
A Pooled Analysis of Preoperative Inflammatory Biomarkers to Predict 90-Day Outcomes in Patients with an Aneurysmal Subarachnoid Hemorrhage: A Single-Center Retrospective Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients’ Data
2.3. Outcome Measurement
2.4. Statistical Analysis
3. Results
3.1. Inflammatory Biomarker-Related Risk Factors Associated with 90-Day Unfavorable Outcomes
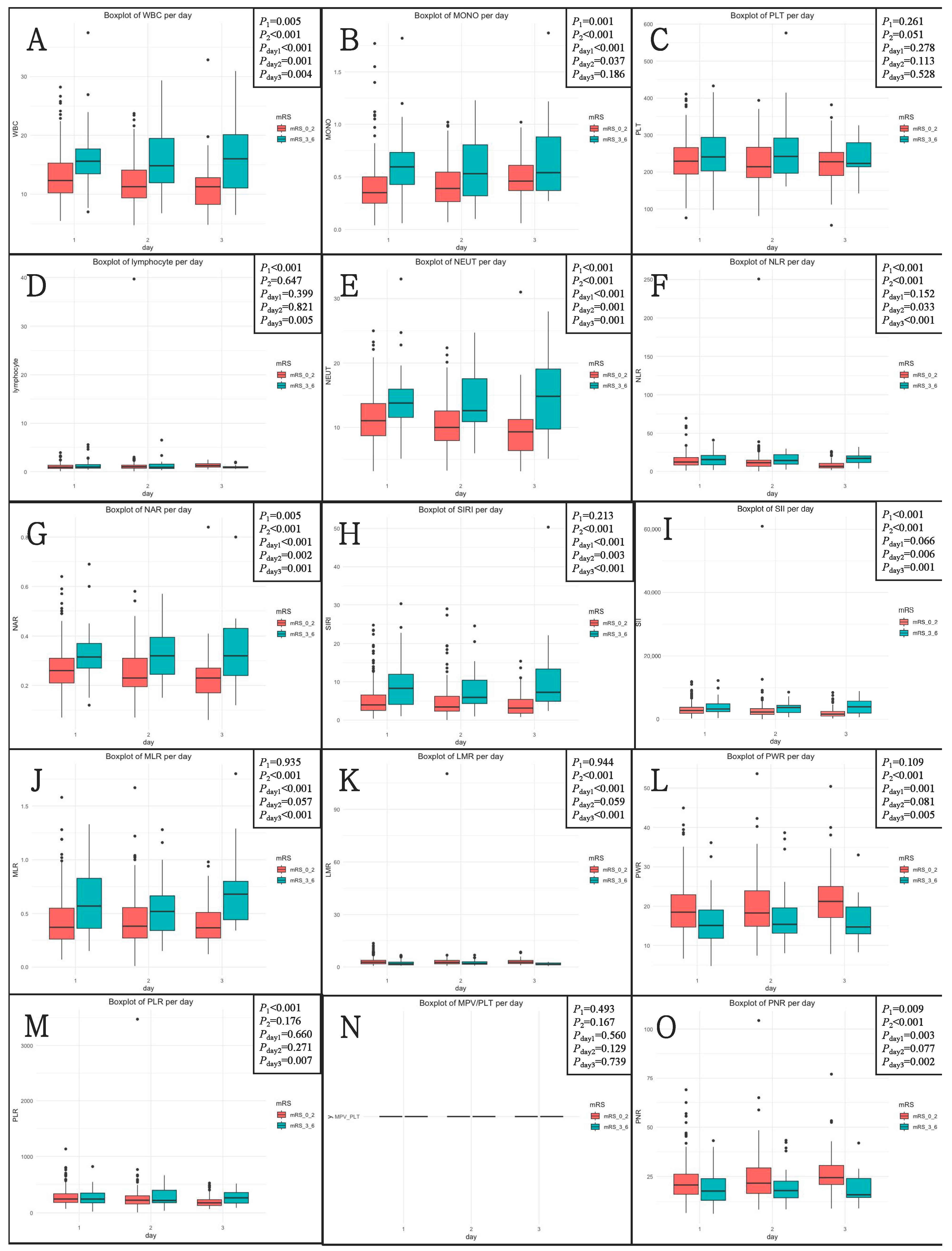
3.2. Associations between Inflammatory Biomarkers and WFNS Grade, mFS Grade, and Graeb Score
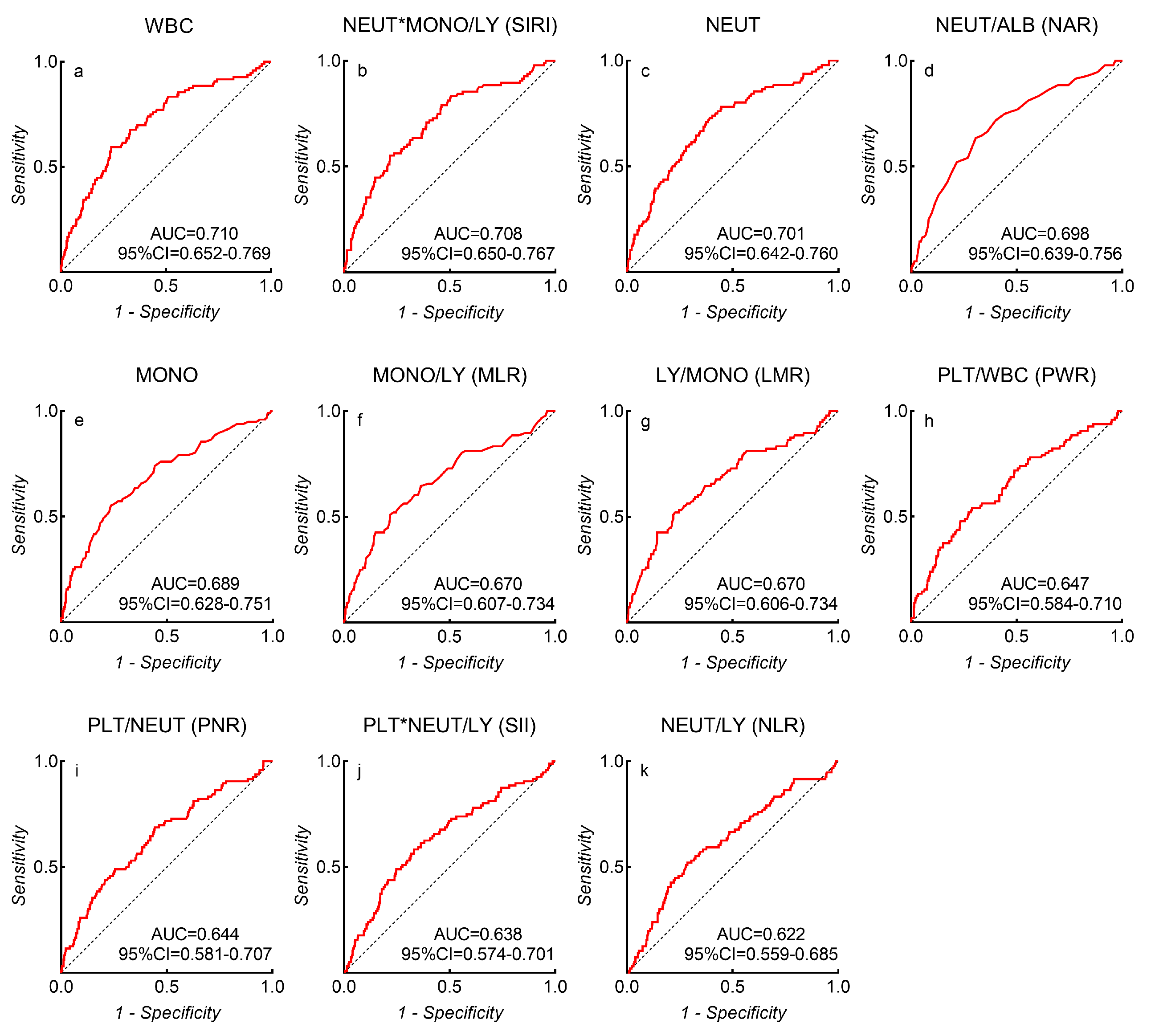
3.3. Receiver Operating Characteristic Curve Analysis
3.4. Associations between Inflammatory Biomarkers and In-Hospital Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lovelock, C.E.; Rinkel, G.J.; Rothwell, P.M. Time trends in outcome of subarachnoid hemorrhage: Population-based study and systematic review. Neurology 2010, 74, 1494–1501. [Google Scholar] [CrossRef] [PubMed]
- Mukhtar, T.K.; Molyneux, A.J.; Hall, N.; Yeates, D.R.; Goldacre, R.; Sneade, M.; Clarke, A.; Goldacre, M.J. The falling rates of hospital admission, case fatality, and population-based mortality for subarachnoid hemorrhage in England, 1999–2010. J. Neurosurg. 2016, 125, 698–704. [Google Scholar] [CrossRef] [PubMed]
- Fujii, M.; Yan, J.; Rolland, W.B.; Soejima, Y.; Caner, B.; Zhang, J.H. Early brain injury, an evolving frontier in subarachnoid hemorrhage research. Transl. Stroke Res. 2013, 4, 432–446. [Google Scholar] [CrossRef]
- Kusaka, G.; Ishikawa, M.; Nanda, A.; Granger, D.N.; Zhang, J.H. Signaling pathways for early brain injury after subarachnoid hemorrhage. J. Cereb. Blood Flow Metab. 2004, 24, 916–925. [Google Scholar] [CrossRef] [PubMed]
- Sehba, F.A.; Friedrich, V. Early events after aneurysmal subarachnoid hemorrhage. Acta. Neurochir. Suppl. 2015, 120, 23–28. [Google Scholar] [CrossRef]
- Suzuki, H. What is early brain injury? Transl. Stroke Res. 2015, 6, 1–3. [Google Scholar] [CrossRef]
- Aronowski, J.; Zhao, X. Molecular pathophysiology of cerebral hemorrhage: Secondary brain injury. Stroke 2011, 42, 1781–1786. [Google Scholar] [CrossRef]
- Macdonald, R.L.; Schweizer, T.A. Spontaneous subarachnoid haemorrhage. Lancet 2017, 389, 655–666. [Google Scholar] [CrossRef]
- Sehba, F.A.; Pluta, R.M.; Zhang, J.H. Metamorphosis of subarachnoid hemorrhage research: From delayed vasospasm to early brain injury. Mol. Neurobiol. 2011, 43, 27–40. [Google Scholar] [CrossRef]
- Dodd, W.S.; Laurent, D.; Dumont, A.S.; Hasan, D.M.; Jabbour, P.M.; Starke, R.M.; Hosaka, K.; Polifka, A.J.; Hoh, B.L.; Chalouhi, N. Pathophysiology of Delayed Cerebral Ischemia After Subarachnoid Hemorrhage: A Review. J. Am. Heart Assoc. 2021, 10, e021845. [Google Scholar] [CrossRef]
- Rothoerl, R.D.; Axmann, C.; Pina, A.L.; Woertgen, C.; Brawanski, A. Possible role of the C-reactive protein and white blood cell count in the pathogenesis of cerebral vasospasm following aneurysmal subarachnoid hemorrhage. J. Neurosurg. Anesthesiol. 2006, 18, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Chou, S.H.; Feske, S.K.; Simmons, S.L.; Konigsberg, R.G.; Orzell, S.C.; Marckmann, A.; Bourget, G.; Bauer, D.J.; De Jager, P.L.; Du, R.; et al. Elevated peripheral neutrophils and matrix metalloproteinase 9 as biomarkers of functional outcome following subarachnoid hemorrhage. Transl. Stroke Res. 2011, 2, 600–607. [Google Scholar] [CrossRef] [PubMed]
- Feghali, J.; Kim, J.; Gami, A.; Rapaport, S.; Caplan, J.M.; McDougall, C.G.; Huang, J.; Tamargo, R.J.; Jackson, C.M. Monocyte-based inflammatory indices predict outcomes following aneurysmal subarachnoid hemorrhage. Neurosurg. Rev. 2021, 44, 3499–3507. [Google Scholar] [CrossRef] [PubMed]
- Giede-Jeppe, A.; Reichl, J.; Sprugel, M.I.; Lucking, H.; Hoelter, P.; Eyupoglu, I.Y.; Kuramatsu, J.B.; Huttner, H.B.; Gerner, S.T. Neutrophil-to-lymphocyte ratio as an independent predictor for unfavorable functional outcome in aneurysmal subarachnoid hemorrhage. J. Neurosurg. 2019, 132, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Liu, Y.; Zhang, S.; Wang, C.; Zou, C.; Li, A. Neutrophil-to-Albumin Ratio as a Biomarker of Delayed Cerebral Ischemia After Aneurysmal Subarachnoid Hemorrhage. World Neurosurg. 2021, 147, e453–e458. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.W.; Yi, H.J.; Lee, D.H.; Sung, J.H. Prognostic Significance of Various Inflammation-Based Scores in Patients with Mechanical Thrombectomy for Acute Ischemic Stroke. World Neurosurg. 2020, 141, e710–e717. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Huang, Y.; Li, S.; Lin, J.; Liu, W.; Ding, Z.; Li, X.; Chen, Y.; Pang, W.; Yang, D.; et al. Platelet-to-White Blood Cell Ratio: A Prognostic Predictor for 90-Day Outcomes in Ischemic Stroke Patients with Intravenous Thrombolysis. J. Stroke Cerebrovasc. Dis. 2016, 25, 2430–2438. [Google Scholar] [CrossRef]
- Yun, S.; Jun Yi, H.; Hoon Lee, D.; Hoon Sung, J. Clinical significance of platelet to neutrophil ratio and platelet to lymphocyte ratio in patients with aneurysmal subarachnoid hemorrhage. J. Clin. Neurosci. 2021, 92, 49–54. [Google Scholar] [CrossRef]
- Wang, Z.; Pei, W.; Chen, L.; Ning, Y.; Luo, Y. Mean Platelet Volume/Platelet Count Ratio is Associated with Poor Clinical Outcome After Aneurysmal Subarachnoid Hemorrhage. J. Stroke Cerebrovasc. Dis. 2020, 29, 105208. [Google Scholar] [CrossRef]
- Yun, S.; Yi, H.J.; Lee, D.H.; Sung, J.H. Systemic Inflammation Response Index and Systemic Immune-inflammation Index for Predicting the Prognosis of Patients with Aneurysmal Subarachnoid Hemorrhage. J. Stroke Cerebrovasc. Dis. 2021, 30, 105861. [Google Scholar] [CrossRef]
- Luo, F.; Li, Y.; Zhao, Y.; Sun, M.; He, Q.; Wen, R.; Xie, Z. Systemic immune-inflammation index predicts the outcome after aneurysmal subarachnoid hemorrhage. Neurosurg. Rev. 2022, 45, 1607–1615. [Google Scholar] [CrossRef] [PubMed]
- Connolly, E.S., Jr.; Rabinstein, A.A.; Carhuapoma, J.R.; Derdeyn, C.P.; Dion, J.; Higashida, R.T.; Hoh, B.L.; Kirkness, C.J.; Naidech, A.M.; Ogilvy, C.S.; et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: A guideline for healthcare professionals from the American Heart Association/american Stroke Association. Stroke 2012, 43, 1711–1737. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.H.; Burkett, A.; Paz, A.; Savarraj, J.P.; Hinds, S.; Hergenroeder, G.; Gusdon, A.M.; Ren, X.; Hong, J.H.; Choi, H.A. Systemic inflammatory markers of persistent cerebral edema after aneurysmal subarachnoid hemorrhage. J. Neuroinflamm. 2022, 19, 199. [Google Scholar] [CrossRef] [PubMed]
- Saand, A.R.; Yu, F.; Chen, J.; Chou, S.H. Systemic inflammation in hemorrhagic strokes-A novel neurological sign and therapeutic target? J. Cereb. Blood Flow Metab. 2019, 39, 959–988. [Google Scholar] [CrossRef] [PubMed]
- Muroi, C.; Hugelshofer, M.; Seule, M.; Tastan, I.; Fujioka, M.; Mishima, K.; Keller, E. Correlation among systemic inflammatory parameter, occurrence of delayed neurological deficits, and outcome after aneurysmal subarachnoid hemorrhage. Neurosurgery 2013, 72, 367–375, discussion 375. [Google Scholar] [CrossRef] [PubMed]
- Schneider, U.C.; Schiffler, J.; Hakiy, N.; Horn, P.; Vajkoczy, P. Functional analysis of Pro-inflammatory properties within the cerebrospinal fluid after subarachnoid hemorrhage in vivo and in vitro. J. Neuroinflamm. 2012, 9, 28. [Google Scholar] [CrossRef]
- Friedrich, V.; Flores, R.; Muller, A.; Bi, W.; Peerschke, E.I.; Sehba, F.A. Reduction of neutrophil activity decreases early microvascular injury after subarachnoid haemorrhage. J. Neuroinflamm. 2011, 8, 103. [Google Scholar] [CrossRef]
- Li, R.; Lin, F.; Chen, Y.; Lu, J.; Han, H.; Ma, L.; Zhao, Y.; Yan, D.; Li, R.; Yang, J.; et al. A 90-Day Prognostic Model Based on the Early Brain Injury Indicators after Aneurysmal Subarachnoid Hemorrhage: The TAPS Score. Transl. Stroke Res. 2022; online ahead of print. [Google Scholar] [CrossRef]
- Ren, H.; Liu, X.; Wang, L.; Gao, Y. Lymphocyte-to-Monocyte Ratio: A Novel Predictor of the Prognosis of Acute Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2017, 26, 2595–2602. [Google Scholar] [CrossRef]
- Guo, H.; Zhao, Z.; Zhang, R.; Chen, P.; Zhang, X.; Cheng, F.; Gou, X. Monocytes in the Peripheral Clearance of Amyloid-beta and Alzheimer’s Disease. J. Alzheimers Dis. 2019, 68, 1391–1400. [Google Scholar] [CrossRef]
- Walsh, K.B.; Sekar, P.; Langefeld, C.D.; Moomaw, C.J.; Elkind, M.S.; Boehme, A.K.; James, M.L.; Osborne, J.; Sheth, K.N.; Woo, D.; et al. Monocyte Count and 30-Day Case Fatality in Intracerebral Hemorrhage. Stroke 2015, 46, 2302–2304. [Google Scholar] [CrossRef]
- Frontera, J.A.; Provencio, J.J.; Sehba, F.A.; McIntyre, T.M.; Nowacki, A.S.; Gordon, E.; Weimer, J.M.; Aledort, L. The Role of Platelet Activation and Inflammation in Early Brain Injury Following Subarachnoid Hemorrhage. Neurocrit. Care 2017, 26, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Bell, J.D.; Thomas, T.C.; Lass, E.; Ai, J.; Wan, H.; Lifshitz, J.; Baker, A.J.; Macdonald, R.L. Platelet-mediated changes to neuronal glutamate receptor expression at sites of microthrombosis following experimental subarachnoid hemorrhage. J. Neurosurg. 2014, 121, 1424–1431. [Google Scholar] [CrossRef] [PubMed]
- Si, Y.; Liu, J.; Shan, W.; Zhang, Y.; Han, C.; Wang, R.; Sun, L. Association of lymphocyte-to-monocyte ratio with total coronary plaque burden in patients with coronary artery disease. Coron. Artery Dis. 2020, 31, 650–655. [Google Scholar] [CrossRef] [PubMed]
- Pan, P.; Zhang, X.; Li, Q.; Zhao, H.; Qu, J.; Zhang, J.H.; Liu, X.; Feng, H.; Chen, Y. Cyclosporine A alleviated matrix metalloproteinase 9 associated blood-brain barrier disruption after subarachnoid hemorrhage in mice. Neurosci. Lett. 2017, 649, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Lin, F.; Chen, Y.; Lu, J.; Han, H.; Yan, D.; Li, R.; Yang, J.; Li, Z.; Zhang, H.; et al. In-hospital complication-related risk factors for discharge and 90-day outcomes in patients with aneurysmal subarachnoid hemorrhage after surgical clipping and endovascular coiling: A propensity score-matched analysis. J. Neurosurg. 2021, 137, 381–392. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patient Characteristics | mRS Score at 90 Days | p | |
|---|---|---|---|
| mRS 0–2 | mRS 3–6 | ||
| No. of patients | 447 | 96 | |
| Female, n (%) | 256 (57.3) | 51 (53.1) | 0.457 |
| Age, years, mean ± SD | 53.9 ± 11.0 | 58.7 ± 10.8 | <0.001 |
| Current smoking, n (%) | 134 (30.0) | 27 (28.1) | 0.718 |
| Hypertension, n (%) | 255 (57.0) | 71 (74.0) | 0.002 |
| Hyperlipidemia, n (%) | 40 (8.9) | 7 (7.3) | 0.600 |
| Diabetes mellitus, n (%) | 35 (7.8) | 10 (10.4) | 0.404 |
| Posterior circulation, n (%) | 53 (11.9) | 11 (11.5) | 0.913 |
| WFNS grade 4–5, n (%) | 73 (16.3) | 56 (58.3) | <0.001 |
| mFS grade 3–4, n (%) | 339 (75.8) | 89 (92.7) | <0.001 |
| Graeb score 5–12, n (%) | 26 (5.8) | 22 (22.9) | <0.001 |
| SEBES score 3–4, n (%) | 213 (47.7) | 50 (52.1) | 0.430 |
| Acute hydrocephalus, n (%) | 175 (39.1) | 50 (52.1) | 0.020 |
| White blood cell count *, median (IQR) | 11.86 (9.40–14.68) | 15.26 (12.44–18.54) | <0.001 |
| Monocyte count *, median (IQR) | 0.39 (0.26–0.54) | 0.57 (0.40–0.81) | <0.001 |
| Platelet count *, median (IQR) | 225.0 (188.0–265.0) | 237.5 (202.3–288.5) | 0.051 |
| Lymphocyte count *, median (IQR) | 0.99 (0.70–1.38) | 0.88 (0.71–1.40) | 0.647 |
| Neutrophil count *, median (IQR) | 10.51 (7.97–13.27) | 13.56 (11.03–16.34) | <0.001 |
| NLR, median (IQR) | 11.06 (6.97–15.70) | 15.21 (8.99–21.00) | <0.001 |
| NAR, median (IQR) | 0.25 (0.19–0.31) | 0.32 (0.25–0.39) | <0.001 |
| SIRI, median (IQR) | 3.68 (2.36–6.24) | 7.06 (4.13–11.70) | <0.001 |
| SII, median (IQR) | 2470 (1535–3548) | 3412 (2089–5002) | <0.001 |
| MLR, median (IQR) | 0.37 (0.26–0.54) | 0.57 (0.36–0.79) | <0.001 |
| LMR, median (IQR) | 2.70 (1.87–3.79) | 1.77 (1.26–2.79) | <0.001 |
| PWR, median (IQR) | 19.00 (14.96–23.51) | 15.26 (12.13–19.80) | <0.001 |
| PLR, median (IQR) | 225.4 (162.1–313.9) | 245.4 (171.5–374.9) | 0.176 |
| MPV/PLT, median (IQR) | 0.04 (0.03–0.05) | 0.04 (0.03–0.05) | 0.167 |
| PNR, median (IQR) | 21.69 (16.60–27.92) | 17.67 (13.29–21.10) | <0.001 |
| Treatment modality | 0.040 | ||
| Surgical clipping, n (%) | 200 (44.7) | 54 (56.3) | |
| Endovascular coiling, n (%) | 247 (55.3) | 42 (43.8) | |
| Variables | OR * (95% CI) | p |
|---|---|---|
| WBC | 1.15 (1.08–1.22) | <0.001 |
| SIRI | 1.09 (1.04–1.14) | <0.001 |
| NEUT | 1.14 (1.08–1.22) | <0.001 |
| NAR | 110.19 (9.42–1288.36) | <0.001 |
| MONO | 7.38 (2.75–19.76) | <0.001 |
| MLR | 4.70 (1.92–11.48) | 0.001 |
| LMR | - | - |
| PWR | - | - |
| PNR | - | - |
| SII | - | - |
| NLR | - | - |
| Inflammatory Biomarkers | Subgroup | OR * (95% CI) | p | p for Interaction |
|---|---|---|---|---|
| WBC | WFNS 1–3 | 1.13 (1.04–1.22) | 0.003 | <0.001 |
| WFNS 4–5 | 1.17 (1.07–1.27) | <0.001 | ||
| SIRI | WFNS 1–3 | 1.11 (1.04–1.20) | 0.003 | 0.697 |
| WFNS 4–5 | 1.07 (1.01–1.23) | 0.016 | ||
| NEUT | WFNS 1–3 | 1.13 (1.04–1.22) | 0.006 | <0.001 |
| WFNS 4–5 | 1.16 (1.06–1.27) | 0.001 | ||
| NAR | WFNS 1–3 | 63.17 (2.28–1752.82) | 0.014 | <0.001 |
| WFNS 4–5 | 71.25 (2.26–2249.10) | 0.015 | ||
| MONO | WFNS 1–3 | 11.65 (2.70–50.25) | 0.001 | <0.001 |
| WFNS 4–5 | 5.41 (1.66–17.64) | 0.005 | ||
| MLR | WFNS 1–3 | 8.94 (2.37–33.75) | 0.001 | 0.505 |
| WFNS 4–5 | 3.55 (1.15–10.93) | 0.028 | ||
| LMR | WFNS 1–3 | - | - | 0.074 |
| WFNS 4–5 | - | - | ||
| PWR | WFNS 1–3 | - | - | 0.063 |
| WFNS 4–5 | - | - | ||
| PNR | WFNS 1–3 | - | - | 0.110 |
| WFNS 4–5 | - | - | ||
| SII | WFNS 1–3 | 1.00 (1.00–1.00) | 0.011 | 0.527 |
| WFNS 4–5 | - | - | ||
| NLR | WFNS 1–3 | - | - | 0.806 |
| WFNS 4–5 | - | - |
| Inflammatory Biomarkers | Subgroup | OR * (95% CI) | p | p for Interaction |
|---|---|---|---|---|
| WBC | Surgical clipping | 1.18 (1.08–1.27) | <0.001 | 0.012 |
| Endovascular coiling | 1.13 (1.04–1.23) | 0.006 | ||
| SIRI | Surgical clipping | 1.10 (1.04–1.17) | 0.001 | 0.020 |
| Endovascular coiling | - | - | ||
| NEUT | Surgical clipping | 1.17 (1.08–1.26) | <0.001 | 0.014 |
| Endovascular coiling | 1.13 (1.03–1.24) | 0.011 | ||
| NAR | Surgical clipping | 855.57 (23.85–30,698.28) | <0.001 | 0.005 |
| Endovascular coiling | - | - | ||
| MONO | Surgical clipping | 17.46 (4.22–72.19) | <0.001 | 0.006 |
| Endovascular coiling | - | - | ||
| MLR | Surgical clipping | 7.55 (2.29–24.97) | 0.001 | 0.009 |
| Endovascular coiling | - | - | ||
| LMR | Surgical clipping | 0.72 (0.55–0.93) | 0.013 | 0.258 |
| Endovascular coiling | - | - | ||
| PWR | Surgical clipping | - | - | 0.304 |
| Endovascular coiling | - | - | ||
| PNR | Surgical clipping | - | - | 0.234 |
| Endovascular coiling | - | - | ||
| SII | Surgical clipping | 1.00 (1.00–1.00) | 0.018 | 0.358 |
| Endovascular coiling | - | - | ||
| NLR | Surgical clipping | - | - | 0.751 |
| Endovascular coiling | - | - |
| Inflammatory Biomarkers | WFNS | mFS | Graeb | ||||||
|---|---|---|---|---|---|---|---|---|---|
| WFNS 1–3 | WFNS 4–5 | p | mFS 1–2 | mFS 3–4 | p | Graeb 0–4 | Graeb 5–12 | p | |
| WBC *, median (IQR) | 11.70 (9.35–14.33) | 15.54 (12.10–18.77) | <0.001 | 10.82 (8.35–12.94) | 12.79 (10.46–15.94) | <0.001 | 12.12 (9.55–15.17) | 15.87 (13.23–18.93) | <0.001 |
| SIRI, median (IQR) | 3.64 (2.32–5.92) | 6.71 (3.60–12.61) | <0.001 | 3.04 (1.78–4.52) | 4.76 (2.80–8.35) | <0.001 | 3.95 (2.45–6.71) | 8.38 (4.27–13.28) | <0.001 |
| NEUT *, median (IQR) | 10.27 (7.70–12.74) | 13.53 (10.57–16.92) | <0.001 | 9.12 (6.73–11.43) | 11.39 (8.91–14.37) | <0.001 | 10.68 (8.08–13.47) | 14.37 (11.76–16.74) | <0.001 |
| NAR, median (IQR) | 0.24 (0.19–0.30) | 0.31 (0.25–0.39) | <0.001 | 0.22 (0.16–0.27) | 0.27 (0.21–0.34) | <0.001 | 0.25 (0.19–0.31) | 0.32 (0.28–0.40) | <0.001 |
| MONO *, median (IQR) | 0.39 (0.26–0.54) | 0.53 (0.34–0.75) | <0.001 | 0.40 (0.26–0.54) | 0.41 (0.28–0.59) | 0.128 | 0.39 (0.27–0.57) | 0.54 (0.40–0.89) | <0.001 |
| MLR, median (IQR) | 0.37 (0.26–0.53) | 0.53 (0.35–0.76) | <0.001 | 0.33 (0.24–0.44) | 0.42 (0.29–0.62) | <0.001 | 0.38 (0.27–0.56) | 0.63 (0.37–0.86) | <0.001 |
| LMR, median (IQR) | 2.71 (1.89–3.83) | 1.88 (1.31–2.93) | <0.001 | 3.00 (2.25–4.11) | 2.40 (1.61–3.46) | <0.001 | 2.61 (1.78–3.73) | 1.59 (1.17–2.70) | <0.001 |
| PWR, median (IQR) | 19.40 (15.53–23.72) | 14.69 (12.14–19.10) | <0.001 | 22.02 (16.58–26.69) | 17.37 (13.88–22.40) | <0.001 | 18.61 (14.79–23.43) | 14.07 (9.53–19.20) | <0.001 |
| PNR, median (IQR) | 22.33 (17.44–28.84) | 16.59 (13.35–20.95) | <0.001 | 25.71 (20.31–31.52) | 19.43 (15.46–25.94) | <0.001 | 21.36 (16.29–27.62) | 15.29 (10.63–21.17) | <0.001 |
| SII, median (IQR) | 2478 (1528–3588) | 3130 (1995–5072) | <0.001 | 1972 (1175–3052) | 2733 (1754–4156) | <0.001 | 2524 (1609–3827) | 3145 (2218–4232) | 0.039 |
| NLR, median (IQR) | 10.92 (6.91–15.68) | 13.27 (8.88–22.44) | <0.001 | 8.33 (5.13–12.94) | 12.18 (8.14–18.66) | <0.001 | 11.46 (7.28–16.71) | 14.78 (8.89–20.86) | 0.010 |
| Patient Characteristics | Before Propensity Score Matching | After Propensity Score Matching | ||||
|---|---|---|---|---|---|---|
| mRS 0–2 | mRS 3–6 | p | mRS 0–2 | mRS 3–6 | p | |
| No. of patients | 447 | 96 | 86 | 86 | ||
| Female, n (%) | 256 (57.3) | 51 (53.1) | 0.457 | 50 (58.1) | 43 (50.0) | 0.284 |
| Age, years, mean ± SD | 53.9 ± 11.0 | 58.7 ± 10.8 | <0.001 | 57.8 ± 10.6 | 58.0 ± 10.9 | 0.898 |
| Current smoking, n (%) | 134 (30.0) | 27 (28.1) | 0.718 | 23 (26.7) | 27 (31.4) | 0.502 |
| Hypertension, n (%) | 255 (57.0) | 71 (74.0) | 0.002 | 68 (79.1) | 62 (72.1) | 0.287 |
| Hyperlipidemia, n (%) | 40 (8.9) | 7 (7.3) | 0.600 | 7 (8.1) | 5 (5.8) | 0.549 |
| Diabetes mellitus, n (%) | 35 (7.8) | 10 (10.4) | 0.404 | 7 (8.1) | 9 (10.5) | 0.600 |
| Posterior circulation, n (%) | 53 (11.9) | 11 (11.5) | 0.913 | 14 (16.3) | 10 (11.6) | 0.379 |
| WFNS grade 4–5, n (%) | 73 (16.3) | 56 (58.3) | <0.001 | 45 (52.3) | 46 (53.5) | 0.879 |
| mFS grade 3–4, n (%) | 339 (75.8) | 89 (92.7) | <0.001 | 83 (96.5) | 79 (91.9) | 0.192 |
| Graeb score 5–12, n (%) | 26 (5.8) | 22 (22.9) | <0.001 | 13 (15.1) | 16 (18.6) | 0.541 |
| SEBES score 3–4, n (%) | 213 (47.7) | 50 (52.1) | 0.430 | 41 (47.7) | 45 (52.3) | 0.542 |
| Acute hydrocephalus, n (%) | 175 (39.1) | 50 (52.1) | 0.020 | 47 (54.7) | 44 (51.2) | 0.647 |
| Surgical clipping, n (%) | 200 (44.7) | 54 (56.3) | 0.040 | 43 (50.0) | 48 (55.8) | 0.445 |
| Variables | WBC * | SIRI | NEUT * | ||||||
| >14.82 | ≤14.82 | p | >6.77 | ≤6.77 | p | >11.39 | ≤11.39 | p | |
| N = 80 | N = 92 | N = 74 | N = 98 | N = 100 | N = 72 | ||||
| Delayed cerebral ischemia, n (%) | 36 (45.0) | 34 (37.0) | 0.284 | 33 (44.6) | 37 (37.8) | 0.366 | 42 (42.0) | 28 (38.9) | 0.682 |
| Intracranial infection, n (%) | 12 (15.0) | 10 (10.9) | 0.419 | 8 (10.8) | 14 (14.3) | 0.499 | 15 (15.0) | 7 (9.7) | 0.307 |
| Stress ulcer bleeding, n (%) | 19 (23.8) | 29 (31.5) | 0.257 | 22 (29.7) | 26 (26.5) | 0.643 | 24 (24.0) | 24 (33.3) | 0.178 |
| Hypoproteinemia, n (%) | 40 (50.0) | 38 (41.3) | 0.253 | 35 (47.3) | 43 (43.9) | 0.656 | 47 (47.0) | 31 (43.1) | 0.608 |
| Pneumonia, n (%) | 55 (68.8) | 38 (41.3) | <0.001 | 49 (66.2) | 44 (44.9) | 0.006 | 63 (63.0) | 30 (41.7) | 0.006 |
| Deep vein thrombosis, n (%) | 13 (16.3) | 12 (13.0) | 0.552 | 14 (18.9) | 11 (11.2) | 0.156 | 16 (16.0) | 9 (12.5) | 0.521 |
| Variables | NAR | MONO * | MLR | ||||||
| >0.29 | ≤0.29 | p | >0.55 | ≤0.55 | p | >0.56 | ≤0.56 | p | |
| N = 86 | N = 86 | N = 67 | N = 105 | N = 69 | N = 103 | ||||
| Delayed cerebral ischemia, n (%) | 37 (43.0) | 33 (38.4) | 0.535 | 28 (41.8) | 42 (40.0) | 0.816 | 28 (40.6) | 42 (40.8) | 0.979 |
| Intracranial infection, n (%) | 13 (15.1) | 9 (10.5) | 0.361 | 13 (19.4) | 9 (8.6) | 0.038 | 8 (11.6) | 14 (13.6) | 0.701 |
| Stress ulcer bleeding, n (%) | 23 (26.7) | 25 (29.1) | 0.734 | 20 (29.9) | 28 (26.7) | 0.650 | 20 (29.0) | 28 (27.2) | 0.796 |
| Hypoproteinemia, n (%) | 43 (50.0) | 35 (40.7) | 0.221 | 30 (44.8) | 48 (45.7) | 0.904 | 31 (44.9) | 47 (45.6) | 0.928 |
| Pneumonia, n (%) | 59 (68.6) | 34 (39.5) | <0.001 | 40 (59.7) | 53 (50.5) | 0.236 | 45 (65.2) | 48 (46.6) | 0.016 |
| Deep vein thrombosis, n (%) | 14 (16.3) | 11 (12.8) | 0.516 | 13 (19.4) | 12 (11.4) | 0.148 | 12 (17.4) | 13 (12.6) | 0.384 |
| Variables | LMR | PWR | PNR | ||||||
| <1.79 | ≥1.79 | p | <15.62 | ≥15.62 | p | <20.72 | ≥20.72 | p | |
| N = 71 | N = 101 | N = 80 | N = 92 | N = 102 | N = 70 | ||||
| Delayed cerebral ischemia, n (%) | 30 (42.3) | 40 (39.6) | 0.728 | 33 (41.3) | 37 (40.2) | 0.891 | 40 (39.2) | 30 (42.9) | 0.633 |
| Intracranial infection, n (%) | 8 (11.3) | 14 (13.9) | 0.616 | 12 (15.0) | 10 (10.9) | 0.419 | 15 (14.7) | 7 (10.0) | 0.364 |
| Stress ulcer bleeding, n (%) | 20 (28.2) | 28 (27.7) | 0.949 | 22 (27.5) | 26 (28.3) | 0.912 | 30 (29.4) | 18 (25.7) | 0.595 |
| Hypoproteinemia, n (%) | 33 (46.5) | 45 (44.6) | 0.803 | 38 (47.5) | 40 (43.5) | 0.597 | 50 (49.0) | 28 (40.0) | 0.243 |
| Pneumonia, n (%) | 47 (66.2) | 46 (45.5) | 0.008 | 53 (66.3) | 40 (43.5) | 0.003 | 64 (62.7) | 29 (41.4) | 0.006 |
| Deep vein thrombosis, n (%) | 12 (16.9) | 13 (12.9) | 0.460 | 14 (17.5) | 11 (12.0) | 0.304 | 19 (18.6) | 6 (8.6) | 0.066 |
| Variables | SII | NLR | |||||||
| >3102 | ≤3102 | p | >14.88 | ≤14.88 | p | ||||
| N = 84 | N = 88 | N = 74 | N = 98 | ||||||
| Delayed cerebral ischemia, n (%) | 36 (42.9) | 34 (38.6) | 0.573 | 31 (41.9) | 39 (39.8) | 0.782 | |||
| Intracranial infection, n (%) | 13 (15.5) | 9 (10.2) | 0.303 | 12 (16.2) | 10 (10.2) | 0.243 | |||
| Stress ulcer bleeding, n (%) | 22 (26.2) | 26 (29.5) | 0.624 | 18 (24.3) | 30 (30.6) | 0.363 | |||
| Hypoproteinemia, n (%) | 43 (51.2) | 35 (39.8) | 0.133 | 37 (50.0) | 41 (41.8) | 0.287 | |||
| Pneumonia, n (%) | 55 (65.5) | 38 (43.2) | 0.003 | 47 (63.5) | 46 (46.9) | 0.031 | |||
| Deep vein thrombosis, n (%) | 14 (16.7) | 11 (12.5) | 0.438 | 14 (18.9) | 11 (11.2) | 0.156 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nie, Z.; Lin, F.; Li, R.; Chen, X.; Zhao, Y. A Pooled Analysis of Preoperative Inflammatory Biomarkers to Predict 90-Day Outcomes in Patients with an Aneurysmal Subarachnoid Hemorrhage: A Single-Center Retrospective Study. Brain Sci. 2023, 13, 257. https://doi.org/10.3390/brainsci13020257
Nie Z, Lin F, Li R, Chen X, Zhao Y. A Pooled Analysis of Preoperative Inflammatory Biomarkers to Predict 90-Day Outcomes in Patients with an Aneurysmal Subarachnoid Hemorrhage: A Single-Center Retrospective Study. Brain Sciences. 2023; 13(2):257. https://doi.org/10.3390/brainsci13020257
Chicago/Turabian StyleNie, Zhaobo, Fa Lin, Runting Li, Xiaolin Chen, and Yuanli Zhao. 2023. "A Pooled Analysis of Preoperative Inflammatory Biomarkers to Predict 90-Day Outcomes in Patients with an Aneurysmal Subarachnoid Hemorrhage: A Single-Center Retrospective Study" Brain Sciences 13, no. 2: 257. https://doi.org/10.3390/brainsci13020257