
“Pandemic Fatigue” in South America: A Multi-Center Report from Argentina, Bolivia, Paraguay, Peru, and Uruguay

 , ,
, ,  ,
,  ,
,
Abstract
:1. Introduction
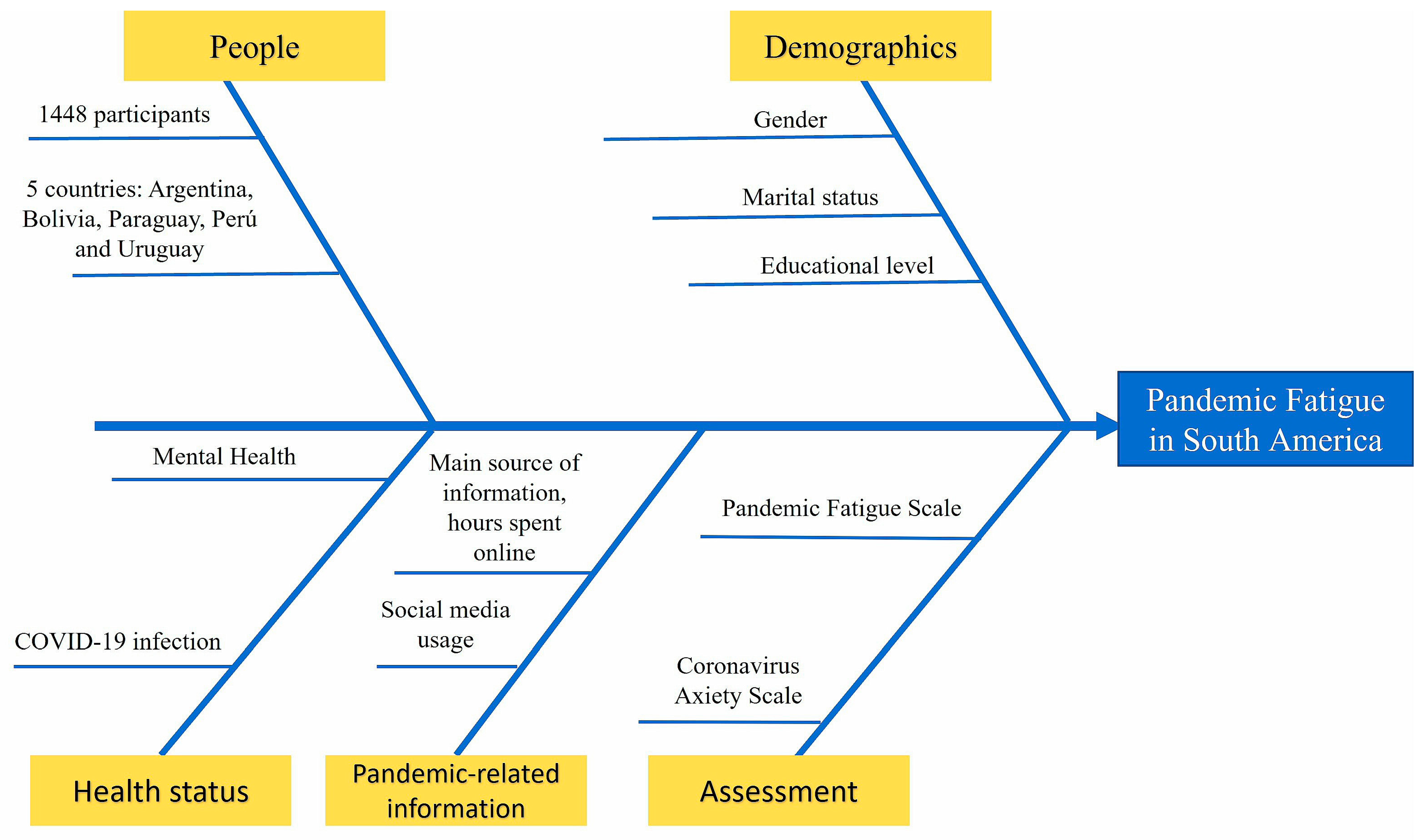
2. Methods
2.1. Study Design
2.2. Assessment Tools
2.3. Ethical Considerations
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions and Final Remarks
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Torales, J.; Ríos-González, C.; Barrios, I.; O’Higgins, M.; González, I.; García, O.; Castaldelli-Maia, J.M.; Ventriglio, A. Self-Perceived Stress During the Quarantine of COVID-19 Pandemic in Paraguay: An Exploratory Survey. Front. Psychiatry 2020, 11, 558691. [Google Scholar] [CrossRef] [PubMed]
- Boadle, A. WHO Says the Americas Are New COVID-19 Epicenter as Deaths Surge in Latin America. Healthcare & Pharma News, 26 May 2020. [Google Scholar]
- Garcia, P.J.; Alarcón, A.; Bayer, A.; Buss, P.; Guerra, G.; Ribeiro, H.; Rojas, K.; Saenz, R.; Salgado de Snyder, N.; Solimano, G.; et al. COVID-19 Response in Latin America. Am. J. Trop. Med. Hyg. 2020, 103, 1765–1772. [Google Scholar] [CrossRef]
- NICE Overview|COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19|Guidance|NICE. Available online: https://www.nice.org.uk/guidance/ng188 (accessed on 27 January 2023).
- NIH. NIH Launches New Initiative to Study “Long COVID”; National Institutes of Health: Bethesda, MD, USA, 2021. [Google Scholar]
- World Health Organization. Mental Health and COVID-19: Early Evidence of the Pandemic’s Impact. Available online: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-Sci_Brief-Mental_health-2022.1 (accessed on 14 February 2023).
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The Psychological Impact of Quarantine and How to Reduce It: Rapid Review of the Evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- The British Academy. The COVID Decade: Understanding the Long-Term Societal Impacts of COVID-19; The British Academy: London, UK, 2021. [Google Scholar]
- Chew, Q.H.; Wei, K.C.; Vasoo, S.; Chua, H.C.; Sim, K. Narrative Synthesis of Psychological and Coping Responses towards Emerging Infectious Disease Outbreaks in the General Population: Practical Considerations for the COVID-19 Pandemic. Singap. Med. J. 2020, 61, 350–356. [Google Scholar] [CrossRef]
- Kumar, A.; Nayar, K.R. COVID 19 and Its Mental Health Consequences. J. Ment. Health 2021, 30, 1–2. [Google Scholar] [CrossRef]
- Barrios, I.; Ríos-González, C.; O’Higgins, M.; González-Urbieta, I.; García, O.; Almirón-Santacruz, J.; Navarro, R.; Melgarejo, O.; Ruiz Díaz, N.; Castaldelli-Maia, J.M.; et al. Psychometric Properties of the Spanish Version of the Fear of COVID-19 Scale in Paraguayan Population. Ir. J. Psychol. Med. 2021, 38, 266–271. [Google Scholar] [CrossRef] [PubMed]
- Shevlin, M.; Nolan, E.; Owczarek, M.; McBride, O.; Murphy, J.; Gibson Miller, J.; Hartman, T.K.; Levita, L.; Mason, L.; Martinez, A.P.; et al. COVID-19-Related Anxiety Predicts Somatic Symptoms in the UK Population. Br. J. Health Psychol. 2020, 25, 875–882. [Google Scholar] [CrossRef]
- Arora, A.; Jha, A.K.; Alat, P.; Das, S.S. Understanding Coronaphobia. Asian J. Psychiatr. 2020, 54, 102384. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.; Rachor, G.S.; Asmundson, G.J.G. Who Develops Pandemic Fatigue? Insights from Latent Class Analysis. PLoS ONE 2022, 17, e0276791. [Google Scholar] [CrossRef]
- World Health Organization. Pandemic Fatigue: Reinvigorating the Public to Prevent COVID-19: Policy Framework for Supporting Pandemic Prevention and Management: Revised Version November 2020; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2020. [Google Scholar]
- Masten, A.S.; Cicchetti, D. Resilience in Development: Progress and Transformation. In Developmental Psychopathology; Cicchetti, D., Ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2016; pp. 1–63. ISBN 978-1-119-12555-6. [Google Scholar]
- Sandler, C.X.; Wyller, V.B.B.; Moss-Morris, R.; Buchwald, D.; Crawley, E.; Hautvast, J.; Katz, B.Z.; Knoop, H.; Little, P.; Taylor, R.; et al. Long COVID and Post-Infective Fatigue Syndrome: A Review. Open Forum Infect. Dis. 2021, 8, ofab440. [Google Scholar] [CrossRef] [PubMed]
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: Major Findings, Mechanisms and Recommendations. Nat. Rev. Microbiol. 2023, 21, 133–146. [Google Scholar] [CrossRef]
- Cuadrado, E.; Maldonado, M.A.; Tabernero, C.; Arenas, A.; Castillo-Mayén, R.; Luque, B. Construction and Validation of a Brief Pandemic Fatigue Scale in the Context of the Coronavirus-19 Public Health Crisis. Int. J. Public Health 2021, 66, 1604260. [Google Scholar] [CrossRef]
- Lee, S.A. Coronavirus Anxiety Scale: A Brief Mental Health Screener for COVID-19 Related Anxiety. Death Stud. 2020, 44, 393–401. [Google Scholar] [CrossRef] [Green Version]
- Caycho-Rodríguez, T.; Vilca, L.W.; Peña-Calero, B.N.; Barboza-Palomino, M.; White, M.; Reyes-Bossio, M. Measurement of Coronaphobia in Older Adults: Validation of the Spanish Version of the Coronavirus Anxiety Scale. Rev. Esp. Geriatr. Gerontol. 2022, 57, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Caycho-Rodríguez, T.; Vilca, L.W.; Carbajal-León, C.; White, M.; Vivanco-Vidal, A.; Saroli-Araníbar, D.; Peña-Calero, B.N.; Moreta-Herrera, R. Coronavirus Anxiety Scale: New Psychometric Evidence for the Spanish Version Based on CFA and IRT Models in a Peruvian Sample. Death Stud. 2022, 46, 1090–1099. [Google Scholar] [CrossRef]
- Habersaat, K.B.; Betsch, C.; Danchin, M.; Sunstein, C.R.; Böhm, R.; Falk, A.; Brewer, N.T.; Omer, S.B.; Scherzer, M.; Sah, S.; et al. Ten Considerations for Effectively Managing the COVID-19 Transition. Nat. Hum. Behav. 2020, 4, 677–687. [Google Scholar] [CrossRef]
- Hassanien, N.S.; Adawi, A.M.; Alzahrani, T.A.; Adawi, E.A. The Mediating Role of Resilience and Electronic Health Literacy in the Relationship Between Pandemic Fatigue and Adherence to Preventive Behaviours Against COVID-19. Cureus 2022, 14, e29553. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Blazquez, C.; Romay-Barja, M.; Falcon, M.; Ayala, A.; Forjaz, M.J. Psychometric Properties of the COVID-19 Pandemic Fatigue Scale: Cross-Sectional Online Survey Study. JMIR Public Health Surveill. 2022, 8, e34675. [Google Scholar] [CrossRef]
- Dos Santos, G.B.; Beleza, A.C.S.; Sato, T.D.O.; Carvalho, C.; Serrão, P.R.M.D.S. Fatigue, Sleep Quality and Mental Health Symptoms in Brazilian Women during the COVID-19 Pandemic: Longitudinal Study. Sci. Rep. 2022, 12, 20346. [Google Scholar] [CrossRef] [PubMed]
- Labrague, L.J.; Ballad, C.A. Lockdown Fatigue among College Students during the COVID-19 Pandemic: Predictive Role of Personal Resilience, Coping Behaviors, and Health. Perspect. Psychiatr. Care 2021, 57, 1905–1912. [Google Scholar] [CrossRef] [PubMed]
- Vindegaard, N.; Benros, M.E. COVID-19 Pandemic and Mental Health Consequences: Systematic Review of the Current Evidence. Brain Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef] [PubMed]
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A. The Outbreak of COVID-19 Coronavirus and Its Impact on Global Mental Health. Int. J. Soc. Psychiatry 2020, 66, 317–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.J.; Meeker, T.J.; Tulloch, I.K.; Mullins, J.; Park, J.-H.; Bae, S.H. Pandemic Fatigue and Anxiety Sensitivity as Associated Factors with Posttraumatic Stress Symptoms among University Students in South Korea during the Prolonged COVID-19 Pandemic. Int. J. Public Health 2022, 67, 1604552. [Google Scholar] [CrossRef]
- Serafini, G.; Parmigiani, B.; Amerio, A.; Aguglia, A.; Sher, L.; Amore, M. The Psychological Impact of COVID-19 on the Mental Health in the General Population. QJM 2020, 113, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Cleofas, J.V.; Oducado, R.M.F. COVID-19 Death Occurrences, Pandemic Fatigue, and Well-Being. J. Loss Trauma 2022, 27, 679–682. [Google Scholar] [CrossRef]
- Krakowczyk, J.B.; Planert, J.; Skoda, E.-M.; Dinse, H.; Kaup, T.; Teufel, M.; Bäuerle, A. Pandemic Fatigue, Psychopathological Risk Factors, and Vaccination Attitudes during the COVID-19 Pandemic in 2021–a Network Analysis. J. Affect. Disord. Rep. 2022, 8, 100345. [Google Scholar] [CrossRef]
- Labrague, L.J. Pandemic Fatigue and Clinical Nurses’ Mental Health, Sleep Quality and Job Contentment during the COVID-19 Pandemic: The Mediating Role of Resilience. J. Nurs. Manag. 2021, 29, 1992–2001. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Yu, W.; Cao, X. Experience Pandemic Fatigue? Social Media Use May Play a Role: Testing a Model of Pandemic Fatigue Development from a Social Media Perspective. Health Commun. 2022, 1–11. [Google Scholar] [CrossRef]
- Torales, J.; Barrios, I.; O’Higgins, M.; Almirón-Santacruz, J.; Gonzalez-Urbieta, I.; García, O.; Rios-González, C.; Castaldelli-Maia, J.M.; Ventriglio, A. COVID-19 Infodemic and Depressive Symptoms: The Impact of the Exposure to News about COVID-19 on the General Paraguayan Population. J. Affect. Disord. 2022, 298, 599–603. [Google Scholar] [CrossRef]
- Moore, D.; Tarnai, J. Evaluating Nonresponsenerror in Mail Surveys. In Survey Nonresponse; Groves, R., Dillman, D., Eltinge, J., Little, R., Eds.; John Wiley & Sons: New York, NY, USA, 2002; pp. 197–211. [Google Scholar]
- Ceban, F.; Ling, S.; Lui, L.M.W.; Lee, Y.; Gill, H.; Teopiz, K.M.; Rodrigues, N.B.; Subramaniapillai, M.; Di Vincenzo, J.D.; Cao, B.; et al. Fatigue and cognitive impairment in Post-COVID-19 Syndrome: A systematic review and meta-analysis. Brain Behav. Immun. 2022, 101, 93–135. [Google Scholar] [CrossRef]
- Xin, L.; Wang, L.; Cao, X.; Tian, Y.; Yang, Y.; Wang, K.; Kang, Z.; Zhao, M.; Feng, C.; Wang, X.; et al. Prevalence and Influencing Factors of Pandemic Fatigue among Chinese Public in Xi’an City during COVID-19 New Normal: A Cross-Sectional Study. Front. Public Health 2022, 10, 971115. [Google Scholar] [CrossRef] [PubMed]
- Koçak, O.; Koçak, Ö.E.; Younis, M.Z. The Psychological Consequences of COVID-19 Fear and the Moderator Effects of Individuals’ Underlying Illness and Witnessing Infected Friends and Family. Int. J. Environ. Res. Public Health 2021, 18, 1836. [Google Scholar] [CrossRef] [PubMed]
- Warriner, K.; Goyder, J.; Miller, S. Evaluating Socio-Economic Status (SES) Bias in Survey Nonresponse. J. Off. Stat. 2002, 18, 1–11. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | n | % | Mean | SD | SE | p-Value |
|---|---|---|---|---|---|---|
| Country Argentina Bolivia Uruguay Peru Paraguay Gender Female Male Non-binary I prefer not to say Marital status Partnered—married Separated—divorced Single Widowed Education Primary education Secondary education University education Previous infection by COVID-19 Not I don’t know Yes Loss of a relative or close friend during the pandemic Yes Not Vaccination I have not been vaccinated Yes, two doses Yes, two doses plus two boosters Yes, two doses plus one booster Yes, one dose Diagnosed with a mental disorder Not Yes Currently under care of mental health professionals Not Yes Regularly on psychotropic treatments Not Yes | 295 294 279 277 303 1048 386 6 8 645 71 717 15 2 142 1304 266 145 1037 859 589 23 229 284 897 15 1149 299 1097 351 1286 162 | 20.4 20.3 19.3 19.1 20.9 72.4 26.7 0.4 0.6 44.5 4.9 49.5 1.0 0.1 9.8 90.1 18.4 10.0 71.6 59.3 40.7 1.6 15.8 19.6 61.9 1.0 79.4 20.6 75.8 24.2 88.8 11.2 | 21.62 21.89 21.14 22.60 21.47 21.62 21.99 22.00 24.38 21.56 19.52 22.11 22.07 17.50 20.99 21.83 20.53 22.24 21.98 22.54 21.18 26.65 23.33 20.75 21.51 22.00 21.55 22.46 21.56 22.29 21.68 22.16 | 7.77 7.95 8.01 8.15 7.85 7.74 8.42 12.92 8.25 7.88 7.98 7.95 9.15 3.54 8.86 7.84 8.09 8.16 7.86 7.79 8.01 8.85 8.24 8.62 7.50 9.52 7.95 7.91 7.97 7.87 7.92 8.14 | 0.45 0.46 0.48 0.49 0.45 0.24 0.43 5.27 2.92 0.31 0.95 0.29 2.36 2.50 0.74 0.22 0.50 0.68 0.24 0.32 0.27 1.84 0.54 0.51 0.25 2.46 0.23 0.46 0.24 0.42 0.22 0.64 | 0.255 0.681 0.06 0.369 0.021 0.001 <0.001 0.078 0.134 0.472 |
| Characteristics | n | % | Mean | SD | SE | p-Value |
|---|---|---|---|---|---|---|
| Major source of stress Money Study None Intimate/Family Relationships Work Housing Hours spent in information 1 to 3 h per day 4 to 6 h per day 7 to 8 h per day More than 8 h per day Main source of information Newspapers Radio Social media Scientific journals TV Social media Tik-Tok Main source of information Friends Coworkers Family Health/government agencies | 418 204 75 266 451 34 1251 121 28 48 65 43 1022 97 221 240 107 19 656 107 91 161 1089 | 28.9 14.1 5.2 18.4 31.1 23 86.4 8.4 1.9 3.3 4.5 3.0 70.6 6.7 15.3 23.48 10.47 1.86 64.19 7.4 6.3 11.1 75.2 | 21.85 21.80 19.95 22.60 21.42 21.35 21.75 20.65 22.11 24.02 19.92 19.95 22.21 19.77 21.29 21.39 23.50 18.26 22.42 23.84 22.84 23.02 21.25 | 8.32 7.97 7.36 7.65 7.95 5.91 7.92 8.24 7.21 8.07 6.37 7.06 7.86 8.50 8.45 7.68 8.28 5.14 7.87 8.81 7.91 7.71 7.84 | 0.41 0.56 0.85 0.47 0.37 1.01 0.22 0.75 1.36 1.16 0.79 1.08 0.25 0.86 0.57 0.50 0.80 1.18 0.31 0.85 0.83 0.61 0.24 | 0.166 0.099 0.003 <0.001 0.001 |
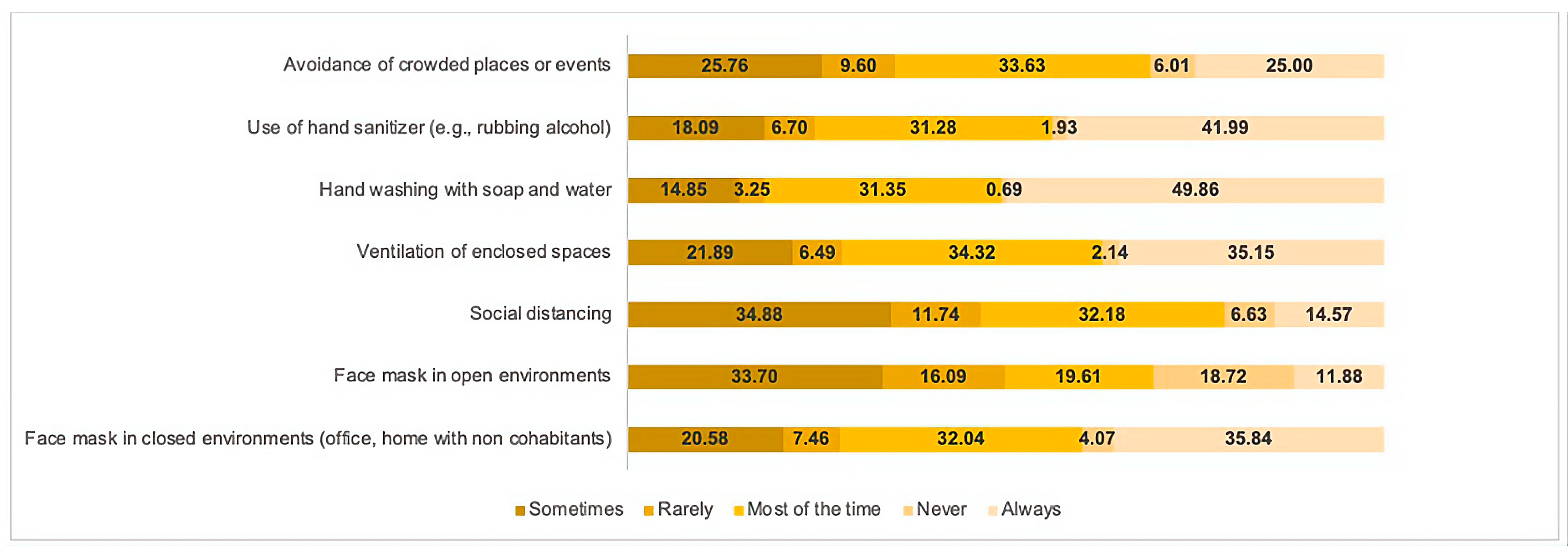
| Protective Measures | Mean | SD | SE | p-Value |
|---|---|---|---|---|
| Face mask in closed environments Sometimes Rarely Most of the time Never Always Face mask in open environments Sometimes Rarely Most of the time Never Always Social distancing Sometimes Rarely Most of the time Never Always Ventilation of enclosed spaces Sometimes Rarely Most of the time Never Always Hand washing Sometimes Rarely Most of the time Never Always Use of hand sanitizer Sometimes Rarely Most of the time Never Always Avoidance of crowded places or events Sometimes Rarely Most of the time Never Always | 24.57 25.93 21.27 28.39 18.90 21.61 22.81 18.82 26.25 18.34 22.12 24.80 20.32 27.44 18.90 23.91 23.28 21.35 29.00 20.04 23.81 24.68 22.46 26.20 20.41 23.54 24.91 21.84 27.57 20.11 23.13 24.06 20.44 28.33 19.56 | 7.82 8.42 6.98 7.60 7.42 7.60 7.24 6.63 8.09 7.94 7.77 7.35 7.10 8.89 8.02 8.04 6.99 7.37 8.06 8.01 8.35 7.47 7.72 7.24 7.76 8.08 6.95 7.46 9.14 7.90 7.50 7.38 7.24 8.25 8.12 | 0.45 0.81 0.32 0.99 0.32 0.34 0.47 0.39 0.49 0.61 0.35 0.56 0.33 0.91 0.55 0.45 0.72 0.33 1.45 0.36 0.57 1.09 0.36 2.29 0.29 0.50 0.71 0.35 1.73 0.32 0.39 0.63 0.33 0.88 0.43 | <0.001 <0.001 <0.001 <0.001 <0.001 <0.001 <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Torales, J.; González-Urbieta, I.; Barrios, I.; Waisman-Campos, M.; Terrazas-Landivar, A.; Viola, L.; Caycho-Rodríguez, T.; Melgarejo, O.; Navarro, R.; García, O.; et al. “Pandemic Fatigue” in South America: A Multi-Center Report from Argentina, Bolivia, Paraguay, Peru, and Uruguay. Brain Sci. 2023, 13, 444. https://doi.org/10.3390/brainsci13030444
Torales J, González-Urbieta I, Barrios I, Waisman-Campos M, Terrazas-Landivar A, Viola L, Caycho-Rodríguez T, Melgarejo O, Navarro R, García O, et al. “Pandemic Fatigue” in South America: A Multi-Center Report from Argentina, Bolivia, Paraguay, Peru, and Uruguay. Brain Sciences. 2023; 13(3):444. https://doi.org/10.3390/brainsci13030444
Chicago/Turabian StyleTorales, Julio, Israel González-Urbieta, Iván Barrios, Marcela Waisman-Campos, Alexandra Terrazas-Landivar, Laura Viola, Tomás Caycho-Rodríguez, Osvaldo Melgarejo, Rodrigo Navarro, Oscar García, and et al. 2023. "“Pandemic Fatigue” in South America: A Multi-Center Report from Argentina, Bolivia, Paraguay, Peru, and Uruguay" Brain Sciences 13, no. 3: 444. https://doi.org/10.3390/brainsci13030444