

Based on Tau PET Radiomics Analysis for the Classification of Alzheimer’s Disease and Mild Cognitive Impairment
 and
and
Abstract
:1. Introduction
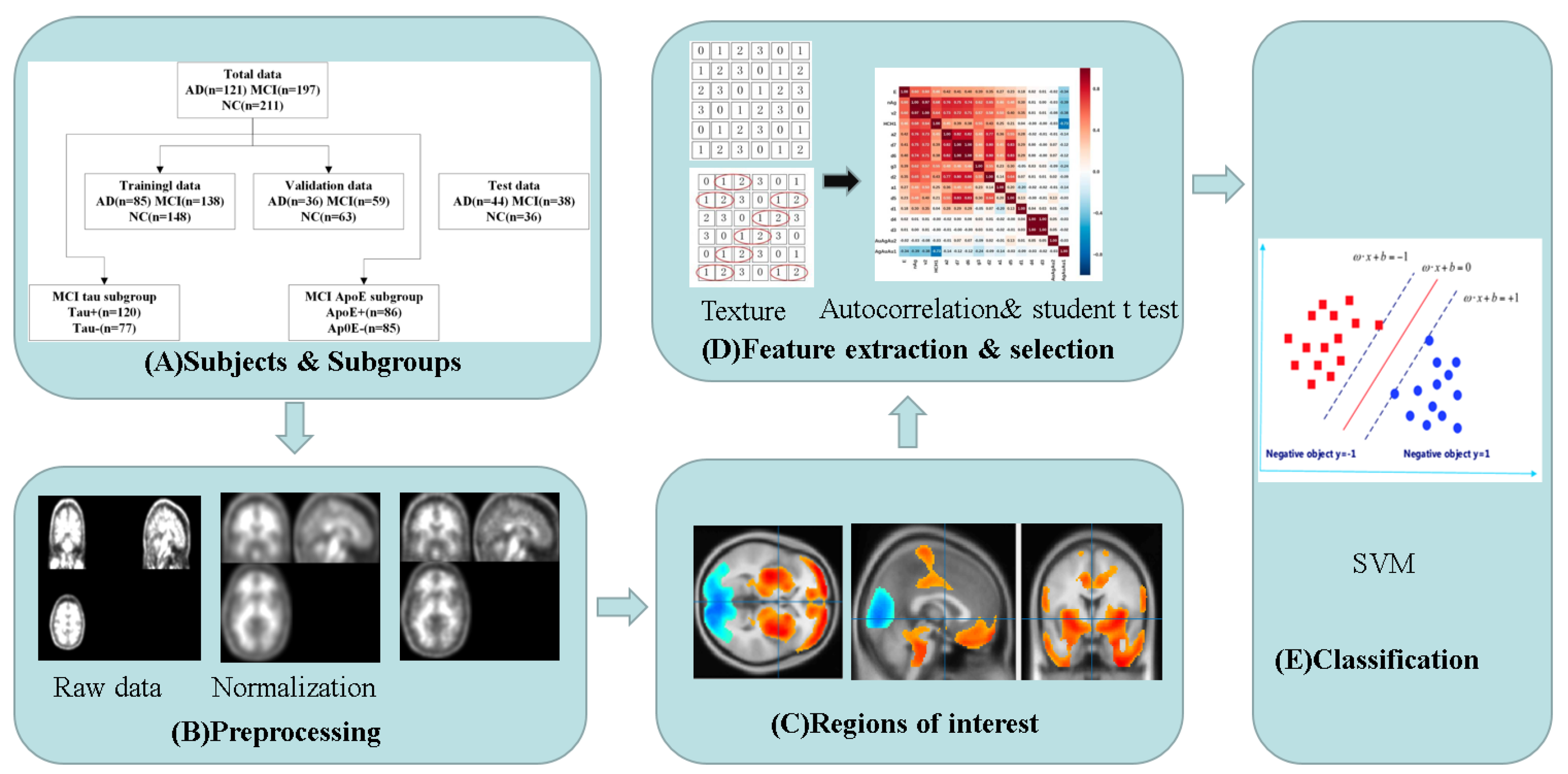
2. Materials and Methods
2.1. Subjects
2.2. Radiomics Model
2.3. Comparative Models
2.4. Radiomics Model in MCI Subgroups
2.5. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics
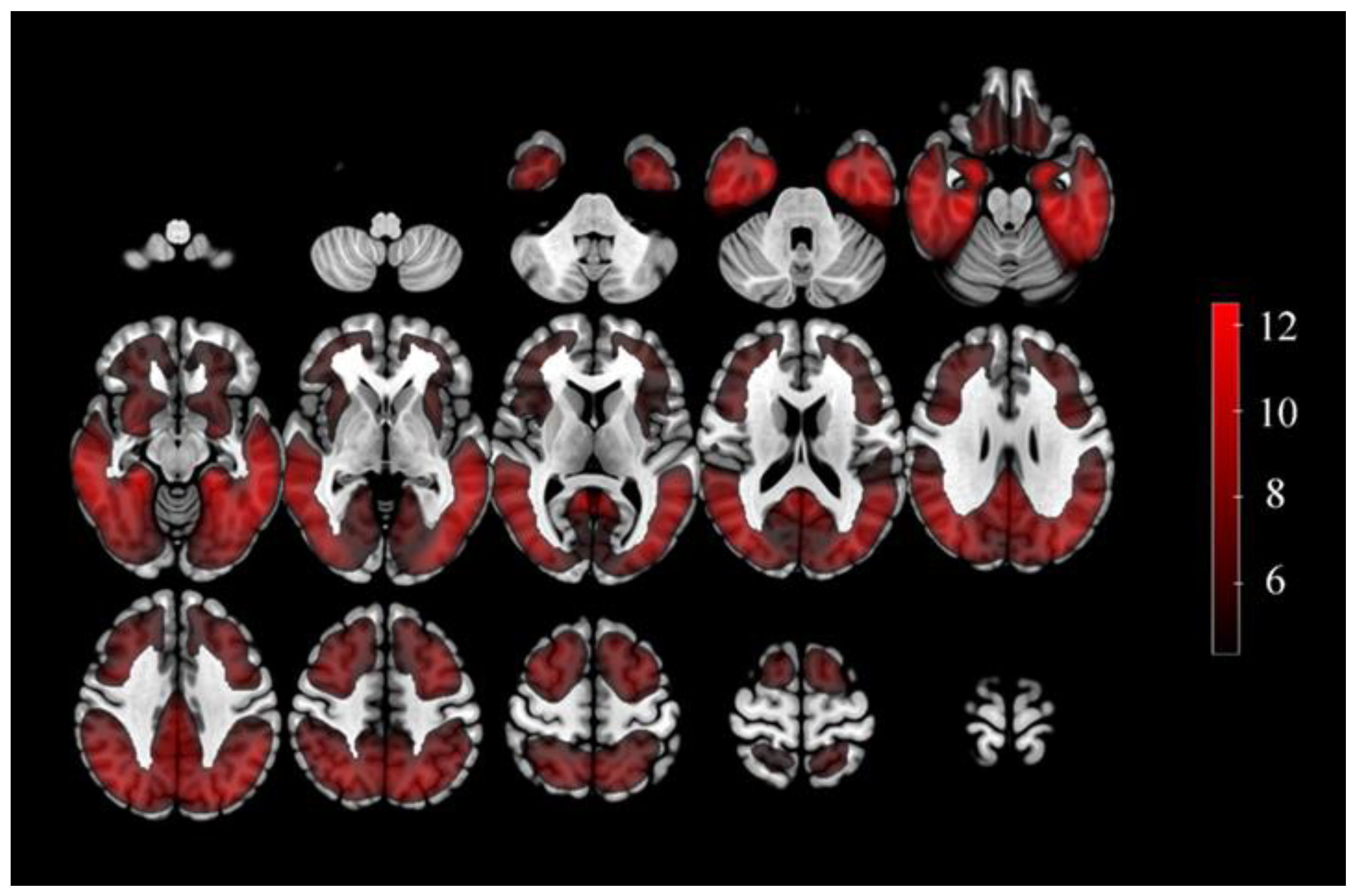
3.2. The Defined ROIs and Selected Features
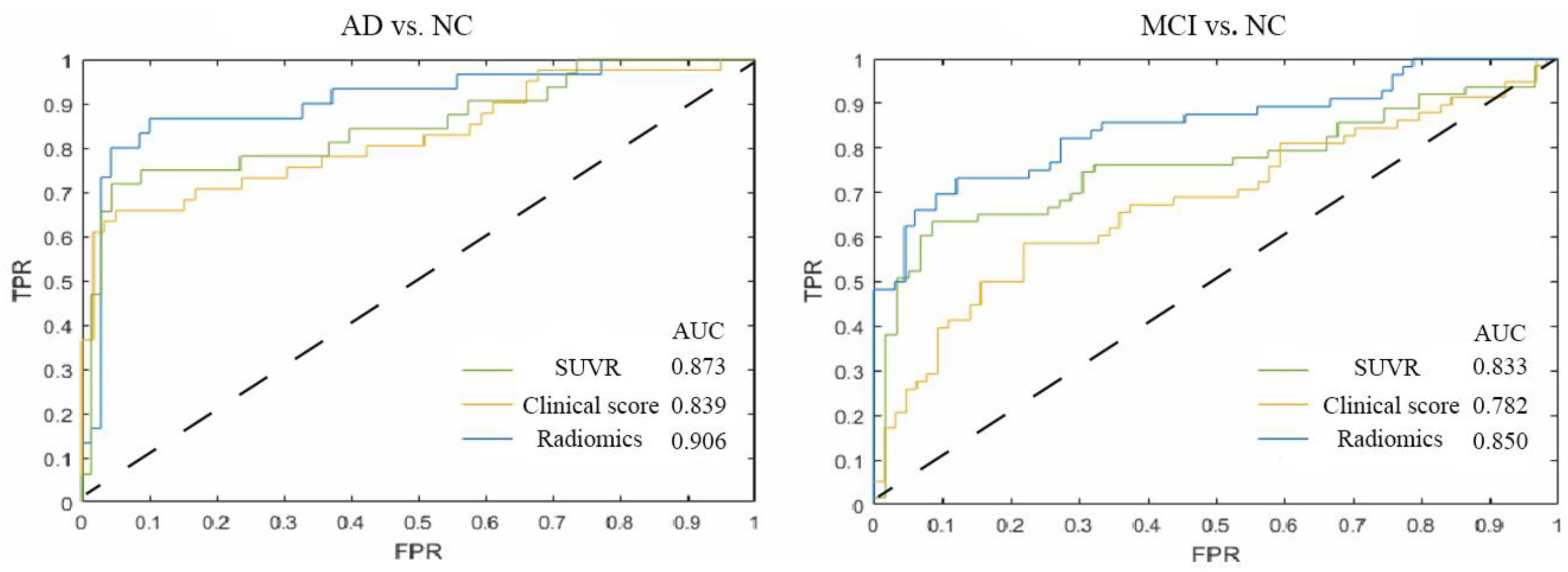
3.3. Tau PET Radiomics Model for the Diagnosis AD/MCI
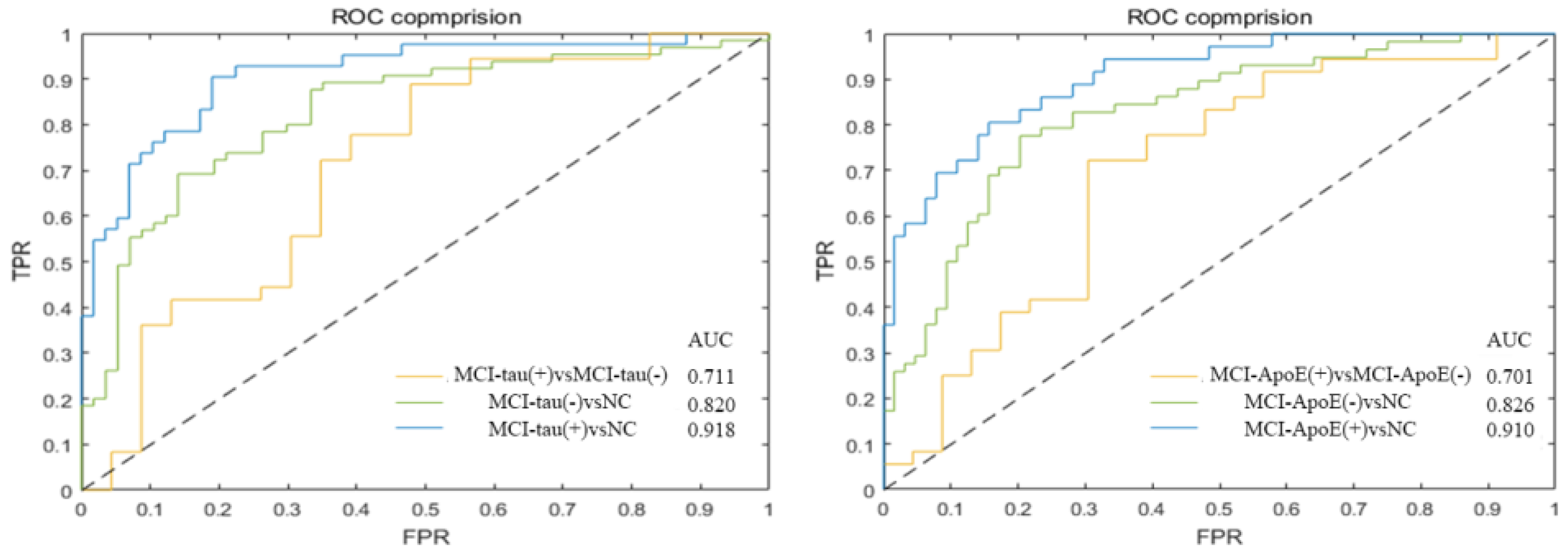
3.4. Tau PET Radiomics Model for the Diagnosis MCI Subgroups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AD | Alzheimer’s Disease |
| MCI | Mild Cognitive Impairment |
| NC | Normal control |
| SVM | Support vector machine |
| SUVR | Standard uptake value ratio |
| PET | Positron emission tomography |
| 18F-FDG | 18F- fluoro-2-deoxyglucose |
| ApoE | apolipoprotein E |
| Aβ | Amyloid β-protein |
| ROIs | Regions of interest |
| ADNI | Alzheimer Disease Neuroimaging Initiative |
| MMSE | Mini-Mental State Examination |
| GLCM | Gray-Level Co-occurrence Matrix |
| GLRLM | Gray-Level Run-Length Matrix |
| GLSZM | Gray-Level Size Zone Matrix |
| NGTDM | Neighborhood Gray-Tone Difference Matrix |
| ROC | Receiver operating characteristic |
| AUC | Areas under the curve |
References
- Jack, C.R.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Dunn, B.; Haeberlein, S.B.; Holtzman, D.M.; Jagust, W.; Jessen, F.; Karlawish, J.; et al. NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease. Alzheimer’s Dement. 2018, 14, 535–562. [Google Scholar] [CrossRef] [PubMed]
- McCollum, L.E.; Das, S.R.; Xie, L.; de Flores, R.; Wang, J.; Xie, S.X.; Wisse, L.E.M.; Yushkevich, P.A.; Wolk, D.A. Oh brother, where art tau? Amyloid, neurodegeneration, and cognitive decline without elevated tau. NeuroImage Clin. 2021, 31, 102717. [Google Scholar] [CrossRef] [PubMed]
- Betthauser, T.J.; Koscik, R.L.; Jonaitis, E.M.; Allison, S.L.; Cody, K.A.; Erickson, C.M.; Rowley, H.A.; Stone, C.K.; Mueller, K.D.; Clark, L.R.; et al. Amyloid and tau imaging biomarkers explain cognitive decline from late middle-age. Brain 2020, 143, 320–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ossenkoppele, R.; Smith, R.; Mattsson-Carlgren, N.; Groot, C.; Leuzy, A.; Strandberg, O.; Palmqvist, S.; Olsson, T.; Jogi, J.; Stormrud, E.; et al. Accuracy of Tau Positron Emission Tomography as a Prognostic Marker in Preclinical and Prodromal Alzheimer Disease: A Head-to-Head Comparison Against Amyloid Positron Emission Tomography and Magnetic Resonance Imaging. JAMA Neurol. 2021, 78, 961–971. [Google Scholar] [CrossRef]
- Buckley, R.F.; Hanseeuw, B.; Schultz, A.P.; Vannini, P.; Aghjayan, S.L.; Properzi, M.J.; Jackson, J.D.; Mormino, E.C.; Rentz, D.M.; Sperling, R.A.; et al. Region-Specific Association of Subjective Cognitive Decline with Tauopathy Independent of Global β-Amyloid Burden. JAMA Neurol. 2017, 74, 1455–1463. [Google Scholar] [CrossRef] [PubMed]
- Maschio, C.; Ni, R. Amyloid and Tau Positron Emission Tomography Imaging in Alzheimer’s Disease and Other Tauopathies. Front. Aging Neurosci. 2022, 14, 838034. [Google Scholar] [CrossRef]
- Devous Sr., M.D.; Fleisher, A.S.; Pontecorvo, M.J.; Lu, M.; Siderowf, A.; Navitsky, M.; Kennedy, I.; Southekal, S.; Harris, T.S.; Mintun, M.A. Relationships Between Cognition and Neuropathological Tau in Alzheimer’s Disease Assessed by 18F Flortaucipir PET. J. Alzheimer’s Dis. 2021, 80, 1091–1104. [Google Scholar] [CrossRef]
- Kroth, H.; Oden, F.; Molette, J.; Schieferstein, H.; Capotosti, F.; Mueller, A.; Berndt, M.; Schmitt-Willich, H.; Darmency, V.; Gabellieri, E.; et al. Discovery and preclinical characterization of [18F]PI-2620, a next-generation tau PET tracer for the assessment of tau pathology in Alzheimer’s disease and other tauopathies. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2178–2189. [Google Scholar] [CrossRef] [Green Version]
- Shi, Y.; Murzin, A.G.; Falcon, B.; Epstein, A.; Machin, J.; Tempest, P.; Newell, K.L.; Vidal, R.; Garringer, H.J.; Sahara, N.; et al. Cryo-EM structures of tau filaments from Alzheimer’s disease with PET ligand APN-1607. Acta Neuropathol. 2021, 141, 697–708. [Google Scholar] [CrossRef]
- Botha, H.; Mantyh, W.G.; Graff-Radford, J.; Machulda, M.M.; Przybelski, S.A.; Wiste, H.J.; Senjem, M.L.; Parisi, J.E.; Petersen, R.C.; Murray, M.E.; et al. Tau-negative amnestic dementia masquerading as Alzheimer disease dementia. Neurology 2018, 90, e940–e946. [Google Scholar] [CrossRef]
- Whitwell, J.L.; Martin, P.; Radford, J.G.; Machulda, M.M.; Senjem, M.L.; Schwarz, C.G.; Weigand, S.D.; Spychalla, A.J.; Drubach, D.A.; Jack, C.R.; et al. The role of age on tau PET uptake and gray matter atrophy in atypical Alzheimer’s disease. Alzheimer’s Dement. 2019, 15, 675–685. [Google Scholar] [CrossRef] [PubMed]
- Guo, T.; Landau, S.M.; Jagust, W.J. Age, vascular disease, and Alzheimer’s disease pathologies in amyloid negative elderly adults. Alzheimer’s Res. Ther. 2021, 13, 174. [Google Scholar] [CrossRef] [PubMed]
- Wegmann, S.; Bennett, R.E.; Delorme, L.; Robbins, A.B.; Hu, M.; McKenzie, D.; Kirk, M.J.; Schiantarelli, J.; Tunio, N.; Amaral, A.C.; et al. Experimental evidence for the age dependence of tau protein spread in the brain. Sci. Adv. 2019, 5, w6404. [Google Scholar] [CrossRef] [Green Version]
- Mayerhoefer, M.E.; Materka, A.; Langs, G.; Haggstrom, I.; Szczypinski, P.; Gibbs, P.; Cook, G. Introduction to Radiomics. J. Nucl. Med. 2020, 61, 488–495. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Zhang, J.; Li, Z.; Li, L.; Huang, B. Using Deep Learning Radiomics to Distinguish Cognitively Normal Adults at Risk of Alzheimer’s Disease from Normal Control: An Exploratory Study Based on Structural MRI. Front. Med. 2022, 9, 894726. [Google Scholar] [CrossRef] [PubMed]
- Alongi, P.; Laudicella, R.; Panasiti, F.; Stefano, A.; Comelli, A.; Giaccone, P.; Arnone, A.; Minutoli, F.; Quartuccio, N.; Cupidi, C.; et al. Radiomics Analysis of Brain [18F]FDG PET/CT to Predict Alzheimer’s Disease in Patients with Amyloid PET Positivity: A Preliminary Report on the Application of SPM Cortical Segmentation, Pyradiomics and Machine-Learning Analysis. Diagnostics 2022, 12, 933. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Jiang, J.; Li, Z.; Sheng, C.; Du, W.; Li, X.; Han, Y. Identification of subjective cognitive decline due to Alzheimer’s disease using multimodal MRI combining with machine learning. Cereb. Cortex 2022, 33, 557–566. [Google Scholar] [CrossRef]
- Li, Y.; Jiang, J.; Lu, J.; Jiang, J.; Zhang, H.; Zuo, C. Radiomics: A novel feature extraction method for brain neuron degeneration disease using18F-FDG PET imaging and its implementation for Alzheimer’s disease and mild cognitive impairment. Ther. Adv. Neurol. Disord. 2019, 12, 1160684164. [Google Scholar] [CrossRef] [Green Version]
- La Joie, R.; Visani, A.V.; Lesman-Segev, O.H.; Baker, S.L.; Edwards, L.; Iaccarino, L.; Soleimani-Meigooni, D.N.; Mellinger, T.; Janabi, M.; Miller, Z.A.; et al. Association of APOE4 and Clinical Variability in Alzheimer Disease with the Pattern of Tau- and Amyloid-PET. Neurology 2021, 96, e650–e661. [Google Scholar] [CrossRef]
- Durairajan, S.S.K.; Selvarasu, K.; Bera, M.R.; Rajaram, K.; Iyaswamy, A.; Li, M. Alzheimer’s Disease and other Tauopathies: Exploring Efficacy of Medicinal Plant-derived Compounds in Alleviating Tau-mediated Neurodegeneration. Curr. Mol. Pharm. 2022, 15, 361. [Google Scholar] [CrossRef]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R., Jr.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albert, M.S.; DeKosky, S.T.; Dickson, D.; Dubois, B.; Feldman, H.H.; Fox, N.C.; Gamst, A.; Holtzman, D.M.; Jagust, W.J.; Petersen, R.C.; et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s Dement. 2011, 7, 270–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, F.T.; Li, X.Y.; Lu, J.Y.; Wu, P.; Li, L.; Liang, X.N.; Ju, Z.Z.; Jiao, F.Y.; Chen, M.J.; Ge, J.J.; et al. 18F-FlorzolotauTau Positron Emission Tomography Imaging in Patients with Multiple SystemAtrophy–Parkinsonian Subtype. Mov. Disord. 2022, 37, 1915–1923. [Google Scholar] [CrossRef] [PubMed]
- Hsu, J.; Lin, K.; Hsiao, I.; Huang, K.; Liu, C.; Wu, H.; Weng, Y.; Huang, C.; Chang, C.; Yen, T.; et al. The Imaging Features and Clinical Associations of a Novel Tau PET Tracer—18F-APN1607 in Alzheimer Disease. Clin. Nucl. Med. 2020, 45, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Devous, M.D.; Joshi, A.D.; Navitsky, M.; Southekal, S.; Pontecorvo, M.J.; Shen, H.; Lu, M.; Shankle, W.R.; Seibyl, J.P.; Marek, K.; et al. Test–Retest Reproducibility for the Tau PET Imaging Agent Flortaucipir F 18. J. Nucl. Med. 2018, 59, 937–943. [Google Scholar] [CrossRef] [Green Version]
- Vallières, M.; Freeman, C.R.; Skamene, S.R.; El Naqa, I. A radiomics model from joint FDG-PET and MRI texture features for the prediction of lung metastases in soft-tissue sarcomas of the extremities. Phys. Med. Biol. 2015, 60, 5471–5496. [Google Scholar] [CrossRef]
- Feng, Q.; Ding, Z. MRI Radiomics Classification and Prediction in Alzheimer’s Disease and Mild Cognitive Impairment: A Review. Curr. Alzheimer Res. 2020, 17, 297–309. [Google Scholar] [CrossRef]
- Won, S.Y.; Park, Y.W.; Park, M.; Ahn, S.S.; Kim, J.; Lee, S. Quality Reporting of Radiomics Analysis in Mild Cognitive Impairment and Alzheimer’s Disease: A Roadmap for Moving Forward. Korean J. Radiol. 2020, 21, 1345–1354. [Google Scholar] [CrossRef]
- Feng, Q.; Niu, J.; Wang, L.; Pang, P.; Wang, M.; Liao, Z.; Song, Q.; Jiang, H.; Ding, Z. Comprehensive classification models based on amygdala radiomic features for Alzheimer’s disease and mild cognitive impairment. Brain Imaging Behav. 2021, 15, 2377–2386. [Google Scholar] [CrossRef]
- Du, Y.; Zhang, S.; Fang, Y.; Qiu, Q.; Zhao, L.; Wei, W.; Tang, Y.; Li, X. Radiomic Features of the Hippocampus for Diagnosing Early-Onset and Late-Onset Alzheimer’s Disease. Front. Aging Neurosci. 2022, 13, 789099. [Google Scholar] [CrossRef]
- Ding, Y.; Zhao, K.; Che, T.; Du, K.; Sun, H.; Liu, S.; Zheng, Y.; Li, S.; Liu, B.; Liu, Y. Quantitative Radiomic Features as New Biomarkers for Alzheimer’s Disease: An Amyloid PET Study. Cereb. Cortex 2021, 31, 3950–3961. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Wang, M.; Lu, J.; Bao, W.; Li, L.; Jiang, J.; Zuo, C. Parametric Estimation of Reference Signal Intensity for Semi-Quantification of Tau Deposition: A Flortaucipir and [18F]-APN-1607 Study. Front. Neurosci. 2021, 15, 598234. [Google Scholar] [CrossRef] [PubMed]
- Pinto, T.C.C.; Machado, L.; Bulgacov, T.M.; Rodrigues-Júnior, A.L.; Costa, M.L.G.; Ximenes, R.C.C.; Sougey, E.B. Is the Montreal Cognitive Assessment (MoCA) screening superior to the Mini-Mental State Examination (MMSE) in the detection of mild cognitive impairment (MCI) and Alzheimer’s Disease (AD) in the elderly? Int. Psychogeriatr. 2019, 31, 491–504. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.; Lin, Y.; Yang, L.; Wang, Y.; Cai, S.; Pang, L.; Wu, X.; Huang, L. A multipredictor model to predict the conversion of mild cognitive impairment to Alzheimer’s disease by using a predictive nomogram. Neuropsychopharmacology 2020, 45, 358–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abner, E.L.; Kryscio, R.J.; Schmitt, F.A.; Fardo, D.W.; Moga, D.C.; Ighodaro, E.T.; Jicha, G.A.; Yu, L.; Dodge, H.H.; Xiong, C.; et al. Outcomes after diagnosis of mild cognitive impairment in a large autopsy series. Ann. Neurol. 2017, 81, 549–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Josephs, K.A.; Weigand, S.D.; Whitwell, J.L. Characterizing Amyloid-Positive Individuals with Normal Tau PET Levels After 5 Years. Neurology 2022, 98, e2282–e2292. [Google Scholar] [CrossRef] [PubMed]
- Ren, D.; Lopez, O.L.; Lingler, J.H.; Conley, Y. The Effect of the APOE ε2ε4 Genotype on the Development of Alzheimer’s Disease (AD) and Mild Cognitive Impairment (MCI) in Non-Latino Whites. J. Am. Geriatr. Soc. 2020, 68, 1044–1049. [Google Scholar] [CrossRef]
- Yan, S.; Zheng, C.; Paranjpe, M.D.; Li, Y.; Li, W.; Wang, X.; Benzinger, T.L.S.; Lu, J.; Zhou, Y. Sex modifies APOE ε4 dose effect on brain tau deposition in cognitively impaired individuals. Brain 2021, 144, 3201–3211. [Google Scholar] [CrossRef]
- Safieh, M.; Korczyn, A.D.; Michaelson, D.M. ApoE4: An emerging therapeutic target for Alzheimer’s disease. BMC Med. 2019, 17, 64. [Google Scholar] [CrossRef] [Green Version]
- Jellinger, K.A. Recent update on the heterogeneity of the Alzheimer’s disease spectrum. J. Neural Transm. 2022, 129, 1–24. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (Years) | Sex (Male/Female) | Education (Years) | MMSE | |
|---|---|---|---|---|
| ANDI cohort | ||||
| AD (n = 121) | 72.1 ± 7.5 * | 55/66 * | 15.5 ± 2.6 * | 24.0 ± 3.3 * |
| MCI (n = 197) | 71.1 ± 7.4 † | 108/89 † | 16.4 ± 2.5 † | 27.9 ± 1.9 †‡ |
| NC (n = 211) | 71.2 ± 6.4 | 79/132 | 16.7 ± 2.3 | 29.1 ± 1.2 |
| Huashan hospital | ||||
| AD (n = 44) | 58.2 ± 9.6 | 17/27 | 9.8 ± 4.2 * | 16.6 ± 6.9 * |
| MCI (n = 33) | 69.4 ± 8.4 †‡ | 10/23 | 10.4 ± 3.2 † | 25.6 ± 1.8 †‡ |
| NC (n = 36) | 58.5 ± 8.2 | 18/20 | 10.1 ± 2.1 | 27.2 ± 2.5 |
| Model | Accuracy (%) | Sensibility (%) | Specificity (%) |
|---|---|---|---|
| Radiomics | |||
| Validation | 84.8 ± 4.5 | 76.1 ± 5.1 | 88.7 ± 2.9 |
| Test | 81.9 ± 6.1 | 83.8 ± 4.9 | 78.6 ± 7.3 |
| SUVR | |||
| Validation | 80.3 ± 1.4 | 61.5 ± 3.5 | 87.0 ± 5.0 |
| Test | 75.1 ± 3.5 | 60.8 ± 7.8 | 79.1 ± 1.5 |
| Clinical scores | |||
| Validation | 70.5 ± 5.2 | 58.2 ± 13.9 | 79.9 ± 12.0 |
| Test | 66.4 ± 10.2 | 53.3 ± 6.5 | 70.2 ± 11.7 |
| Model | Accuracy (%) | Sensibility (%) | Specificity (%) |
|---|---|---|---|
| Radiomics | |||
| Validation | 73.1 ± 3.6 | 71.3 ± 6.1 | 75.0 ± 5.5 |
| Test | 63.5 ± 8.7 | 65.7 ± 8.8 | 60.6 ± 5.8 |
| SUVR | |||
| Validation | 70.8 ± 2.7 | 58.5 ± 14.8 | 88.4 ± 9.8 |
| Test | 68.7 ± 5.5 | 53.8 ± 14.4 | 86.7 ± 8.7 |
| Clinical scores | |||
| Validation | 65.1 ± 5.2 | 42.5 ± 13.9 | 87.5 ± 12.0 |
| Test | 63.1 ± 11.0 | 49.8 ± 9.6 | 80.5 ± 21.5 |
| Accuracy (%) | Sensibility (%) | Specificity (%) | |
|---|---|---|---|
| MCI-tau(+) vs. NC | |||
| Train | 93.5 ± 2.7 | 92.0 ± 2.2 | 94.1 ± 3.6 |
| Validation | 72.3 ± 3.5 | 70.4 ± 5.9 | 74.0 ± 5.8 |
| MCI-tau(-) vs. NC | |||
| Train | 91.7 ± 0.9 | 91.0 ± 1.2 | 92.0 ± 3.4 |
| Validation | 71.9 ± 3.6 | 70.1 ± 6.0 | 73.5 ± 5.1 |
| MCI-tau(+) vs. MCI-tau(+) | |||
| Train | 83.4 ± 5.2 | 88.5 ± 7.3 | 80.1 ± 4.5 |
| Validation | 63.7 ± 5.9 | 69.4 ± 6.6 | 53.2 ± 8.0 |
| Accuracy (%) | Sensibility (%) | Specificity (%) | |
|---|---|---|---|
| MCI-ApoE(+) vs. NC | |||
| Train | 92.7 ± 1.1 | 92.7 ± 2.1 | 93.8 ± 1.8 |
| Validation | 73.5 ± 4.3 | 68.0 ± 3.8 | 76.6 ± 4.6 |
| MCI-ApoE(-) vs. NC | |||
| Train | 92.5 ± 2.9 | 91.0 ± 3.3 | 92.9 ± 2.0 |
| Validation | 70.1 ± 3.9 | 68.0 ± 3.0 | 72.8 ± 5.1 |
| MCI-ApoE(+) vs. MCI-ApoE(-) | |||
| Train | 87.1 ± 8.9 | 90.3 ± 10.5 | 83.6 ± 5.7 |
| Validation | 62.5 ± 5.4 | 71.6 ± 7.2 | 51.6 ± 11.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiao, F.; Wang, M.; Sun, X.; Ju, Z.; Lu, J.; Wang, L.; Jiang, J.; Zuo, C. Based on Tau PET Radiomics Analysis for the Classification of Alzheimer’s Disease and Mild Cognitive Impairment. Brain Sci. 2023, 13, 367. https://doi.org/10.3390/brainsci13020367
Jiao F, Wang M, Sun X, Ju Z, Lu J, Wang L, Jiang J, Zuo C. Based on Tau PET Radiomics Analysis for the Classification of Alzheimer’s Disease and Mild Cognitive Impairment. Brain Sciences. 2023; 13(2):367. https://doi.org/10.3390/brainsci13020367
Chicago/Turabian StyleJiao, Fangyang, Min Wang, Xiaoming Sun, Zizhao Ju, Jiaying Lu, Luyao Wang, Jiehui Jiang, and Chuantao Zuo. 2023. "Based on Tau PET Radiomics Analysis for the Classification of Alzheimer’s Disease and Mild Cognitive Impairment" Brain Sciences 13, no. 2: 367. https://doi.org/10.3390/brainsci13020367