
Differences of Modality Use between Telepractice and Face-to-Face Administration of the Scenario-Test in Persons with Dementia-Related Speech Disorder
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Assessment
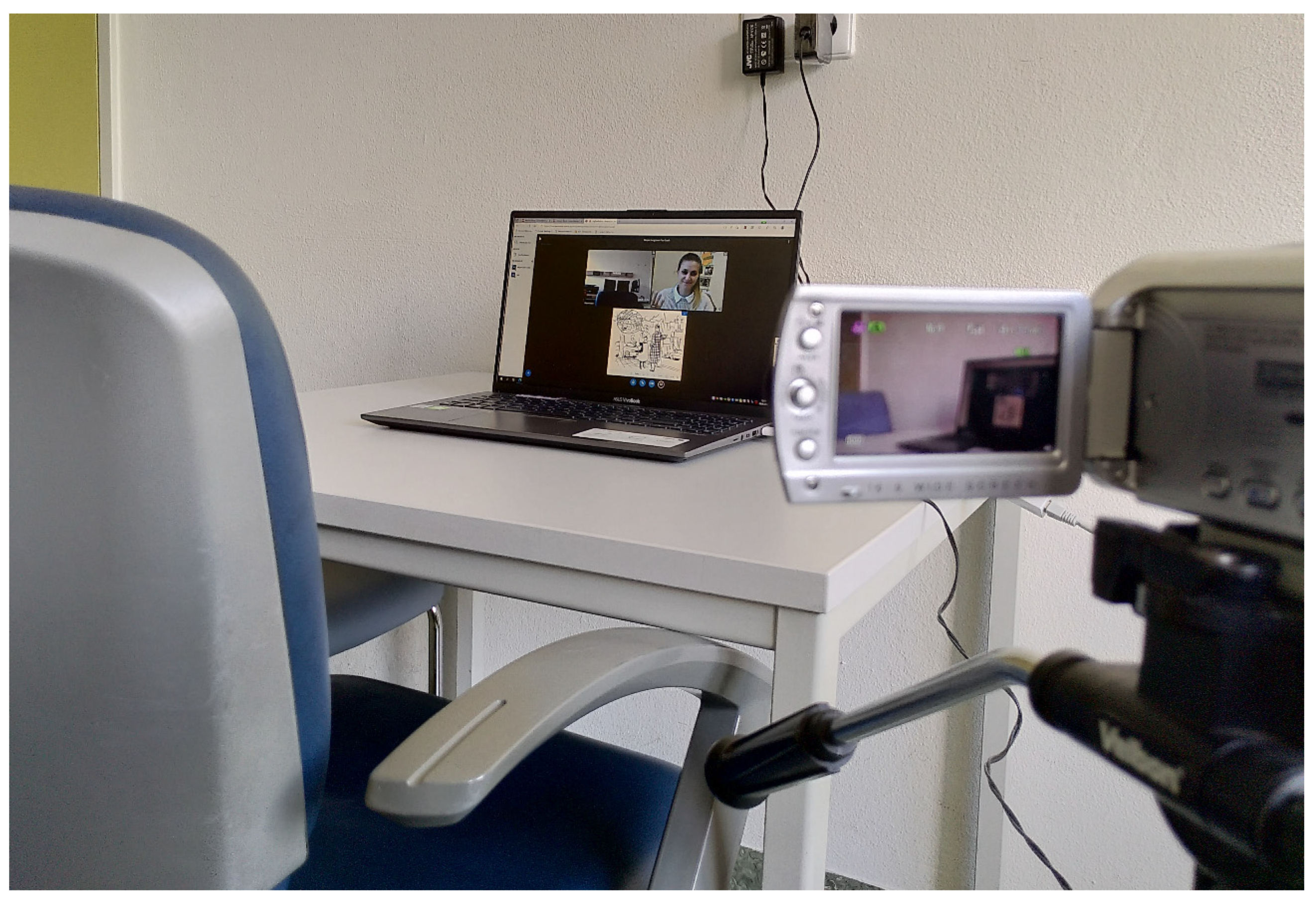
2.2. Procedure
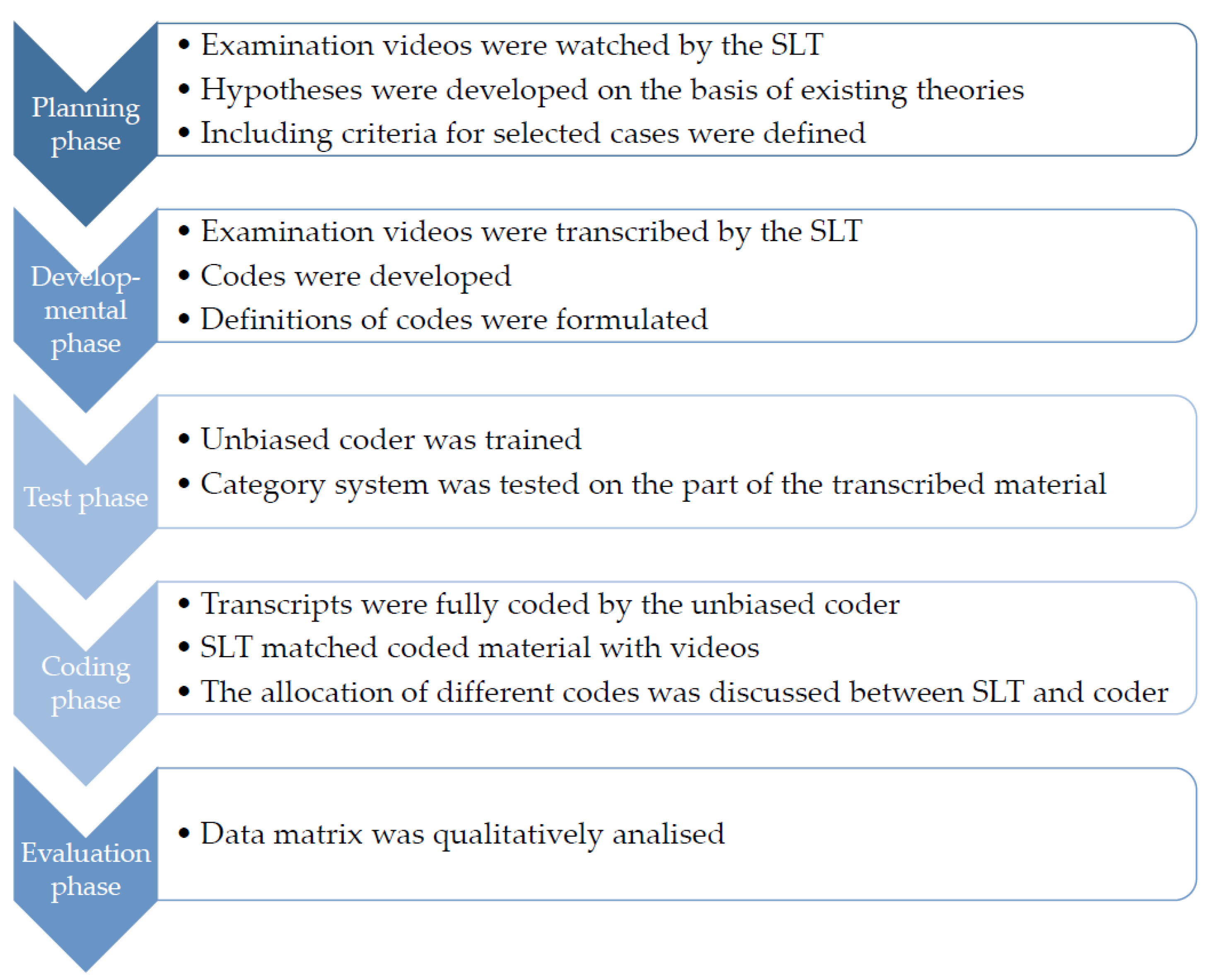
2.3. Qualitative Data Extraction
2.4. Qualitative Data Analysis
3. Results
3.1. Participants
3.2. Category System
3.3. Participant 1 (P1)
Qualitative Analysis in the Case of P1
E: “I will ask you a few more questions. You may answer yes or no. When answering, think about the picture you have just seen and answer the questions in the same way as the situation is depicted. Do you have a headache?”P1: “Yes… perfectly. Yes”(Telediagnostics at P1: 175–176)
E: “For example, you could make a gesture (…)”P1: “Yes?”E: “Stop Stop!” (raises arm as well as right hand, extends palm towards the screen.)P1: (looks towards the hand) “Five. Yes, exactly”(Telediagnostics at P1: 45–48)
E: “Hm. Ok. I’ll ask another question. Are you looking for a [hεmt] (shirt)?”P1: “A [hʊnt] (dog)?”(F2F at P1: 69–70)
(Dimly draws people with oversized jumpers, similarity to item template clearly recognisable)(F2F at P1: 76–76)
(E. puts the sheet in front of A6)P1: “Do-o-o-o!” (draws, sighs) “I don’t know.”(F2F at P1, pos. 164)
P1: “And do, today?” (unintelligible)P1′s wife: “That’s all right, darling. Just leave it and listen to what Mrs Gauch tells you. Don’t do anything about it. Don’t pretend anything. Okay? Good.”P1: (unintelligible, smiles, leans forward towards the screen, wife disappears from view).(Telediagnostics at P1, pos. 20–22)
3.4. Participant 2 (P2)
Qualitative Analysis in the Case of P2
P2: “Um, yes, tell me: Doesn’t the certificate [actually: prescription] say that I want something liquid? Not necessarily for intoxication, but to get over the cough better.”(Telediagnostics at P2: 58)
P2: “Yes, I don’t know, did we also order the Lus soup? We actually just wanted to eat (laughs) Schni-Schnitzel. But it doesn’t matter. The cutlery isn’t perfect at all, so maybe you can go back again. And then bring us here? (brings hands together gesticulating at chest level, forms a rhombus of fingers, then lowers hands again) Well, I’m not actually and probably (points to the right) you’ve now hired me as a revolutionary and an [other]. I’m actually always polite, as long as no one gives me any guff (gestures unspecifically) (drops his hands) so I’ve still managed to keep that. Then you can also manage it with just a few words. That’s my opinion (points to himself). You certainly don’t see it differently.”(F2F with P2: 182)
E: “Would you make that clear in another way?”P2: “Yes…” (stands up in front of the PC) “I would stand up.” (extends right arm) “Give the hand” (shakes right hand and raises left arm so that hand is at shoulder level) “put the arm on the shoulder and say: And next time you come to me.”(Telediagnostics at P2, pos. 81–82)
E: (…) “You have been coughing (makes gesture and sound to “cough”) for weeks. You (points with the cursor to the person in the scenario) go to the doctor. What’s wrong?, he asks.”P2: “What, what, what does he ask? Sorry. I didn’t understand them. [Double lot?]”(Telediagnostics at P2, pos. 31–32)
3.5. Participant 3 (P3)
Qualitative Analysis in the Case of P3
E: (…, turns to item 1a) “You may look at the picture first (short pause, points to person in item 1a) This is you again. You are in a clothes shop. You want to buy a new jumper. The shop assistant approaches you and asks: How can I help you?”(turns to white intermediate page)P3: “How can I help you? What colour should the jumper be and what thickness, so that it is nice and warm”.(F2F at P3, items 25–27)
P3: “I’m a bit too nervous for the whole story now”.(F2F at P3: 198–198)
P3: (quietly) “I can’t concentrate (raises left hand to forehead, adjusts glasses, looks at test folder, sighs) no, I can’t cope… “I’m unable to think clearly” [had already had] like we tested over there.”(F2F at P3: 104)
P3: (has eyes on table in front of him, takes notes while the scenario is shown/creates memory aid).(Telediagnostics at P3: 54–54)
P3: “Mrs Müller, have you ever handled [actually: ironed] silk blouse clothing (unintelligible)? Can you do that? Then I would entrust them to you then.”(Telediagnostics at P3, item 110)
E: “Then you have found the right jumper. Now you would like to know how much the jumper costs (gesture for “money”).”
P3: “Ok. (nods his head, points the biros at the test pad).”
E: “But you can’t find the price tag. What do you do?” (turns to white intermediate page)
P3: (indistinct, reaching out towards the test folder)
E: “Yes. I’ll repeat it all over again. …”.(F2F at P3, items 79–83)
3.6. Comparison of the Qualitative Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- “Ei-einwandfrei. Von daher gesehen. Ja.” (F2F at P1: 314–314)
- Die was, die? (F2F at P1: 104–104)
- U: “Hm. Ok. Ich stell noch ne Frage. Suchen Sie ein Hemd?”; P1: “N‘ Hund?” (F2F at P1: 69–70)
- (zeichnet schemenhaft Menschen mit übergroßem Pullover, Ähnlichkeit zu Itemvorlage deutlich erkennbar) (F2F at P1: 76–76)
- (U. legt das Blatt vor P1) “Do-o-o-o!” (P1 zeichnet, seufzt) “Ich weiß es nit.” (F2F at P1: 164)
- P1: “Und do, heute? (unverständlich)”; Ehefrau von A6: “Das ist ok so, Schatz. Einfach lassen und hören, was die Frau Gauch dir sagt. Nichts machen dran. Nichts verstellen. Ok? Gut.”; P1: (unverständlich, lächelt, lehnt sich nach vorne in Richtung Bildschirm, Ehefrau verschwindet aus Sichtfeld). (Telediagnostics at P1: 20–22)
- seufzt, lacht (Telediagnostics at P1: 60–60)
- “Das ist ok so, Schatz. Einfach lassen und hören, was die Frau Gauch dir sagt. Nichts machen dran. Nichts verstellen. Ok? Gut.” (Telediagnostics at P1: 21–21)
- U: “Ich stelle Ihnen noch einige Fragen. Sie dürfen mit Ja oder Nein antworten. Denken sie bei den Antworten an das Bild was sie gerade gesehen haben und beantworten sie die Fragen geauso, wie es zu der dargestellten Situation passt. Haben sie Kopfschmerzen?”; P1: “Ja… einwandfrei. Ja.” (Telediagnostics at P1: 175–176)
- U: “Sie könnten zum Beispiel eine Geste machen (…)”; P1: “Ja?”; U: „Halt Stop!“ (hebt den Arm sowie die rechte Hand, streckt Handfläche in Richtung des Bildschirms.; A6: (guckt in Richtung der Hand) “Fünf. Ja genau.” (Telediagnostics at P1: 45–48)
- “bäh” (schüttelt Hand beim Wort „bäh“, wackelt mit den Händen in der Luft, führt diese dann zusammen und faltet sie vor der Brust) “staubig sieht der aus.” (F2F at P2: 152–152)
- P2: “Ja ich weiß gar nicht haben wir die Lus-Suppe mitbestellt? Wir wollten doch eigentlich nur (lacht) Schni-Schnitzel essen. Aber, es ist ja egal. Das die das Besteck ist doch überhaupt nicht vollkommen können sie da gerade vielleicht nochmal zurückgehen. Und uns dann noch hierher bringen? (führt Hände gestikulierend auf Brusthöhe zusammen, bildet eine Raute aus Fingern, lässt Hände anschließend wieder sinken) Also ich bin eigentlich nicht und wahrscheinlich (deutet nach rechts zur Seite) haben Sie mich jetzt als ein Revoluzzer und ein [Anderer] eingestellt. Ich bin eigentlich immer, solange mir keiner doof kommt (gestikuliert unspezifisch) höflich (lässt Hände sinken) also das hab ich mir doch noch erhalten können. Dann kann man auch mit wenigen Worten kann man das scha-schaffen. Das ist meine Meinung (deutet auf sich). Sie sehen das sicherlich nicht anders.” (F2F at P2: 182)
- U: “Würden Sie das noch anders deutlich machen?”; P2: “Ja… (steht vor dem PC auf) Ich würde aufstehen. (Streckt rechten Arm aus) Die Hand geben (schüttelt rechte Hand und hebt den linken Arm, sodass Hand auf Schulterhöhe) den Arm auf die Schulter legen und sagen: Und das nächste Mal kommst Du zu mir. (Telediagnostics at P2: 81–82)
- U: “Sie husten (macht Geste und Geräusch zu „husten“) schon wochenlang. Sie (deutet mit dem Cursor auf den Menschen im Szenario) gehen zum Arzt. Was ist los?, fragt der.”; P1: “Was, was, was fragt der? Entschuldigung. Ich habe sie nicht verstanden. [Doppellos?]” (Telediagnostics at P2: 31–32)
- P2: “Ähm ja sagen Sie mal: Steht auf dem Attest denn nicht, dass ich etwas Flüssiges haben möchte? Nicht unbedingt zum Berauschen, sondern um den Husten besser zu überstehen.” (Telediagnostics at P2: 58)
- P3: “Ich hab alles vor Augen und dann krieg ich’s nicht ausgedrückt.” (F2F at P3: 190–190)
- U: (blättert um zu Item 1a) “Sie dürfen sich das Bild erstmal anschauen” (kurze Pause, deutet auf Mensch in Item 1a) “Dies sind Sie wieder. Sie sind in einem Bekleidungsgeschäft. Sie möchten einen neuen Pullover kaufen. Die Verkäuferin kommt auf Sie zu und fragt: Wie kann ich Ihnen helfen?” (U. blättert um auf weiße Zwischenseite); P3: “Wie kann ich Ihnen helfen? Welche Farbe soll der Pullover haben und welche Stärke, damit er schön wärmt.” (F2F at P3: 25–27)
- P3: “Ich bin für die ganze Geschichte ein bisschen zu nervös jetzt.” (F2F at P3: 198–198)
- P3: (leise) “Ich kann mich nicht konzentrieren (hebt linke Hand an die Stirn, rückt Brille zurecht, Blick auf Testmappe gerichtet, seufzt) “ne, komm ich nicht klar… ich bin wie vernagelt [hatte ich] wie wir da drüben getestet haben schon mal gehabt.” (F2F at P3: 104)
- U: “Dann haben Sie den richtigen Pullover gefunden. Sie möchten nun noch wissen wie viel der Pullover kostet” (Geste für “Geld”); P3: “Ok.” (nickt mit dem Kopf, richtet den Kugelschreiber auf die Testunterlage); U: Aber sie können das Preisschild nicht finden. Was tun Sie? (blättert um auf weiße Zwischenseite); P3: (undeutlich, ausstreckende Bewegung in Richtung Testmappe); U: Ja. Ich wiederhole es nochmal ganz. (…)” (F2F at P3: 79–83)
- P3: (macht sich Notizen) “Ich frage den Taxifahrer höflich: Wenn Sie mir einen Gefallen tun wollen–weil mir wird immer schlecht beim Autofahren—dass ich jetzt vorne sitzen darf. [Und nicht hinten]” (Telediagnostics at P3: 38–38)
- P3: “Dann darf ich Ihnen nochmal die-die Passage wo sie im-im Meer waren bei den schönen Temperaturen in Barcelona dass Sie die Passage nochmal wiederholen. Ich würde das ganz gerne einfädeln. Dass ich auch [eine] Tour machen kann. (…)” (Telediagnostics at P3: 104–104)
- P3: (hat Blick auf Tisch vor sich gerichtet, macht sich während das Szenario gezeigt wird Notizen/schafft Erinnerungshilfe) (Telediagnostics at P3: 54–54)
- P3: “Frau Müller haben Sie schonmal [Seiden-]blusen Kleidung (unverständlich) behandelt? Können Sie das? Dann würde ich [sie ihnen dann mal] anvertrauen.” (Telediagnostics at P3: 110)
References
- Heidler, M.-D. Einteilung, Diagnostik und Therapie von Demenzen und demenziell bedingten Sprachstörungen. Sprache Stimme Gehör 2011, 35, 111–119. [Google Scholar] [CrossRef]
- Magnin, E.; Démonet, J.-F.; Wallon, D.; Dumurgier, J.; Troussière, A.-C.; Jager, A.; Duron, E.; Gabelle, A.; de La Sayette, V.; Volpe-Gillot, L.; et al. Primary Progressive Aphasia in the Network of French Alzheimer Plan Memory Centers. J. Alzheimer’s Dis. JAD 2016, 54, 1459–1471. [Google Scholar] [CrossRef]
- Coyle-Gilchrist, I.T.S.; Dick, K.M.; Patterson, K.; Vázquez Rodríquez, P.; Wehmann, E.; Wilcox, A.; Lansdall, C.J.; Dawson, K.E.; Wiggins, J.; Mead, S.; et al. Prevalence, characteristics, and survival of frontotemporal lobar degeneration syndromes. Neurology 2016, 86, 1736–1743. [Google Scholar] [CrossRef] [Green Version]
- Hameister, I.; Nickels, L.; Abel, S.; Croot, K. “Do you have mowing the lawn ?”—Improvements in word retrieval and grammar following constraint-induced language therapy in primary progressive aphasia. Aphasiology 2017, 31, 308–331. [Google Scholar] [CrossRef] [Green Version]
- Tippett, D.C. Classification of primary progressive aphasia: Challenges and complexities. F1000Research 2020, 9, 64. [Google Scholar] [CrossRef] [Green Version]
- Gorno-Tempini, M.L.; Hillis, A.E.; Weintraub, S.; Kertesz, A.; Mendez, M.; Cappa, S.F.; Ogar, J.M.; Rohrer, J.D.; Black, S.; Boeve, B.F.; et al. Classification of primary progressive aphasia and its variants. Neurology 2011, 76, 1006–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teichmann, M.; Migliaccio, R.; Kas, A.; Dubois, B. Logopenic progressive aphasia beyond Alzheimer’s—An evolution towards dementia with Lewy bodies: Table 1. J. Neurol. Neurosurg. Psychiatry 2013, 84, 113–114. [Google Scholar] [CrossRef] [PubMed]
- Deuschl, G.; Maier, W. Demenzen: Leitlinien für Diagnostik und Therapie in der Neurologie 2016. Available online: https://dgn.org/leitlinien/leitlinie-diagnose-und-therapie-von-demenzen-2016/ (accessed on 22 October 2022).
- Dressel, K.; Lange, I. Klassifikation und Therapie der primär progressiven Aphasie. In Daseinsvorsorge, Wettbewerb und Kommunale Selbstverwaltung im Bereich der Liberalisierten Energiewirtschaft; Universitätsverlag Potsdam: Potsdam, Germany, 2015. [Google Scholar]
- Beukelman, D.R.; Fager, S.; Ball, L.; Dietz, A. AAC for adults with acquired neurological conditions: A review. Augment. Altern. Commun. 2007, 23, 230–242. [Google Scholar] [CrossRef]
- Fried-Oken, M.; Beukelman, D.R.; Hux, K. Current and future AAC research considerations for adults with acquired cognitive and communication impairments. Assist. Technol. Off. J. RESNA 2011, 24, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Utianski, R.L. (Ed.) Primary Progressive Aphasia and Other Frontotemporal Dementias: Diagnosis and Treatment of Associated Communication Disorders; Plural Publishing, Inc.: San Diego, CA, USA, 2020. [Google Scholar]
- Hillis, A.E.; Tuffiash, E.; Caramazza, A. Modality-specific deterioration in naming verbs in nonfluent primary progressive aphasia. J. Cogn. Neurosci. 2002, 14, 1099–1108. [Google Scholar] [CrossRef]
- Murray, L.L. Longitudinal treatment of primary progressive aphasia: A case study. Aphasiology 1998, 12, 651–672. [Google Scholar] [CrossRef] [Green Version]
- Parakh, R.; Roy, E.; Koo, E.; Black, S. Pantomime and imitation of limb gestures in relation to the severity of Alzheimer’s disease. Brain Cogn. 2004, 55, 272–274. [Google Scholar] [CrossRef] [PubMed]
- Nelissen, N.; Pazzaglia, M.; Vandenbulcke, M.; Sunaert, S.; Fannes, K.; Dupont, P.; Aglioti, S.M.; Vandenberghe, R. Gesture Discrimination in Primary Progressive Aphasia: The Intersection between Gesture and Language Processing Pathways. J. Neurosci. 2010, 30, 6334–6341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knels, C. Sprache und Ernährung bei Demenz: Klinik, Diagnostik und Therapie; Georg Thieme Verlag: Stuttgart, Germany, 2018. [Google Scholar]
- Powell, J. Hilfen zur Kommunikation bei Demenz; unveränderte auflage; Kuratorium Deutsche Altershilfe: Köln, Germany, 2011; Volume 7. [Google Scholar]
- Bier, N.; Brambati, S.; Macoir, J.; Paquette, G.; Schmitz, X.; Belleville, S.; Faucher, C.; Joubert, S. Relying on procedural memory to enhance independence in daily living activities: Smartphone use in a case of semantic dementia. Neuropsychol. Rehabil. 2015, 25, 913–935. [Google Scholar] [CrossRef]
- Khayum, B.; Wieneke, C.; Rogalski, E.; Robinson, J.; O’Hara, M. Thinking Outside the Stroke: Treating Primary Progressive Aphasia (PPA). Perspect. Gerontol. 2012, 17, 37–49. [Google Scholar] [CrossRef]
- Gallée, J.; Volkmer, A. A Window Into Functional Communication: Leveraging Naturalistic Speech Samples in Primary Progressive Aphasia. Perspect ASHA SIGs 2021, 6, 704–713. [Google Scholar] [CrossRef]
- Doedens, W.J.; Meteyard, L. Measures of functional, real-world communication for aphasia: A critical review. Aphasiology 2020, 34, 492–514. [Google Scholar] [CrossRef] [Green Version]
- Wallace, S.J.; Worrall, L.; Rose, T.; Le Dorze, G.; Breitenstein, C.; Hilari, K.; Babbitt, E.; Bose, A.; Brady, M.; Cherney, L.R.; et al. A core outcome set for aphasia treatment research: The ROMA consensus statement. Int. J. Stroke Off. J. Int. Stroke Soc. 2019, 14, 180–185. [Google Scholar] [CrossRef]
- Schütz, S. Kommunikationsorientierte Therapie bei Aphasie: Mit 24 Tabellen; MIT Online-Kopiervorlagen; E. Reinhardt: München, Germany, 2013. [Google Scholar]
- Nobis-Bosch, R.; Bruehl, S.; Krzok, F.; Jakob, H. Szenario-Test: Testung Verbaler und Non-Verbaler Aspekte Aphasischer Kommunikation; Prolog: Köln, Germany, 2020. [Google Scholar]
- Taylor-Rubin, C.; Croot, K.; Power, E.; Savage, S.A.; Hodges, J.R.; Togher, L. Communication behaviors associated with successful conversation in semantic variant primary progressive aphasia. Int. Psychogeriatr. 2017, 29, 1619–1632. [Google Scholar] [CrossRef]
- Morin, A.; Pressat-Laffouilhere, T.; Sarazin, M.; Lagarde, J.; Roue-Jagot, C.; Olivieri, P.; Paquet, C.; Cognat, E.; Dumurgier, J.; Pasquier, F.; et al. Telemedicine in French Memory Clinics During the COVID-19 Pandemic. J. Alzheimer’s Dis. JAD 2022, 86, 525–530. [Google Scholar] [CrossRef]
- Capra, R.; Mattioli, F. Tele-health in neurology: An indispensable tool in the management of the SARS-CoV-2 epidemic. J. Neurol. 2020, 267, 1885–1886. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Implementing Telemedicine Services during COVID-19: Guiding Principles and Considerations for a Stepwise Approach. Available online: https://iris.wpro.who.int/bitstream/handle/10665.1/14651/WPR-DSE-2020-032-eng.pdf?sequence=4 (accessed on 3 June 2021).
- Dial, H.R.; Hinshelwood, H.A.; Grasso, S.M.; Hubbard, H.I.; Gorno-Tempini, M.-L.; Henry, M.L. Investigating the utility of teletherapy in individuals with primary progressive aphasia. Clin. Interv. Aging 2019, 14, 453–471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raiser, T.; Croot, K.; Nickels, L.; Taylor, C.; Danek, A. Telemedicine in Primary Progressive Aphasia. Aphasie Verwandte Geb. Aphasie Domaines Assoc. 2014, 3, 37–40. [Google Scholar]
- Rogalski, E.J.; Saxon, M.; McKenna, H.; Wieneke, C.; Rademaker, A.; Corden, M.E.; Borio, K.; Mesulam, M.-M.; Khayum, B. Communication Bridge: A pilot feasibility study of Internet-based speech-language therapy for individuals with progressive aphasia. Alzheimer’s Dement. 2016, 2, 213–221. [Google Scholar] [CrossRef] [Green Version]
- Agha, Z.; Roter, D.L.; Schapira, R.M. An evaluation of patient-physician communication style during telemedicine consultations. J. Med. Internet Res. 2009, 11, e36. [Google Scholar] [CrossRef]
- O’Connell, M.E.; Crossley, M.; Cammer, A.; Morgan, D.; Allingham, W.; Cheavins, B.; Dalziel, D.; Lemire, M.; Mitchell, S.; Morgan, E. Development and evaluation of a telehealth videoconferenced support group for rural spouses of individuals diagnosed with atypical early-onset dementias. Dementia 2014, 13, 382–395. [Google Scholar] [CrossRef]
- Nagel, T.; Yellowlees, P. Telemedicine in the Top End. Australas Psychiatry 1995, 3, 317–319. [Google Scholar] [CrossRef]
- Dekhtyar, M.; Braun, E.J.; Billot, A.; Foo, L.; Kiran, S. Videoconference Administration of the Western Aphasia Battery-Revised: Feasibility and Validity. Am. J. Speech-Lang. Pathol. 2020, 29, 673–687. [Google Scholar] [CrossRef] [Green Version]
- Guo, Y.E.; Togher, L.; Power, E.; Hutomo, E.; Yang, Y.-F.; Tay, A.; Yen, S.-C.; Koh, G.C.-H. Assessment of Aphasia Across the International Classification of Functioning, Disability and Health Using an iPad-Based Application. Telemed. J. E-Health Off. J. Am. Telemed. Assoc. 2017, 23, 313–326. [Google Scholar] [CrossRef]
- Hall, N.; Boisvert, M.; Steele, R. Telepractice in the assessment and treatment of individuals with aphasia: A systematic review. Int. J. Telerehabilitation 2013, 5, 27–38. [Google Scholar] [CrossRef] [Green Version]
- Heidler, M.-D. Kognitive Dysphasien: Differenzialdiagnostik Aphasischer und Nichtaphasischer Zentraler Sprachstörungen Sowie Therapeutische Konsequenzen; Lang: Frankfurt am Main, Germany, 2006. [Google Scholar]
- Armour, M.; Del Toro, C.M.; Kiran, S.; Raymer, A.M.; Wallace, S.E. Supportive Communication for Individuals with Aphasia. Arch. Phys. Med. Rehabil. 2021, 102, 1437–1439. [Google Scholar] [CrossRef]
- Purdy, M.; Koch, A. Prediction of strategy usage by adults with aphasia. Aphasiology 2006, 20, 337–348. [Google Scholar] [CrossRef] [Green Version]
- Sabodash, V.; Mendez, M.F.; Fong, S.; Hsiao, J.J. Suicidal behavior in dementia: A special risk in semantic dementia. Am. J. Alzheimer’s Dis. Other Dement. 2013, 28, 592–599. [Google Scholar] [CrossRef]
- Brandt, R.; Hanser, H. Kahlschlag im Gehirn. Gehirn Geist 2003, 3, 30–35. [Google Scholar]
- Davidson, B.; Worrall, L.; Hickson, L. Identifying the communication activities of older people with aphasia: Evidence from naturalistic observation. Aphasiology 2003, 17, 243–264. [Google Scholar] [CrossRef]
- Uekermann, J.; Thoma, P.; Daum, I. Proverb interpretation changes in aging. Brain Cogn. 2008, 67, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Champagne-Lavau, M.; Monetta, L.; Moreau, N. Impact of educational level on metaphor processing in older adults. Rev. Française Linguist. Appliquée 2012, XVII, 89–100. [Google Scholar] [CrossRef] [Green Version]
- Simmons-Mackie, N.; Kagan, A. Communication strategies used by ‘good’ versus ‘poor’ speaking partners of individuals with aphasia. Aphasiology 1999, 13, 807–820. [Google Scholar] [CrossRef]
- Kuckartz, U. Qualitative Inhaltsanalyse: Methoden, Praxis, Computerunterstützung; überarbeitete Auflage; Beltz Verlagsgruppe: Weinheim, Germany, 2018; Volume 4. [Google Scholar]
- van der Meulen, I.; van de Sandt-Koenderman, W.M.E.; Duivenvoorden, H.J.; Ribbers, G.M. Measuring verbal and non-verbal communication in aphasia: Reliability, validity, and sensitivity to change of the Scenario Test. Int. J. Lang. Commun. Disord. 2010, 45, 424–435. [Google Scholar] [CrossRef]
- Dresing, T.; Pehl, T. Praxisbuch Interview, Transkription & Analyse: Anleitungen und Regelsysteme für Qualitativ Forschende; Auflage; Eigenverlag: Marburg, Germany, 2018; Volume 8. [Google Scholar]
- MAXQDA, VERBI Software: Berlin, Germany, 1989–2021.
- Baddeley, A. Working Memory. Science 1992, 255, 556–559. [Google Scholar] [CrossRef]
- Kindell, J.; Sage, K.; Keady, J.; Wilkinson, R. Adapting to conversation with semantic dementia: Using enactment as a compensatory strategy in everyday social interaction. Int. J. Lang. Commun. Disord. 2013, 48, 497–507. [Google Scholar] [CrossRef]
- Simmons-mackie, N.N.; Damico, J.S. Reformulating the definition of compensatory strategies in aphasia. Aphasiology 1997, 11, 761–781. [Google Scholar] [CrossRef]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oksenberg, L.; Cannell, C.; Kalton, G. New Strategies for Pretesting Survey Questions. J. Off. Stat. 1991, 7, 349–365. [Google Scholar]
- Devane, N.; Behn, N.; Marshall, J.; Ramachandran, A.; Wilson, S.; Hilari, K. The use of virtual reality in the rehabilitation of aphasia: A systematic review. Disabil. Rehabil. 2022, 1–20. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant’s Code | P1 | P2 | P3 |
|---|---|---|---|
| Age at start of study | 66 | 79 | 68 |
| Age at symptom onset | 61 | 76 | 66 |
| Gender | male | male | male |
| Years of education | 13 | 11 | 14 |
| Diagnosis * | nfvPPA | AD | svPPA |
| Depression * | No | No | Yes |
| In speech therapy treatment | No | Yes | Yes |
| Code | Definitions | Examples from the Material |
|---|---|---|
| Verbal | Aphasic symptoms | “F-Flawless. Seen from that point of view. Yes.” (F2F at P1: 314–314) |
| Expression of excessive demand | Metalinguistic comments that address a heightened awareness of disturbance | “I have everything and then in front of my eyes and then I can’t express it.” (F2F at P3: 190–190) |
| Nonverbal | Use of writing/drawing/gesturing | wiggles hands in the air while exclaiming “eww” (F2F at P2: 152–152) |
| Perceptual | Due to poor sound/image quality; due to presbycusis or presbyopia | “The what, the?” (F2F at P1: 104–104) |
| Use of aids | Compensatory use of objects or media beyond nonverbal communication | makes notes to compensate for deficits in working memory (Telediagnostics at P3: 38–38) |
| Executive | Deficits in inhibition/thinking/planning; Deficits in cognitive flexibility and theory of mind | “Then I would like you to repeat the passage where you were in the sea in the beautiful temperatures in Barcelona. I would like to arrange that. That I can also do [a] tour. (…)” (Telediagnostics at P3: 104–104) |
| Affective | Expressing emotions via meta-linguistic comments/sighing | sighs, laughs (Telediagnostics at P1: 60–60) |
| Communication partner assistance | Indications of dependence/ Peculiarities of the communication partners | “That’s okay, honey. Just let it be and listen to what Mrs. Gauch tells you. Don’t do anything about it. Don’t pretend. Okay? Good.” (Telediagnostics at P1: 21–21) |
| Participants | P1 | P2 | P3 | |||
|---|---|---|---|---|---|---|
| Setting | F2F | Tele | F2F | Tele | F2F | Tele |
| Verbal | 92 | 97 | 65 | 52 | 23 | 33 |
| Expression of excessive demand | 6 | 4 | 0 | 0 | 13 | 1 |
| Nonverbal | 19 | 3 | 15 | 6 | 2 | 0 |
| Perceptual | 5 | 2 | 0 | 4 | 1 | 0 |
| Use of aids | 0 | 0 | 0 | 0 | 0 | 6 |
| Executive functions | 6 | 3 | 20 | 12 | 41 | 38 |
| Affective | 20 | 18 | 21 | 7 | 4 | 1 |
| Communication partner assistance | 0 | 12 | 0 | 0 | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gauch, M.; Corsten, S.; Geschke, K.; Heinrich, I.; Leinweber, J.; Spelter, B. Differences of Modality Use between Telepractice and Face-to-Face Administration of the Scenario-Test in Persons with Dementia-Related Speech Disorder. Brain Sci. 2023, 13, 204. https://doi.org/10.3390/brainsci13020204
Gauch M, Corsten S, Geschke K, Heinrich I, Leinweber J, Spelter B. Differences of Modality Use between Telepractice and Face-to-Face Administration of the Scenario-Test in Persons with Dementia-Related Speech Disorder. Brain Sciences. 2023; 13(2):204. https://doi.org/10.3390/brainsci13020204
Chicago/Turabian StyleGauch, Mirjam, Sabine Corsten, Katharina Geschke, Isabel Heinrich, Juliane Leinweber, and Bianca Spelter. 2023. "Differences of Modality Use between Telepractice and Face-to-Face Administration of the Scenario-Test in Persons with Dementia-Related Speech Disorder" Brain Sciences 13, no. 2: 204. https://doi.org/10.3390/brainsci13020204