unchanged in Verubecestat Alzheimer’s Disease Clinical Trial but Correlate with Baseline Regional Brain Atrophy. J. Alzheimer’s Dis. 2021, 79, 275–287. [Google Scholar] [CrossRef]
- Galvin, J.E.; Kleiman, M.J.; Walker, M. Using Optical Coherence Tomography to Screen for Cognitive Impairment and Dementia. J. Alzheimer’s Dis. 2021, 84, 723–736. [Google Scholar] [CrossRef] [PubMed]
- Zhao, A.; Fang, F.; Li, B.; Chen, Y.; Qiu, Y.; Wu, Y.; Xu, W.; Deng, Y. Visual Abnormalities Associate with Hippocampus in Mild Cognitive Impairment and Early Alzheimer’s Disease. Front. Aging Neurosci. 2021, 12, 597491. [Google Scholar] [CrossRef] [PubMed]
- O’Shea, D.M.; de Wit, L.; Tanner, J.; Mejia Kurasz, A.; Amofa, P.; Perez Lao, A.; Levy, S.-A.; Chandler, M.; Smith, G. Hippocampal Subfields in Mild Cognitive Impairment: Associations with Objective and Informant-Report of Memory Function. Arch. Clin. Neuropsychol. Off. J. Natl. Acad. Neuropsychol. 2022, 37, 1502–1514. [Google Scholar] [CrossRef] [PubMed]
- Furcila, D.; Domínguez-Álvaro, M.; DeFelipe, J.; Alonso-Nanclares, L. Subregional Density of Neurons, Neurofibrillary Tangles and Amyloid Plaques in the Hippocampus of Patients with Alzheimer’s Disease. Front. Neuroanat. 2019, 13, 99. [Google Scholar] [CrossRef] [Green Version]
- Izzo, J.; Andreassen, O.A.; Westlye, L.T.; van der Meer, D. The association between hippocampal subfield volumes in mild cognitive impairment and conversion to Alzheimer’s disease. Brain Res. 2020, 1728, 146591. [Google Scholar] [CrossRef]
- Braak, H.; Del Tredici, K. From the Entorhinal Region via the Prosubiculum to the Dentate Fascia: Alzheimer Disease-Related Neurofibrillary Changes in the Temporal Allocortex. J. Neuropathol. Exp. Neurol. 2020, 79, 163–175. [Google Scholar] [CrossRef] [PubMed]
- Teipel, S.J.; Wegrzyn, M.; Meindl, T.; Frisoni, G.; Bokde, A.L.W.; Fellgiebel, A.; Filippi, M.; Hampel, H.; Klöppel, S.; Hauenstein, K.; et al. Anatomical MRI and DTI in the diagnosis of Alzheimer’s disease: A European multicenter study. J. Alzheimer’s Dis. JAD 2012, 31 (Suppl. 3), S33–S47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, S.; Ong, Y.-T.; Hilal, S.; Loke, Y.M.; Wong, T.Y.; Chen, C.L.-H.; Cheung, C.Y.; Zhou, J. The Association between Retinal Neuronal Layer and Brain Structure is Disrupted in Patients with Cognitive Impairment and Alzheimer’s Disease. J. Alzheimer’s Dis. JAD 2016, 54, 585–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mutlu, U.; Ikram, M.K.; Roshchupkin, G.V.; Bonnemaijer, P.W.M.; Colijn, J.M.; Vingerling, J.R.; Niessen, W.J.; Ikram, M.A.; Klaver, C.C.W.; Vernooij, M.W. Thinner retinal layers are associated with changes in the visual pathway: A population-based study. Hum. Brain Mapp. 2018, 39, 4290–4301. [Google Scholar] [CrossRef]
- Yu, J.; Li, J.; Huang, X. The Beijing version of the Montreal Cognitive Assessment as a brief screening tool for mild cognitive impairment: A community-based study. BMC Psychiatry 2012, 12, 156. [Google Scholar] [CrossRef] [Green Version]
- Morris, J.C. The Clinical Dementia Rating (CDR): Current version and scoring rules. Neurology 1993, 43, 2412–2414. [Google Scholar] [CrossRef]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Petersen, R.C.; Stevens, J.C.; Ganguli, M.; Tangalos, E.G.; Cummings, J.L.; DeKosky, S.T. Practice parameter: Early detection of dementia: Mild cognitive impairment (an evidence-based review). Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2001, 56, 1133–1142. [Google Scholar] [CrossRef] [Green Version]
- Iglesias, J.E.; Augustinack, J.C.; Nguyen, K.; Player, C.M.; Player, A.; Wright, M.; Roy, N.; Frosch, M.P.; McKee, A.C.; Wald, L.L.; et al. A computational atlas of the hippocampal formation using ex vivo, ultra-high resolution MRI: Application to adaptive segmentation of in vivo MRI. NeuroImage 2015, 115, 117–137. [Google Scholar] [CrossRef]
- Fischl, B.; Dale, A.M. Measuring the thickness of the human cerebral cortex from magnetic resonance images. Proc. Natl. Acad. Sci. USA 2000, 97, 11050–11055. [Google Scholar] [CrossRef] [Green Version]
- Kühn, S.; Musso, F.; Mobascher, A.; Warbrick, T.; Winterer, G.; Gallinat, J. Hippocampal subfields predict positive symptoms in schizophrenia: First evidence from brain morphometry. Transl. Psychiatry 2012, 2, e127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koch, K.; Reess, T.J.; Rus, O.G.; Zimmer, C. Extensive learning is associated with gray matter changes in the right hippocampus. NeuroImage 2016, 125, 627–632. [Google Scholar] [CrossRef] [PubMed]
- Sämann, P.G.; Iglesias, J.E.; Gutman, B.; Grotegerd, D.; Leenings, R.; Flint, C.; Dannlowski, U.; Clarke-Rubright, E.K.; Morey, R.A.; van Erp, T.G.M.; et al. FreeSurfer-based segmentation of hippocampal subfields: A review of methods and applications, with a novel quality control procedure for ENIGMA studies and other collaborative efforts. Hum. Brain Mapp. 2022, 43, 207–233. [Google Scholar] [CrossRef] [PubMed]
- Cui, Z.; Zhong, S.; Xu, P.; He, Y.; Gong, G. PANDA: A pipeline toolbox for analyzing brain diffusion images. Front. Hum. Neurosci. 2013, 7, 42. [Google Scholar] [CrossRef] [Green Version]
- Hua, K.; Zhang, J.; Wakana, S.; Jiang, H.; Li, X.; Reich, D.S.; Calabresi, P.A.; Pekar, J.J.; van Zijl, P.C.M.; Mori, S. Tract probability maps in stereotaxic spaces: Analyses of white matter anatomy and tract-specific quantification. NeuroImage 2008, 39, 336–347. [Google Scholar] [CrossRef] [Green Version]
- Meeter, L.H.; Kaat, L.D.; Rohrer, J.D.; van Swieten, J.C. Imaging and fluid biomarkers in frontotemporal dementia. Nat. Rev. Neurol. 2017, 13, 406–419. [Google Scholar] [CrossRef] [Green Version]
- Dalan, D.; Nandini, P.; Angayarkanni, N.; Kaviarasan, K.; Thanikachalam, S.; Das, U.N.; Ratra, D. Interchangeability of retinal perfusion indices in different-sized angiocubes: An optical coherence tomography angiography study in diabetic retinopathy. Indian J. Ophthalmol. 2020, 68, 484–489. [Google Scholar]
- Rosenfeld, P.J.; Durbin, M.K.; Roisman, L.; Zheng, F.; Miller, A.; Robbins, G.; Schaal, K.B.; Gregori, G. ZEISS Angioplex™ Spectral Domain Optical Coherence Tomography Angiography: Technical Aspects. Dev. Ophthalmol. 2016, 56, 18–29. [Google Scholar]
- O’Brien, L.M.; Ziegler, D.A.; Deutsch, C.K.; Frazier, J.A.; Herbert, M.R.; Locascio, J.J. Statistical adjustments for brain size in volumetric neuroimaging studies: Some practical implications in methods. Psychiatry Res. 2011, 193, 113–122. [Google Scholar] [CrossRef] [Green Version]
- Pellegrini, M.; Vagge, A.; Ferro Desideri, L.; Bernabei, F.; Triolo, G.; Mastropasqua, R.; Del Noce, C.; Borrelli, E.; Sacconi, R.; Iovino, C.; et al. Optical Coherence Tomography Angiography in Neurodegenerative Disorders. J. Clin. Med. 2020, 9, 1706. [Google Scholar] [CrossRef]
- Den Haan, J.; Verbraak, F.D.; Visser, P.J.; Bouwman, F.H. Retinal thickness in Alzheimer’s disease: A systematic review and meta-analysis. Alzheimers Dement. 2017, 6, 162–170. [Google Scholar]
- Zhao, W.; Wang, X.; Yin, C.; He, M.; Li, S.; Han, Y. Trajectories of the Hippocampal Subfields Atrophy in the Alzheimer’s Disease: A Structural Imaging Study. Front. Neuroinform. 2019, 13, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byun, M.S.; Park, S.W.; Lee, J.H.; Yi, D.; Jeon, S.Y.; Choi, H.J.; Joung, H.; Ghim, U.H.; Park, U.C.; Kim, Y.K.; et al. Association of Retinal Changes with Alzheimer Disease Neuroimaging Biomarkers in Cognitively Normal Individuals. JAMA Ophthalmol. 2021, 139, 548–556. [Google Scholar] [CrossRef]
- Toth, P.; Tarantini, S.; Csiszar, A.; Ungvari, Z. Functional vascular contributions to cognitive impairment and dementia: Mechanisms and consequences of cerebral autoregulatory dysfunction, endothelial impairment, and neurovascular uncoupling in aging. Am. J. Physiol. Heart Circ. Physiol. 2017, 312, H1–H20. [Google Scholar] [CrossRef] [Green Version]
- Kamagata, K.; Andica, C.; Kato, A.; Saito, Y.; Uchida, W.; Hatano, T.; Lukies, M.; Ogawa, T.; Takeshige-Amano, H.; Akashi, T.; et al. Diffusion Magnetic Resonance Imaging-Based Biomarkers for Neurodegenerative Diseases. Int. J. Mol. Sci. 2021, 22, 5216. [Google Scholar] [CrossRef]
- Alexander, A.L.; Lee, J.E.; Lazar, M.; Field, A.S. Diffusion tensor imaging of the brain. Neurother. J. Am. Soc. Exp. NeuroTher. 2007, 4, 316–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nowrangi, M.A.; Lyketsos, C.G.; Leoutsakos, J.-M.S.; Oishi, K.; Albert, M.; Mori, S.; Mielke, M.M. Longitudinal, region-specific course of diffusion tensor imaging measures in mild cognitive impairment and Alzheimer’s disease. Alzheimers Dement. 2013, 9, 519–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kantarci, K.; Murray, M.E.; Schwarz, C.G.; Reid, R.I.; Przybelski, S.A.; Lesnick, T.; Zuk, S.M.; Raman, M.R.; Senjem, M.L.; Gunter, J.L.; et al. White-matter integrity on DTI and the pathologic staging of Alzheimer’s disease. Neurobiol. Aging 2017, 56, 172–179. [Google Scholar] [CrossRef]
- Xie, S.; Xiao, J.X.; Wang, Y.H.; Wu, H.K.; Gong, G.L.; Jiang, X.X. Evaluation of bilateral cingulum with tractography in patients with Alzheimer’s disease. Neuroreport 2005, 16, 1275–1278. [Google Scholar] [CrossRef]
- Pievani, M.; Agosta, F.; Pagani, E.; Canu, E.; Sala, S.; Absinta, M.; Geroldi, C.; Ganzola, R.; Frisoni, G.B.; Filippi, M. Assessment of white matter tract damage in mild cognitive impairment and Alzheimer’s disease. Hum. Brain Mapp. 2010, 31, 1862–1875. [Google Scholar] [CrossRef]
- Jack, C.R.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Dunn, B.; Haeberlein, S.B.; Holtzman, D.M.; Jagust, W.; Jessen, F.; Karlawish, J.; et al. NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease. Alzheimers Dement. 2018, 14, 535–562. [Google Scholar] [CrossRef] [PubMed]
- Jack, C.R.; Knopman, D.S.; Jagust, W.J.; Petersen, R.C.; Weiner, M.W.; Aisen, P.S.; Shaw, L.M.; Vemuri, P.; Wiste, H.J.; Weigand, S.D.; et al. Tracking pathophysiological processes in Alzheimer’s disease: An updated hypothetical model of dynamic biomarkers. Lancet Neurol. 2013, 12, 207–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Items | CN (21) | CI (24) | F/T | p |
|---|---|---|---|---|
| Age, year | 61.43 ± 7.52 | 67 ± 7.83 | −2.49 | 0.016 * |
| Education, year | 13.95 ± 2.16 | 10.63 ± 2.5 | 4.92 | p < 0.001 *** |
| Gender, female/male | 14/7 | 17/8 | 0.009 | 0.924 |
| MMSE | 28.81 ± 1.17 | 24.5 ± 5.27 | −3.83 | p < 0.001 *** |
| MoCA | 26.95 ± 1.5 | 19 ± 4.95 | −5.74 | p < 0.001 *** |
| eTIV | 1,923,091.48 ± 145,178.78 | 1,987,143.36 ± 93,560.77 | −0.64 | 0.526 |
| HAMD | 4.33 ± 4.69 | 5.19 ± 4.92 | −0.55 | 0.58 |
| HAMA | 7.00 ± 6.89 | 7.76 ± 7.04 | −0.34 | 0.74 |
| Items | CN (21) | CI (27) | t | p-Value |
|---|---|---|---|---|
| Hippocampal_tail | 702.9 ± 61.72 | 663.69 ± 65.34 | 2.36 | 0.132 |
| subiculum | 539.8 ± 32.33 | 490.49 ± 53.87 | 6.99 | 0.012 * |
| CA1 | 744.04 ± 61.14 | 700 ± 62.6 | 3.06 | 0.088 |
| hippocampal-fissure | 235.78 ± 31.42 | 236.55 ± 35.79 | 0.4 | 0.532 |
| presubiculum | 385.86 ± 26.55 | 348.25 ± 37.25 | 6.4 | 0.015 * |
| parasubiculum | 71.91 ± 8.04 | 75.5 ± 10.77 | 2.13 | 0.152 |
| molecular_layer_HP | 685.99 ± 50.79 | 626.81 ± 70.51 | 4.88 | 0.033 * |
| GC-ML-DG | 362.08 ± 20.41 | 337.89 ± 37.77 | 4.36 | 0.043 * |
| CA3 | 251.61 ± 21.46 | 237 ± 29.88 | 1.98 | 0.167 |
| CA4 | 307.47 ± 14.48 | 293.5 ± 31.51 | 3.72 | 0.061 |
| fimbria | 89.75 ± 10.94 | 79.65 ± 16.77 | 2.5 | 0.122 |
| HATA | 69.16 ± 9.77 | 66.39 ± 11.32 | 0.006 | 0.941 |
| Whole_hippocampus | 4210.56 ± 256.59 | 3919.17 ± 358.11 | 4.86 | 0.033 * |
| eTIV (mm3) | 1,923,091.48 ± 145,178.78 | 1,987,143.36 ± 93,560.77 | −0.64 | 0.526 |
| Items | CN (21) | CI (25) | F | p-Value |
|---|---|---|---|---|
| CgH (MD) | 0.00073 ± 0.000046 | 0.00077 ± 0.000051 | 4.24 | 0.046 * |
| CgH (AxD) | 0.00115 ± 0.000062 | 0.00119 ± 0.000056 | 5.04 | 0.03 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, Z.; Wang, L.; Zhu, D.; Qin, R.; Sheng, X.; Ke, Z.; Shao, P.; Zhao, H.; Xu, Y.; Bai, F. Retinal Alterations as Potential Biomarkers of Structural Brain Changes in Alzheimer’s Disease Spectrum Patients. Brain Sci. 2023, 13, 460. https://doi.org/10.3390/brainsci13030460
Hu Z, Wang L, Zhu D, Qin R, Sheng X, Ke Z, Shao P, Zhao H, Xu Y, Bai F. Retinal Alterations as Potential Biomarkers of Structural Brain Changes in Alzheimer’s Disease Spectrum Patients. Brain Sciences. 2023; 13(3):460. https://doi.org/10.3390/brainsci13030460
Chicago/Turabian StyleHu, Zheqi, Lianlian Wang, Dandan Zhu, Ruomeng Qin, Xiaoning Sheng, Zhihong Ke, Pengfei Shao, Hui Zhao, Yun Xu, and Feng Bai. 2023. "Retinal Alterations as Potential Biomarkers of Structural Brain Changes in Alzheimer’s Disease Spectrum Patients" Brain Sciences 13, no. 3: 460. https://doi.org/10.3390/brainsci13030460