
Executive Function Deficits and Borderline Personality Disorder Symptomatology in a Nonclinical Adult Sample: A Latent Variable Analysis
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. Borderline Personality Disorder Symptomatology
2.2.2. Updating-Working Memory Capacity
Colour Keep-Track Task
Letter Keep-Track Task
Number Keep-Track Task
2.2.3. Inhibitory Control
Simon Task
Erikson-Flanker Task
Stroop Task
2.2.4. Cognitive Flexibility
Animacy-Locomotion Task
Colour-Shape Task
Magnitude-Parity Task
2.3. Procedure
2.4. Plan of Analysis
2.5. Transparency and Openness
3. Results
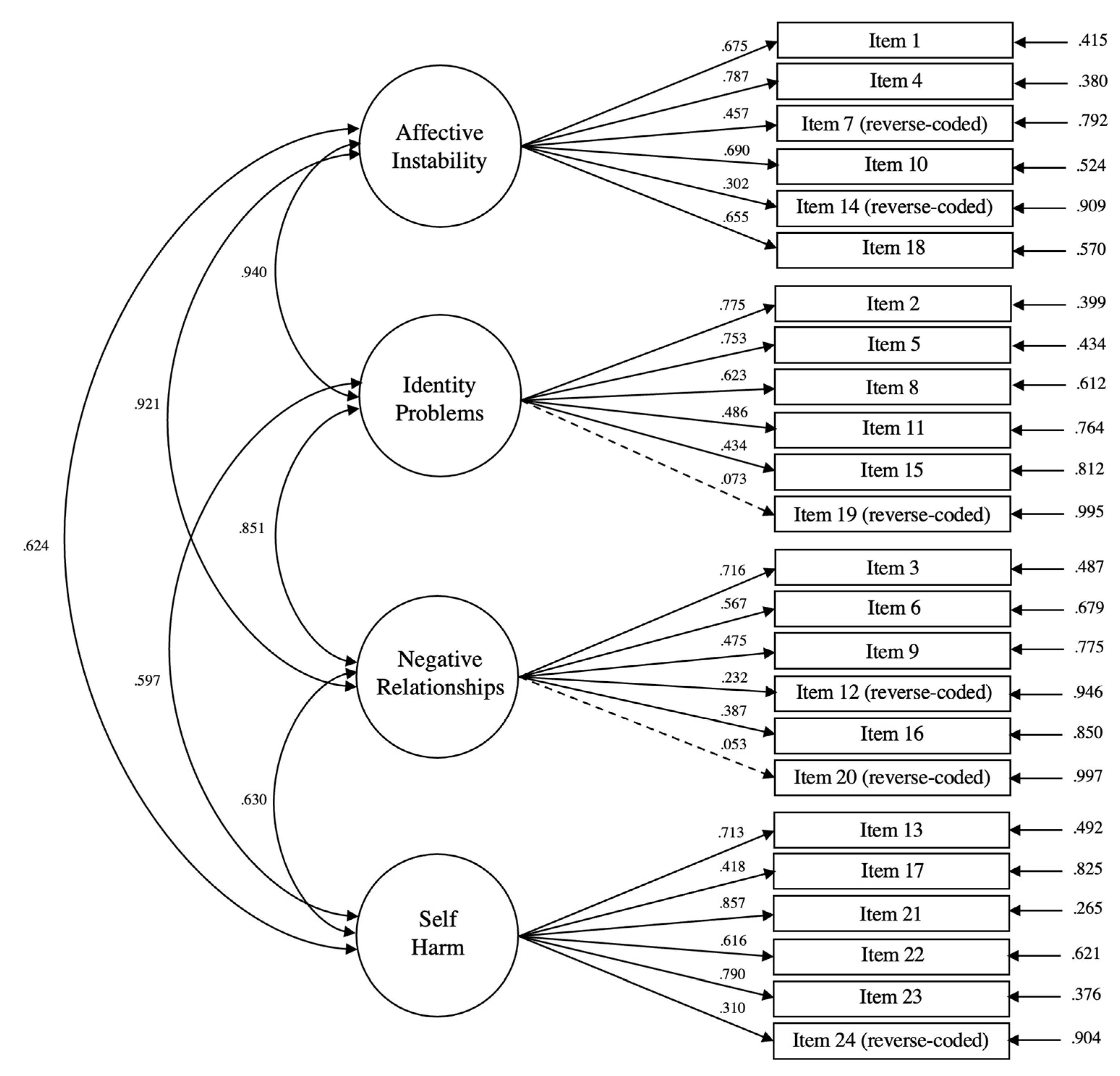
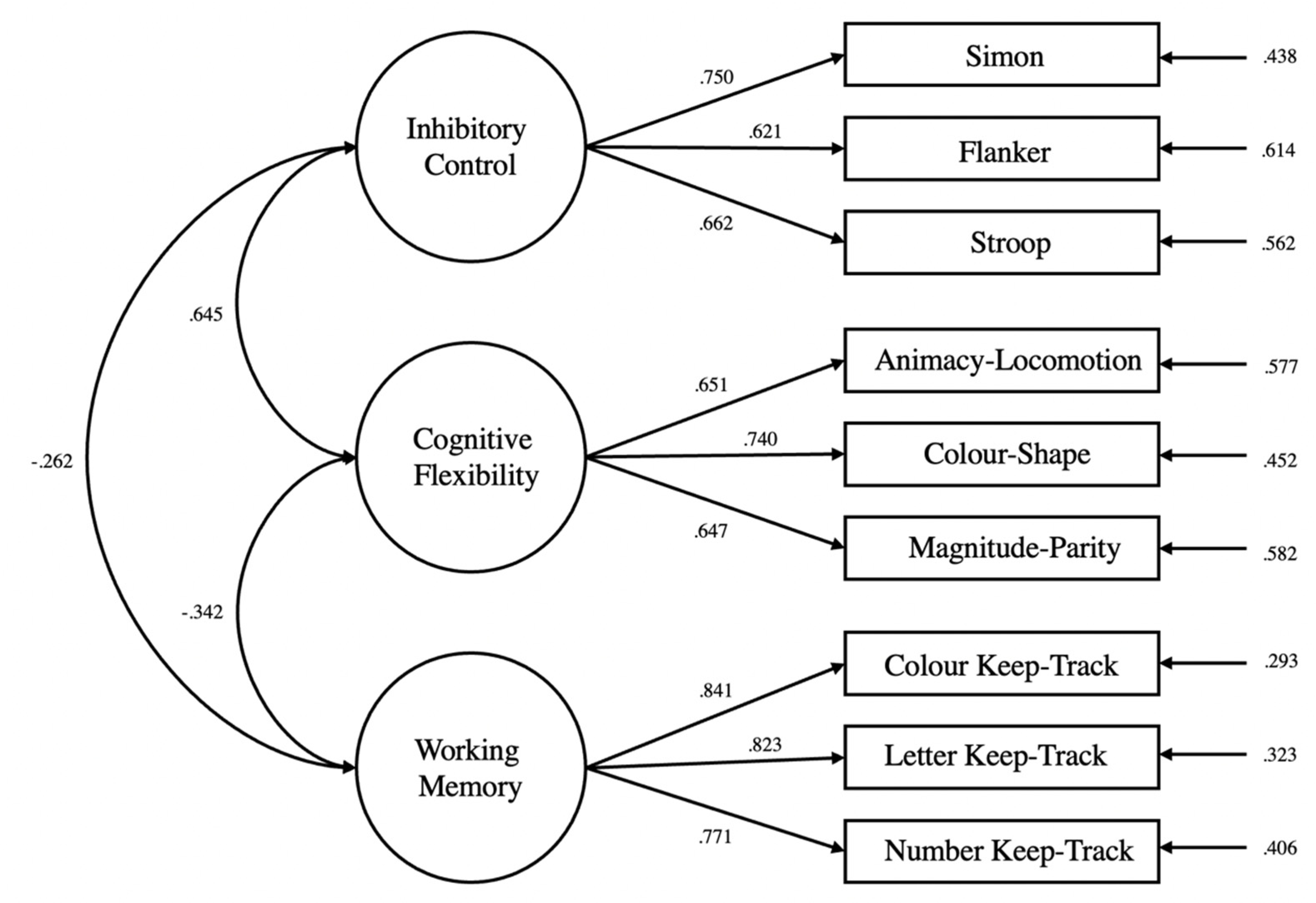
3.1. Confirmatory Factor Analysis
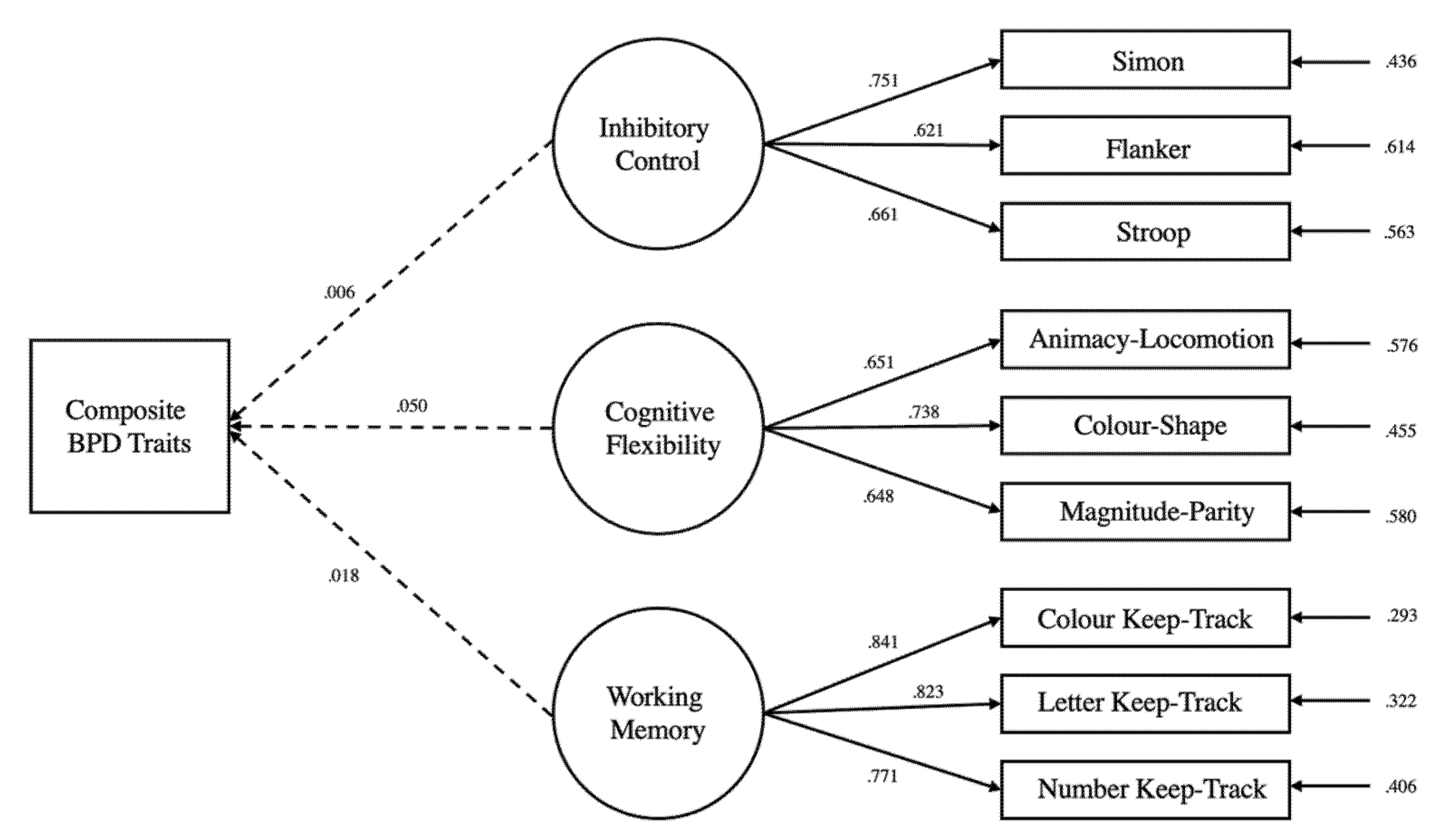
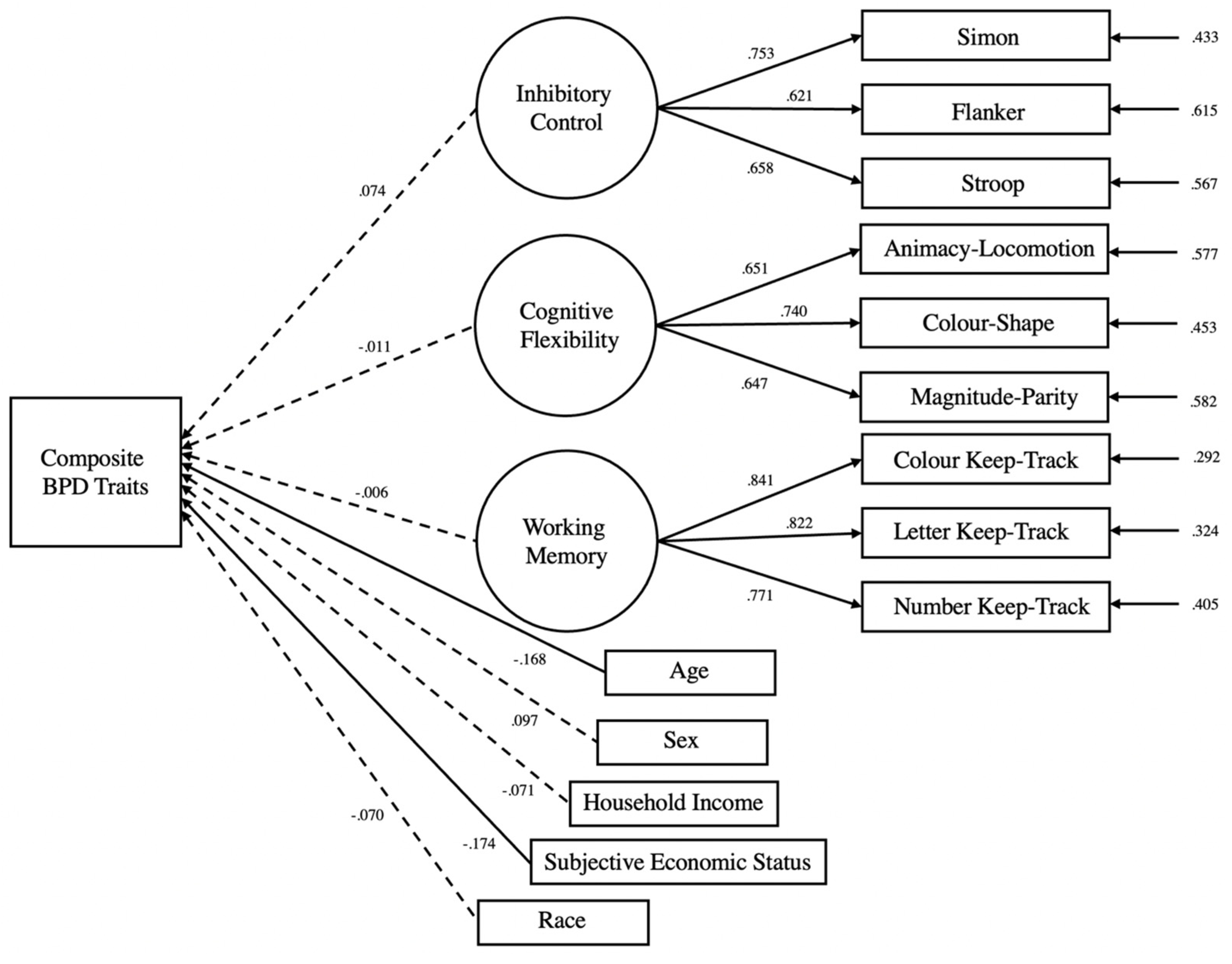
3.2. Structural Equation Modelling
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Paris, J. Borderline personality disorder. Can. Med Assoc. J. 2005, 172, 1579–1583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cleary, M.; Siegfried, N.; Walter, G. Experience, knowledge and attitudes of mental health staff regarding clients with a borderline personality disorder. Int. J. Ment. Health Nurs. 2002, 11, 186–191. [Google Scholar] [CrossRef]
- Sulzer, S.H. Does “difficult patient” status contribute to de facto demedicalization? The case of borderline personality disorder. Soc. Sci. Med. 2015, 142, 82–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, A.; Links, P.S. Aggression in Borderline Personality Disorder: Evidence for Increased Risk and Clinical Predictors. Curr. Psychiatry Rep. 2011, 14, 62–69. [Google Scholar] [CrossRef] [PubMed]
- IsHak, W.W.; Elbau, I.; Ismail, A.; Delaloye, S.; Ha, K.; Bolotaulo, N.I.; Nashawati, R.; Cassmassi, B.; Wang, C. Quality of Life in Borderline Personality Disorder. Harv. Rev. Psychiatry 2013, 21, 138–150. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar] [CrossRef]
- Sayrs, J.; Whiteside, U. Borderline Personality Disorder. In Practitioner’s Guide to Evidence-Based Psychotherapy; Fisher, J.E., O’Donohue, W.T., Eds.; Springer: Chicago, IL, USA, 2006; pp. 151–160. [Google Scholar] [CrossRef]
- Aviram, R.B.; Brodsky, B.S.; Stanley, B. Borderline Personality Disorder, Stigma, and Treatment Implications. Harv. Rev. Psychiatry 2006, 14, 249–256. [Google Scholar] [CrossRef]
- Coolidge, F.L.; Segal, D.L.; Stewart, S.E.; Ellett, J.A. Neuropsychological Dysfunction in Children with Borderline Personality Disorder Features: A Preliminary Investigation. J. Res. Pers. 2000, 34, 554–561. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, C.A.; Thompson, K.N.; Nicholas, C.L.; Hartmann, J.A.; Chanen, A.M. Potential mechanisms underlying sleep disturbance in young people with borderline personality disorder features: An exploratory study. Bord. Pers. Disord. Emot. Dysregulation 2022, 9, 1–13. [Google Scholar] [CrossRef]
- Paris, J. Suicidality in Borderline Personality Disorder. Medicina 2019, 55, 223. [Google Scholar] [CrossRef] [Green Version]
- Paris, J.; Zweig-Frank, H. A 27-year follow-up of patients with borderline personality disorder. Compr. Psychiatry 2001, 42, 482–487. [Google Scholar] [CrossRef]
- Shen, C.; Wang, M.P.; Chu, J.T.; Wan, A.; Viswanath, K.; Chan, S.S.C.; Lam, T.H.; Bacigalupe, G.; Zhang, M.; Sapkota, B.; et al. Sharing Family Life Information Through Video Calls and Other Information and Communication Technologies and the Association With Family Well-Being: Population-Based Survey. JMIR Ment. Health 2017, 4, e57. [Google Scholar] [CrossRef] [PubMed]
- Lieb, K.; Zanarini, M.C.; Schmahl, C.; Linehan, M.M.; Bohus, M. Borderline personality disorder. Lancet 2004, 364, 453–461. [Google Scholar] [CrossRef]
- Stone, M.H.; Friedman, H.J. The Fate of Borderline Patients: Successful Outcome and Psychiatric Practice; Guilford Press: New York, NY, USA, 1990. [Google Scholar]
- Trull, T.J. Borderline personality disorder features in nonclinical young adults: 1. Identification and validation. Psychol. Assess. 1995, 7, 33–41. [Google Scholar] [CrossRef]
- Ellison, W.D.; Rosenstein, L.K.; Morgan, T.A.; Zimmerman, M. Community and Clinical Epidemiology of Borderline Personality Disorder. Psychiatr. Clin. North Am. 2018, 41, 561–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winsper, C.; Zanarini, M.; Wolke, D. Prospective study of family adversity and maladaptive parenting in childhood and borderline personality disorder symptoms in a non-clinical population at 11 years. Psychol. Med. 2012, 42, 2405–2420. [Google Scholar] [CrossRef] [Green Version]
- Fonseca-Pedrero, E.; Paino, M.; Lemos-Giráldez, S.; Sierra-Baigrie, S.; González, M.P.G.-P.; Bobes, J.; Muňiz, J. Borderline Personality Traits in Nonclinical Young Adults. J. Pers. Disord. 2011, 25, 542–556. [Google Scholar] [CrossRef] [Green Version]
- Daley, S.E.; Burge, D.; Hammen, C. Borderline personality disorder symptoms as predictors of 4-year romantic relationship dysfunction in young women: Addressing issues of specificity. J. Abnorm. Psychol. 2000, 109, 451–460. [Google Scholar] [CrossRef]
- Vega, D.; Torrubia, R.; Marco-Pallarés, J.; Soto, A.; Rodriguez-Fornells, A. Metacognition of daily self-regulation processes and personality traits in borderline personality disorder. J. Affect. Disord. 2020, 267, 243–250. [Google Scholar] [CrossRef]
- Németh, N.; Péterfalvi, Á.; Czéh, B.; Tényi, T.; Simon, M. Examining the Relationship Between Executive Functions and Mentalizing Abilities of Patients With Borderline Personality Disorder. Front. Psychol. 2020, 11, 1583. [Google Scholar] [CrossRef]
- McClure, G.; Hawes, D.J.; Dadds, M. Borderline personality disorder and neuropsychological measures of executive function: A systematic review. Pers. Ment. Health 2015, 10, 43–57. [Google Scholar] [CrossRef]
- Wright, A.G.C.; Hallquist, M.N.; Stepp, S.; Scott, L.N.; Beeney, J.E.; Lazarus, S.A.; Pilkonis, P.A. Modeling Heterogeneity in Momentary Interpersonal and Affective Dynamic Processes in Borderline Personality Disorder. Assessment 2016, 23, 484–495. [Google Scholar] [CrossRef] [Green Version]
- Miyake, A.; Friedman, N.P.; Emerson, M.J.; Witzki, A.H.; Howerter, A.; Wager, T.D. The Unity and Diversity of Executive Functions and Their Contributions to Complex “Frontal Lobe” Tasks: A Latent Variable Analysis. Cogn. Psychol. 2000, 41, 49–100. [Google Scholar] [CrossRef] [Green Version]
- Diamond, A. Executive Functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frontiers | A Bidirectional Relationship between Executive Function and Health Behavior: Evidence, Implica-tions, and Future Directions. Available online: https://www.frontiersin.org/articles/10.3389/fnins.2016.00386/full (accessed on 29 December 2022).
- Ng, W.Q.; Hartanto, A. The effect of executive function on the development of chronic pain: A prospective longitudinal study. Soc. Sci. Med. 2022, 314, 115478. [Google Scholar] [CrossRef] [PubMed]
- Hartanto, A.; Yong, J.C.; Toh, W.X. Bidirectional Associations between Obesity and Cognitive Function in Midlife Adults: A Longitudinal Study. Nutrients 2019, 11, 2343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, J.K.; Lui, L.-Y.; Yaffe, K. Executive Function, More Than Global Cognition, Predicts Functional Decline and Mortality in Elderly Women. J. Gerontol. Ser. A 2007, 62, 1134–1141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- St Clair-Thompson, H.L.; Gathercole, S.E. Executive functions and achievements in school: Shifting, updating, inhibition, and working memory. Q. J. Exp. Psychol. 2006, 59, 745–759. [Google Scholar] [CrossRef]
- Titz, C.; Karbach, J. Working memory and executive functions: Effects of training on academic achievement. Psychol. Res. 2014, 78, 852–868. [Google Scholar] [CrossRef]
- Hartanto, A.; Yang, H.; Yang, S. Bilingualism positively predicts mathematical competence: Evidence from two large-scale studies. Learn. Individ. Differ. 2018, 61, 216–227. [Google Scholar] [CrossRef]
- Hartanto, A.; Yang, H. Testing theoretical assumptions underlying the relation between anxiety, mind wandering, and task-switching: A diffusion model analysis. Emotion 2022, 22, 493–510. [Google Scholar] [CrossRef]
- Pe, M.L.; Koval, P.; Kuppens, P. Executive well-being: Updating of positive stimuli in working memory is associated with subjective well-being. Cognition 2013, 126, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.-S.; Nasir, H.; Pheh, K.-S.; Cong, C.W.; Tay, K.-W.; Cheong, J.-Q. The Mediating Role of Work Engagement in the Relationship between Executive Functioning Deficits and Employee Well-Being. Int. J. Environ. Res. Public Health 2022, 19, 13386. [Google Scholar] [CrossRef] [PubMed]
- Toh, W.X.; Yang, H.; Hartanto, A. Executive Function and Subjective Well-being in Middle and Late Adulthood. J. Gerontol. Ser. B 2019, 75, e69–e77. [Google Scholar] [CrossRef] [PubMed]
- Moriguchi, Y. The early development of executive function and its relation to social interaction: A brief review. Front. Psychol. 2014, 5, 388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riggs, N.R.; Jahromi, L.B.; Razza, R.P.; Dillworth-Bart, J.E.; Mueller, U. Executive function and the promotion of social–emotional competence. J. Appl. Dev. Psychol. 2006, 27, 300–309. [Google Scholar] [CrossRef]
- Cropley, M.; Collis, H. The Association Between Work-Related Rumination and Executive Function Using the Behavior Rating Inventory of Executive Function. Front. Psychol. 2020, 11. [Google Scholar] [CrossRef]
- Fisher, G.G.; Chaffee, D.S.; Tetrick, L.E.; Davalos, D.B.; Potter, G.G. Cognitive functioning, aging, and work: A review and recommendations for research and practice. J. Occup. Health Psychol. 2017, 22, 314–336. [Google Scholar] [CrossRef]
- Collins, A.; Koechlin, E. Reasoning, Learning, and Creativity: Frontal Lobe Function and Human Decision-Making. PLOS Biol. 2012, 10, e1001293. [Google Scholar] [CrossRef]
- Hagenhoff, M.; Franzen, N.; Koppe, G.; Baer, N.; Scheibel, N.; Sammer, G.; Gallhofer, B.; Lis, S. Executive functions in borderline personality disorder. Psychiatry Res. 2013, 210, 224–231. [Google Scholar] [CrossRef]
- Putnam, K.M.; Silk, K.R. Emotion dysregulation and the development of borderline personality disorder. Dev. Psychopathol. 2005, 17, 899–925. [Google Scholar] [CrossRef]
- Bickel, W.K.; Jarmolowicz, D.P.; Mueller, E.T.; Gatchalian, K.M.; McClure, S.M. Are executive function and impulsivity antipodes? A conceptual reconstruction with special reference to addiction. Psychopharmacology 2012, 221, 361–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hendrawan, D.; Yamakawa, K.; Kimura, M.; Murakami, H.; Ohira, H. Executive functioning performance predicts subjective and physiological acute stress reactivity: Preliminary results. Int. J. Psychophysiol. 2012, 84, 277–283. [Google Scholar] [CrossRef]
- Lantrip, C.; Isquith, P.K.; Koven, N.S.; Welsh, K.; Roth, R.M. Executive Function and Emotion Regulation Strategy Use in Adolescents. Appl. Neuropsychol. Child 2014, 5, 50–55. [Google Scholar] [CrossRef]
- Marceau, E.M.; Kelly, P.J.; Solowij, N. The relationship between executive functions and emotion regulation in females attending therapeutic community treatment for substance use disorder. Drug Alcohol Depend. 2018, 182, 58–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyake, A.; Emerson, M.J.; Friedman, N.P. Assessment of executive functions in clinical settings: Problems and recommendations. Semin. Speech Lang. 2000, 21, 0169–0183. [Google Scholar] [CrossRef] [PubMed]
- Friedman, N.P.; Miyake, A. The Relations Among Inhibition and Interference Control Functions: A Latent-Variable Analysis. J. Exp. Psychol. Gen. 2004, 133, 101–135. [Google Scholar] [CrossRef] [Green Version]
- Carr, S.; Francis, A. Childhood maltreatment and adult personality disorder symptoms in a non-clinical sample. Aust. Psychol. 2009, 44, 146–155. [Google Scholar] [CrossRef]
- Morey, L.C. Personality Assessment Inventory: Professional Manual; Psychological Assessment Resources: Odessa, FL, USA, 1991. [Google Scholar]
- Hartanto, A.; Lee, K.Y.X.; Chua, Y.J.; Quek, F.Y.X.; Majeed, N.M. Smartphone use and daily cognitive failures: A critical examination using a daily diary approach with objective smartphone measures. Br. J. Psychol. 2022. [Google Scholar] [CrossRef]
- Ng, M.H.; Lua, V.Y.; Majeed, N.M.; Hartanto, A. Does trait self-esteem serve as a protective factor in maintaining daily affective well-being? Multilevel analyses of daily diary studies in the US and Singapore. Pers. Individ. Differ. 2022, 198, 111804. [Google Scholar] [CrossRef]
- Lua, V.Y.Q.; Majeed, N.M.; Leung, A.K.-Y.; Hartanto, A. A daily within-person investigation on the link between social expectancies to be busy and emotional wellbeing: The moderating role of emotional complexity acceptance. Cogn. Emot. 2022, 36, 773–780. [Google Scholar] [CrossRef]
- Hartanto, A.; Wong, J.; Lua, V.Y.Q.; Tng, G.Y.Q.; Kasturiratna, K.T.A.S.; Majeed, N.M. A Daily Diary Investigation of the Fear of Missing Out and Diminishing Daily Emotional Well-Being: The Moderating Role of Cognitive Reappraisal. Psychol. Rep. 2022, 00332941221135476. [Google Scholar] [CrossRef]
- Adler, N.E.; Epel, E.S.; Castellazzo, G.; Ickovics, J.R. Relationship of Subjective and Objective Social Status with Psychological and Physiological Functioning: Preliminary Data in Healthy, White Women. Health Psychol. 2000, 19, 586–592. [Google Scholar] [CrossRef]
- von Bastian, C.C.; Souza, A.S.; Gade, M. No evidence for bilingual cognitive advantages: A test of four hypotheses. J. Exp. Psychol. Gen. 2016, 145, 246–258. [Google Scholar] [CrossRef] [PubMed]
- Von Bastian, C.C.; Locher, A.; Ruflin, M. Tatool: A Java-based open-source programming framework for psychological studies. Behav. Res. Methods 2012, 45, 108–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Draheim, C.; Hicks, K.L.; Engle, R.W. Combining Reaction Time and Accuracy. Perspect. Psychol. Sci. 2016, 11, 133–155. [Google Scholar] [CrossRef] [PubMed]
- Simeonova, D.; Paunova, R.; Stoyanova, K.; Todeva-Radneva, A.; Kandilarova, S.; Stoyanov, D. Functional MRI Correlates of Stroop N-Back Test Underpin the Diagnosis of Major Depression. J. Integr. Neurosci. 2022, 21, 113. [Google Scholar] [CrossRef] [PubMed]
- Gärtner, A.; Strobel, A. Individual Differences in Inhibitory Control: A latent Variable Analysis. J. Cogn. 2021, 4, 17. [Google Scholar] [CrossRef]
- West, R.; Alain, C. Age-related decline in inhibitory control contributes to the increased Stroop effect observed in older adults. Psychophysiology 2000, 37, 179–189. [Google Scholar] [CrossRef]
- Friedman, N.P. Research on individual differences in executive functions. Represent. Process. Biling. Morphol. 2016, 6, 535–548. [Google Scholar] [CrossRef] [Green Version]
- Lang, J.A. Validation of the Five Digit Test in a Clinical Sample: An Alternative to the Stroop Color-Word Task with Possible Cultural Implications. Ph.D. Thesis, Alliant International University, Alhambra, CA, USA, 2002. [Google Scholar]
- Wolach, A.H.; McHale, M.A.; Tarlea, A. Numerical Stroop Effect. Percept. Mot. Ski. 2004, 98, 67–77. [Google Scholar] [CrossRef]
- Bush, G.; Whalen, P.J.; Rosen, B.R.; Jenike, M.A.; McInerney, S.C.; Rauch, S.L. The counting stroop: An in-terference task specialized for functional neuroimaging-validation study with functional MRI. Hum. Brain Mapp. 1998, 6, 270–282. [Google Scholar] [CrossRef]
- Bush, G.; Whalen, P.J.; Shin, L.M.; Rauch, S.L. The counting Stroop: A cognitive interference task. Nat. Protoc. 2006, 1, 230–233. [Google Scholar] [CrossRef]
- Szűcs, D.; Soltész, F. Event-related potentials dissociate facilitation and interference effects in the numerical Stroop paradigm. Neuropsychologia 2007, 45, 3190–3202. [Google Scholar] [CrossRef] [PubMed]
- Kaufmann, L.; Ischebeck, A.; Weiss, E.; Koppelstaetter, F.; Siedentopf, C.; Vogel, S.E.; Gotwald, T.; Marksteiner, J.; Wood, G. An fMRI study of the numerical Stroop task in individuals with and without minimal cognitive impairment. Cortex 2008, 44, 1248–1255. [Google Scholar] [CrossRef]
- Hartanto, A.; Yang, H. The role of bilingual interactional contexts in predicting interindividual variability in executive functions: A latent variable analysis. J. Exp. Psychol. Gen. 2020, 149, 609–633. [Google Scholar] [CrossRef]
- Hartanto, A.; Ong, N.C.H.; Ng, W.Q.; Majeed, N.M. The Effect of State Gratitude on Cognitive Flexibility: A Within-Subject Experimental Approach. Brain Sci. 2020, 10, 413. [Google Scholar] [CrossRef]
- Hughes, J.N.; Im, M.H.; Wehrly, S.E. Effect of peer nominations of teacher–student support at individual and classroom levels on social and academic outcomes. J. Sch. Psychol. 2014, 52, 309–322. [Google Scholar] [CrossRef] [Green Version]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Browne, M.W.; Cudeck, R. Alternative ways of assessing model fit. Sociol. Methods Res. 1992, 21, 230–258. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022; Available online: https://www.R-project.org/ (accessed on 23 June 2022).
- Rosseel, Y. lavaan: AnRPackage for Structural Equation Modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef] [Green Version]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 7th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2012. [Google Scholar]
- Bergh, D. Sample Size and Chi-Squared Test of Fit—A Comparison Between a Random Sample Approach and a Chi-Square Value Adjustment Method Using Swedish Adolescent Data. In Pacific Rim Objective Measurement Symposium (PROMS) 2014 Conference Proceedings; Zhang, Q., Yang, H., Eds.; Springer: Berlin, Heidelberg, 2015; pp. 197–211. [Google Scholar] [CrossRef]
- Martin-Löf, P. The Notion of Redundancy and Its Use as a Quantitative Measure of the Discrepancy between a Statistical Hypothesis and a Set of Observational Data [with Discussion]. Scand. J. Stat. 1974, 1, 3–18. [Google Scholar]
- Tyrer, P.; Reed, G.M.; Crawford, M.J. Classification, assessment, prevalence, and effect of personality disorder. Lancet 2015, 385, 717–726. [Google Scholar] [CrossRef] [PubMed]
- Bradley, G.L.; Sparks, B.A.; Weber, K. Perceived prevalence and personal impact of negative online reviews. J. Serv. Manag. 2016, 27, 507–533. [Google Scholar] [CrossRef]
- Weaver, T.L.; Clum, G.A. Early family environments and traumatic experiences associated with borderline personality disorder. J. Consult. Clin. Psychol. 1993, 61, 1068–1075. [Google Scholar] [CrossRef] [PubMed]
- Bourvis, N.; Aouidad, A.; Cabelguen, C.; Cohen, D.; Xavier, J. How Do Stress Exposure and Stress Regulation Relate to Borderline Personality Disorder? Front. Psychol. 2017, 8, 2054. [Google Scholar] [CrossRef] [Green Version]
- Zielinski, M.J.; Veilleux, J.C. Examining the relation between borderline personality features and social support: The mediating role of rejection sensitivity. Pers. Individ. Differ. 2014, 70, 235–238. [Google Scholar] [CrossRef]
- Lavner, J.A.; Lamkin, J.; Miller, J.D. Borderline personality disorder symptoms and newlyweds’ observed communication, partner characteristics, and longitudinal marital outcomes. J. Abnorm. Psychol. 2015, 124, 975–981. [Google Scholar] [CrossRef]
- Levy, K.N. The implications of attachment theory and research for understanding borderline personality disorder. Dev. Psychopathol. 2005, 17, 959–986. [Google Scholar] [CrossRef]
- Friedman, N.P.; Miyake, A.; Young, S.E.; DeFries, J.C.; Corley, R.P.; Hewitt, J.K. Individual differences in executive functions are almost entirely genetic in origin. J. Exp. Psychol. Gen. 2008, 137, 201–225. [Google Scholar] [CrossRef] [Green Version]
- Logue, S.F.; Gould, T.J. The neural and genetic basis of executive function: Attention, cognitive flexibility, and response inhibition. Pharmacol. Biochem. Behav. 2014, 123, 45–54. [Google Scholar] [CrossRef] [Green Version]
- Ferguson, H.J.; Brunsdon, V.E.A.; Bradford, E.E.F. The developmental trajectories of executive function from adolescence to old age. Sci. Rep. 2021, 11, 1382. [Google Scholar] [CrossRef] [PubMed]
- Friedman, N.P.; Miyake, A. Unity and diversity of executive functions: Individual differences as a window on cognitive structure. Cortex 2017, 86, 186–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luciana, M.; Conklin, H.M.; Hooper, C.J.; Yarger, R.S. The Development of Nonverbal Working Memory and Executive Control Processes in Adolescents. Child Dev. 2005, 76, 697–712. [Google Scholar] [CrossRef] [PubMed]
- Hartanto, A.; Toh, W.X.; Yang, H. Age matters: The effect of onset age of video game play on task-switching abilities. Atten. Percept. Psychophys 2016, 78, 1125–1136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Åberg, M.A.I.; Pedersen, N.L.; Torén, K.; Svartengren, M.; Bäckstrand, B.; Johnsson, T.; Cooper-Kuhn, C.M.; Åberg, N.D.; Nilsson, M.; Kuhn, H.G. Cardiovascular fitness is associated with cognition in young adulthood. Proc. Natl. Acad. Sci. USA 2009, 106, 20906–20911. [Google Scholar] [CrossRef] [Green Version]
- Pascual, J.C.; Palomares, N.; Ibáñez, Á.; Portella, M.J.; Arza, R.; Reyes, R.; Feliu-Soler, A.; Díaz-Marsá, M.; Saiz-Ruiz, J.; Soler, J.; et al. Efficacy of cognitive rehabilitation on psychosocial functioning in Borderline Personality Disorder: A randomized controlled trial. BMC Psychiatry 2015, 15, 255. [Google Scholar] [CrossRef] [Green Version]
- Vita, A.; Deste, G.; Barlati, S.; Poli, R.; Cacciani, P.; De Peri, L.; Sacchetti, E. Feasibility and effectiveness of cognitive remediation in the treatment of borderline personality disorder. Neuropsychol. Rehabil. 2016, 28, 416–428. [Google Scholar] [CrossRef]
- Chiappini, S.; Picutti, E.; Alessi, M.C.; Di Carlo, F.; D’Andrea, G.; Miuli, A.; Pettorruso, M.; Martinotti, G.; di Giannantonio, M. Efficacy of Noninvasive Brain Stimulation on Borderline Personality Disorder Core Symptoms: A Systematic Review. J. Pers. Disord. 2022, 36, 505–526. [Google Scholar] [CrossRef]
- Lisoni, J.; Barlati, S.; Deste, G.; Ceraso, A.; Nibbio, G.; Baldacci, G.; Vita, A. Efficacy and tolerability of Brain Stimulation interventions in Borderline Personality Disorder: State of the art and future perspectives—A systematic review. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2022, 116, 110537. [Google Scholar] [CrossRef]
- Videler, A.C.; Hutsebaut, J.; Schulkens, J.E.M.; Sobczak, S.; van Alphen, S.P.J. A Life Span Perspective on Borderline Personality Disorder. Curr. Psychiatry Rep. 2019, 21, 51. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | M (SD) | Observed Range | Theoretical Range | Reliability d | |
|---|---|---|---|---|---|
| Demographics | |||||
| Sex (% female) | 233 | 73% | |||
| Age | 233 | 21.64 (2.00) | 18–30 | ||
| Race (% Ethnic Majority) | 233 | 79% | |||
| Household income a | 233 | 3.15 (1.57) | 1–6 | 1–6 | |
| Subjective socioeconomic status b | 233 | 6.10 (1.35) | 2–9 | 1–10 | |
| Borderline Personality Disorder Trait Dimensions | |||||
| Affective Instability | 233 | 7.03 (3.52) | 0–18 | 0–18 | 0.77 |
| Identity Problems | 233 | 9.14 (3.64) | 1–18 | 0–18 | 0.69 |
| Negative Relationships | 233 | 8.17 (3.23) | 1–17 | 0–18 | 0.53 |
| Self-Harm | 233 | 5.11 (3.73) | 0–18 | 0–18 | 0.79 |
| Executive functions c | |||||
| Colour Keep-Track | 233 | 0.56 (0.17) | 0.09–0.94 | 0.00–1.00 | 0.95 |
| Letter Keep-Track | 233 | 0.72 (0.14) | 0.07–0.99 | 0.00–1.00 | 0.94 |
| Number Keep-Track | 233 | 0.71 (0.21) | 0.16–1.00 | 0.00–1.00 | 0.96 |
| Simon task | 232 | 7.12 (1.71) | 3.28–12.04 | 1–20 | 0.79 |
| Flanker task | 231 | 6.43 (1.31) | 3.72–14.89 | 1–20 | 0.72 |
| Stroop task | 227 | 6.78 (1.38) | 3.49–11.55 | 1–20 | 0.79 |
| Animacy-Size task | 233 | 6.74 (1.18) | 4.38–13.57 | 1–20 | 0.73 |
| Colour-Shape task | 233 | 6.90 (1.30) | 4.36–13.00 | 1–20 | 0.72 |
| Magnitude-Parity task | 233 | 7.13 (1.40) | 3.23–11.93 | 1–20 | 0.75 |
| df | χ2 | pχ2 | AIC | BIC | SRMR | RMSEA | CFI | TLI | |
|---|---|---|---|---|---|---|---|---|---|
| Confirmatory Factor Analysis | |||||||||
| PAI-BOR | 246 | 750.16 | 0.000 | 13610.63 | 13879.81 | 0.081 | 0.094 | 0.758 | 0.729 |
| Executive Functions | 24 | 38.780 | 0.029 | 3748.63 | 3852.16 | 0.047 | 0.051 | 0.977 | 0.966 |
| Structural Equation Modelling | |||||||||
| Unadjusted | |||||||||
| Composite BPD | 30 | 46.082 | 0.031 | 4079.27 | 4200.06 | 0.045 | 0.048 | 0.975 | 0.963 |
| Affective Instability | 30 | 49.680 | 0.013 | 4198.45 | 4319.24 | 0.047 | 0.053 | 0.970 | 0.955 |
| Identity Problem | 30 | 47.560 | 0.022 | 4184.18 | 4304.97 | 0.046 | 0.050 | 0.973 | 0.960 |
| Negative Relationships | 30 | 45.407 | 0.035 | 4128.72 | 4249.50 | 0.045 | 0.047 | 0.976 | 0.964 |
| Self-harm | 30 | 43.834 | 0.049 | 4195.54 | 4316.33 | 0.045 | 0.044 | 0.979 | 0.968 |
| Adjusted | |||||||||
| Composite BPD | 75 | 118.82 | 0.001 | 4067.36 | 4205.40 | 0.056 | 0.050 | 0.937 | 0.920 |
| Affective Instability | 75 | 121.52 | 0.001 | 4184.35 | 4322.39 | 0.056 | 0.052 | 0.934 | 0.916 |
| Identity Problem | 75 | 119.70 | 0.001 | 4169.24 | 4307.28 | 0.056 | 0.051 | 0.936 | 0.919 |
| Negative Relationships | 75 | 118.57 | 0.001 | 4129.56 | 4267.60 | 0.056 | 0.050 | 0.936 | 0.919 |
| Self-harm | 75 | 118.09 | 0.001 | 4196.69 | 4334.73 | 0.056 | 0.050 | 0.937 | 0.920 |
| Composite BPD | Affective Instability | Identity Problems | Negative Relationships | Self-Harm | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Predictor | Unadjusted | Adjusted | Unadjusted | Adjusted | Unadjusted | Adjusted | Unadjusted | Adjusted | Unadjusted | Adjusted |
| Executive Functions | ||||||||||
| Inhibitory control | 0.006 | 0.074 | −0.079 | −0.002 | −0.012 | 0.062 | −0.054 | −0.019 | 0.155 | 0.189 |
| Cognitive flexibility | 0.050 | −0.011 | 0.148 | 0.082 | 0.036 | −0.036 | 0.120 | 0.101 | −0.133 | −0.167 |
| Working memory | 0.018 | −0.006 | 0.017 | 0.001 | 0.097 | 0.054 | 0.004 | 0.011 | −0.059 | −0.081 |
| Covariates | ||||||||||
| Age | −0.168 * | −0.120 | −0.172 * | −0.070 | −0.174 * | |||||
| Sex (0 = male, 1 = female) | 0.097 | 0.157* | 0.131 | 0.013 | 0.005 | |||||
| Household income | −0.071 | −0.080 | −0.052 | −0.089 | −0.013 | |||||
| Subjective socioeconomic status | −0.174 * | −0.180 * | −0.155 * | −0.136 | −0.090 | |||||
| Race (0 = majority, 1 = minority) | −0.070 | −0.042 | −0.130 * | −0.018 | −0.032 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Veerapandian, K.D.; Tan, G.X.D.; Majeed, N.M.; Hartanto, A. Executive Function Deficits and Borderline Personality Disorder Symptomatology in a Nonclinical Adult Sample: A Latent Variable Analysis. Brain Sci. 2023, 13, 206. https://doi.org/10.3390/brainsci13020206
Veerapandian KD, Tan GXD, Majeed NM, Hartanto A. Executive Function Deficits and Borderline Personality Disorder Symptomatology in a Nonclinical Adult Sample: A Latent Variable Analysis. Brain Sciences. 2023; 13(2):206. https://doi.org/10.3390/brainsci13020206
Chicago/Turabian StyleVeerapandian, Keisha D., Gabriel X. D. Tan, Nadyanna M. Majeed, and Andree Hartanto. 2023. "Executive Function Deficits and Borderline Personality Disorder Symptomatology in a Nonclinical Adult Sample: A Latent Variable Analysis" Brain Sciences 13, no. 2: 206. https://doi.org/10.3390/brainsci13020206