
Executive Profile of the Logopenic Variant of Primary Progressive Aphasia: Comparison with the Semantic and Non-Fluent Variants and Alzheimer’s Disease

 , ,
, ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Population
2.2. Methods
3. Results
3.1. Demographic Data Comparison
3.2. Group Comparison to Controls
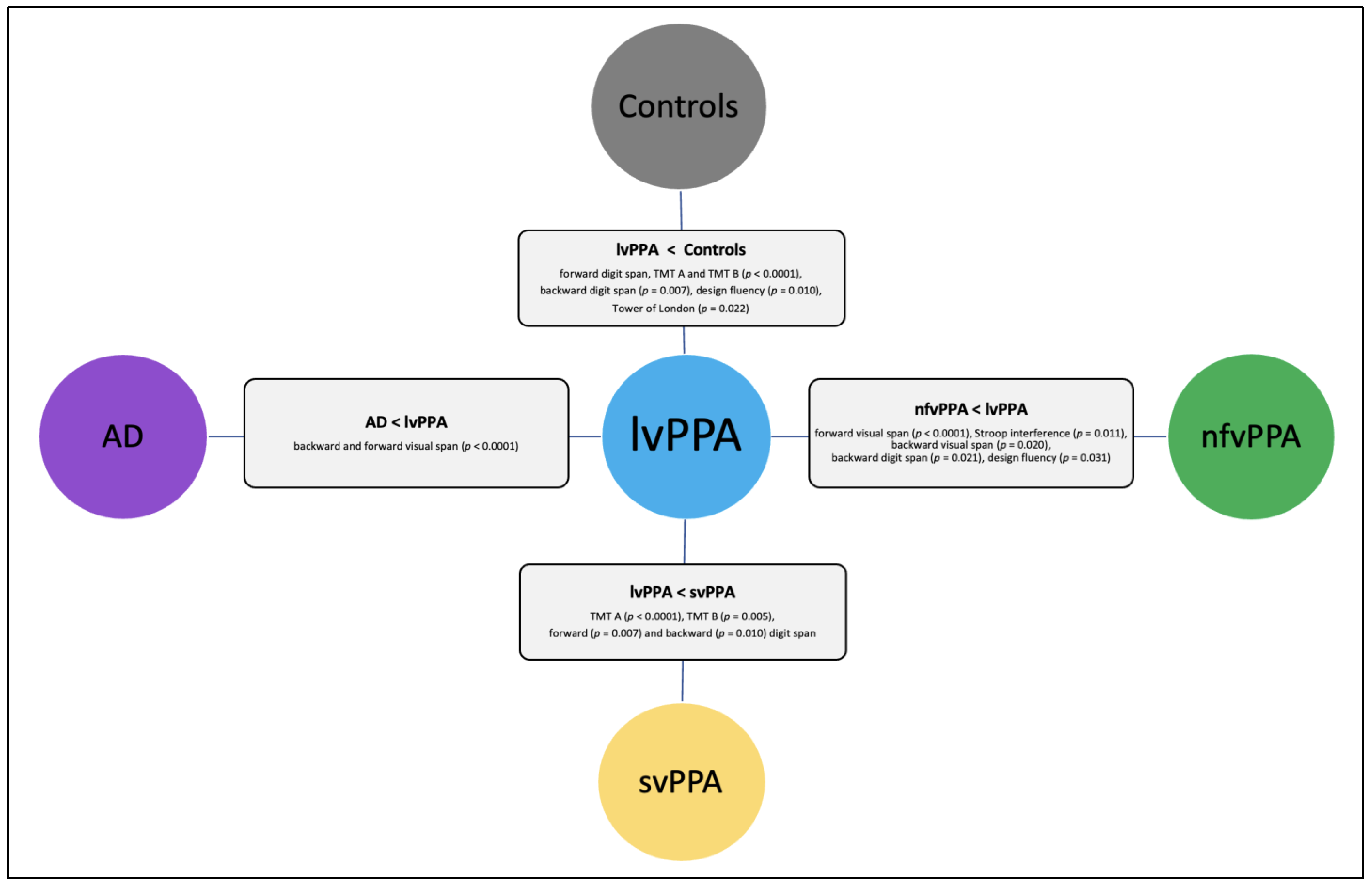
3.3. Clinical Groups Comparisons
4. Discussion
4.1. lvPPA and Control Groups
4.2. nfvPPA and Control Groups
4.3. svPPA and Control Groups
4.4. AD and Control Groups
4.5. lvPPA and nfvPPA Groups
4.6. lvPPA and svPPA Groups
4.7. lvPPA and AD Groups
4.8. Other Between-Group Differences
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pick, A. Über die Beziehungen der senilen Hirnatrophie zur Aphasie. Prag. Med. Wochenschr. 1892, 17, 165–167. [Google Scholar]
- Mesulam, M.-M. Slowly progressive aphasia without generalized dementia. Ann. Neurol. 1982, 11, 592–598. [Google Scholar] [CrossRef] [PubMed]
- Gorno-Tempini, M.L.; Hillis, A.E.; Weintraub, S.; Kertesz, A.; Mendez, M.; Cappa, S.F.; Ogar, J.M.; Rohrer, J.D.; Black, S.; Boeve, B.F.; et al. Classification of primary progressive aphasia and its variants. Neurology 2011, 2, 1006–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mesulam, M. Primary progressive aphasia. Ann. Neurol. 2001, 49, 425–432. [Google Scholar] [CrossRef]
- Mesulam, M.-M.; Coventry, C.; Bigio, E.H.; Geula, C.; Thompson, C.; Bonakdarpour, B.; Gefen, T.; Rogalski, E.J.; Weintraub, S. Nosology of primary progressive aphasia and the neuropathology of language. Adv. Exp. Med. Biol. 2021, 1281, 33–49. [Google Scholar]
- Leyton, C.E.; Villemagne, V.L.; Savage, S.; Pike, K.E.; Ballard, K.J.; Piguet, O.; Burrell, J.R.; Rowe, C.C.; Hodges, J.R. Subtypes of progressive aphasia: Application of the international consensus criteria and validation using β-amyloid imaging. Brain 2011, 134, 3030–3043. [Google Scholar] [CrossRef] [Green Version]
- Vandenberghe, R. Classification of the primary progressive aphasias: Principles and review of progress since 2011. Alzheimers Res. Ther. 2016, 8, 16. [Google Scholar] [CrossRef] [Green Version]
- Marshall, C.R.; Hardy, C.J.D.; Volkmer, A.; Russell, L.L.; Bond, R.L.; Fletcher, P.D.; Clark, C.N.; Mummery, C.J.; Schott, J.M.; Rossor, M.N.; et al. Primary progressive aphasia: A clinical approach. J. Neurol. 2018, 265, 1474–1490. [Google Scholar] [CrossRef] [Green Version]
- Tee, B.L.; Gorno-Tempini, M.L. Primary progressive aphasia: A model for neurodegenerative disease. Curr. Opin. Neurol. 2019, 32, 255–265. [Google Scholar] [CrossRef]
- Mesulam, M.; Wicklund, A.; Johnson, N.; Rogalski, E.; Léger, G.C.; Rademaker, A.; Weintraub, S.; Bigio, E.H. Alzheimer and frontotemporal pathology in subsets of primary progressive aphasia. Ann. Neurol. 2008, 63, 709–719. [Google Scholar] [CrossRef] [Green Version]
- Mesulam, M.; Wieneke, C.; Rogalski, E.; Cobia, D.; Thompson, C.; Weintraub, S. Quantitative template for subtyping primary progressive aphasia. Arch. Neurol. 2009, 66, 1545–1551. [Google Scholar] [CrossRef] [Green Version]
- Alzheimer’s Association. 2022 Alzheimer’s disease facts and figures. Alzheimer’s Dement. 2022, 18, 700–789. [Google Scholar] [CrossRef]
- Joubert, S.; Gour, N.; Guedj, E.; Didic, M.; Gu, C. Early-onset and late-onset Alzheimer’s disease are associated with distinct patterns of memory impairment. Cortex 2016, 4, 217–232. [Google Scholar] [CrossRef]
- Townley, R.A.; Graff-Radford, J.; Mantyh, W.G.; Botha, H.; Polsinelli, A.J.; Przybelski, S.A.; Machulda, M.M.; Makhlouf, A.T.; Senjem, M.L.; Murray, M.E.; et al. Progressive dysexecutive syndrome due to Alzheimer’s disease: A description of 55 cases and comparison to other phenotypes. Brain Commun. 2020, 2, fcaa068. [Google Scholar] [CrossRef] [PubMed]
- Godefroy, O.; Martinaud, O.; Narme, P.; Joseph, P.-A.; Mosca, C.; Lhommée, E.; Meulemans, T.; Czernecki, V.; Bertola, C.; Labauge, P.; et al. Dysexecutive disorders and their diagnosis: A position paper. Cortex 2018, 109, 322–335. [Google Scholar] [CrossRef]
- Diamond, A. Executive functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alexander, M.P.; Benson, D.F.; Stuss, D.T. Frontal lobes and language. Brain Lang. 1989, 37, 656–691. [Google Scholar] [CrossRef]
- Baddeley, A.D. Working memory. Curr. Biol. 2010, 20, 136–140. [Google Scholar] [CrossRef] [Green Version]
- Miyake, A.; Emerson, M.J.; Friedman, N.P. Assessment of executive functions in clinical settings: Problems and recommendations. Semin. Speech Lang. 2000, 21, 169–183. [Google Scholar] [CrossRef]
- Stuss, D.T. Functions of the frontal lobes: Relation to executive functions. J. Int. Neuropsychol. Soc. 2011, 17, 759–765. [Google Scholar] [CrossRef] [Green Version]
- Mesulam, M. Primary progressive aphasia—A language-based dementia. N. Engl. J. Med. 2003, 349, 1535–1542. [Google Scholar] [CrossRef] [PubMed]
- Eikelboom, W.S.; Janssen, N.; Jiskoot, L.C.; van den Berg, E.; Roelofs, A.; Kessels, R.P.C. Episodic and working memory function in primary progressive aphasia: A meta-analysis. Neurosci. Biobehav. Rev. 2018, 92, 243–254. [Google Scholar] [CrossRef]
- Harris, J.M.; Saxon, J.A.; Jones, M.; Snowden, J.S.; Thompson, J.C. Neuropsychological differentiation of progressive aphasic disorders. J. Neuropsychol. 2018, 13, 214–239. [Google Scholar] [CrossRef] [Green Version]
- Lukic, S.; Mandelli, M.L.; Welch, A.; Jordan, K.; Shwe, W.; Neuhaus, J.; Miller, Z.; Hubbard, H.I.; Henry, M.; Miller, B.L.; et al. Neurocognitive basis of repetition deficits in primary progressive aphasia. Brain Lang. 2019, 194, 35–45. [Google Scholar] [CrossRef]
- Plonka, A.; Mouton, A.; Macoir, J.; Tran, T.-M.; Derremaux, A.; Robert, P.; Manera, V.; Gros, A. Primary progressive aphasia: Use of graphical markers for an early and differential diagnosis. Brain Sci. 2021, 11, 1198. [Google Scholar] [CrossRef]
- Ramanan, S.; Foxe, D.; El-Omar, H.; Ahmed, R.M.; Hodges, J.R.; Piguet, O.; Irish, M. Evidence for a pervasive autobiographical memory impairment in logopenic progressive aphasia. Neurobiol. Aging 2021, 108, 168–178. [Google Scholar] [CrossRef]
- Ranasinghe, K.G.; Hinkley, L.B.; Beagle, A.J.; Mizuiri, D.; Honma, S.M.; Welch, A.E.; Hubbard, I.; Mandelli, M.L.; Miller, Z.A.; Garrett, C.; et al. Distinct spatiotemporal patterns of neuronal functional connectivity in primary progressive aphasia variants. Brain 2017, 140, 2737–2751. [Google Scholar] [CrossRef] [Green Version]
- Bettcher, B.M.; Sturm, V.E. Neuropsychological assessment of primary progressive aphasia (PPA). Perspect. Neurophysiol. Neurogenic Speech Lang. Disord. 2014, 24, 128–136. [Google Scholar] [CrossRef] [Green Version]
- Butts, A.M.; Machulda, M.M.; Duffy, J.R.; Strand, E.A.; Whitwell, J.L.; Josephs, K.A. Neuropsychological profiles differ among the three variants of primary progressive aphasia. J. Int. Neuropsychol. Soc. 2015, 21, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Foxe, D.G.; Irish, M.; Hodges, J.R.; Piguet, O. Verbal and visuospatial span in logopenic progressive aphasia and Alzheimer’s disease. J. Int. Neuropsychol. Soc. 2013, 19, 247–253. [Google Scholar] [CrossRef]
- Foxe, D.; Leyton, C.E.; Hodges, J.R.; Burrell, J.R.; Irish, M.; Piguet, O. The neural correlates of auditory and visuospatial span in logopenic progressive aphasia and Alzheimer’s disease. Cortex 2016, 83, 39–50. [Google Scholar] [CrossRef]
- Foxe, D.; Irish, M.; Roquet, D.; Scharfenberg, A.; Bradshaw, N.; Hodges, J.R.; Burrell, J.R.; Piguet, O. Visuospatial short-term and working memory disturbance in the primary progressive aphasias: Neuroanatomical and clinical implications. Cortex 2020, 132, 223–237. [Google Scholar] [CrossRef]
- Hardy, C.J.D.; Buckley, A.H.; Downey, L.E.; Lehmann, M.; Zimmerer, V.C.; Varley, R.A.; Crutch, S.J.; Rohrer, J.D.; Warrington, E.K.; Warren, J.D. The language profile of behavioral variant frontotemporal dementia. J. Alzheimer’s Dis. 2015, 50, 359–371. [Google Scholar] [CrossRef] [PubMed]
- Magnin, E.; Chopard, G.; Ferreira, S.; Sylvestre, G.; Dariel, E.; Ryff, I.; Mertz, C.; Lamidieu, C.; Hidalgo, J.; Tio, G.; et al. Initial neuropsychological profile of a series of 20 patients with logopenic variant of primary progressive aphasia. J. Alzheimer’s Dis. 2013, 36, 799–808. [Google Scholar] [CrossRef] [PubMed]
- Magnin, E.; Teichmann, M.; Martinaud, O.; Moreaud, O.; Ryff, I.; Belliard, S.; Pariente, J.; Moulin, T.; Vandel, P.; Démonet, J.F. Particularités du variant logopénique au sein des aphasies progressives primaires. Rev. Neurol. 2015, 171, 16–30. [Google Scholar] [CrossRef]
- Matias-Guiu, J.A.; Díaz-Álvarez, J.; Cuetos, F.; Cabrera-Martín, M.N.; Segovia-Ríos, I.; Pytel, V.; Moreno-Ramos, T.; Carreras, J.L.; Matías-Guiu, J.; Ayala, J.L. Machine learning in the clinical and language characterisation of primary progressive aphasia variants. Cortex 2019, 119, 312–323. [Google Scholar] [CrossRef]
- Montembeault, M.; Chapleau, M.; Jarret, J.; Boukadi, M.; Laforce, R.; Wilson, M.A.; Rouleau, I.; Brambati, S.M. Differential language network functional connectivity alterations in Alzheimer’s disease and the semantic variant of primary progressive aphasia. Cortex 2019, 117, 284–298. [Google Scholar] [CrossRef]
- Heidler-Gary, J.; Gottesman, R.; Newhart, M.; Chang, S.; Ken, L.; Hillis, A.E. Utility of behavioral versus cognitive measures in differentiating between subtypes of frontotemporal lobar degeneration and Alzheimer’s disease. Dement. Geriatr. Cogn. Disord. 2007, 23, 184–193. [Google Scholar] [CrossRef]
- Desgranges, B.; Matuszewski, V.; Piolino, P.; Chételat, G.; Mézenge, F.; Landeau, B.; de la Sayette, V.; Belliard, S.; Eustache, F. Anatomical and functional alterations in semantic dementia: A voxel-based MRI and PET study. Neurobiol. Aging 2007, 28, 1904–1913. [Google Scholar] [CrossRef] [Green Version]
- Foxe, D.; Cheung, S.C.; Cordato, N.J.; Burrell, J.R.; Ahmed, R.M.; Taylor-Rubin, C.; Irish, M.; Piguet, O. Verbal short-term memory disturbance in the primary progressive aphasias: Challenges and distinctions in a clinical setting. Brain Sci. 2021, 11, 1060. [Google Scholar] [CrossRef]
- Macoir, J.; Lavoie, M.; Laforce, R.; Brambati, S.M.; Wilson, M.A. Dysexecutive symptoms in primary progressive aphasia: Beyond diagnostic criteria. J. Geriatr. Psychiatry Neurol. 2017, 30, 151–161. [Google Scholar] [CrossRef]
- Gorno-Tempini, M.L.; Brambati, S.M.; Ginex, V.; Ogar, J.; Dronkers, N.F.; Marcone, A.; Perani, D.; Garibotto, V.; Cappa, S.F.; Miller, B.L. The logopenic/phonological variant of primary progressive aphasia. Neurology 2008, 71, 1227–1234. [Google Scholar] [CrossRef] [Green Version]
- Meyer, A.M.; Snider, S.F.; Campbell, R.E.; Friedman, R.B. Phonological short-term memory in logopenic variant primary progressive aphasia and mild Alzheimer’s disease. Cortex 2015, 71, 183–189. [Google Scholar] [CrossRef] [Green Version]
- Migliaccio, R.; Boutet, C.; Valabregue, R.; Ferrieux, S.; Nogues, M.; Lehéricy, S.; Dormont, D.; Levy, R.; Dubois, B.; Teichmann, M. The brain network of naming: A lesson from primary progressive aphasia. PLoS ONE 2016, 11, e0148707. [Google Scholar] [CrossRef] [Green Version]
- Rohrer, J.D.; Ridgway, G.R.; Crutch, S.J.; Hailstone, J.; Goll, J.C.; Clarkson, M.J.; Mead, S.; Beck, J.; Mummery, C.; Ourselin, S.; et al. Progressive logopenic/phonological aphasia: Erosion of the language network. NeuroImage 2010, 49, 984–993. [Google Scholar] [CrossRef] [Green Version]
- Montembeault, M.; Brambati, S.M.; Gorno-Tempini, M.L.; Migliaccio, R. Clinical, anatomical, and pathological features in the three variants of primary progressive aphasia: A review. Front. Neurol. 2018, 9, 692. [Google Scholar] [CrossRef] [Green Version]
- Ramanan, S.; Roquet, D.; Goldberg, Z.; Hodges, J.R.; Piguet, O.; Irish, M.; Lambon Ralph, M.A. Establishing two principal dimensions of cognitive variation in logopenic progressive aphasia. Brain Commun. 2020, 17, fcaa125. [Google Scholar] [CrossRef]
- Ramanan, S.; Irish, M.; Patterson, K.; Rowe, J.B.; Gorno-Tempini, M.L.; Lambon Ralph, M.A. Understanding the multidimensional cognitive deficits of logopenic variant primary progressive aphasia. Brain 2022, 145, 2955–2966. [Google Scholar] [CrossRef]
- Gorno-Tempini, M.L.; Dronkers, N.F.; Rankin, K.P.; Ogar, J.M.; Phengrasamy, L.; Rosen, H.J.; Julene, K.; Weiner, M.W.; Miller, B.L. Cognition and anatomy in three variants of primary progressive aphasia. Ann. Neurol. 2004, 55, 335–346. [Google Scholar] [CrossRef] [Green Version]
- Rohrer, J.D.; Rossor, M.N.; Warren, J.D. Alzheimer’s pathology in primary progressive aphasia. Neurobiol. Aging 2012, 33, 744–752. [Google Scholar] [CrossRef] [Green Version]
- Baddeley, A. Working memory and language: An overview. J. Commun. Disord. 2003, 36, 189–208. [Google Scholar] [CrossRef]
- Harciarek, M.; Cosentino, S. Language, executive function and social cognition in the diagnosis of frontotemporal dementia syndromes. Int. Rev. Psychiatry 2013, 25, 178–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coemans, S.; Keulen, S.; Savieri, P.; Tsapkini, K.; Engelborghs, S.; Chrispeels, N.; Vandenborre, D.; Paquier, P.; Wilssens, I.; Declerck, M.; et al. Executive functions in primary progressive aphasia: A meta-analysis. Cortex 2022, 157, 304–322. [Google Scholar] [CrossRef] [PubMed]
- Rahul, D.R.; Ponniah, R.J. Language impairment in primary progressive aphasia and other neurodegenerative diseases. J. Genet. 2019, 98, 95. [Google Scholar] [CrossRef] [PubMed]
- Teichmann, M.; Kas, A.; Boutet, C.; Ferrieux, S.; Nogues, M.; Samri, D.; Rogan, C.; Dormont, D.; Dubois, B.; Migliaccio, R. Deciphering logopenic primary progressive aphasia: A clinical, imaging and biomarker investigation. Brain 2013, 136, 3474–3488. [Google Scholar] [CrossRef] [PubMed]
- Bergeron, D.; Gorno-Tempini, M.L.; Rabinovici, G.D.; Santos-Santos, M.A.; Seeley, W.; Miller, B.L.; Pijnenburg, Y.; Keulen, M.A.; Groot, C.; van Berckel, B.N.M.; et al. Prevalence of amyloid-β pathology in distinct variants of primary progressive aphasia. Ann. Neurol. 2018, 84, 729–740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mesulam, M.M.; Weintraub, S.; Rogalski, E.J.; Wieneke, C.; Geula, C.; Bigio, E.H. Asymmetry and heterogeneity of Alzheimer’s and frontotemporal pathology in primary progressive aphasia. Brain 2014, 137, 1176–1192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conca, F.; Esposito, V.; Giusto, G.; Cappa, S.F.; Catricalà, E. Characterization of the logopenic variant of primary progressive aphasia: A systematic review and meta-analysis. Ageing Res. Rev. 2022, 82, 101760. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State.” A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Wechsler, D. Wechsler Adult Intelligence Scale—Fourth Edition (WAIS-IV); Éditions du Centre de psychologie appliquée: Paris, France, 2008. [Google Scholar] [CrossRef]
- Wechsler, D. Wechsler Memory Scale—WMS-MEM-III: Echelle Clinique de Mémoire de Wechsler; Éditions du Centre de Psychologie Appliquée: Paris, France, 2001. [Google Scholar]
- Reitan, R.M. The relation of the Trail Making Test to organic brain damage. J. Consult. Psychol. 1955, 19, 393–394. [Google Scholar] [CrossRef]
- Stroop, J.R. Studies of interference in serial verbal reactions. J. Exp. Psychol. 1935, 18, 643–662. [Google Scholar] [CrossRef]
- Shallice, T. Specific impairments of planning. Philos. Trans. R. Soc. Lond. B. Biol. Sci. 1982, 298, 199–209. [Google Scholar] [CrossRef] [PubMed]
- Ruff, R.M.; Light, R.H.; Evans, R.W. The Ruff figural fluency test: A normative study with adults. Dev. Neuropsychol. 1987, 3, 37–51. [Google Scholar] [CrossRef]
- Mesulam, M.-M.; Wieneke, C.; Thompson, C.; Rogalski, E.; Weintraub, S. Quantitative classification of primary progressive aphasia at early and mild impairment stages. Brain 2012, 135, 1537–1553. [Google Scholar] [CrossRef] [PubMed]
- Mandelli, M.L.; Vilaplana, E.; Brown, J.A.; Hubbard, H.I.; Binney, R.J.; Attygalle, S.; Santos-Santos, M.A.; Miller, Z.A.; Pakvasa, M.; Henry, M.L.; et al. Healthy brain connectivity predicts atrophy progression in non-fluent variant of primary progressive aphasia. Brain 2016, 139, 2778–2791. [Google Scholar] [CrossRef] [PubMed]
- Kamath, V.; Sutherland, E.R.; Chaney, G.-A. A meta-analysis of neuropsychological functioning in the logopenic variant of primary progressive aphasia: Comparison with the semantic and non-fluent variants. J. Int. Neuropsychol. Soc. 2020, 26, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Snowden, J.S. Semantic dementia and the left and right temporal lobes. Cortex 2018, 107, 188–203. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Álvarez, A.; Cabrera-Martín, M.N.; Pytel, V.; Delgado-Alonso, C.; Matías-Guiu, J.; Matias-Guiu, J.A. Design and verbal fluency in Alzheimer’s disease and frontotemporal dementia: Clinical and metabolic correlates. J. Int. Neuropsychol. Soc. 2022, 28, 947–962. [Google Scholar] [CrossRef]
- Franceschi, M.; Caffarra, P.; De Vreese, L.; Pelati, O.; Pradelli, S.; Savarè, R.; Cerutti, R.; Grossi, E. Visuospatial planning and problem solving in Alzheimer’s disease patients: A study with the Tower of London test. Dement. Geriatr. Cogn. Disord. 2007, 24, 424–428. [Google Scholar] [CrossRef]
- Lukic, S.; Borghesani, V.; Weis, E.; Welch, A.; Bogley, R.; Neuhaus, J.; Deleon, J.; Miller, Z.A.; Kramer, J.H.; Miller, B.L.; et al. Dissociating nouns and verbs in temporal and perisylvian networks: Evidence from neurodegenerative diseases. Cortex 2021, 142, 47–61. [Google Scholar] [CrossRef] [PubMed]
- Beales, A.; Whitworth, A.; Cartwright, J.; Panegyres, P.K.; Kane, R.T. Profiling sentence repetition deficits in primary progressive aphasia and Alzheimer’s disease: Error patterns and association with digit span. Brain Lang. 2019, 194, 1–11. [Google Scholar] [CrossRef]
- Rohrer, J.D.; Rossor, M.N.; Warren, J.D. Syndromes of nonfluent primary progressive aphasia. Neurology 2010, 75, 603–610. [Google Scholar] [CrossRef] [Green Version]
- Joubert, S.; Vallet, G.T.; Montembeault, M.; Boukadi, M.; Wilson, M.A.; Laforce, R.J.; Rouleau, I.; Brambati, S.M. Comprehension of concrete and abstract words in semantic variant primary progressive aphasia and Alzheimer’s disease: A behavioral and neuroimaging study. Brain Lang. 2017, 170, 93–102. [Google Scholar] [CrossRef]
- Joyal, M.; Brambati, S.M.; Laforce, R.J.; Montembeault, M.; Boukadi, M.; Rouleau, I.; Macoir, J.; Joubert, S.; Fecteau, S.; Wilson, M.A. The role of the left anterior temporal lobe for unpredictable and complex mappings in word reading. Front. Psychol. 2017, 8, 517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henry, M.L.; Grasso, S.M. Assessment of individuals with primary progressive aphasia. Semin. Speech Lang. 2018, 39, 231–241. [Google Scholar] [CrossRef]
- Tippett, D.C. Classification of primary progressive aphasia: Challenges and complexities. F1000Research 2020, 9, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaeverbeke, J.; Gabel, S.; Meersmans, K.; Bruffaerts, R.; Liuzzi, A.G.; Evenepoel, C.; Dries, E.; Van Bouwel, K.; Sieben, A.; Pijnenburg, Y.; et al. Single-word comprehension deficits in the nonfluent variant of primary progressive aphasia. Alzheimer’s Res. Ther. 2018, 10, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basaglia-Pappas, S.; Ferré, P.; Borg, C.; Dutang, C.; Joanette, Y.; Thomas-Antérion, C. Évaluation de la communication verbale dans le trouble cognitif léger et la maladie d’Alzheimer. Apport du protocole MEC-P. Rev. Neuropsychol. 2014, 6, 163–172. [Google Scholar] [CrossRef]
- Basaglia-Pappas, S.; Laurent, B.; Lefebvre, L. Diagnostic et spécificités des aphasies primaires progressives. Neurologies 2020, 23, 57–62. [Google Scholar]


{kind=link}
{kind=link}
| Controls (n = 41) | lvPPA (n = 22) | nfvPPA (n = 22) | svPPA (n = 26) | AD (n = 32) | F | p-Value | |
|---|---|---|---|---|---|---|---|
| Gender (M/F) | 13/28 | 13/9 | 7/15 | 8/18 | 18/14 | 7.612 1 | 0.124 |
| Handedness (R/L) | 39/2 | 20/2 | 21/1 | 26/0 | 32/0 | ||
| Age: mean (SD) Minimum/maximum | 65.73 (±10.1) 41/86 | 68.95 (±9.3) 46/84 | 69.55 (±4.8) 57/78 | 66.27 (±10.2) 48/83 | 68.66 (±9.5) 53/85 | 1.458 | 0.285 |
| Education: mean (SD) | 12.07 (±3.7) | 11.59 (±2.5) | 11.68 (±2.8) | 12.42 (±3.5) | 11.69 (±2.7) | 1.667 | 0.183 |
| Disease duration months (SD) | / | 26.45 (±3.54) | 27.00 (±4.44) | 27.46 (±4.85) | 25.31 (±5.85) | 1.542 | 0.194 |
| MMSE/30 (SD) | 29.22 (±0.9) | 26.05 (±1.8) a,c | 22.64 (±5.1) a,b | 26.58 (±3.6) b,d | 22.75 (±2.9) c,d | 82.930 | < 0.001 |
| Controls n = 41 | lvPPA n = 22 | nfvPPA n = 22 | svPPA n = 26 | AD n = 32 | Mann-Whitney Tests | |
|---|---|---|---|---|---|---|
| Forward digit span (SD) | 6.05 (1.32) | 4.57 (0.97) | 4.56 (1.01) | 5.50 (1.01) | 5.20 (1.78) | lvPPA, nfvPPA < C **; AD < C *; nfvPPA < AD *; nfvPPA < svPPA **; nfvPPA < lvPPA *; lvPPA < svPPA * |
| Backward digit span(SD) | 4.39 (1.35) | 3.71 (1.25) | 3.00 (0.70) | 4.71 (1.63) | 4.20 (1.09) | nfvPPA < C **; AD < C *; nfvPPA < AD *; AD < svPPA *; nfvPPA < svPPA **; nfvPPA < lvPPA *; lvPPA < svPPA * |
| Forward visuospatial span (SD) | 5.90 (0.83) | 5.43 (0.53) | 4,22 (0.66) | 5.79 (0.89) | 3.80 (0.44) | nfvPPA, AD < C **; AD < svPPA **; AD < lvPPA **; nfvPPA < svPPA **; nfvPPA < lvPPA ** |
| Backward visuospatial span (SD) | 4.85 (1.15) | 4.43 (0.87) | 3.89 (1.05) | 5.14 (0.77) | 3.20 (1.64) | AD < C **; nfvPPA < C *; AD < svPPA **; AD < lvPPA **; nfvPPA < svPPA **; nfvPPA < lvPPA **; nfvPPA < lvPPA * |
| Stroop interference (s)(SD) | 128.90 (25.96) | 197.00 (135.13) | 322.33 (149.63) | 130.79 (33.18) | 218.80 (42.92) | nfvPPA, AD < C **; AD < svPPA *; nfvPPA < svPPA **; nfvPPA < lvPPA * |
| TMT A (s) (SD) | 41.12 (14.05) | 68.71 (24.24) | 83.89 (39.73) | 43.29 (10.02) | 78.00 (20.62) | lvPPA, nfvPPA, AD < C **; AD < svPPA **; nfvPPA < svPPA **; nfvPPA < lvPPA *; lvPPA < svPPA ** |
| TMT B (s) (SD) | 96.24 (31.47) | 190.86 (103.15) | 274.67 (113.09) | 119.86 (75.13) | 165.80 (49.73) | lvPPA, nfvPPA, AD < C **; AD < svPPA *; nfvPPA < svPPA **; nfvPPA < lvPPA *; lvPPA < svPPA * |
| RFFT No. of Prod. (SD) | 73.39 (20.81) | 60.43 (24.86) | 33.33 (18.77) | 64.14 (20.67) | 41.40 (37.95) | nfvPPA, AD < C **; lvPPA, svPPA < C *; AD < svPPA*; nfvPPA < svPPA **; nfvPPA < lvPPA **; nfvPPA < lvPPA * |
| Tower of London No. Mvt. 3 N (SD) | 3.06 (0.19) | 3.18 (0.25) | 3.33 (0.33 | 3.04 (0.11) | 3.40 (0.59) | lvPPA, nfvPPA, AD < C *; nfvPPA < svPPA * |
| Tower of London No. Mvt. 5 N (SD) | 5.91 (1.32) | 8.33 (5.91) | 11.77 (2.90) | 6.71 (2.70) | 8.40 (4.12) | nfvPPA < C **; nfvPPA < svPPA *; nfvPPA < lvPPA **; nfvPPA < lvPPA * |
| Tower of London No. Mvt. 5 i+ (SD) | 5.46 (1.31) | 5.80 (1.16) | 7.88 (5.83) | 6.11 (2.41) | 8.66 (4.57) | AD < C **; lvPPA < C *; AD < svPPA * |
| Tower of London No. Mvt. 5 i- (SD) | 7.02 (2.25) | 11.71 (5.68) | 14.92 (7.71) | 7.35 (2.62) | 14.33 (5.12) | lvPPA, nfvPPA, AD < C *; AD < svPPA *; nfvPPA < svPPA * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Basaglia-Pappas, S.; Laurent, B.; Getenet, J.-C.; Boulangé, A.; Rendón de laCruz, A.; Simoes Loureiro, I.; Lefebvre, L. Executive Profile of the Logopenic Variant of Primary Progressive Aphasia: Comparison with the Semantic and Non-Fluent Variants and Alzheimer’s Disease. Brain Sci. 2023, 13, 406. https://doi.org/10.3390/brainsci13030406
Basaglia-Pappas S, Laurent B, Getenet J-C, Boulangé A, Rendón de laCruz A, Simoes Loureiro I, Lefebvre L. Executive Profile of the Logopenic Variant of Primary Progressive Aphasia: Comparison with the Semantic and Non-Fluent Variants and Alzheimer’s Disease. Brain Sciences. 2023; 13(3):406. https://doi.org/10.3390/brainsci13030406
Chicago/Turabian StyleBasaglia-Pappas, Sandrine, Bernard Laurent, Jean-Claude Getenet, Anne Boulangé, Aurelia Rendón de laCruz, Isabelle Simoes Loureiro, and Laurent Lefebvre. 2023. "Executive Profile of the Logopenic Variant of Primary Progressive Aphasia: Comparison with the Semantic and Non-Fluent Variants and Alzheimer’s Disease" Brain Sciences 13, no. 3: 406. https://doi.org/10.3390/brainsci13030406