
Targeting the Tumor Immune Microenvironment Could Become a Potential Therapeutic Modality for Aggressive Pituitary Adenoma
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Patients and Design
2.2. Immunohistochemistry
2.3. Statistical Analysis
3. Result
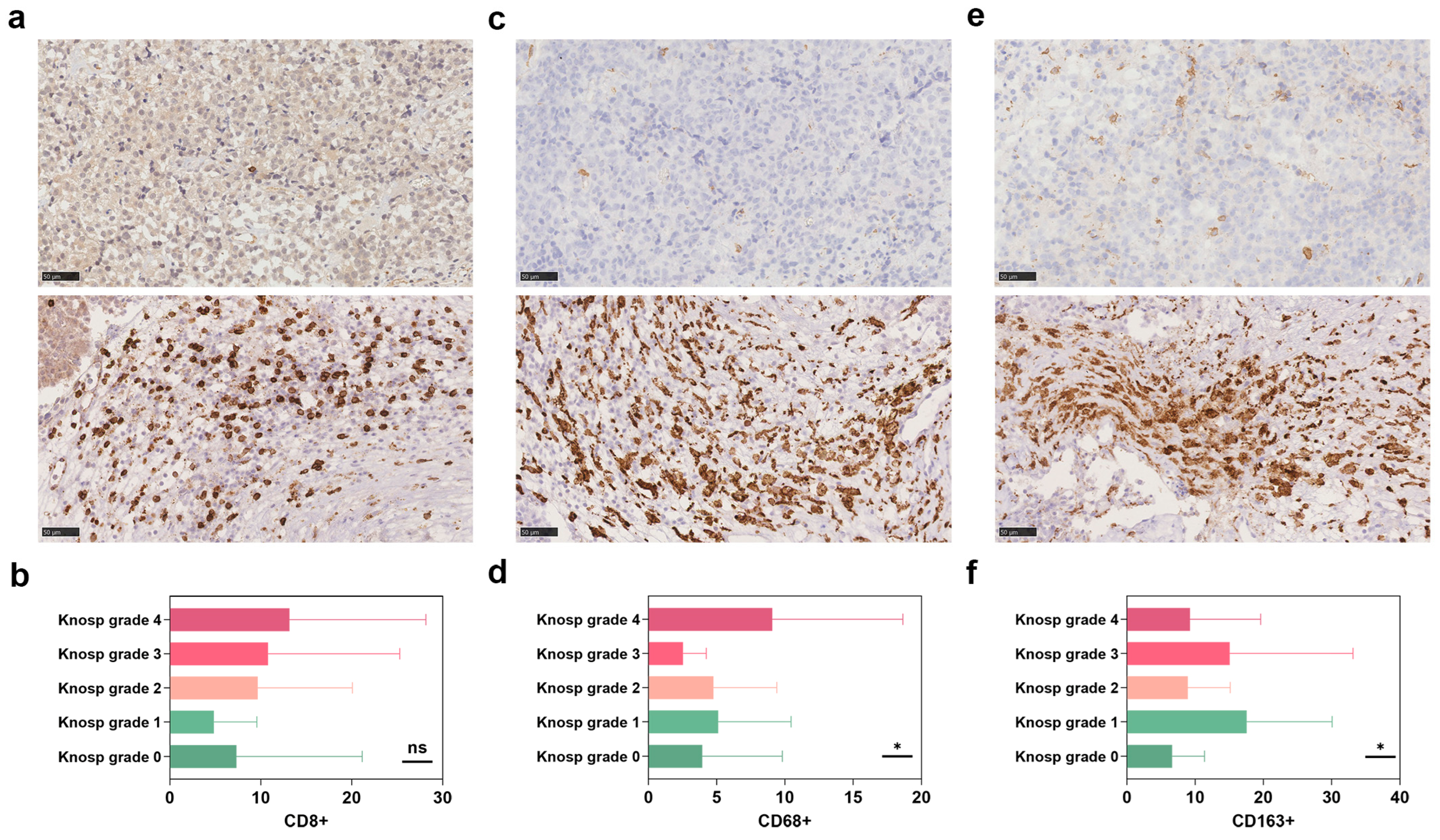
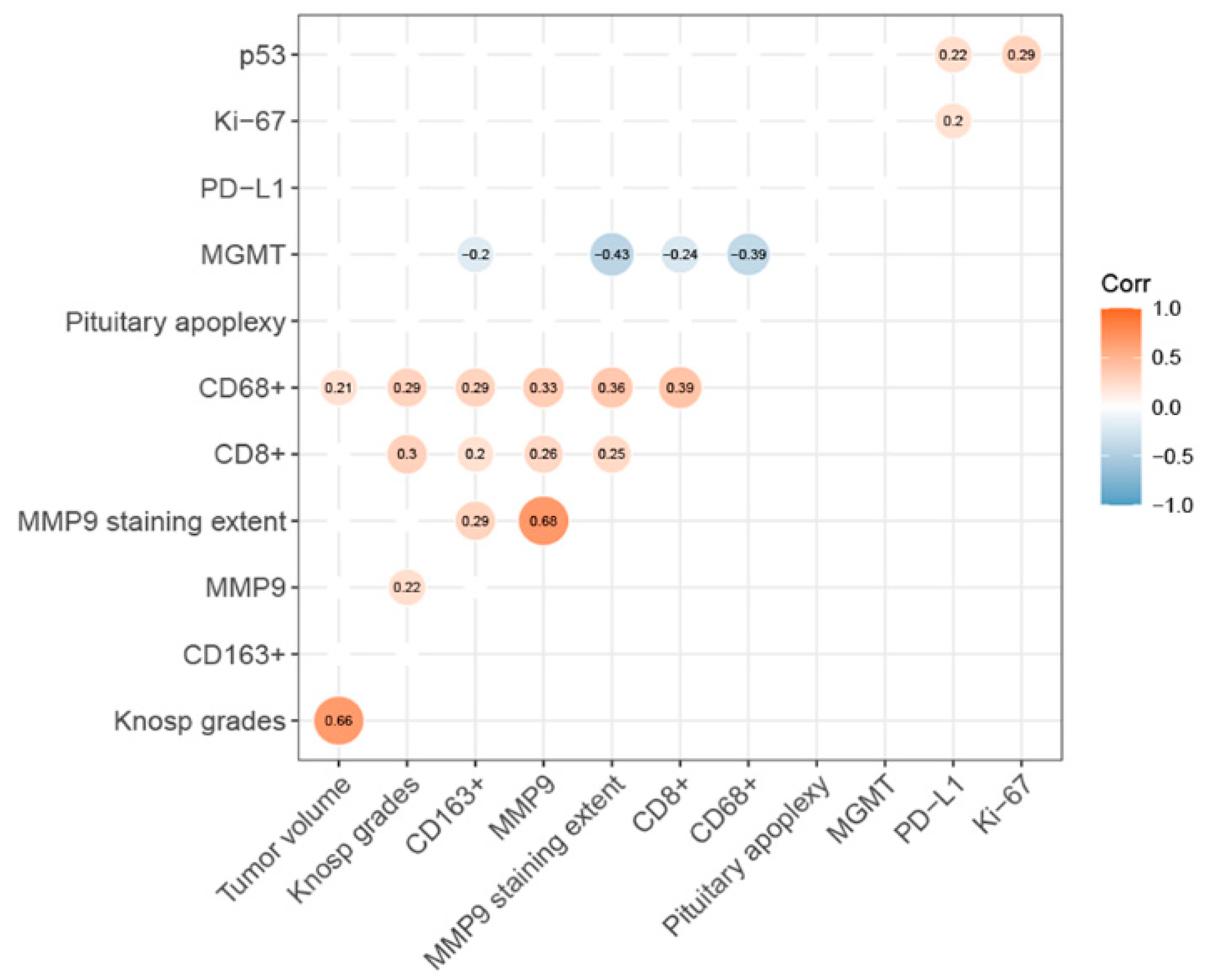
3.1. Markers of Invasiveness and Aggressive Infiltration
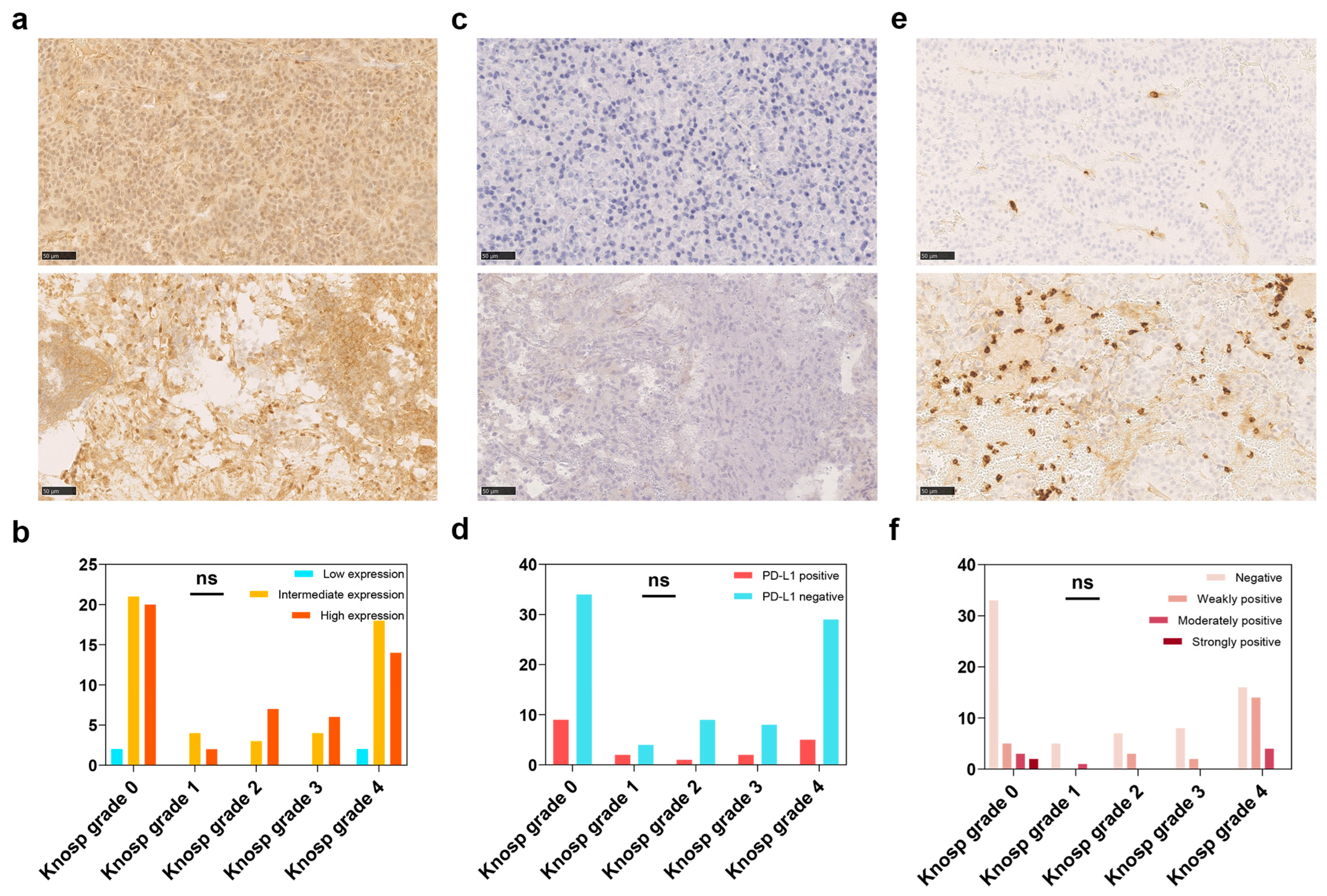
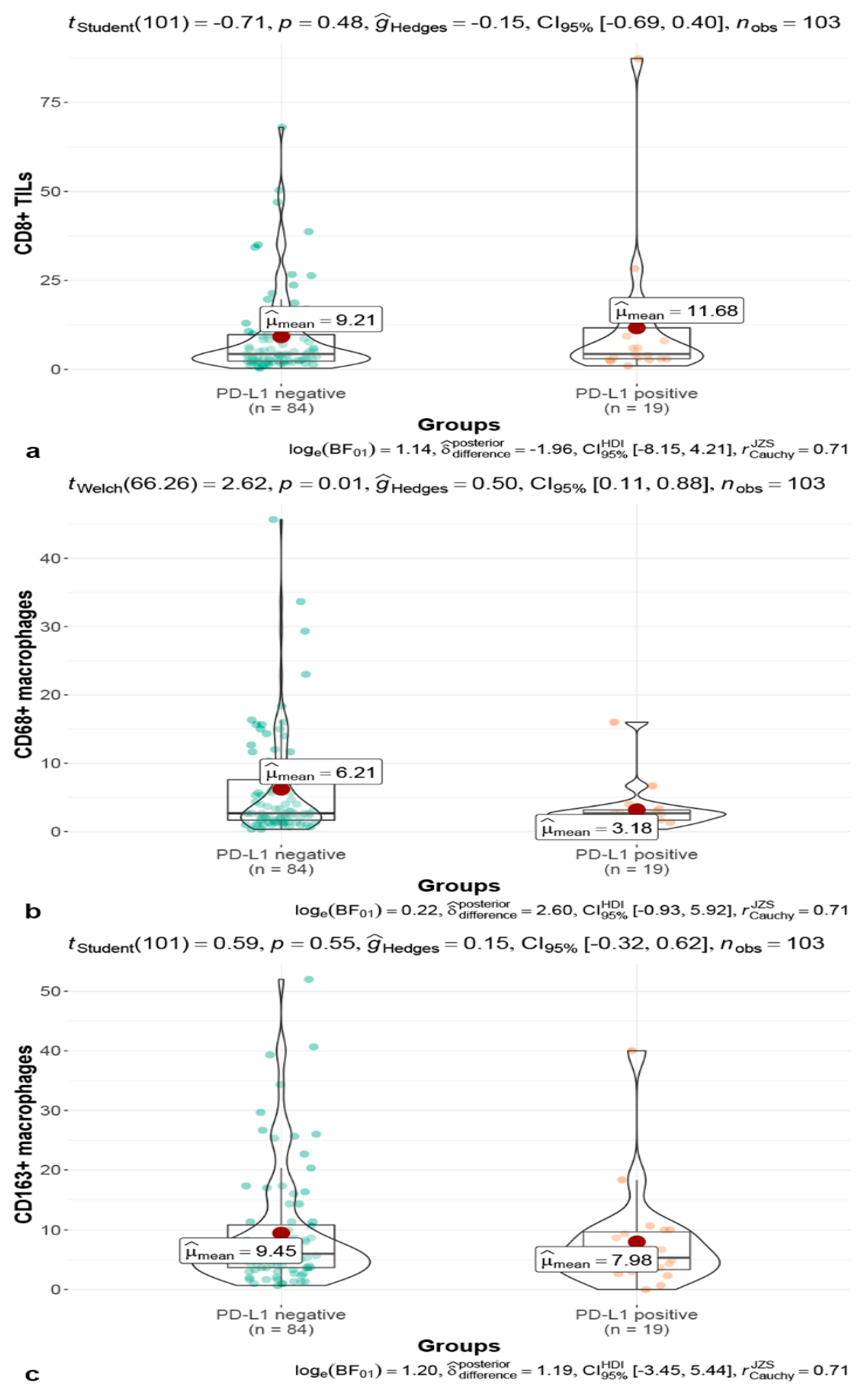
3.2. MGMT and Immune Checkpoint
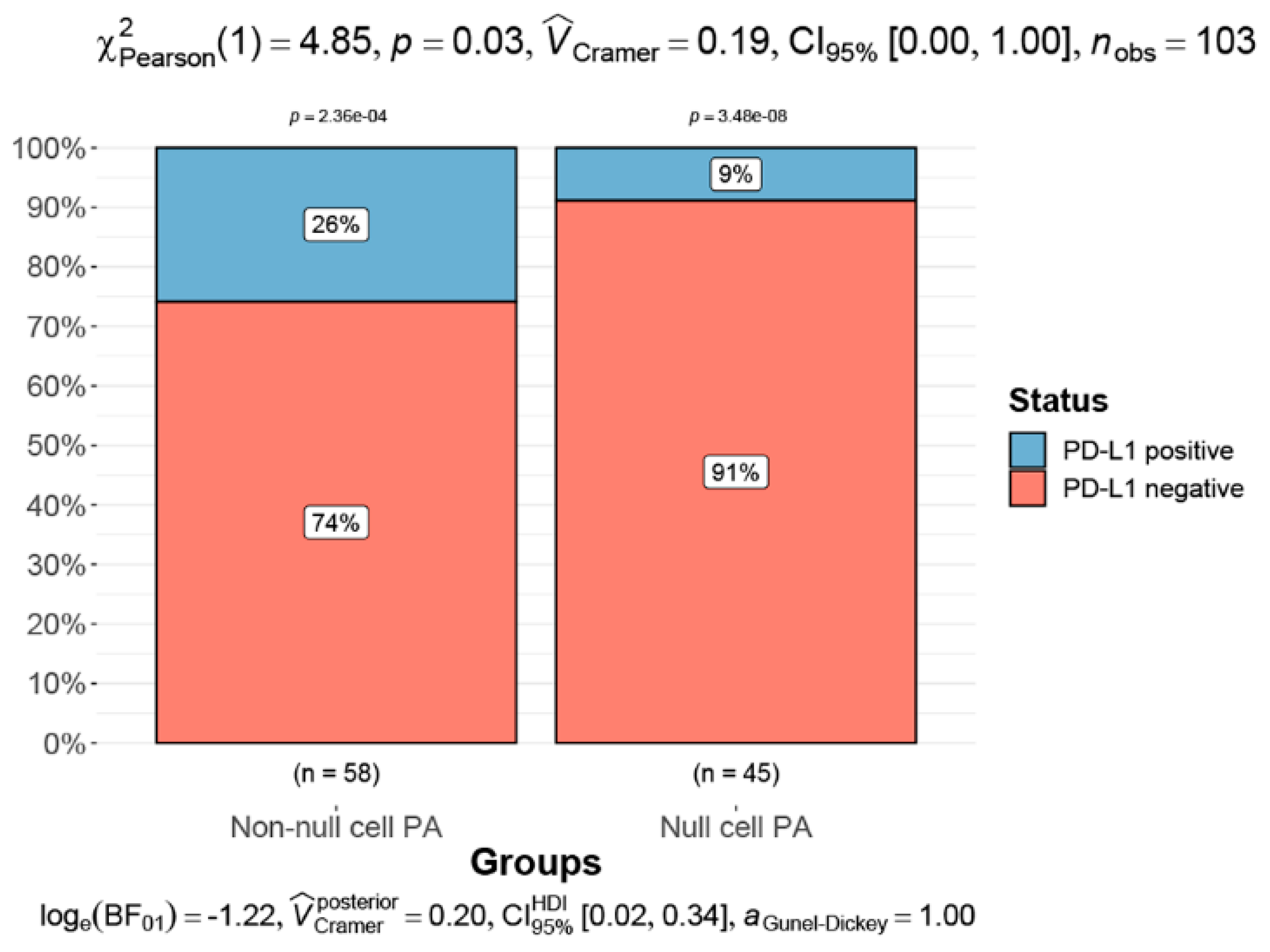
3.3. Classifications and Apoplexy of Pituitary Adenoma
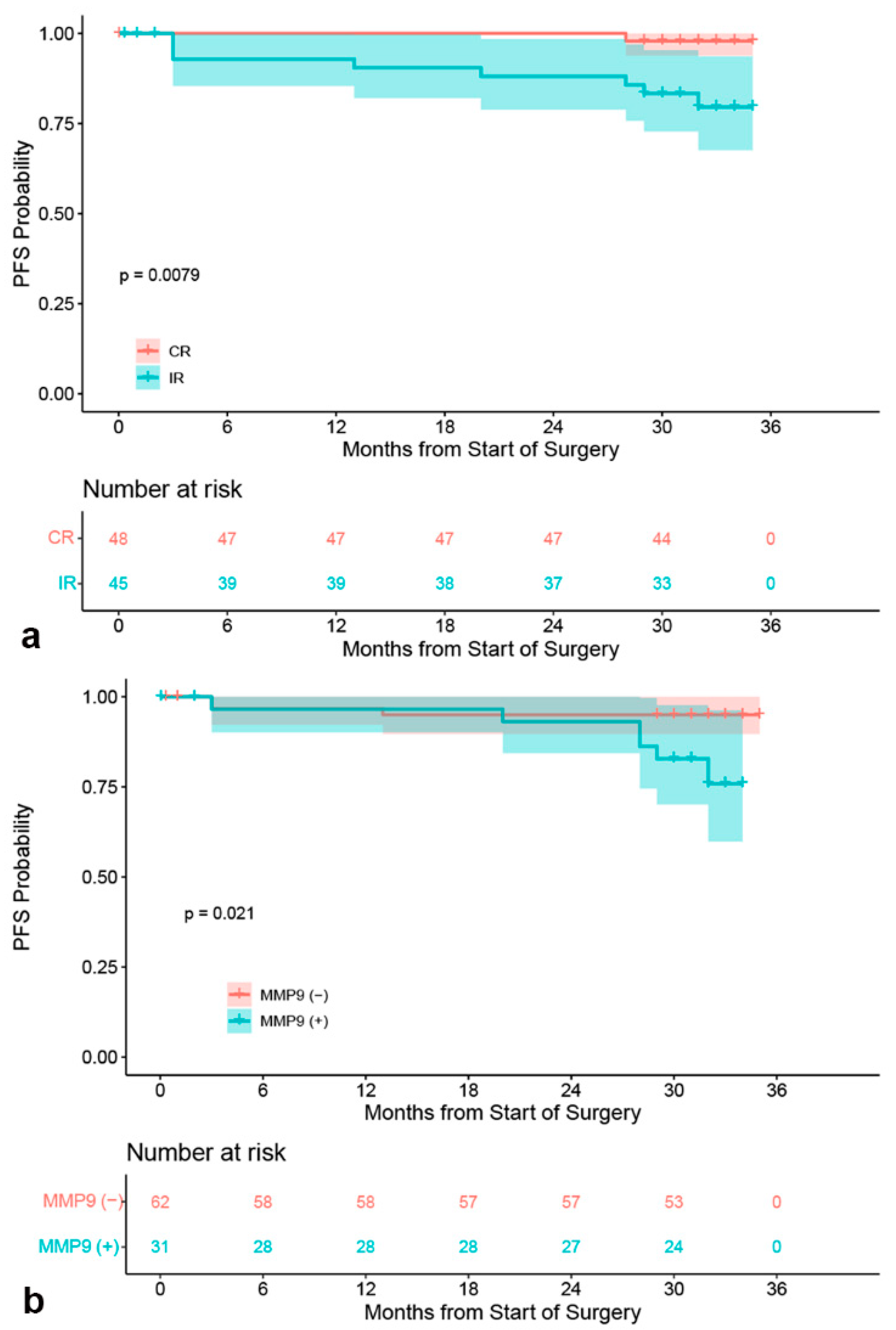
3.4. Survival Analysis
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Melmed, S. Pituitary-Tumor Endocrinopathies. N. Engl. J. Med. 2020, 382, 937–950. [Google Scholar] [CrossRef]
- Molitch, M.E. Diagnosis and Treatment of Pituitary Adenomas: A Review. JAMA 2017, 317, 516–524. [Google Scholar] [CrossRef] [PubMed]
- Heaney, A. Management of aggressive pituitary adenomas and pituitary carcinomas. J. Neurooncol. 2014, 117, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Nomikos, P.; Buchfelder, M.; Fahlbusch, R. The outcome of surgery in 668 patients with acromegaly using current criteria of biochemical ‘cure’. Eur. J. Endocrinol. 2005, 152, 379–387. [Google Scholar]
- Rhee, I. Diverse macrophages polarization in tumor microenvironment. Arch. Pharm. Res. 2016, 39, 1588–1596. [Google Scholar] [CrossRef]
- Komohara, Y.; Jinushi, M.; Takeya, M. Clinical significance of macrophage heterogeneity in human malignant tumors. Cancer Sci. 2014, 105, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Zhou, W.; Ke, S.Q.; Huang, Z.; Flavahan, W.; Fang, X.; Paul, J.; Wu, L.; Sloan, A.E.; McLendon, R.E.; Li, X.; et al. Periostin secreted by glioblastoma stem cells recruits M2 tumour-associated macrophages and promotes malignant growth. Nat. Cell Biol. 2015, 17, 170–182. [Google Scholar] [CrossRef] [Green Version]
- Maimela, N.R.; Liu, S.; Zhang, Y. Fates of CD8+ T cells in Tumor Microenvironment. Comput. Struct. Biotechnol. J. 2019, 17, 1–13. [Google Scholar] [CrossRef]
- Sato, M.; Tamura, R.; Tamura, H.; Mase, T.; Kosugi, K.; Morimoto, Y.; Yoshida, K.; Toda, M. Analysis of Tumor Angiogenesis and Immune Microenvironment in Non-Functional Pituitary Endocrine Tumors. J. Clin. Med. 2019, 8, 695. [Google Scholar] [CrossRef] [Green Version]
- Kemeny, H.R.; Elsamadicy, A.A.; Farber, S.H.; Champion, C.D.; Lorrey, S.J.; Chongsathidkiet, P.; Woroniecka, K.I.; Cui, X.; Shen, S.H.; Rhodin, K.E.; et al. Targeting PD-L1 Initiates Effective Antitumor Immunity in a Murine Model of Cushing Disease. Clin. Cancer Res. 2020, 26, 1141–1151. [Google Scholar] [CrossRef]
- Gong, J.; Zhao, Y.; Abdel-Fattah, R.; Amos, S.; Xiao, A.; Lopes, M.B.; Hussaini, I.M.; Laws, E.R. Matrix metalloproteinase-9, a potential biological marker in invasive pituitary adenomas. Pituitary 2008, 11, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Matsumoto, Y.; Okada, M.; Miyake, K.; Kunishio, K.; Kawai, N.; Tamiya, T.; Nagao, S. Matrix metalloproteinase 2 and 9 expression correlated with cavernous sinus invasion of pituitary adenomas. J. Med. Investig. 2005, 52, 151–158. [Google Scholar] [CrossRef] [Green Version]
- Mucha, S.A.; Meleń-Mucha, G.; Godlewski, A.; Stepień, H. Inhibition of estrogen-induced pituitary tumor growth and angiogenesis in Fischer 344 rats by the matrix metalloproteinase inhibitor batimastat. Virchows Arch. 2007, 450, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Fu, D.; Calvo, J.A.; Samson, L.D. Balancing repair and tolerance of DNA damage caused by alkylating agents. Nat. Rev. Cancer 2012, 12, 104–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, S.; Shahinian, H.; Maya, M.M.; Yong, W.; Heaney, A.P. Temozolomide: A novel treatment for pituitary carcinoma. Lancet Oncol. 2006, 7, 518–520. [Google Scholar] [CrossRef]
- Kovacs, K.; Scheithauer, B.W.; Lombardero, M.; McLendon, R.E.; Syro, L.V.; Uribe, H.; Ortiz, L.D.; Penagos, L.C. MGMT immunoexpression predicts responsiveness of pituitary tumors to temozolomide therapy. Acta Neuropathol. 2008, 115, 261–262. [Google Scholar] [CrossRef]
- Micko, A.; Wöhrer, A.; Höftberger, R.; Vila, G.; Marosi, C.; Knosp, E.; Wolfsberger, S. MGMT and MSH6 immunoexpression for functioning pituitary macroadenomas. Pituitary 2017, 20, 643–653. [Google Scholar] [CrossRef] [Green Version]
- Dai, C.; Sun, B.; Liu, X.; Bao, X.; Feng, M.; Yao, Y.; Wei, J.; Deng, K.; Yang, C.; Li, X.; et al. O-6-Methylguanine-DNA methyltransferase expression is associated with pituitary adenoma tumor recurrence: A systematic meta-analysis. Oncotarget 2017, 8, 19674–19683. [Google Scholar] [CrossRef] [Green Version]
- Han, S.; Yang, Z.; Yang, Y.; Qi, X.; Yan, C.; Yu, C. Individual Treatment Decisions for Central Neurocytoma. Front. Neurol. 2020, 11, 834. [Google Scholar] [CrossRef]
- Barkhoudarian, G.; Kelly, D.F. Pituitary Apoplexy. Neurosurg. Clin. N. Am. 2019, 30, 457–463. [Google Scholar] [CrossRef]
- Scheithauer, B.W.; Kovacs, K.T.; Laws, E.R., Jr.; Randall, R.V. Pathology of invasive pituitary tumors with special reference to functional classification. J. Neurosurg. 1986, 65, 733–744. [Google Scholar] [CrossRef] [PubMed]
- Lopes, M. The 2017 World Health Organization classification of tumors of the pituitary gland: A summary. Acta Neuropathol. 2017, 134, 521–535. [Google Scholar] [CrossRef]
- Raverot, G.; Dantony, E.; Beauvy, J.; Vasiljevic, A.; Mikolasek, S.; Borson-Chazot, F.; Jouanneau, E.; Roy, P.; Trouillas, J. Risk of Recurrence in Pituitary Neuroendocrine Tumors: A Prospective Study Using a Five-Tiered Classification. J. Clin. Endocrinol. Metab. 2017, 102, 3368–3374. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Adam, B.; Jack, A.S.; Lam, A.; Broad, R.W.; Chik, C.L. Immune Cell Infiltrates in Pituitary Adenomas: More Macrophages in Larger Adenomas and More T Cells in Growth Hormone Adenomas. Endocr. Pathol. 2015, 26, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Geng, X.; Li, Z.; Chen, Z.; Liu, Y.; Liu, P.; Wang, Q.; Li, C.; Ai, D.; Li, Z. The Relationship Between Phospho-p38, Matrix Metalloproteinase 9, and Major Histocompatibility Complex Class I Chain-Related Molecule A Expression in Pituitary Adenomas Demonstrates a New Mechanism of Pituitary Adenoma Immune Escape. World Neurosurg. 2019, 123, e116–e124. [Google Scholar] [CrossRef] [PubMed]
- Herbst, R.S.; Soria, J.C.; Kowanetz, M.; Fine, G.D.; Hamid, O.; Gordon, M.S.; Sosman, J.A.; McDermott, D.F.; Powderly, J.D.; Gettinger, S.N.; et al. Predictive correlates of response to the anti-PD-L1 antibody MPDL3280A in cancer patients. Nature 2014, 515, 563–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCormack, A.I.; McDonald, K.L.; Gill, A.J.; Clark, S.J.; Burt, M.G.; Campbell, K.A.; Braund, W.J.; Little, N.S.; Cook, R.J.; Grossman, A.B.; et al. Low O6-methylguanine-DNA methyltransferase (MGMT) expression and response to temozolomide in aggressive pituitary tumours. Clin. Endocrinol. 2009, 71, 226–233. [Google Scholar] [CrossRef]
- Qian, B.Z.; Pollard, J.W. Macrophage diversity enhances tumor progression and metastasis. Cell 2010, 141, 39–51. [Google Scholar] [CrossRef] [Green Version]
- Marques, P.; Barry, S.; Carlsen, E.; Collier, D.; Ronaldson, A.; Dorward, N.; Grieve, J.; Mendoza, N.; Nair, R.; Muquit, S.; et al. The role of the tumour microenvironment in the angiogenesis of pituitary tumours. Endocrine 2020, 70, 593–606. [Google Scholar] [CrossRef]
- Lewis, C.E.; Harney, A.S.; Pollard, J.W. The Multifaceted Role of Perivascular Macrophages in Tumors. Cancer Cell 2016, 30, 365. [Google Scholar] [CrossRef] [Green Version]
- Mondal, S.; Adhikari, N.; Banerjee, S.; Amin, S.A.; Jha, T. Matrix metalloproteinase-9 (MMP-9) and its inhibitors in cancer: A minireview. Eur. J. Med. Chem. 2020, 194, 112260. [Google Scholar] [CrossRef] [PubMed]
- Yamada, S.; Aiba, T.; Sano, T.; Kovacs, K.; Shishiba, Y.; Sawano, S.; Takada, K. Growth hormone-producing pituitary adenomas: Correlations between clinical characteristics and morphology. Neurosurgery 1993, 33, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Marques, P.; Barry, S.; Carlsen, E.; Collier, D.; Ronaldson, A.; Awad, S.; Dorward, N.; Grieve, J.; Mendoza, N.; Muquit, S.; et al. Chemokines modulate the tumour microenvironment in pituitary neuroendocrine tumours. Acta Neuropathol. Commun. 2019, 7, 172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, P.F.; Wang, T.J.; Yang, Y.K.; Yao, K.; Li, Z.; Li, Y.M.; Yan, C.X. The expression profile of PD-L1 and CD8(+) lymphocyte in pituitary adenomas indicating for immunotherapy. J. Neurooncol. 2018, 139, 89–95. [Google Scholar] [CrossRef]
- Corry, D.B.; Kiss, A.; Song, L.Z.; Song, L.; Xu, J.; Lee, S.; Werb, Z.; Kheradmand, F. Overlapping and independent contributions of MMP2 and MMP9 to lung allergic inflammatory cell egression through decreased CC chemokines. FASEB J. 2004, 18, 995–997. [Google Scholar] [CrossRef] [Green Version]
- Benson, H.L.; Mobashery, S.; Chang, M.; Kheradmand, F.; Hong, J.S.; Smith, G.N.; Shilling, R.A.; Wilkes, D.S. Endogenous matrix metalloproteinases 2 and 9 regulate activation of CD4+ and CD8+ T cells. Am. J. Respir. Cell Mol. Biol. 2011, 44, 700–708. [Google Scholar] [CrossRef] [Green Version]
- Röver, L.K.; Gevensleben, H.; Dietrich, J.; Bootz, F.; Landsberg, J.; Goltz, D.; Dietrich, D. PD-1 (PDCD1) Promoter Methylation Is a Prognostic Factor in Patients with Diffuse Lower-Grade Gliomas Harboring Isocitrate Dehydrogenase (IDH) Mutations. EBioMedicine 2018, 28, 97–104. [Google Scholar] [CrossRef] [Green Version]
- Hölzl, D.; Hutarew, G.; Zellinger, B.; Schlicker, H.U.; Schwartz, C.; Winkler, P.A.; Sotlar, K.; Kraus, T. Integrated analysis of programmed cell death ligand 1 expression reveals increased levels in high-grade glioma. J. Cancer Res. Clin. Oncol. 2021, 147, 2271–2280. [Google Scholar] [CrossRef]
- Gültekin, G.D.; Çabuk, B.; Vural, Ç.; Ceylan, S. Matrix metalloproteinase-9 and tissue inhibitor of matrix metalloproteinase-2: Prognostic biological markers in invasive prolactinomas. J. Clin. Neurosci. 2015, 22, 1282–1287. [Google Scholar] [CrossRef]
- Syro, L.V.; Rotondo, F.; Camargo, M.; Ortiz, L.D.; Serna, C.A.; Kovacs, K. Temozolomide and Pituitary Tumors: Current Understanding, Unresolved Issues, and Future Directions. Front. Endocrinol. 2018, 9, 318. [Google Scholar] [CrossRef] [Green Version]
- McCormack, A.; Kaplan, W.; Gill, A.J.; Little, N.; Cook, R.; Robinson, B.; Clifton-Bligh, R. MGMT expression and pituitary tumours: Relationship to tumour biology. Pituitary 2013, 16, 208–219. [Google Scholar] [CrossRef] [PubMed]
- Caccese, M.; Barbot, M.; Ceccato, F.; Padovan, M.; Gardiman, M.P.; Fassan, M.; Denaro, L.; Emanuelli, E.; D’Avella, D.; Scaroni, C.; et al. Lombardi, Rapid disease progression in patient with mismatch-repair deficiency pituitary ACTH-secreting adenoma treated with checkpoint inhibitor pembrolizumab. Anticancer. Drugs 2020, 31, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Maghrouni, A.; Givari, M.; Jalili-Nik, M.; Mollazadeh, H.; Bibak, B.; Sadeghi, M.M.; Afshari, A.R.; Johnston, T.P.; Sahebkar, A. Targeting the PD-1/PD-L1 pathway in glioblastoma multiforme: Preclinical evidence and clinical interventions. Int. Immunopharmacol. 2021, 93, 107403. [Google Scholar] [CrossRef]
- Halevy, C.; Whitelaw, B.C. How effective is temozolomide for treating pituitary tumours and when should it be used. Pituitary 2017, 20, 261–266. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | N (%) |
|---|---|
| Patients (n) | 103 |
| Age, mean years ± SD (range) | 45.02 ± 14.91 (15–79) |
| Average follow-up time (range) | 30.56 ± 6.53 (<1–35) months |
| Primary adenomas | 79 (76.70%) |
| Recurent adenomas | 24 (23.30%) |
| Gender | |
| Male | 54 (52.43%) |
| Female | 49 (47.57%) |
| Symptoms and signs | |
| Visual deficit | 48 (46.60%) |
| Headache | 45 (43.69%) |
| Menstrual disturbances | 13 (12.62%) |
| Sexual dysfunction | 6 (5.83%) |
| Polydipsia and polyuria | 3 (2.91%) |
| Incidental finding | 3 (2.91%) |
| Gross tumor volume median | 7.08 cm3 (0.28 to 245 cm3) |
| Pituitary apoplexy | 10 (9.71%) |
| Knosp classification grades | |
| Grade 0 | 43 (41.75%) |
| Grade 1 | 6 (5.83%) |
| Grades 2 | 10 (9.71%) |
| Grades 3 | 10 (9.71%) |
| Grades 4 | 34 (33.01%) |
| Pathological classifications | |
| Somatotroph adenomas | 8 (7.77%) |
| Lactotroph adenomas | 18 (17.48%) |
| Thyrotroph adenoma | 1 (0.97%) |
| Corticotroph adenomas | 5 (4.84%) |
| Gonadotroph adenoma | 22 (21.36%) |
| Null cell adenoma | 45 (43.69%) |
| Plurihormonal adenomas | 4 (3.88%) |
| Secretory pituitary adenomas | 54 (52.43%) |
| GH-secreting adenomas | 4 (3.88%) |
| Prolactinomas | 26 (25.24%) |
| ACTH-secreting adenomas | 8 (3.88%) |
| FSH-secreting adenomas | 2 (7.77%) |
| Plurihormonal-secreting adenomas | 14 (13.59%) |
| Non-functional adenomas | 49 (47.57%) |
| Immunohistochemical results | |
| Ki-67 median | 1.50% (0–25%) |
| P53 positive | 3 (2.91%) |
| MGMT expression | |
| <10% | 4 (3.88%) |
| 10–90% | 50 (48.54%) |
| ≥90% | 49 (47.57%) |
| PD-L1 positive | 19 (18.45%) |
| MMP-9 staining extent | |
| <5% | 89 (86.41%) |
| 5–25% | 5 (4.85%) |
| 26–50% | 1 (0.97%) |
| >50% | 8 (7.77%) |
| MMP-9 final scores | |
| negative | 69 (66.99%) |
| weakly positive | 24 (23.30%) |
| moderately positive | 8 (7.77%) |
| strongly positive | 2 (1.94%) |
| Surgical approach | |
| microscope transsphenoidal surgery | 55 (53.40%) |
| endoscopic transsphenoidal surgery | 27 (26.21%) |
| craniotomy | 21 (20.39%) |
| Resection extent | |
| CR (complete resection) | 55 (53.40%) |
| IR (incomplete resection) | 48 (46.60%) |
| Variables | Univariate Regression | Multivariate Regression | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | |
| Pituitary apoplexy | 1.291 × 10−8 | 0.00–Inf | 1.00 | 8.43 × 10−9 | 0.00–Inf | 1.00 |
| Knosp grades | 1.48 | 0.68–0.77 | 0.25 | 1.18 | 0.51–2.74 | 0.70 |
| Recurrent tumor | 3.64 | 0.51–25.82 | 0.20 | 2.14 | 0.26–17.20 | 0.47 |
| Extent of resection | 3.20 | 0.33–30.80 | 0.31 | 1.35 | 0.08–23.47 | 0.84 |
| MMP-9 expression | 4.22 | 0.44–40.61 | 0.21 | 4.80 | 0.38–60.65 | 0.23 |
| MGMT expression | 1.16 | 0.21–6.57 | 0.87 | 1.56 | 0.25–9.65 | 0.63 |
| PD-L1 expression | 2.91 × 10−9 | 0.00–Inf | 1.00 | 4.22 × 10−9 | 0.00–Inf | 1.00 |
| Histopathological classifications | 1.84 | 0.61–5.52 | 0.28 | 1.35 | 0.42–4.32 | 0.62 |
| Functional classifications | 0.94 | 0.58–1.52 | 0.80 | 0.82 | 0.49–1.39 | 0.46 |
| Variables | Univariate Regression | Multivariate Regression | ||||
|---|---|---|---|---|---|---|
| Exp(coef) | 95% CI | p | Exp(coef) | 95% CI | p | |
| Pituitary apoplexy | 1.27 × 10−8 | 0.00–Inf | 1.00 | 3.24 × 10−8 | 0.00–Inf | 1.00 |
| Knosp grades | 1.27 | 0.86–1.87 | 0.22 | 0.69 | 0.41–1.14 | 0.15 |
| Recurrent tumor | 5.21 | 1.40–19.41 | 0.01 | 5.13 | 1.07–24.61 | 0.04 |
| Extent of resection | 9.83 | 1.23–78.66 | 0.03 | 7.60 | 0.71–81.15 | 0.09 |
| MMP-9 positive | 4.18 | 1.11–17.88 | 0.04 | 4.40 | 0.91–21.21 | 0.06 |
| MGMT expression | 0.67 | 0.24–1.93 | 0.47 | 0.79 | 0.22–2.84 | 0.72 |
| PD-L1 expression | 0.57 | 0.12–2.73 | 0.48 | 1.10 | 0.13–9.33 | 0.93 |
| Histopathological classifications | 1.11 | 0.74–1.64 | 0.62 | 1.09 | 0.60–1.98 | 0.77 |
| Functional classifications | 0.98 | 0.70–1.36 | 0.89 | 0.94 | 0.61–1.44 | 0.76 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, Z.; Tian, X.; Yao, K.; Yang, Y.; Zhang, L.; Liu, N.; Yan, C.; Qi, X.; Han, S. Targeting the Tumor Immune Microenvironment Could Become a Potential Therapeutic Modality for Aggressive Pituitary Adenoma. Brain Sci. 2023, 13, 164. https://doi.org/10.3390/brainsci13020164
Yang Z, Tian X, Yao K, Yang Y, Zhang L, Liu N, Yan C, Qi X, Han S. Targeting the Tumor Immune Microenvironment Could Become a Potential Therapeutic Modality for Aggressive Pituitary Adenoma. Brain Sciences. 2023; 13(2):164. https://doi.org/10.3390/brainsci13020164
Chicago/Turabian StyleYang, Zuocheng, Xuemei Tian, Kun Yao, Yakun Yang, Linpeng Zhang, Ning Liu, Changxiang Yan, Xueling Qi, and Song Han. 2023. "Targeting the Tumor Immune Microenvironment Could Become a Potential Therapeutic Modality for Aggressive Pituitary Adenoma" Brain Sciences 13, no. 2: 164. https://doi.org/10.3390/brainsci13020164