
Neurocognitive Deficits in First-Episode and Chronic Psychotic Disorders: A Systematic Review from 2009 to 2022
Abstract
:1. Introduction
2. Methods
2.1. Pre-Registration
2.2. Inclusion Criteria
2.3. Data Sources and Search Terms
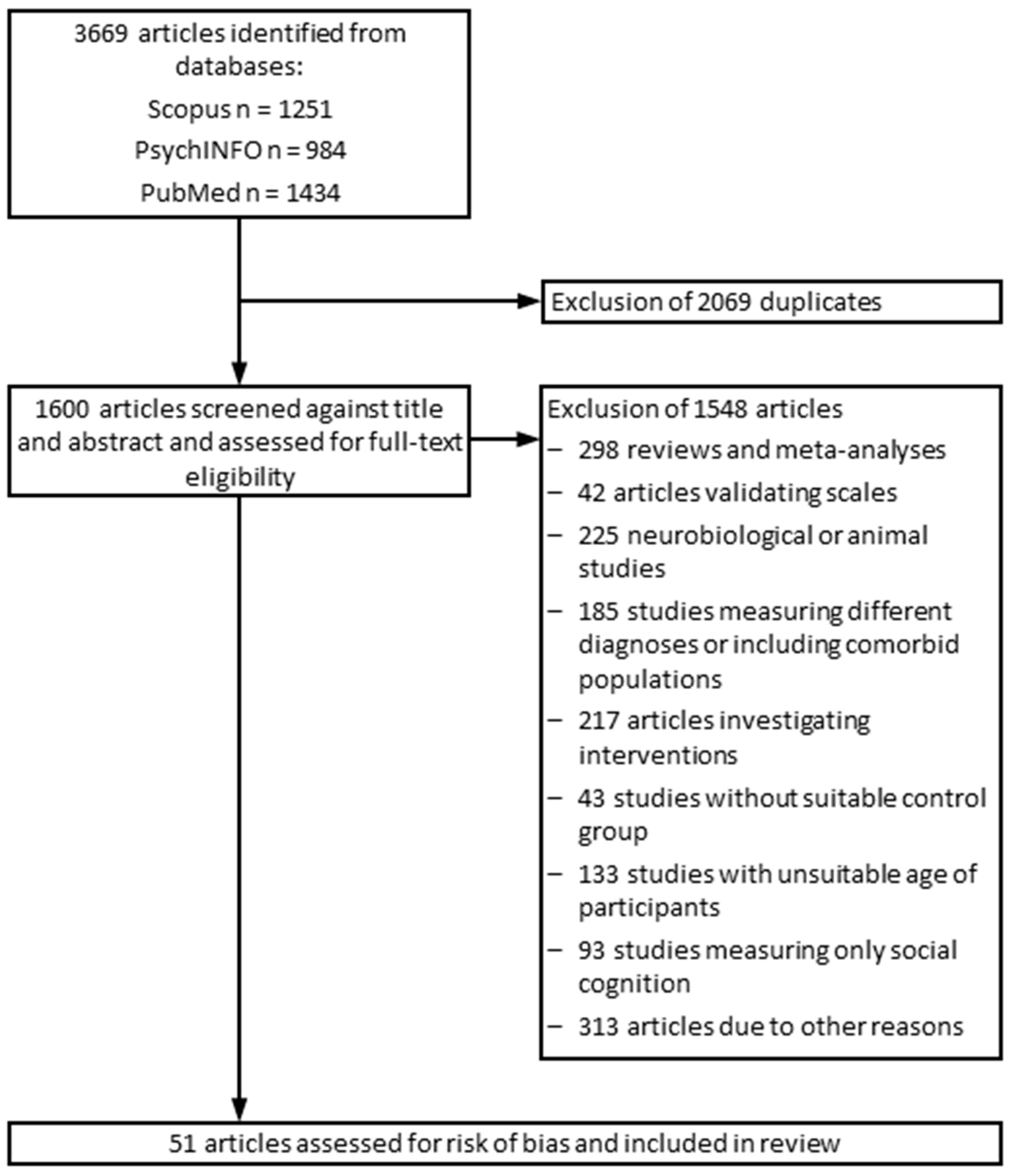
2.4. Study Selection and Data Extraction
2.5. Risk of Bias Assessment
2.6. Synthesis of Study Outcomes
3. Results
3.1. Included Studies and Clinical Subgroups
- (1)
- chronic schizophrenia (CHS);
- (2)
- deficit chronic schizophrenia with stable negative symptoms (CHS-D);
- (3)
- non-deficit chronic schizophrenia (CHS-ND);
- (4)
- chronic schizophrenia treatment non-responders (CHS-NR);
- (5)
- chronic schizophrenia treatment partial responders (CHS-PR);
- (6)
- chronic schizophrenia without motor retardation (CHS-NMR);
- (7)
- chronic schizophrenia with motor retardation (CHS-MR);
- (8)
- chronic schizophrenia without oxidative stress (CHS-NOS);
- (9)
- chronic schizophrenia with oxidative stress (CHS-OS);
- (10)
- high risk of psychotic disorders (HRP);
- (11)
- early stages of high risk for psychotic disorders (HRP-early);
- (12)
- late stages of high risk of psychotic disorders (HRP-late);
- (13)
- first-episode psychotic disorder (FEP);
- (14)
- first-episode schizophrenia (FES);
- (15)
- non-remitted first-episode schizophrenia (FES-NR);
- (16)
- remitted first-episode schizophrenia (FES-R);
- (17)
- schizophrenic patients (SZ).
3.2. Risk of Bias Assessment
3.3. Cognitive Performance of Patient Groups vs. Healthy Control Groups
3.4. Cognitive Performance of First-Episode vs. Chronically Affected Patients
3.5. Cognitive Profiles of High-Risk Patients
3.6. Siblings of First-Episode Patients
4. Discussion
4.1. The Global Deficit Hypothesis
4.2. The Longitudinal Stability Hypothesis
4.3. Limitations and Recommendations to Lower the Risk of Bias in Future Studies
4.4. Recommendations for the Clinical Treatment of Patients with Psychotic Disorders
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Heinrichs, R.W.; Zakzanis, K.K. Neurocognitive deficit in schizophrenia: A quantitative review of the evidence. Neuropsychology 1998, 12, 426–445. [Google Scholar] [CrossRef] [PubMed]
- Mesholam-Gately, R.I.; Giuliano, A.J.; Goff, K.P.; Faraone, S.V.; Seidman, L.J. Neurocognition in first-episode schizophrenia: A meta-analytic review. Neuropsychology 2009, 23, 315–336. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, J.; Giangrande, E.; Weinberger, D.R.; Dickinson, D. The global cognitive impairment in schizophrenia: Consistent over decades and around the world. Schizophr. Res. 2013, 150, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Catalan, A.; Salazar de Pablo, G.; Aymerich, C.; Damiani, S.; Sordi, V.; Radua, J.; Oliver, D.; McGuire, P.; Giuliano, A.J.; Stone, W.S.; et al. Neurocognitive Functioning in Individuals at Clinical High Risk for Psychosis: A Systematic Review and Meta-analysis. JAMA Psychiatry 2021, 78, 859–867. [Google Scholar] [CrossRef] [PubMed]
- Sheffield, J.M.; Karcher, N.R.; Barch, D.M. Cognitive Deficits in Psychotic Disorders: A Lifespan Perspective. Neuropsychol. Rev. 2018, 28, 509–533. [Google Scholar] [CrossRef] [PubMed]
- Green, M.F.; Schooler, N.R.; Kern, R.S.; Frese, F.J.; Granberry, W.; Harvey, P.D.; Karson, C.N.; Peters, N.; Stewart, M.; Seidman, L.J.; et al. Evaluation of functionally meaningful measures for clinical trials of cognition enhancement in schizophrenia. Am. J. Psychiatry 2011, 168, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Harvey, P.D. What is the evidence for changes in cognition and functioning over the lifespan in patients with schizophrenia? J. Clin. Psychiatry 2014, 75, 34–38. [Google Scholar] [CrossRef]
- Bora, E. Neurodevelopmental origin of cognitive impairment in schizophrenia. Psychol. Med. 2015, 45, 1–9. [Google Scholar] [CrossRef]
- Owen, M.J.; O’Donovan, M.C.; Thapar, A.; Craddock, N. Neurodevelopmental hypothesis of schizophrenia. Br. J. Psychiatry 2018, 198, 173–175. [Google Scholar] [CrossRef]
- Rapoport, J.L.; Giedd, J.N.; Gogtay, N. Neurodevelopmental model of schizophrenia: Update 2012. Mol. Psychiatry 2012, 17, 1228–1238. [Google Scholar] [CrossRef] [Green Version]
- Woodberry, K.A.; Giuliano, A.J.; Seidman, L.J. Premorbid IQ in schizophrenia: A meta-analytic review. Am. J. Psychiatry 2008, 165, 579–587. [Google Scholar] [CrossRef] [PubMed]
- Menkes, M.W.; Armstrong, K.; Blackford, J.U.; Heckers, S.; Woodward, N.D. Neuropsychological functioning in early and chronic stages of schizophrenia and psychotic bipolar disorder. Schizophr. Res. 2019, 206, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Kiraz, S.; Demir, E. Global Scientific Outputs of Schizophrenia Publications from 1975 to 2020: A Bibliometric Analysis. Psychiatr. Q. 2021, 92, 1725–1744. [Google Scholar] [CrossRef]
- Fioravanti, M.; Bianchi, V.; Cinti, M.E. Cognitive deficits in schizophrenia: An updated metanalysis of the scientific evidence. BMC Psychiatry 2012, 12, 64. [Google Scholar] [CrossRef] [PubMed]
- Allott, K.; Liu, P.; Proffitt, T.M.; Killackey, E. Cognition at illness onset as a predictor of later functional outcome in early psychosis: Systematic review and methodological critique. Schizophr. Res. 2011, 125, 221–235. [Google Scholar] [CrossRef] [PubMed]
- Fett, A.-K.J.; Reichenberg, A.; Velthorst, E. Lifespan evolution of neurocognitive impairment in schizophrenia—A narrative review. Schizophr. Res. Cogn. 2022, 28, 100237. [Google Scholar] [CrossRef] [PubMed]
- McCleery, A.; Nuechterlein, K.H. Cognitive impairment in psychotic illness: Prevalence, profile of impairment, developmental course, and treatment considerations. Dialogues Clin. Neurosci. 2019, 21, 239–248. [Google Scholar] [CrossRef]
- Koutsouleris, N.; Davatzikos, C.; Borgwardt, S.; Gaser, C.; Bottlender, R.; Frodl, T.; Falkai, P.; Riecher-Rössler, A.; Möller, H.J.; Reiser, M.; et al. Accelerated brain aging in schizophrenia and beyond: A neuroanatomical marker of psychiatric disorders. Schizophr. Bull. 2014, 40, 1140–1153. [Google Scholar] [CrossRef]
- Kirkpatrick, B.; Messias, E.; Harvey, P.D.; Fernandez-Egea, E.; Bowie, C.R. Is schizophrenia a syndrome of accelerated aging? Schizophr. Bull. 2008, 34, 1024–1032. [Google Scholar] [CrossRef]
- Fatouros-Bergman, H.; Cervenka, S.; Flyckt, L.; Edman, G.; Farde, L. Meta-analysis of cognitive performance in drug-naïve patients with schizophrenia. Schizophr. Res. 2014, 158, 156–162. [Google Scholar] [CrossRef] [Green Version]
- Fett, A.K.J.; Velthorst, E.; Reichenberg, A.; Ruggero, C.J.; Callahan, J.L.; Fochtmann, L.J.; Carlson, G.A.; Perlman, G.; Bromet, E.J.; Kotov, R. Long-term Changes in Cognitive Functioning in Individuals with Psychotic Disorders: Findings from the Suffolk County Mental Health Project. JAMA Psychiatry 2019, 77, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Nuechterlein, K.H.; Green, M.F.; Kern, R.S.; Baade, L.E.; Barch, D.M.; Cohen, J.D.; Essock, S.; Fenton, W.S.; Frese, F.J., 3rd; Gold, J.M.; et al. The MATRICS Consensus Cognitive Battery, part 1: Test selection, reliability, and validity. Am. J. Psychiatry 2008, 165, 203–213. [Google Scholar] [CrossRef]
- Al-Dujaili, A.H.; Mousa, R.F.; Al-Hakeim, H.K.; Maes, M. High Mobility Group Protein 1 and Dickkopf-Related Protein 1 in Schizophrenia and Treatment-Resistant Schizophrenia: Associations with Interleukin-6, Symptom Domains, and Neurocognitive Impairments. Schizophr. Bull. 2021, 47, 530–541. [Google Scholar] [CrossRef]
- Al-Hakeim, H.K.; Almulla, A.F.; Maes, M. The Neuroimmune and Neurotoxic Fingerprint of Major Neurocognitive Psychosis or Deficit Schizophrenia: A Supervised Machine Learning Study. Neurotox. Res. 2020, 37, 753–771. [Google Scholar] [CrossRef]
- Beck, K.I.; Simonsen, A.; Wang, H.; Yang, L.; Zhou, Y.; Bliksted, V. Cross-cultural comparison of theory of mind deficits in patients with schizophrenia from China and Denmark: Different aspects of ToM show different results. Nord. J. Psychiatry 2020, 74, 366–373. [Google Scholar] [CrossRef]
- Bliksted, V.; Fagerlund, B.; Weed, E.; Frith, C.; Videbech, P. Social cognition and neurocognitive deficits in first-episode schizophrenia. Schizophr. Res. 2014, 153, 9–17. [Google Scholar] [CrossRef]
- Bosnjak Kuharic, D.; Makaric, P.; Kekin, I.; Rossini Gajsak, L.; Zivkovic, M.; Ostojic, D.; Silic, A.; Bajic, Z.; Lukacevic Lovrencic, I.; Beezhold, J.; et al. Changes of neurocognitive status in patients with the first-episode psychosis after 18 months of treatment-A prospective cohort study. Psychiatry Res. 2021, 304, 114131. [Google Scholar] [CrossRef]
- Chattopadhyay, S.; Patil, N.M.; Nayak, R.B.; Chate, S.S.; Singh, O.P. Neurocognitive Profile in Indian Individuals Genetically at Risk of Schizophrenia. Indian J. Psychol. Med. 2020, 42, 155–161. [Google Scholar] [CrossRef]
- Chen, S.; Tian, L.; Chen, N.; Xiu, M.H.; Wang, Z.R.; Wang, Y.C.; Tan, Y.L.; Wang, C.Y. More dampened monocytic Toll-like receptor 4 response to lipopolysaccharide and its association with cognitive function in Chinese Han first-episode patients with schizophrenia. Schizophr. Res. 2019, 206, 300–306. [Google Scholar] [CrossRef]
- Chen, S.; Liu, Y.; Liu, D.; Zhang, G.; Wu, X. The difference of social cognitive and neurocognitive performance between patients with schizophrenia at different stages and influencing factors. Schizophr. Res. Cogn. 2021, 24, 100195. [Google Scholar] [CrossRef] [PubMed]
- Correa-Ghisays, P.; Sánchez-Ortí, J.V.; Balanzá-Martínez, V.; Selva-Vera, G.; Vila-Francés, J.; Magdalena-Benedito, R.; Victor, V.M.; Escribano-López, I.; Hernández-Mijares, A.; Vivas-Lalinde, J.; et al. Transdiagnostic neurocognitive deficits in patients with type 2 diabetes mellitus, major depressive disorder, bipolar disorder, and schizophrenia: A 1-year follow-up study. J. Affect. Disord. 2022, 300, 99–108. [Google Scholar] [CrossRef]
- Cuesta, M.J.; Moreno-Izco, L.; Ribeiro, M.; López-Ilundain, J.M.; Lecumberri, P.; Cabada, T.; Lorente-Omeñaca, R.; Sánchez-Torres, A.M.; Gómez, M.S.; Peralta, V. Motor abnormalities and cognitive impairment in first-episode psychosis patients, their unaffected siblings and healthy controls. Schizophr. Res. 2018, 200, 50–55. [Google Scholar] [CrossRef] [PubMed]
- da Motta, C.; Pato, M.T.; Barreto Carvalho, C.; Castilho, P. The neurocognitive and functional profile of schizophrenia in a genetically homogenous European sample. Psychiatry Res. 2021, 304, 114140. [Google Scholar] [CrossRef] [PubMed]
- De la Torre, G.G.; Doval, S.; López-Sanz, D.; García-Sedeño, M.; Ramallo, M.A.; Bernal, M.; González-Torre, S. Neurocognitive Impairment in Severe Mental Illness. Comparative study with Spanish Speaking Patients. Brain Sci. 2021, 11, 389. [Google Scholar] [CrossRef]
- Eisenacher, S.; Rausch, F.; Ainser, F.; Englisch, S.; Becker, A.; Mier, D.; Fenske, S.; Meyer-Lindenberg, A.; Kirsch, P.; Zink, M. Early cognitive basic symptoms are accompanied by neurocognitive impairment in patients with an ‘at-risk mental state’ for psychosis. Early Interv. Psychiatry 2018, 12, 586–595. [Google Scholar] [CrossRef]
- Ferretjans, R.; de Souza, R.P.; Panizzutti, B.; Ferrari, P.; Mantovani, L.; de Campos-Carli, S.M.; Santos, R.R.; Guimarães, F.C.; Teixeira, A.L.; Gama, C.S.; et al. Cannabinoid receptor gene polymorphisms and cognitive performance in patients with schizophrenia and controls. Rev. Bras. De Psiquiatr. 2022, 44, 26–34. [Google Scholar] [CrossRef]
- Frommann, I.; Pukrop, R.; Brinkmeyer, J.; Bechdolf, A.; Ruhrmann, S.; Berning, J.; Decker, P.; Riedel, M.; Möller, H.J.; Wölwer, W.; et al. Neuropsychological profiles in different at-risk states of psychosis: Executive control impairment in the early- and additional memory dysfunction in the late-prodromal state. Schizophr. Bull. 2011, 37, 861–873. [Google Scholar] [CrossRef]
- Giordano, G.M.; Perrottelli, A.; Mucci, A.; Di Lorenzo, G.; Altamura, M.; Bellomo, A.; Brugnoli, R.; Corrivetti, G.; Girardi, P.; Monteleone, P.; et al. Investigating the Relationships of P3b with Negative Symptoms and Neurocognition in Subjects with Chronic Schizophrenia. Brain Sci. 2021, 11, 1632. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Li, J.; Wang, J.; Fan, X.; Hu, M.; Shen, Y.; Chen, H.; Zhao, J. Hippocampal and orbital inferior frontal gray matter volume abnormalities and cognitive deficit in treatment-naive, first-episode patients with schizophrenia. Schizophr. Res. 2014, 152, 339–343. [Google Scholar] [CrossRef] [PubMed]
- Hájková, M.; Knížková, K.; Siroňová, A.; Keřková, B.; Jonáš, J.; Šustová, P.; Dorazilová, A.; Rodriguez, M. Cognitive performance and lifetime cannabis use in patients with first-episode schizophrenia spectrum disorder. Cogn. Neuropsychiatry 2021, 26, 257–272. [Google Scholar] [CrossRef]
- He, Z.; Deng, W.; Li, M.; Chen, Z.; Jiang, L.; Wang, Q.; Huang, C.; Collier, D.A.; Gong, Q.; Ma, X.; et al. Aberrant intrinsic brain activity and cognitive deficit in first-episode treatment-naive patients with schizophrenia. Psychol. Med. 2013, 43, 769–780. [Google Scholar] [CrossRef]
- Konstantakopoulos, G.; Ioannidi, N.; Psarros, C.; Patrikelis, P.; Stefanatou, P.; Kravariti, E. The impact of neurocognition on mentalizing in euthymic bipolar disorder versus schizophrenia. Cogn. Neuropsychiatry 2020, 25, 405–420. [Google Scholar] [CrossRef]
- Koshiyama, D.; Miyakoshi, M.; Thomas, M.L.; Joshi, Y.B.; Molina, J.L.; Tanaka-Koshiyama, K.; Sprock, J.; Braff, D.L.; Swerdlow, N.R.; Light, G.A. Unique contributions of sensory discrimination and gamma synchronization deficits to cognitive, clinical, and psychosocial functional impairments in schizophrenia. Schizophr. Res. 2021, 228, 280–287. [Google Scholar] [CrossRef]
- Li, R.R.; Lyu, H.L.; Liu, F.; Lian, N.; Wu, R.R.; Zhao, J.P.; Guo, W.B. Altered functional connectivity strength and its correlations with cognitive function in subjects with ultra-high risk for psychosis at rest. CNS Neurosci. Ther. 2018, 24, 1140–1148. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, G.; Jin, H.; Lyu, H.; Liu, Y.; Guo, W.; Shi, C.; Meyers, J.; Wang, J.; Zhao, J.; et al. Cognitive deficits in subjects at risk for psychosis, first-episode and chronic schizophrenia patients. Psychiatry Res. 2019, 274, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Bi, T.; Zhang, B.; Kuang, Q.; Li, H.; Zong, K.; Zhao, J.; Ning, Y.; She, S.; Zheng, Y. Face and object visual working memory deficits in first-episode schizophrenia correlate with multiple neurocognitive performances. Gen. Psychiatr. 2021, 34, e100338. [Google Scholar] [CrossRef]
- Maes, M.; Sirivichayakul, S.; Kanchanatawan, B.; Carvalho, A.F. In schizophrenia, psychomotor retardation is associated with executive and memory impairments, negative and psychotic symptoms, neurotoxic immune products and lower natural IgM to malondialdehyde. World J. Biol. Psychiatry Off. J. World Fed. Soc. Biol. Psychiatry 2020, 21, 383–401. [Google Scholar] [CrossRef]
- Maes, M.; Sirivichayakul, S.; Matsumoto, A.K.; Michelin, A.P.; de Oliveira Semeão, L.; de Lima Pedrão, J.V.; Moreira, E.G.; Barbosa, D.S.; Carvalho, A.F.; Solmi, M.; et al. Lowered Antioxidant Defenses and Increased Oxidative Toxicity Are Hallmarks of Deficit Schizophrenia: A Nomothetic Network Psychiatry Approach. Mol. Neurobiol. 2020, 57, 4578–4597. [Google Scholar] [CrossRef] [PubMed]
- Maes, M.; Kanchanatawan, B. In (deficit) schizophrenia, a general cognitive decline partly mediates the effects of neuro-immune and neuro-oxidative toxicity on the symptomatome and quality of life. CNS Spectr. 2021, 27, 506–515. [Google Scholar] [CrossRef] [PubMed]
- Mançe Çalışır, Ö.; Atbaşoğlu, E.C.; Devrimci Özgüven, H.; Ölmez, Ş. Cognitive Features of High-functioning Adults with Autism and Schizophrenia Spectrum Disorders. Turk Psikiyatr. Derg (Turk. J. Psychiatry) 2018, 29, 1–10. [Google Scholar]
- McDonald, M.; Christoforidou, E.; Van Rijsbergen, N.; Gajwani, R.; Gross, J.; Gumley, A.I.; Lawrie, S.M.; Schwannauer, M.; Schultze-Lutter, F.; Uhlhaas, P.J. Using Online Screening in the General Population to Detect Participants at Clinical High-Risk for Psychosis. Schizophr. Bull. 2019, 45, 600–609. [Google Scholar] [CrossRef]
- Morales-Muñoz, I.; Jurado-Barba, R.; Fernández-Guinea, S.; Álvarez-Alonso, M.J.; Rodríguez-Jiménez, R.; Jiménez-Arriero, M.A.; Rubio, G. Cognitive impairments in patients with first episode psychosis: The relationship between neurophysiological and neuropsychological assessments. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas. 2017, 36, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Ngoma, M.; Vansteelandt, K.; Delespaul, P.; Krabbendam, L.; Miezi, S.M.; Peuskens, J. Cognitive deficits in nonaffective functional psychoses: A study in the Democratic Republic of Congo. Psychiatry Res. 2010, 180, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Randers, L.; Jepsen, J.R.M.; Fagerlund, B.; Nordholm, D.; Krakauer, K.; Hjorthøj, C.; Glenthøj, B.; Nordentoft, M. Generalized neurocognitive impairment in individuals at ultra-high risk for psychosis: The possible key role of slowed processing speed. Brain Behav. 2021, 11, e01962. [Google Scholar] [CrossRef]
- Saleem, M.M.; Harte, M.K.; Marshall, K.M.; Scally, A.; Brewin, A.; Neill, J.C. First episode psychosis patients show impaired cognitive function—A study of a South Asian population in the UK. J. Psychopharmacol. 2013, 27, 366–373. [Google Scholar] [CrossRef]
- Service, S.K.; Vargas Upegui, C.; Castaño Ramírez, M.; Port, A.M.; Moore, T.M.; Munoz Umanes, M.; Agudelo Arango, L.G.; Díaz-Zuluaga, A.M.; Melo Espejo, J.; López, M.C.; et al. Distinct and shared contributions of diagnosis and symptom domains to cognitive performance in severe mental illness in the Paisa population: A case-control study. Lancet Psychiatry 2020, 7, 411–419. [Google Scholar] [CrossRef]
- Shi, C.; Kang, L.; Yao, S.; Ma, Y.; Li, T.; Liang, Y.; Cheng, Z.; Xu, Y.; Shi, J.; Xu, X.; et al. What is the optimal neuropsychological test battery for schizophrenia in China? Schizophr. Res. 2019, 208, 317–323. [Google Scholar] [CrossRef]
- Tang, X.; Zhou, C.; Gao, J.; Duan, W.; Yu, M.; Xiao, W.; Zhang, X.; Dong, H.; Wang, X.; Zhang, X. Serum BDNF and GDNF in Chinese male patients with deficit schizophrenia and their relationships with neurocognitive dysfunction. BMC Psychiatry 2019, 19, 254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vignapiano, A.; Koenig, T.; Mucci, A.; Giordano, G.M.; Amodio, A.; Altamura, M.; Bellomo, A.; Brugnoli, R.; Corrivetti, G.; Di Lorenzo, G.; et al. Disorganization and cognitive impairment in schizophrenia: New insights from electrophysiological findings. Int. J. Psychophysiol. 2019, 145, 99–108. [Google Scholar] [CrossRef]
- Wang, M.Y.; Ho, N.F.; Sum, M.Y.; Collinson, S.L.; Sim, K. Impact of duration of untreated psychosis and premorbid intelligence on cognitive functioning in patients with first-episode schizophrenia. Schizophr. Res. 2016, 175, 97–102. [Google Scholar] [CrossRef]
- Wu, J.Q.; Chen, D.C.; Tan, Y.L.; Xiu, M.H.; De Yang, F.; Soares, J.C.; Zhang, X.Y. Cognitive impairments in first-episode drug-naive and chronic medicated schizophrenia: MATRICS consensus cognitive battery in a Chinese Han population. Psychiatry Res. 2016, 238, 196–202. [Google Scholar] [CrossRef]
- Xiao, W.; Ye, F.; Liu, C.; Tang, X.; Li, J.; Dong, H.; Sha, W.; Zhang, X. Cognitive impairment in first-episode drug-naïve patients with schizophrenia: Relationships with serum concentrations of brain-derived neurotrophic factor and glial cell line-derived neurotrophic factor. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2017, 76, 163–168. [Google Scholar] [CrossRef]
- Xiu, M.-H.; Wang, D.; Chen, S.; Du, X.-D.; Chen, D.-C.; Chen, N.; Wang, Y.-C.; Yin, G.; Zhang, Y.; Tan, Y.-L.; et al. Interleukin-3, symptoms and cognitive deficits in first-episode drug-naïve and chronic medicated schizophrenia. Psychiatry Res. 2018, 263, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.J.; Xiong, J.W.; Zhao, Y.; Zhan, J.Q.; Chen, H.B.; Yan, K.; Hu, M.R.; Yu, B.; Wei, B. Increased plasma asymmetric dimethylarginine is associated with cognitive deficits in patients with schizophrenia. Psychiatry Res. 2016, 246, 480–484. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Liu, Y.; Wang, G.; Hei, G.; Wang, X.; Li, R.; Li, L.; Wu, R.; Zhao, J. Brain-derived neurotrophic factor is associated with cognitive impairments in first-episode and chronic schizophrenia. Psychiatry Res. 2019, 273, 528–536. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.J.; Luo, T.; Zhao, Y.; Jiang, S.Z.; Xiong, J.W.; Zhan, J.Q.; Yu, B.; Yan, K.; Wei, B. Altered insulin-like growth factor-2 signaling is associated with psychopathology and cognitive deficits in patients with schizophrenia. PLoS ONE 2020, 15, e0226688. [Google Scholar] [CrossRef]
- Zhang, X.Y.; Tang, W.; Xiu, M.H.; Chen, D.C.; Yang, F.D.; Tan, Y.L.; Wang, Z.R.; Zhang, F.; Liu, J.; Liu, L.; et al. Interleukin 18 and cognitive impairment in first episode and drug naïve schizophrenia versus healthy controls. Brain Behav. Immun. 2013, 32, 105–111. [Google Scholar] [CrossRef]
- Zhang, X.; Yao, J.; Lv, Y.; Zhao, X.; Li, Y.; Sui, Y.; Zhiping, D. An Association Study on the Cognitive Function and the Cerebral Grey Matter Volume of Patients with First-Episode Schizophrenia. Shanghai Arch. Psychiatry 2018, 30, 154–167. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Xiao, W.; Chen, K.; Zhan, Q.; Ye, F.; Tang, X.; Zhang, X. Neurocognition and social cognition in remitted first-episode schizophrenia: Correlation with VEGF serum levels. BMC Psychiatry 2019, 19, 403. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Tang, X.; You, W.; Wang, X.; Zhang, X.; Zhang, X.; Yu, M. Altered Patterns of the Fractional Amplitude of Low-Frequency Fluctuation and Functional Connectivity between Deficit and Non-Deficit Schizophrenia. Front Psychiatry 2019, 10, 680. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Yu, M.; Tang, X.; Wang, X.; Zhang, X.; Zhang, X.; Chen, J. Convergent and divergent altered patterns of default mode network in deficit and non-deficit schizophrenia. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2019, 89, 427–434. [Google Scholar] [CrossRef]
- Zhou, C.; Xue, C.; Chen, J.; Amdanee, N.; Tang, X.; Zhang, H.; Zhang, F.; Zhang, X.; Zhang, C. Altered Functional Connectivity of the Nucleus Accumbens Network between Deficit and Non-deficit Schizophrenia. Front. Psychiatry 2021, 12, 704631. [Google Scholar] [CrossRef]
- Zong, X.; Zhang, Q.; He, C.; Huang, X.; Zhang, J.; Wang, G.; Lv, L.; Sang, D.; Zou, X.; Chen, H.; et al. DNA Methylation Basis in the Effect of White Matter Integrity Deficits on Cognitive Impairments and Psychopathological Symptoms in Drug-Naive First-Episode Schizophrenia. Front Psychiatry 2021, 12, 777407. [Google Scholar] [CrossRef]
- Knytl, P.; Voráčková, V.; Dorazilová, A.; Rodriguez, M.; Cvrčková, A.; Kofroňová, E.; Kuchař, M.; Kratochvílová, Z.; Šustová, P.; Čerešňáková, S.; et al. Neuroactive Steroids and Cognitive Functions in First-Episode Psychosis Patients and Their Healthy Siblings. Front. Psychiatry 2019, 10, 390. [Google Scholar] [CrossRef]
- Zhang, H.; Wang, Y.; Hu, Y.; Zhu, Y.; Zhang, T.; Wang, J.; Ma, K.; Shi, C.; Yu, X.; Li, C. Meta-analysis of cognitive function in Chinese first-episode schizophrenia: MATRICS Consensus Cognitive Battery (MCCB) profile of impairment. Gen. Psychiatr. 2019, 32, e100043. [Google Scholar] [CrossRef]
- Kwok, S.C.; Xu, X.; Duan, W.; Wang, X.; Tang, Y.; Allé, M.C.; Berna, F. Autobiographical and episodic memory deficits in schizophrenia: A narrative review and proposed agenda for research. Clin. Psychol. Rev. 2021, 83, 101956. [Google Scholar] [CrossRef]
- Seabury, R.D.; Cannon, T.D. Memory Impairments and Psychosis Prediction: A Scoping Review and Theoretical Overview. Neuropsychol. Rev. 2020, 30, 521–545. [Google Scholar] [CrossRef]
- Dickinson, D.; Harvey, P.D. Systemic hypotheses for generalized cognitive deficits in schizophrenia: A new take on an old problem. Schizophr. Bull. 2009, 35, 403–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roca, M.; Vives, M.; López-Navarro, E.; García-Campayo, J.; Gili, M. Cognitive impairments and depression: A critical review. Actas Esp. Psiquiatr. 2015, 43, 187–193. [Google Scholar]
- Cullen, B.; Ward, J.; Graham, N.A.; Deary, I.J.; Pell, J.P.; Smith, D.J.; Evans, J.J. Prevalence and correlates of cognitive impairment in euthymic adults with bipolar disorder: A systematic review. J. Affect. Disord. 2016, 205, 165–181. [Google Scholar] [CrossRef] [PubMed]
- Kriesche, D.; Woll, C.F.J.; Tschentscher, N.; Engel, R.R.; Karch, S. Neurocognitive deficits in depression: A systematic review of cognitive impairment in the acute and remitted state. Eur. Arch. Psychiatry Clin. Neurosci. 2022; in press. [Google Scholar] [CrossRef]
- Rund, B.R.; Barder, H.E.; Evensen, J.; Haahr, U.; ten Velden Hegelstad, W.; Joa, I.; Johannessen, J.O.; Langeveld, J.; Larsen, T.K.; Melle, I.; et al. Neurocognition and Duration of Psychosis: A 10-year Follow-up of First-Episode Patients. Schizophr. Bull. 2016, 42, 87–95. [Google Scholar] [CrossRef]
- Bergh, S.; Hjorthøj, C.; Sørensen, H.J.; Fagerlund, B.; Austin, S.; Secher, R.G.; Jepsen, J.R.; Nordentoft, M. Predictors and longitudinal course of cognitive functioning in schizophrenia spectrum disorders, 10 years after baseline: The OPUS study. Schizophr. Res. 2016, 175, 57–63. [Google Scholar] [CrossRef]
- Sánchez-Torres, A.M.; Moreno-Izco, L.; Lorente-Omeñaca, R.; Cabrera, B.; Lobo, A.; González-Pinto, A.M.; Merchán-Naranjo, J.; Corripio, I.; Vieta, E.; de la Serna, E.; et al. Individual trajectories of cognitive performance in first episode psychosis: A 2-year follow-up study. Eur. Arch. Psychiatry Clin. Neurosci. 2018, 268, 699–711. [Google Scholar] [CrossRef]
- Barder, H.E.; Sundet, K.; Rund, B.R.; Evensen, J.; Haahr, U.; Ten Velden Hegelstad, W.; Joa, I.; Johannessen, J.O.; Langeveld, J.; Larsen, T.K.; et al. Ten year neurocognitive trajectories in first-episode psychosis. Front. Hum. Neurosci. 2013, 7, 643. [Google Scholar] [CrossRef]
- Zanelli, J.; Mollon, J.; Sandin, S.; Morgan, C.; Dazzan, P.; Pilecka, I.; Reis Marques, T.; David, A.S.; Morgan, K.; Fearon, P.; et al. Cognitive Change in Schizophrenia and Other Psychoses in the Decade Following the First Episode. Am. J. Psychiatry 2019, 176, 811–819. [Google Scholar] [CrossRef]
- Jeste, S.D.; Patterson, T.L.; Palmer, B.W.; Dolder, C.R.; Goldman, S.; Jeste, D.V. Cognitive predictors of medication adherence among middle-aged and older outpatients with schizophrenia. Schizophr. Res. 2003, 63, 49–58. [Google Scholar] [CrossRef]
- Settem, V.; Karanadi, H.; Praharaj, S. Cognitive deficits, depressive symptoms, insight, and medication adherence in remitted patients with schizophrenia. Indian J. Psychiatry 2019, 61, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Bowie, C.R.; Harvey, P.D. Cognitive deficits and functional outcome in schizophrenia. Neuropsychiatr. Dis. Treat. 2006, 2, 531–536. [Google Scholar] [CrossRef] [Green Version]
- Sinkeviciute, I.; Begemann, M.; Prikken, M.; Oranje, B.; Johnsen, E.; Lei, W.U.; Hugdahl, K.; Kroken, R.A.; Rau, C.; Jacobs, J.D.; et al. Efficacy of different types of cognitive enhancers for patients with schizophrenia: A meta-analysis. NPJ Schizophr. 2018, 4, 22. [Google Scholar] [CrossRef] [PubMed]
- Allott, K.; van-der-El, K.; Bryce, S.; Parrish, E.M.; McGurk, S.R.; Hetrick, S.; Bowie, C.R.; Kidd, S.; Hamilton, M.; Killackey, E.; et al. Compensatory Interventions for Cognitive Impairments in Psychosis: A Systematic Review and Meta-Analysis. Schizophr. Bull. 2020, 46, 869–883. [Google Scholar] [CrossRef]
- Kidd, S.A.; Herman, Y.; Virdee, G.; Bowie, C.R.; Velligan, D.; Plagiannakos, C.; Voineskos, A. A comparison of compensatory and restorative cognitive interventions in early psychosis. Schizophr. Res. Cogn. 2020, 19, 100157. [Google Scholar] [CrossRef]
- Vita, A.; Gaebel, W.; Mucci, A.; Sachs, G.; Erfurth, A.; Barlati, S.; Zanca, F.; Giordano, G.M.; Birkedal Glenthøj, L.; Nordentoft, M.; et al. European Psychiatric Association guidance on assessment of cognitive impairment in schizophrenia. Eur. Psychiatry 2022, 65, e58. [Google Scholar] [CrossRef]
- Hasan, A.; Falkai, P.; Lehmann, I.; Janssen, B.; Wobrock, T.; Zielasek, J.; Gaebel, W. Revised S3 guidelines on schizophrenia: Developmental process and selected recommendations. Nervenarzt 2020, 91, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Rossiter, R.; Holmes, S. Access all areas: Creative adaptations for CBT with people with cognitive impairments—Illustrations and issues. Cogn. Behav. Ther. 2013, 6, e9. [Google Scholar] [CrossRef]
- Gallagher, M.; McLeod, H.J.; McMillan, T.M. A systematic review of recommended modifications of CBT for people with cognitive impairments following brain injury. Neuropsychol. Rehabil. 2019, 29, 1–21. [Google Scholar] [CrossRef]


{kind=link}
| First Author, Year | Selection Bias | Clear Diagnostics | Blinding (Patients) | Detection Bias | Incomplete Outcome Data Addressed | Free of Selective Reporting | Summary Assessment |
|---|---|---|---|---|---|---|---|
| Al-Dujaili [2021] | − | + | ? | + | ? | + | − |
| Al-Hakeim [2020] | − | + | ? | + | + | + | − |
| Beck [2020] | + | ? | ? | ? | + | + | ? |
| Bliksted [2014] | + | ? | ? | ? | + | + | ? |
| Bosnjak Kuharic [2021] | − | ? | − | ? | ? | + | − |
| Chattopadhyay [2020] | − | + | ? | ? | + | + | − |
| Chen [2019] | ? | ? | ? | ? | + | + | ? |
| Chen 2021 | − | + | ? | ? | + | + | − |
| Correa-Ghisays [2021] | − | ? | ? | − | + | + | − |
| Cuesta [2018] | ? | ? | ? | + | + | + | ? |
| Da Motta [2021] | − | ? | − | + | + | + | − |
| De la Torre [2021] | + | ? | ? | ? | + | + | ? |
| Eisenacher [2018] | + | ? | ? | ? | + | + | ? |
| Ferretjans [2021] | − | ? | ? | ? | + | + | − |
| Frommann [2011] | + | ? | ? | ? | + | + | ? |
| Giordano [2021] | ? | ? | − | ? | + | + | − |
| Guo [2014] | + | ? | ? | ? | + | + | ? |
| Hájková [2021] | ? | + | ? | ? | + | + | ? |
| He [2013] | + | ? | ? | ? | + | + | ? |
| Konstantakopoulos [2020] | + | ? | ? | ? | + | + | ? |
| Koshiyama [2021] | − | ? | ? | ? | − | + | − |
| Li [2018] | ? | ? | ? | ? | + | + | ? |
| Liu [2019] | + | ? | ? | ? | + | + | ? |
| Liu [2021] | + | ? | ? | ? | ? | + | ? |
| Maes, Sirivichayakul, Kanchanatawan et al. [2020] | ? | + | ? | + | + | + | ? |
| Maes, Sirivichayakul, Matsumoto et al. [2020] | ? | + | ? | ? | + | + | ? |
| Maes [2021] | + | + | ? | ? | + | + | ? |
| Mançe ÇaliŞir [2018] | ? | ? | ? | ? | + | + | ? |
| McDonald [2019] | ? | ? | ? | ? | + | + | ? |
| Morales-Muñoz [2017] | ? | ? | ? | ? | + | + | ? |
| Ngoma [2010] | − | ? | ? | + | + | + | − |
| Randers [2021] | + | ? | ? | ? | + | + | ? |
| Saleem [2013] | + | ? | ? | ? | + | + | ? |
| Service [2021] | ? | ? | ? | + | + | + | ? |
| Shi [2019] | ? | ? | ? | ? | + | + | ? |
| Tang [2019] | ? | ? | ? | ? | + | + | ? |
| Vignapiano [2019] | + | ? | − | ? | + | + | − |
| Wang [2016] | ? | ? | − | ? | + | + | − |
| Wu [2016] | ? | ? | − | ? | + | + | − |
| Xiao [2017] | ? | ? | − | ? | + | + | − |
| Xiu [2018] | ? | ? | ? | ? | + | + | ? |
| Yang [2016] | + | + | ? | ? | + | + | ? |
| Yang [2019] | ? | + | ? | ? | + | + | ? |
| Yang [2020] | + | ? | ? | ? | + | + | ? |
| Zhang [2013] | + | ? | ? | ? | + | + | ? |
| Zhang [2018] | + | ? | ? | ? | + | + | ? |
| Zhao [2019] | + | ? | ? | + | + | + | ? |
| Zhou, Tang et al. [2019] | ? | ? | ? | ? | + | + | ? |
| Zhou, Yu et al. [2019] | ? | ? | ? | ? | + | + | ? |
| Zhou [2021] | ? | ? | ? | ? | + | + | ? |
| Zong [2021] | + | ? | ? | ? | + | + | ? |
| Cognitive Domain | Cognitive Subdomain | Tests |
|---|---|---|
| Attention and Vigilance | CANTAB: rapid visual information processing; CPT; CPT-IP; CTT-1; D2; digit span-forward; DVT; PennCNB: continuous performance test; RBANS: digit span; WMS-III: spatial span-forward | |
| Executive Function | Abstraction | PennCNB: conditional exclusion test; semantic similarities test; WAIS-III: similarities |
| Cognitive Flexibility | CANTAB: intra/extra dimensional set shift; CTT-2; design fluency; FAB; TMT-B, WCST/WCST64 | |
| Inhibition | SCWT: color–word subtest; TAP: go/no-go | |
| Planning | CANTAB: one touch stockings of Cambridge, stockings of Cambridge; ToH; ToL | |
| Reasoning and Problem Solving | Block design test; block diagram test; lPs:3, NAB: mazes; PennCNB: matrix reasoning test; spatial processing (block design); WAIS/WAIS-III/WAIS-RC: block design; WAIS-III: matrix reasoning, picture arrangement | |
| Language | Comprehension | WAIS/WAIS-III: comprehension |
| Naming | RBANS: picture naming | |
| Verbal Fluency | action (verb) fluency; ANT; BACS: verbal fluency; CFT: animal naming; COWAT; phonemic fluency test; RBANS: semantic fluency; semantic fluency test; verbal fluency; VFT | |
| Vocabulary | DART; MWT; vocabulary test; WAIS-III: vocabulary; WTAR | |
| Social Cognition | Animated triangles task; CANTAB: emotion recognition task; CFET; faux pas recognition test; hinting task; MSCEIT; PennCNB: emotion differentiation test, emotion recognition test; emotion discrimination task; TASIT | |
| Verbal Cognition | Verbal Learning | BACS: list learning; CVLT; HVLT-R; RAVLT/15WoR/AVLT; RBANS: list learning; TAVEC; VPA; WMS/WMS-III: logical memory/narrative memory |
| Verbal Memory | Babcock story recall test; CERAD: WLM, word list recall; PennCNB: word memory test; RBANS: list recall, list recognition, story memory, story recall | |
| Visuomotor Processing | BACS: token motor task, symbol coding; CANTAB: reaction time; DSST/WAIS: digit symbol/WAIS-III: digit symbol coding; FFT/FOT; grooved pegboard; PennCNB: finger tapping test; motor praxis test/mouse practice task; RBANS: coding; SCWT: color–word subtests; TMT-A; WAIS-III: symbol search | |
| Visuo-spatial Cognition | Visual Analysis and Construction | PennCNB: line orientation; RBANS: figure copy, line orientation; ROCFT |
| Visual Learning and Memory | BVMT-R; CANTAB: delayed matching to sample; paired associates learning; pattern recognition memory, spatial recognition memory; PennCNB: face memory; visual object learning test; PGI-visual recognition; RBANS: figure recall | |
| Working Memory | BACS: digit sequencing; CANTAB: spatial span, spatial working memory; CPT-OX; digit span-backward; LNS; PASAT/PASAT-50; PennCNB: letter n-back task; serial subtraction; SOPT; TAP: 2-back task; verbal n-back task; visual n-back task; WAIS/WAIS-III: arithmetic; digit span-backward; WMS-III: spatial span-backward |
| Author | Patient Groups (n) | Control Groups (n) | Cognitive Tests (Cognitive Domains) | Main Results |
|---|---|---|---|---|
| Al-Dujaili [26] | CHS-NR (60) CHS-PR (55) | HC (43) | BACS (planning, verbal fluency, verbal learning, visuomotor processing, working memory) | CHS-NR < CHS-PR < HC for planning, verbal fluency, verbal learning, visuomotor processing, working memory. |
| Al-Hakeim [27] | CHS (120) | HC (54) | BACS (planning, verbal fluency, verbal learning, visuomotor processing, working memory) | CHS < HC for planning, verbal fluency, verbal learning, visuomotor processing, working memory. |
| Beck [28] | CHS (66) | HC (67) | BACS (planning, verbal fluency, verbal learning, visuomotor processing, working memory); WAIS-III: block design (reasoning and problem solving), vocabulary (vocabulary) | CHS < HC for reasoning and problem solving, vocabulary, working memory. When controlled for nationality, CHS < HC for verbal fluency, verbal learning, visuomotor processing (token motor task). When controlled for nationality and the interaction between nationality and group, CHS < HC for visuomotor processing (symbol coding). When controlled for nationality and the interaction between nationality and group, CHS = HC for planning. |
| Bliksted [29] | FES (36) | HC (36) | Animated triangles task (social cognition); BACS (planning, verbal fluency, verbal learning, visuomotor processing, working memory); DART (vocabulary); hinting task (social cognition); TASIT (social cognition); WAIS-III: matrix reasoning (reasoning and problem solving), block design (reasoning and problem solving), vocabulary (vocabulary), similarities (abstraction) | FEP < HC for abstraction, reasoning and problem solving, social cognition, verbal fluency, verbal learning, visuomotor processing, vocabulary, working memory. |
| Bosnjak Kuharic [30] | FEP (129) | HC (100) | Block design test (reasoning and problem solving); digit span-forward (attention and vigilance), Backward (working memory); DSST (visuomotor processing); FAB (cognitive flexibility); phonemic fluency test (verbal fluency); RAVLT (verbal learning); ROCFT (visual analysis and construction); SCWT (visuomotor processing, inhibition); semantic fluency test (verbal fluency); TMT-A (visuomotor processing) TMT-B (cognitive flexibility); WMS-III: VPA (verbal learning) | FEP < HC for cognitive flexibility, inhibition, reasoning and problem solving, verbal fluency, verbal learning, visual analysis and construction, visuomotor processing, working memory. FEP = HC for attention and vigilance. |
| Chattopadhyay [31] | CHS (34) | HC (47) | ANT (verbal fluency); design fluency; (cognitive flexibility) digit span-forward (attention and vigilance), backward (working memory); DSST (visuomotor processing); PGI-visual recognition (visual learning and memory); serial subtraction (working memory); verbal N -back test (working memory); visual N -back test (working memory); VPA (verbal learning) | CHS < HC for cognitive flexibility, verbal fluency, verbal learning, visual learning and memory, visuomotor processing, working memory. CHS = HC for attention and vigilance. |
| Chen [32] | FES (42) | HC (36) | MCCB (attention and vigilance, reasoning and problem solving, social cognition, verbal fluency, verbal learning, visual learning and memory, visuomotor processing, working memory) | FEP < HC for attention and vigilance, reasoning and problem solving, social cognition, verbal fluency, verbal learning, visual learning and memory, visuomotor processing, working memory. |
| Chen [33] | FES (50) CHS (158) | HC (40) | MCCB (attention and vigilance, reasoning and problem solving, social cognition, verbal fluency, verbal learning, visual learning and memory, visuomotor processing, working memory) | FES < CHS < HC for MCCB composite score and domains attention and vigilance, reasoning and problem solving, visual learning and memory, visuomotor processing (symbol coding), working memory. FES, CHS < HC for verbal fluency, verbal learning, visuomotor processing (TMT-A). FES < CHS, HC for social cognition. |
| Correa-Ghisays [34] | CHS (30) | HC (28) | FFT (visuomotor processing); ROCFT (visual analysis and construction); SCWT (visuomotor processing, inhibition); TAVEC: V1, V3, V4, V8, V10 (verbal learning); TMT-A (visuomotor processing) TMT-B (cognitive flexibility); VFT: semantic and phonemic forms; WCST (verbal fluency); WAIS-III: digit span-forward (attention and vigilance), backward (working memory), digit symbol coding (visuomotor processing), vocabulary (vocabulary) | CHS < HC for global cognitive score and cognitive domains attention and vigilance, cognitive flexibility, inhibition, verbal fluency, verbal learning, visual analysis and construction, visuomotor processing, working memory. CHS = HC for vocabulary. |
| Cuesta [35] | FEP (50) | HC (24) S-FEP (21) | BVMT-R (visual learning and memory); CPT-IP (attention and vigilance); MSCEIT (social cognition); TAVEC (verbal learning); TMT-A/B (visuomotor processing/cognitive flexibility); WAIS-III: digit span-forward/backward (attention and vigilance/working memory), digit symbol coding (visuomotor processing), LNS (working memory), symbol search (visuomotor processing), vocabulary (vocabulary); WCST-64 (cognitive flexibility); WMS-III: spatial span-forward/backward (attention and vigilance/working memory) | FEP < HC for visual learning and memory, vocabulary. FEP < S-FEP < HC for global cognition score and domains attention and vigilance, social cognition. FEP < S-FEP, HC for cognitive flexibility, verbal learning, visuomotor processing, working memory. |
| Da Motta [36] | CHS (38) | HC (97) | PennCNB (abstraction, attention and vigilance, reasoning and problem solving, social cognition, verbal memory, visual analysis and construction, visuomotor processing, working memory) | CHS < HC for abstraction, attention and vigilance, reasoning and problem solving, social cognition, verbal memory, visual learning and memory, visual analysis and construction, visuomotor processing, working memory. |
| De la Torre [37] | CHS (97) | HC (35) | RBANS-form A (attention and vigilance, naming, verbal fluency, verbal learning, verbal memory, visual analysis and construction, visual learning and memory, visuomotor processing) | CHS < HC for RBANS total performance and domains verbal fluency, verbal learning, verbal memory (list recognition, story memory, story recall), visual analysis and construction, visual learning and memory, visuomotor processing. CHS = HC for attention and vigilance, naming, verbal memory (list recall). |
| Eisenacher [38] | HRP (38) | HC (38) | MCCB (attention and vigilance, reasoning and problem solving, social cognition, verbal fluency, verbal learning, visual learning and memory, visuomotor processing, working memory); WCST (cognitive flexibility) | HRP < HC for MCCB composite score and domains reasoning and problem solving, verbal fluency, verbal learning, visuomotor processing, working memory. HRP = HC for attention and vigilance, cognitive flexibility, visual learning and memory, social cognition. |
| Ferretjans [39] | CHS (69) | HC (43) | BACS (planning, verbal fluency, verbal learning, visuomotor processing, working memory) | CHS < HC for BACS composite score and domains planning, verbal fluency, verbal learning, visuomotor processing, working memory. |
| Frommann [40] | HRP-early (116) HRP-late (89) | HC (87) | CPT-IP (attention and vigilance); LNS (working memory); MWT (vocabulary); AVLT (verbal learning); SOPT (working memory); TMT-A/B (visuomotor processing/cognitive flexibility); verbal fluency; (verbal fluency) WAIS-III: digit symbol coding (visuomotor processing) | HRP-late < HRP-early < HC for general cognitive score and domains cognitive flexibility, verbal learning, visuomotor processing (TMT A). HRP-late < HRP-early, HC for visuomotor processing (Digit Symbol Coding), working memory (SOPT). HRP-late, HRP-early < HC for verbal fluency. HRP-late < HC for attention and vigilance. HRP-late = HRP-early = HC for vocabulary, working memory (LNS). |
| Giordano [41] | CHS (114) | HC (63) | MCCB (attention and vigilance, reasoning and problem solving, social cognition, verbal fluency, verbal learning, visual learning and memory, visuomotor processing, working memory) | CHS < HC for attention and vigilance, reasoning and problem solving, social cognition, verbal fluency, verbal learning, visual learning and memory, visuomotor processing, working memory. |
| Guo [42] | FES (51) | HC (41) | BACS: symbol coding (visuomotor processing); BVMT-R (visual analysis and construction); CFT: animal naming (verbal fluency); HVLT-R (verbal learning); SCWT (visuomotor processing, inhibition); TMT-A (visuomotor processing); WMS-III: spatial span-forward/backward (attention and vigilance/working memory) | FEP < HC for attention and vigilance, inhibition, verbal fluency, verbal learning, visual learning and memory, visuomotor processing, working memory. |
| Hájková [43] | FEP (53) | HC (49) | CPT (attention and vigilance); RAVLT (verbal learning); ROCFT (visual analysis and construction); SCWT (visuomotor processing, inhibition); TMT-A/B (visuomotor processing/cognitive flexibility); verbal fluency (verbal fluency); WAIS-III: comprehension (comprehension), digit span-forward/backward (attention and vigilance/working memory), digit symbol coding (visuomotor processing), LNS (working memory), picture arrangement (reasoning and problem solving), similarities (abstraction), ToL (planning); WMS-III: logical memory (verbal learning), spatial span-forward/backward (attention and vigilance/working memory) | FES < HC for abstraction, attention and vigilance, cognitive flexibility, comprehension, inhibition, planning, reasoning and problem solving, verbal fluency, verbal learning, visual analysis and construction, visuomotor processing, working memory. |
| He [44] | FEP (115) | HC (113) | CANTAB: pattern recognition memory (visual learning and memory), rapid visual information processing (attention and vigilance); TMT-A/B (visuomotor processing/cognitive flexibility); WAIS: digit symbol test (visuomotor processing); WMS: logical memory (verbal learning) | FEP < HC for attention and vigilance, cognitive flexibility, verbal learning, visual learning and memory, visuomotor processing. |
| Konstantakopoulos [45] | CHS (54) | HC (53) | Babcock story recall test (verbal memory); Faux pas recognition test (social cognition); SCWT (visuomotor processing, inhibition); TMT-A/B (visuomotor processing/cognitive flexibility); WAIS: block design (reasoning and problem solving), digit span-backward (working memory), vocabulary (vocabulary); WCST-64 (cognitive flexibility) | CHS < HC for cognitive flexibility, inhibition, reasoning and problem solving, social cognition, verbal memory, visuomotor processing, vocabulary, working memory. |
| Koshiyama [46] | CHS (428) | HC (283) | CVLT (verbal learning); LNS (working memory); WCST (cognitive flexibility) | CHS < HC for cognitive flexibility, verbal learning, working memory. |
| Li [47] | HRP (34) | HC (37) | BACS: symbol coding (visuomotor processing); BVMT-R (visual learning and memory); CPT-IP (attention and vigilance); HVTL-R (verbal learning); SCWT (visuomotor processing, inhibition); TMT-A/B (visuomotor processing/cognitive flexibility) | HRP < HC for attention and vigilance, cognitive flexibility, inhibition, verbal learning, visual learning and memory, visuomotor processing (symbol coding, SCWT color–word subtest). HRP = HC for visuomotor processing (TMT-A). |
| Liu [48] | HRP (73) FES (44) CHS (34) | HC (72) | MCCB (attention and vigilance, reasoning and problem solving, social cognition, verbal fluency, verbal learning, visual learning and memory, visuomotor processing, working memory) | HRP, FES, CHS < HC for MCCB composite score and domains reasoning and problem solving, social cognition, verbal fluency, visual learning and memory, visuomotor processing. FES, CHS < HC for attention and vigilance. CHS < HRP, HC for attention and vigilance. CHS < HC for working memory. FES, HRP = HC for working memory. HRP, FES, CHS = HC for verbal learning. |
| Liu [49] | FES (31) | HC (33) | Block diagram test (reasoning and problem solving); MSCEIT: Managing Emotions (social cognition); RBANS (attention and vigilance, naming, verbal fluency, verbal learning, verbal memory, visual analysis and construction, visual learning and memory, visuomotor processing); TMT-A (visuomotor processing); vocabulary test (vocabulary) | FES < HC for RBANS composite score and domains attention and vigilance, naming, reasoning and problem solving, verbal fluency, verbal learning, verbal memory (immediate, delayed), visual analysis and construction, visual learning and memory, visuomotor processing. FES = HC for social cognition, vocabulary. |
| Maes, Sirivichayakul, Kanchanatawan et al. [50] | CHS-MR (40) CHS-NMR (39) | HC (40) | CANTAB: one touch stockings of Cambridge (planning), rapid visual information processing (attention and vigilance), spatial working memory (working memory); CERAD: VFT (verbal fluency), WLM (verbal memory), word list recall (verbal memory) | CHS-MR < CHS-NMR < HC for attention and vigilance, verbal fluency, verbal memory. CHS-MR, CHS-NMR < HC for planning, working memory. |
| Maes, Sirivichayakul, Matsumoto et al. [51] | CHS-NOS (39) CHS-OS (40) | HC (40) | CANTAB: one touch stockings of Cambridge (planning), spatial working memory (working memory); CERAD: VFT (verbal fluency), WLM (verbal memory), word list recall (verbal memory) | CHS-OS < CHS < HC for verbal fluency, verbal memory. CHS-OS, CHS < HC for planning, working memory. |
| Maes [52] | CHS-ND (40) CHS-D (40) | HC (40) | CANTAB: emotion recognition test (social cognition), intra-extra-dimensional set shift (cognitive flexibility), one touch stockings of Cambridge (planning), paired association learning (visual learning and memory), rapid visual information processing (attention and vigilance), spatial working memory (working memory); CERAD: VFT (verbal fluency), WLM (verbal memory), word list recall (verbal memory) | CHS-D < CHS-ND, HC for attention and vigilance (rapid visual information processing–detection), verbal memory (CERAD: word list recall), visual learning and memory CHS-D < CHS-ND < HC for social cognition, verbal fluency, verbal memory (CERAD: WLM). CHS-D, CHS-ND < HC for attention and vigilance (rapid visual information processing–speed), planning, working memory.– CHS-D < HC for cognitive flexibility. |
| Mançe ÇaliŞir [53] | CHS (17) | HC (23) | RAVLT: delayed recall, immediate memory, learning (verbal learning); WAIS: arithmetic (working memory), block design (reasoning and problem solving), comprehension (comprehension), digit span-forward/backward (attention and vigilance/working memory), digit symbol (visuomotor processing), similarities (abstraction); WCST (cognitive flexibility) | CHS < HC for cognitive flexibility, comprehension, visuomotor processing. CHS = HC for abstraction, attention and vigilance, reasoning and problem solving, verbal learning, working memory. |
| McDonald [54] | HRP (101) | HC (38) | BACS (planning, verbal fluency, verbal learning, visuomotor processing, working memory) | HRP < HC for visuomotor processing (token motor task). HRP = HC for planning, verbal fluency, verbal learning, visuomotor processing (symbol coding) working memory. |
| Morales-Muñoz [55] | FEP (38) | HC (38) | MCCB (attention and vigilance, reasoning and problem solving, social cognition, verbal fluency, verbal learning, visual learning and memory, visuomotor processing, working memory) | FEP < HC for attention and vigilance, reasoning and problem solving, social cognition, verbal fluency, verbal learning, visual learning and memory, visuomotor processing, working memory. |
| Ngoma [56] | FEP (188) | HC (153) | 15WoR (verbal learning); COWAT (verbal fluency); d2 (attention and vigilance); FOT (visuomotor processing); LNS (working memory); ROCFT (visual analysis and construction); SCWT (visuomotor processing/inhibition); TMT-A/B (visuomotor processing/cognitive flexibility); WCST (cognitive flexibility) | CHS < HC for attention and vigilance, cognitive flexibility, inhibition, verbal fluency, verbal learning, visual analysis and construction, visuomotor processing, working memory. |
| Randers [57] | HRP (50) | HC (50) | BACS: digit sequencing (working memory), list learning (verbal learning), symbol coding (visuomotor processing), token motor task (visuomotor processing), verbal fluency (verbal fluency); CANTAB: delayed matching to sample (visual learning and memory), intra/extra-dimensional set shift (cognitive flexibility); rapid visual information processing (attention and vigilance), reaction time (visuomotor processing); spatial span-forward/backward (attention and vigilance/working memory), spatial working memory (working memory), stockings of Cambridge (planning); DART (vocabulary); TMT-A/B (visuomotor processing); WAIS-III: block design (reasoning and problem solving), matrix reasoning (reasoning and problem solving), similarities (abstraction); vocabulary (vocabulary) | HRP < HC for abstraction, attention and vigilance, cognitive flexibility, planning, reasoning and problem solving, verbal fluency, verbal learning, visual learning and memory, visuomotor processing, vocabulary, working memory. |
| Saleem [58] | FEP (20) | HC (15) | CANTAB: intra/extra dimensional set shift (cognitive flexibility), pattern recognition memory (visual learning and memory), reaction time (visuomotor processing), spatial recognition memory (visual learning and memory), stockings of Cambridge (planning); WTAR (vocabulary) | FEP < HC for cognitive flexibility, planning, visual learning and memory, visuomotor processing. FEP = HC for vocabulary. |
| Service [59] | CHS (160) | HC (717) | PennCNB: CPT (attention and vigilance), digit symbol test (visuomotor processing), emotion differentiation test (social cognition), emotion recognition test (social cognition), face memory test (visual learning and memory), letter N -back task (working memory), matrix reasoning test (reasoning and problem solving), motor praxis test (visuomotor processing) | CHS < HC for attention and vigilance, reasoning and problem solving, social cognition, visual learning and memory, visuomotor processing, working memory. |
| Shi [60] | CHS (230) | HC (656) | Action (verb) fluency (verbal fluency); color trails test-I/II (attention and vigilance/cognitive flexibility); grooved pegboard (visuomotor processing); MCCB (attention and vigilance, reasoning and problem solving, social cognition, verbal fluency, verbal learning, visual learning and memory, visuomotor processing, working memory); PASAT-50 (working memory); SCWT (visuomotor processing); WCST-64 (cognitive flexibility) | CHS < HC for attention and vigilance, cognitive flexibility, inhibition, reasoning and problem solving, social cognition, verbal fluency, verbal learning, visual learning and memory, visuomotor processing, working memory. |
| Tang [61] | CHS-D (51) CHS-ND (58) | HC (40) | DVT (attention and vigilance); PASAT (working memory); SCWT (visuomotor processing, inhibition); VFT: actions, animals (verbal fluency); WAIS-RC: block design (reasoning and problem solving) | CHS-D < CHS-ND < HC for inhibition, reasoning and problem solving, verbal fluency, visuomotor processing, working memory. CHS-D < CHS-ND, HC for attention and vigilance. |
| Vignapiano [62] | CHS (145) | HC (69) | MCCB (attention and vigilance, reasoning and problem solving, social cognition, verbal fluency, verbal learning, visual learning and memory, visuomotor processing, working memory) | CHS < HC for MCCB composite score and domains attention and vigilance, reasoning and problem solving, social cognition, verbal learning, visual learning and memory, visuomotor processing, working memory. |
| Wang [63] | FES (81) | HC (73) | BACS (planning, verbal fluency, verbal learning, visuomotor processing, working memory); COWAT (verbal fluency) | FEP < HC for BACS composite score and domains planning, verbal fluency, verbal learning, visuomotor processing, working memory. |
| Wu [64] | FES (79) CHS (132) | HC (124) | MCCB (attention and vigilance, reasoning and problem solving, social cognition, verbal fluency, verbal learning, visual learning and memory, visuomotor processing, working memory) | FES < HC for attention and vigilance, reasoning and problem solving, social cognition, verbal fluency, verbal learning, visual learning and memory, visuomotor processing, working memory. CHS < HC for attention and vigilance, reasoning and problem solving, social cognition, verbal fluency, verbal learning, visual learning and memory, visuomotor processing, working memory. CHS < FES for reasoning and problem solving, social cognition, verbal fluency, verbal learning, visuomotor processing (TMT-A), working memory (digital sequence). CHS = FES for attention and vigilance, visual learning and memory, visuomotor processing (symbol coding), working memory (spatial span). |
| Xiao [65] | FES (58) | HC (55) | Digit span-forward/backward (attention and vigilance); SCWT (visuomotor processing, inhibition); TMT-A/B (visuomotor processing, cognitive flexibility); VFT: animals, actions (verbal fluency) | FES < HC for cognitive flexibility, inhibition, verbal fluency, visuomotor processing, working memory. FES = HC for attention and vigilance. |
| Xiu [66] | FES (45) CHS (35) | HC (40) | RBANS-form A (attention and vigilance, naming, verbal fluency, verbal learning, verbal memory, visual analysis and construction, visual learning and memory, visuomotor processing) | CHS, FEP < HC for RBANS composite score and domains attention and vigilance, naming, verbal fluency, verbal learning, verbal memory (delayed), visual learning and memory, visuomotor processing. CHS < FEP < HC for verbal learning, verbal memory (immediate). CHS < HC for visual analysis and construction. FEP = HC for visual analysis and construction. |
| Yang [67] | FES (21) CHS (26) SZ (47) = FES (21) + CHS (26) | HC (45) | BACS: symbol coding (visuomotor processing); BVMT-R (visual learning and memory); CPT-IP (attention and vigilance); HVLT-R (verbal learning), SCWT (visuomotor processing, inhibition); TMT-A (visuomotor processing); WMS-III: spatial span-forward/backward (attention and vigilance/working memory) | SZ < HC for attention and vigilance, inhibition, verbal learning, visual learning and memory, visuomotor processing, working memory. When controlled for age, gender, years of education and body mass index, SZ = HC for visual learning and memory. CHS = FES for verbal learning, visual learning, visual memory. CHS < FES for attention and vigilance, inhibition, visuomotor processing, working memory. When controlled for age, gender, years of education body mass index and PANSS scores, CHS < FES for attention and vigilance, inhibition, visuomotor processing (SCWT color–word), working memory. When controlled for age, gender, years of education, body mass index and PANSS scores, CHS = FES for verbal learning, visual learning and memory, visuomotor processing (symbol coding, TMT-A). |
| Yang [68] | FES (34) CHS (31) | HC (35) | MCCB (attention and vigilance, reasoning and problem solving, social cognition, verbal fluency, verbal learning, visual learning and memory, visuomotor processing, working memory) | CHS, FES < HC for MCCB composite score and domains attention and vigilance, reasoning and problem solving, social cognition, verbal fluency, verbal learning, visual learning and memory, visuomotor processing, working memory. |
| Yang [69] | CHS (32) | HC (30) | BACS: symbol coding (visuomotor processing); BVMT-R (visual learning and memory); CPT-IP (attention and vigilance); HVLT-R (verbal learning); SCWT (visuomotor processing, inhibition); TMT-A (visuomotor processing); WMS-III: spatial span-forward/backward (attention and vigilance/working memory) | CHS < HC for attention and vigilance, inhibition, verbal learning, visual learning and memory, visuomotor processing, working memory. When controlled for age, gender, years of education and body mass index, CHS = HC for visual learning and memory. |
| Zhang [70] | FES (77) | HC (75) | RBANS (attention and vigilance, naming, verbal fluency, verbal learning, verbal memory, visual analysis and construction, visual learning and memory, visuomotor processing) | FES < HC for attention and vigilance, naming, verbal fluency, verbal learning, verbal memory. FES = HC for visual analysis and construction. |
| Zhang [71] | FES (32) | HC (29) | AVLT (verbal learning); digit span-forward/backward (attention and vigilance/working memory); SCWT (visuomotor processing, inhibition); semantic similarity test (abstraction); TMT-A/B (visuomotor processing, inhibition); VFT (verbal fluency); WCST (cognitive flexibility); | FES < HC for abstraction, attention and vigilance, cognitive flexibility, inhibition, verbal fluency, verbal learning, visuomotor processing, working memory. |
| Zhao [72] | FES-R (65) FES-NR (45) | HC (58) | CFET (social cognition); digit span-forward/backward (attention and vigilance/working memory); HVLT-R (verbal learning); TMT-A/B (visuomotor processing/cognitive flexibility); SCWT (visuomotor processing, inhibition); VFT: actions, animals (verbal fluency) | FES-NR < FES-R < HC for cognitive flexibility, inhibition, verbal fluency (animals), verbal learning, visuomotor processing. FES-NR < FES-R, HC for social cognition, verbal fluency (actions). FES-NR, FES-R = HC for attention and vigilance, working memory. |
| Zhou, Tang et al. [73] | CHS-D (33) CHS-ND (41) | HC (40) | ANT (verbal fluency); COWAT (verbal fluency); DVT (attention and vigilance); SCWT (visuomotor processing, inhibition); spatial processing block design (reasoning and problem solving); TMT-A/B (visuomotor processing/cognitive flexibility); WAIS-RC: block design (reasoning and problem solving) | CHS-D < CHS-ND, HC for attention and vigilance. CHS-D < CHS-ND < HC for cognitive flexibility, reasoning and problem solving (spatial processing: block design), verbal fluency, visuomotor processing CHS-D, CHS-ND < HC for inhibition, reasoning and problem solving (WAIS-RC: block design) |
| Zhou, Yu et al. [74] | CHS-D (37) CHS-ND (38) | HC (38) | ANT (verbal fluency); COWAT (verbal fluency); DVT (attention and vigilance); SCWT (visuomotor processing, inhibition); spatial processing block design (reasoning and problem solving); TMT-A/B (visuomotor processing/cognitive flexibility); WAIS-RC: block design (reasoning and problem solving) | CHS-D < CHS-ND < HC for attention and vigilance, reasoning and problem solving (spatial processing: block design), visuomotor processing (SCWT color–word subtests). CHS-D, CHS-ND < HC for cognitive flexibility, inhibition, reasoning and problem solving (WAIS-RC: block design), verbal fluency, visuomotor processing (TMT-A). |
| Zhou [75] | CHS-D (58) CHS-ND (93) | HC (113) | ANT (verbal fluency); COWAT (verbal fluency); DVT (attention and vigilance); SCWT (visuomotor processing, inhibition); spatial processing block design (reasoning and problem solving); TMT-A/B (visuomotor processing/cognitive flexibility); WAIS-RC: block design (reasoning and problem solving) | CHS-D < CHS-ND < HC for attention and vigilance, reasoning and problem solving (WAIS-RC: block design), verbal fluency (ANT), visuomotor processing (SCWT color–word subtests). CHS-D, CHS-ND < HC for cognitive flexibility, inhibition, reasoning and problem solving (spatial processing block design), verbal fluency (COWAT), visuomotor processing (TMT-A). |
| Zong [76] | FES (42) | HC (38) | Digit span-forward/backward (attention and vigilance/working memory); TMT-A/B (visuomotor processing/cognitive flexibility) | FES < HC for attention and vigilance, cognitive flexibility, visuomotor processing, working memory. |
| Patient Groups vs. Healthy Controls | First-Episode Stage N = 23 Studies | Chronic Stage N = 29 Studies |
|---|---|---|
| 100% of studies reported deficits | Abstraction (N = 3), cognitive flexibility (N = 10), inhibition (N = 8), naming (N = 3), planning (N = 3), reasoning and problem solving (N = 10), verbal fluency (N = 18), verbal memory (N = 3), visuomotor processing (N = 22) | Cognitive flexibility (N = 9), inhibition (N = 9), verbal fluency (N = 22), verbal memory (N = 6), visual analysis and construction (N = 4), visuomotor processing (N = 25) |
| More than 75% of studies report deficits | Attention and vigilance (N = 20), social cognition (N = 9), verbal learning (N = 20), visual learning and memory (N = 13), working memory (N = 18) | Attention and vigilance (N = 20), planning (N = 7), reasoning and problem solving (N = 16), social cognition (N = 11), verbal learning (N = 19), visual learning and memory (N = 14), working memory (N = 24) |
| More than 50% of studies report deficits | Visual analysis and construction (N = 6) | Vocabulary (N = 3) |
| More than 25% of studies report deficits | Vocabulary (N = 4) | none |
| 25% of studies or fewer report deficits | none | none |
| CHS < FES < HC (3 Studies) | FES < CHS < HC (1 Study) | (CHS = FES) < HC (6 Studies) | FES < (CHS = HC) (1 Study) | CHS < HC/ FES = HC (2 Studies) | CHS = FES = HC (2 Studies) | Sum of Significant Results per Domain | |
|---|---|---|---|---|---|---|---|
| Attention and vigilance (6 studies) | 2 | 1 | 4 | 0 | 0 | 0 | 7 |
| Inhibition (1 study) | 1 | 0 | 0 | 0 | 0 | 0 | 1 |
| Naming (1 study) | 0 | 0 | 1 | 0 | 0 | 0 | 1 |
| Reasoning and problem solving (4 studies) | 1 | 1 | 2 | 0 | 0 | 0 | 4 |
| Social cognition (4 studies) | 1 | 0 | 2 | 1 | 0 | 0 | 4 |
| Verbal fluency (5 studies) | 1 | 0 | 4 | 0 | 0 | 0 | 5 |
| Verbal learning (6 studies) | 2 | 0 | 3 | 0 | 0 | 1 | 6 |
| Verbal memory (1 study) | 1 | 0 | 3 | 0 | 0 | 0 | 4 |
| Visual analysis and construction (1 study) | 0 | 0 | 0 | 0 | 2 | 0 | 2 |
| Visual learning and memory (5 studies) | 0 | 1 | 3 | 0 | 0 | 1 | 5 |
| Visuomotor processing (6 studies) | 3 | 1 | 9 | 0 | 0 | 0 | 13 |
| Working memory (5 studies) | 2 | 2 | 3 | 0 | 2 | 0 | 9 |
| Sum of significant tests per comparison | 14 | 6 | 34 | 1 | 4 | 2 |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tschentscher, N.; Woll, C.F.J.; Tafelmaier, J.C.; Kriesche, D.; Bucher, J.C.; Engel, R.R.; Karch, S. Neurocognitive Deficits in First-Episode and Chronic Psychotic Disorders: A Systematic Review from 2009 to 2022. Brain Sci. 2023, 13, 299. https://doi.org/10.3390/brainsci13020299
Tschentscher N, Woll CFJ, Tafelmaier JC, Kriesche D, Bucher JC, Engel RR, Karch S. Neurocognitive Deficits in First-Episode and Chronic Psychotic Disorders: A Systematic Review from 2009 to 2022. Brain Sciences. 2023; 13(2):299. https://doi.org/10.3390/brainsci13020299
Chicago/Turabian StyleTschentscher, Nadja, Christian F. J. Woll, Julia C. Tafelmaier, Dominik Kriesche, Julia C. Bucher, Rolf R. Engel, and Susanne Karch. 2023. "Neurocognitive Deficits in First-Episode and Chronic Psychotic Disorders: A Systematic Review from 2009 to 2022" Brain Sciences 13, no. 2: 299. https://doi.org/10.3390/brainsci13020299