
Association between Antiepileptic Drugs and Incident Parkinson’s Disease among Patients Followed in German Primary Care Practices
 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Database
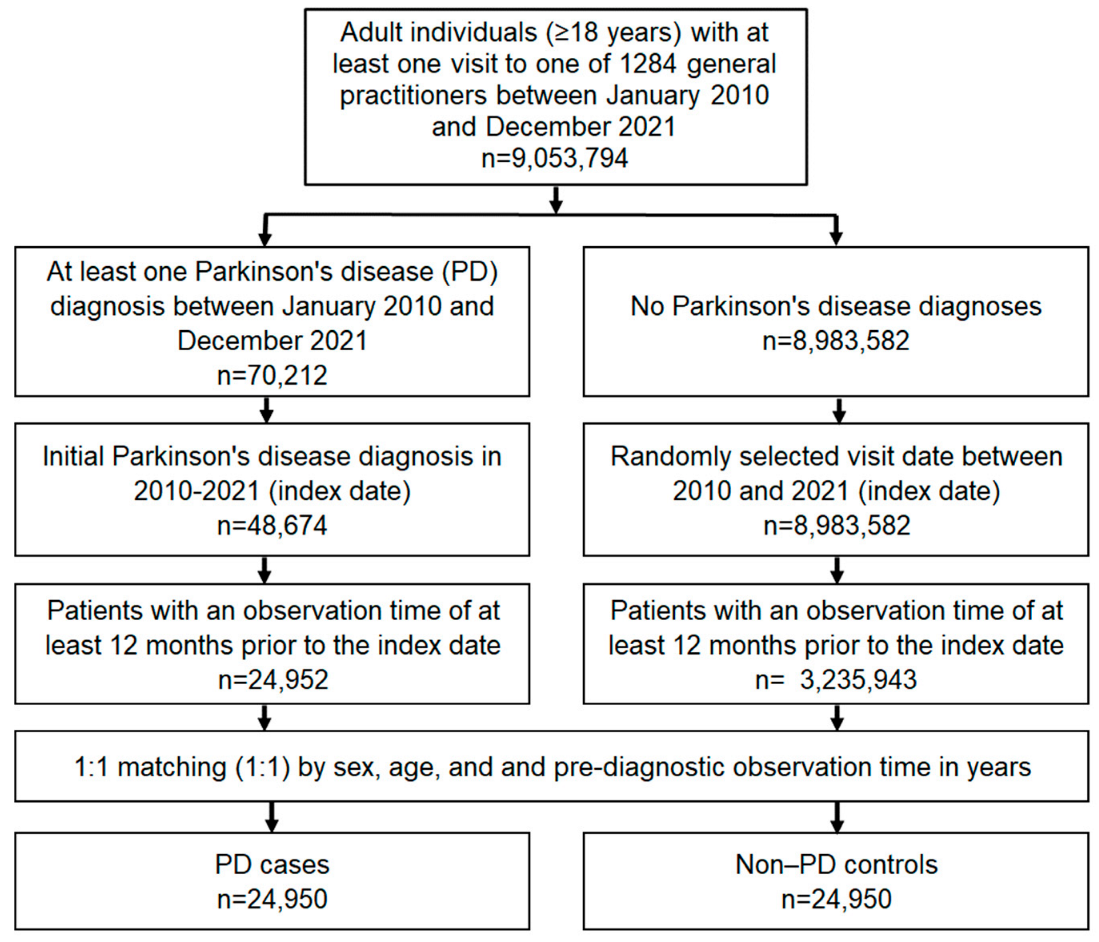
2.2. Study Population
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tysnes, O.B.; Storstein, A. Epidemiology of Parkinson’s disease. J. Neural. Transm. 2017, 124, 901–905. [Google Scholar] [CrossRef] [PubMed]
- Dorsey, E.R.; Sherer, T.; Okun, M.S.; Bloem, B.R. The Emerging Evidence of the Parkinson Pandemic. J. Park. Dis. 2018, 8 (Suppl. S1), S3–S8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heilbron, K.; Noyce, A.J.; Fontanillas, P.; Alipanahi, B.; Nalls, M.A.; Cannon, P.; 23andMe Research Team. The Parkinson’s phenome-traits associated with Parkinson’s disease in a broadly phenotyped cohort. NPJ Park. Dis. 2019, 5, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simonet, C.; Bestwick, J.; Jitlal, M.; Waters, S.; Ben-Joseph, A.; Marshall, C.; Dobson, R.; Marrium, S.; Robson, J.; Jacobs, B.; et al. Assessment of risk factors and early presentations of Parkinson disease in primary care in a diverse UK population. JAMA Neurol. 2022, 79, 359–369. [Google Scholar] [CrossRef] [PubMed]
- Belete, D.; Jacobs, B.M.; Simonet, C.; Bestwick, J.P.; Waters, S.; Marshall, C.R.; Dobson, R.; Noyce, A.J. Association Between Antiepileptic Drugs and Incident Parkinson Disease in the UK Biobank. JAMA Neurol. 2022, 80, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Rathmann, W.; Bongaerts, B.; Carius, H.J.; Kruppert, S.; Kostev, K. Basic characteristics and representativeness of the German Disease Analyzer database. Int. J. Clin. Pharmacol. Ther. 2018, 56, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Rajabally, Y.A.; Martey, J. Neuropathy in Parkinson disease: Prevalence and determinants. Neurology 2011, 77, 1947–1950. [Google Scholar] [CrossRef] [PubMed]
- Scholten, J.; Hamer, H.M.; Kostev, K. Usage of antiepileptic drugs in different diseases in Germany—A retrospective study. Epilepsy Behav. 2020, 111, 107210. [Google Scholar] [CrossRef] [PubMed]
- Brugger, F.; Bhatia, K.P.; Besag, F.M. Valproate-Associated Parkinsonism: A Critical Review of the Literature. CNS Drugs 2016, 30, 527–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahmoud, F.; Tampi, R.R. Valproic acid-induced parkinsonism in the elderly: A comprehensive review of the literature. Am. J. Geriatr. Pharm. 2011, 9, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Pacheco-Paez, T.; Montastruc, F.; Rousseau, V.; Chebane, L.; Lapeyre-Mestre, M.; Renoux, C.; Montastruc, J.L. Parkinsonism associated with gabapentinoid drugs: A pharmacoepidemiologic study. Mov. Disord. 2020, 35, 176–180. [Google Scholar] [CrossRef] [PubMed]
- Rissardo, J.P.; Fornari Caprara, A.L. Lamotrigine-Associated Movement Disorder: A Literature Review. Neurol. India 2021, 69, 1524–1538. [Google Scholar] [CrossRef] [PubMed]
- Sáenz-Farret, M.; Tijssen, M.A.J.; Eliashiv, D.; Fisher, R.S.; Sethi, K.; Fasano, A. Antiseizure Drugs and Movement Disorders. CNS Drugs 2022, 36, 859–876, Erratum in CNS Drugs 2022, 36, 859–876. [Google Scholar] [CrossRef] [PubMed]
- Stathis, P.; Konitsiotis, S.; Tagaris, G.; Peterson, D. VALID-PD Study Group. Levetiracetam for the management of levodopa-induced dyskinesias in Parkinson’s disease. Mov. Disord. 2011, 26, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Borreguero, D.; Odin, P.; Serrano, C. Restless legs syndrome and PD: A review of the evidence for a possible association. Neurology 2003, 61 (Suppl. S3), S49–S55. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Navarro, H.; García-Martín, E.; Agúndez, J.A.G.; Jiménez-Jiménez, F.J. Association between restless legs syndrome and other movement disorders. Neurology 2019, 92, 948–964. [Google Scholar] [CrossRef] [PubMed]
- Schrag, A.; Bohlken, J.; Dammertz, L.; Teipel, S.; Hermann, W.; Akmatov, M.K.; Bätzing, J.; Holstiege, J. Widening the Spectrum of Risk Factors, Comorbidities, and Prodromal Features of Parkinson Disease. JAMA Neurol. 2023, 80, 161–171. [Google Scholar] [CrossRef] [PubMed]
- Paul, D.A.; Qureshi, A.R.M.; Rana, A.Q. Peripheral neuropathy in Parkinson’s disease. Neurol. Sci. 2020, 41, 2691–2701. [Google Scholar] [CrossRef] [PubMed]
- Zis, P.; Grünewald, R.A.; Chaudhuri, R.K.; Hadjivassiliou, M. Peripheral neuropathy in idiopathic Parkinson’s disease: A systematic review. J. Neurol. Sci. 2017, 378, 204–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variable | PD Cases (n = 24,950) | Non-PD Controls (n = 24,950) | p-Value 1 |
|---|---|---|---|
| Mean age (standard deviation) | 75.2 (10.5) | 75.2 (10.5) | 1.000 |
| Age ≤ 60 (%) | 9.3 | 9.3 | 1.000 |
| Age 61–70 (%) | 15.7 | 15.7 | |
| Age 71–80 (%) | 41.7 | 41.7 | |
| Age > 80 (%) | 33.3 | 33.3 | |
| Female (%) | 47.3 | 47.3 | 1.000 |
| Male (%) | 52.7 | 52.7 | |
| Pre-diagnostic observation time in years, mean (standard deviation) | 7.8 (5.0) | 7.8 (5.0) | 1.000 |
| AED Drug | Cases (%) | Controls (%) | COR for PD (95% CI) | p-Value | AOR for PD (95% CI) | p-Value |
|---|---|---|---|---|---|---|
| Any AED | 12.1 | 6.5 | 2.00 (1.87–2.13) | <0.001 | 1.43 (1.33–1.53) | <0.001 |
| Gabapentin | 4.3 | 2.2 | 1.96 (1.76–2.17) | <0.001 | 1.36 (1.22–1.52) | <0.001 |
| Pregabalin | 5.2 | 2.9 | 1.87 (1.70–2.04) | <0.001 | 1.28 (1.15–1.41) | <0.001 |
| Carbamazepine | 1.3 | 0.9 | 1.46 (1.23–1.83) | <0.001 | 0.88 (0.73–1.06) | 0.169 |
| Sodium valproate | 1.2 | 0.3 | 3.78 (2.95–4.85) | <0.001 | 2.39 (1.84–311) | <0.001 |
| Levetiracetam | 1.1 | 0.6 | 1.79 (1.46–2.19) | <0.001 | 1.03 (0.83–1.29) | 0.803 |
| Lamotrigine | 0.4 | 0.2 | 1.89 (1.35–2.64) | <0.001 | 1.05 (0.73–1.50) | 0.804 |
| Epilepsy | 4.2 | 1.8 | 2.39 (1.14–2.67) | <0.001 | 1.91 (1.69–2.15) | <0.001 |
| Restless legs syndrome | 7.2 | 2.1 | 3.62 (3.28–4.00) | <0.001 | 3.02 (2.73–3.34) | <0.001 |
| Neuropathy | 14.2 | 8.2 | 1.84 (1.74–1.95) | <0.001 | 1.53 (1.44–1.62) | <0.001 |
| AED Drug | AEDs Prescribed at Least 12 Months Prior to Index Date | AEDs Prescribed at Least 36 Months Prior to Index Date | ||
|---|---|---|---|---|
| AOR for PD (95% CI) | p-Value | AOR for PD (95% CI) | p-Value | |
| Any AED | 1.50 (1.39–1.62) | <0.001 | 1.43 (1.26–1.63) | <0.001 |
| Gabapentin | 1.40 (1.24–1.60) | <0.001 | 1.41 (1.14–1.74) | 0.002 |
| Pregabalin | 1.49 (1.33–1.67) | <0.001 | 1.98 (1.54–2.53) | <0.001 |
| Carbamazepine | 0.89 (0.73–1.07) | 0.214 | 0.80 (0.62–1.03) | 0.082 |
| Sodium valproate | 2.14 (1.60–2.87) | <0.001 | 1.11 (0.70–1.75) | 0.663 |
| Levetiracetam | 0.92 (0.70–1.20) | 0.530 | 2.00 (0.80–4.96) | 0.137 |
| Lamotrigine | 1.33 (0.87–2.03) | 0.196 | 1.21 (0.51–2.86) | 0.668 |
| Epilepsy | 1.99 (1.77–2.23) | <0.001 | 2.21 (1.97–2.47) | <0.001 |
| Restless legs syndrome | 3.20 (2.90–3.54) | <0.001 | 3.27 (2.96–3.62) | <0.001 |
| Neuropathy | 1.58 (1.49–1.68) | <0.001 | 1.65 (1.55–1.75) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kostev, K.; Doege, C.; Jacob, L.; Smith, L.; Koyanagi, A.; Gollop, C.; Schrag, A. Association between Antiepileptic Drugs and Incident Parkinson’s Disease among Patients Followed in German Primary Care Practices. Brain Sci. 2023, 13, 450. https://doi.org/10.3390/brainsci13030450
Kostev K, Doege C, Jacob L, Smith L, Koyanagi A, Gollop C, Schrag A. Association between Antiepileptic Drugs and Incident Parkinson’s Disease among Patients Followed in German Primary Care Practices. Brain Sciences. 2023; 13(3):450. https://doi.org/10.3390/brainsci13030450
Chicago/Turabian StyleKostev, Karel, Corinna Doege, Louis Jacob, Lee Smith, Ai Koyanagi, Celina Gollop, and Anette Schrag. 2023. "Association between Antiepileptic Drugs and Incident Parkinson’s Disease among Patients Followed in German Primary Care Practices" Brain Sciences 13, no. 3: 450. https://doi.org/10.3390/brainsci13030450