
Does Impaired Plantar Cutaneous Vibration Perception Contribute to Axial Motor Symptoms in Parkinson’s Disease? Effects of Medication and Subthalamic Nucleus Deep Brain Stimulation

Abstract
:1. Introduction
2. Methods
2.1. Subjects
2.2. Equipment and Testing Procedures
2.2.1. Motor Performance
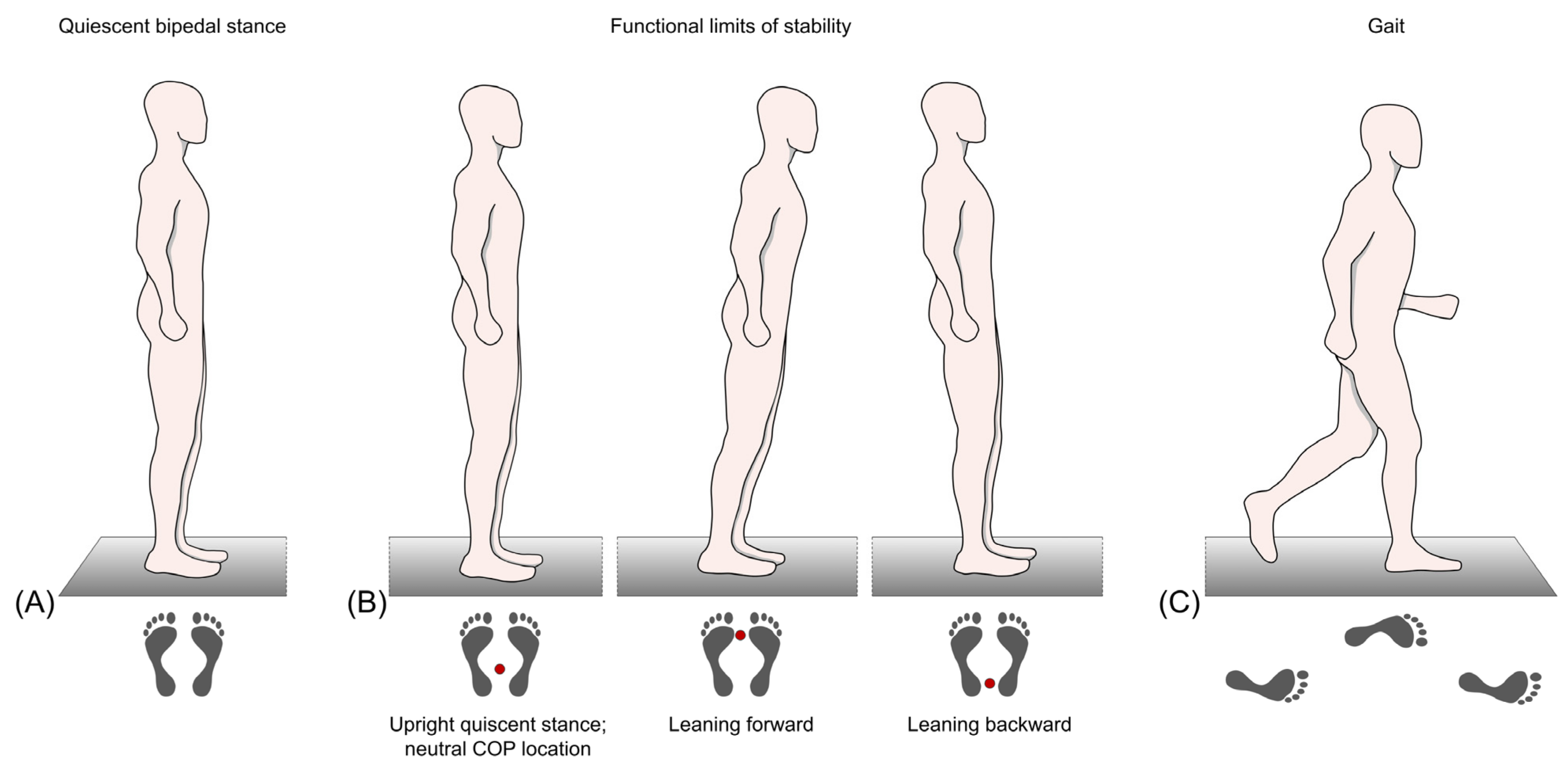
Quiescent Bipedal Stance
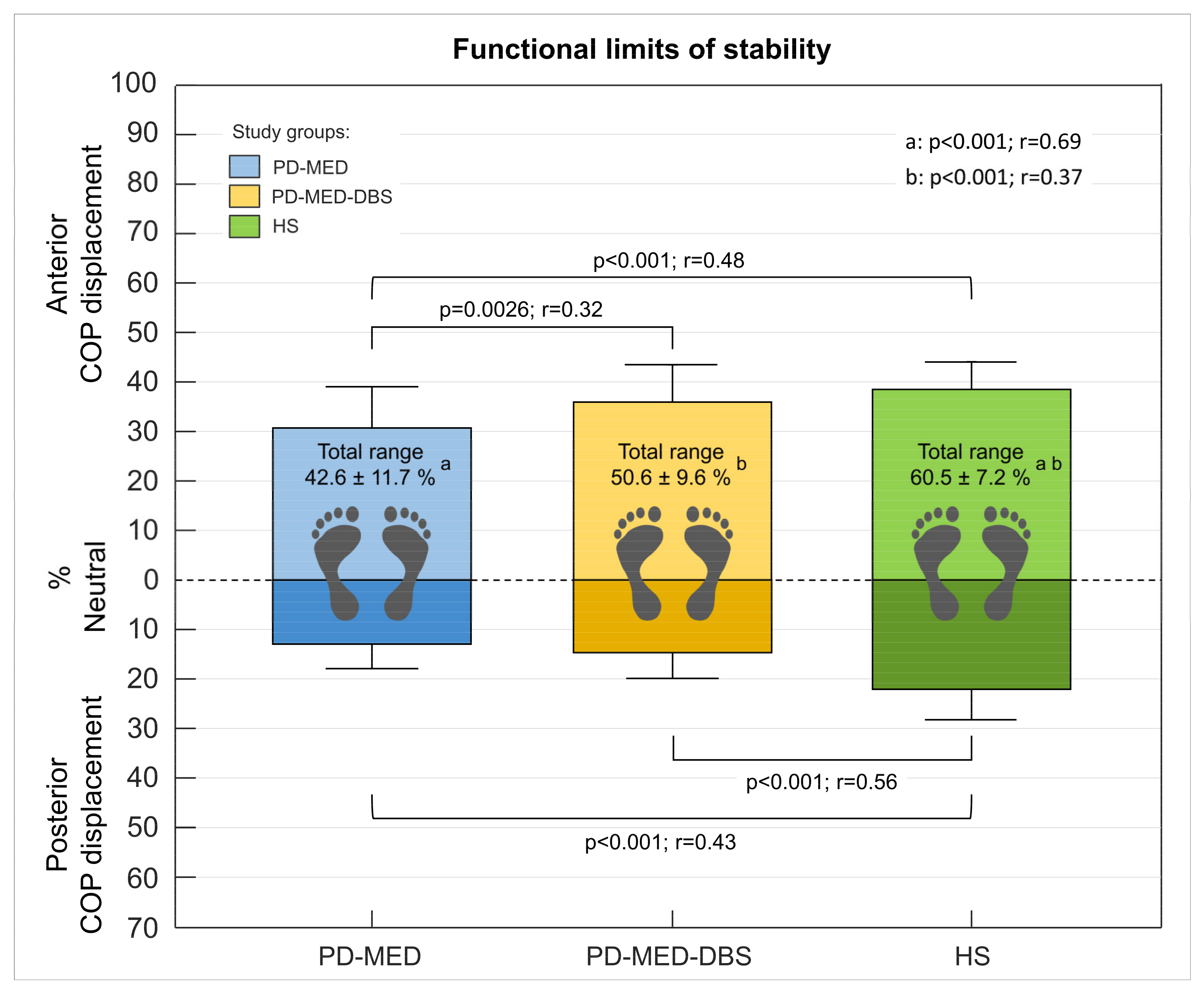
Functional Limits of Stability
Gait
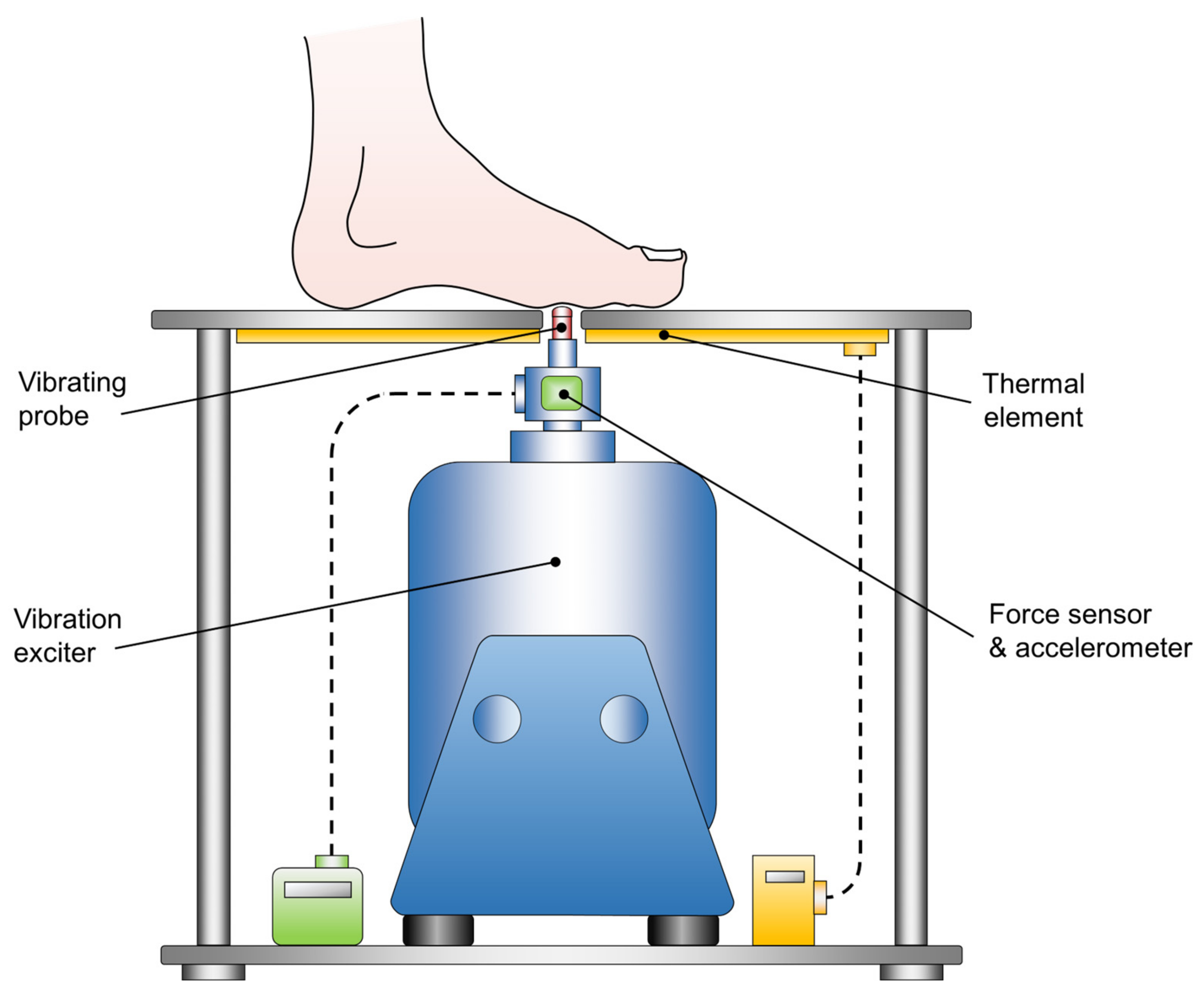
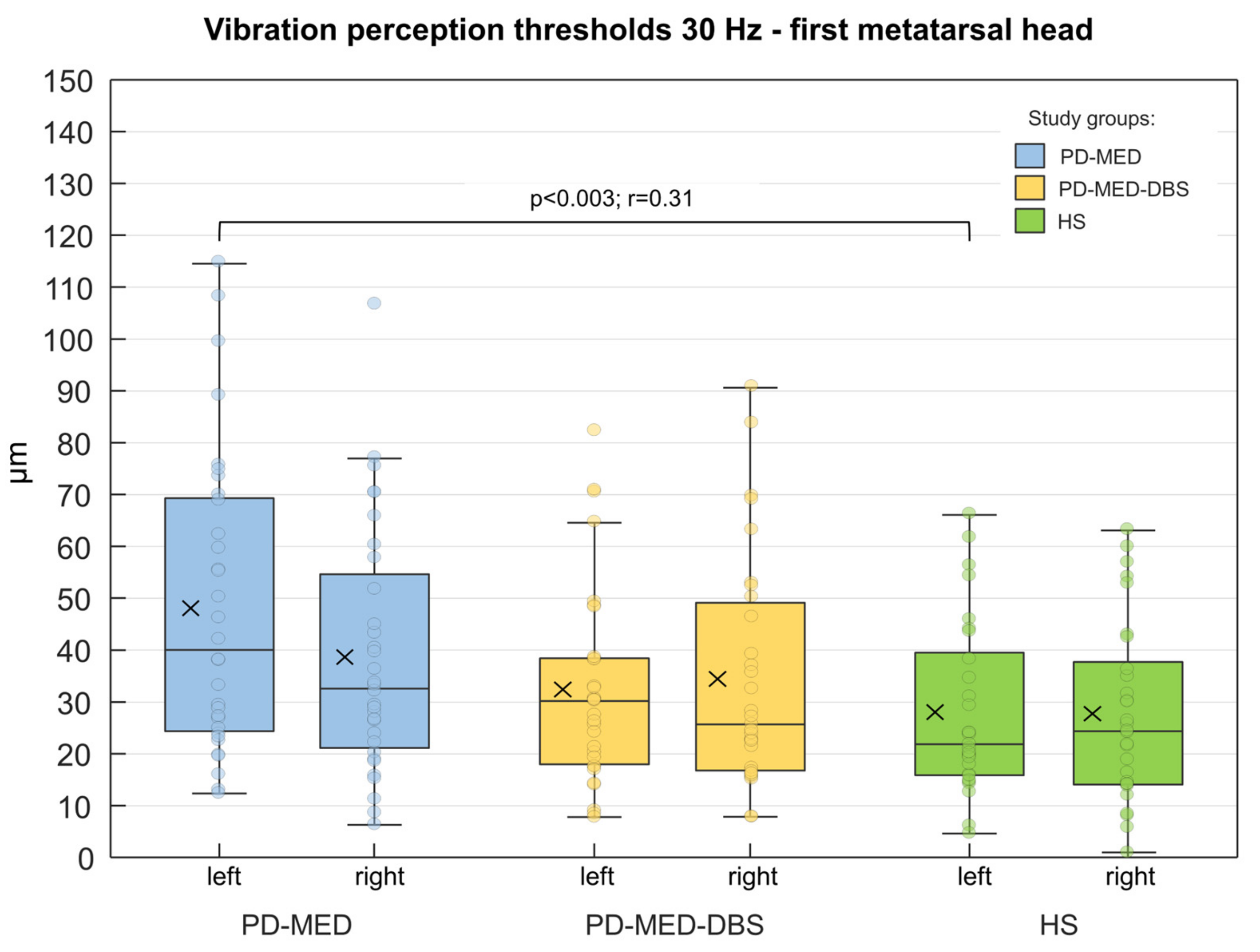
2.2.2. Plantar Vibration Perception
2.3. Data Processing
2.3.1. Motor Performance
Quiescent Bipedal Stance
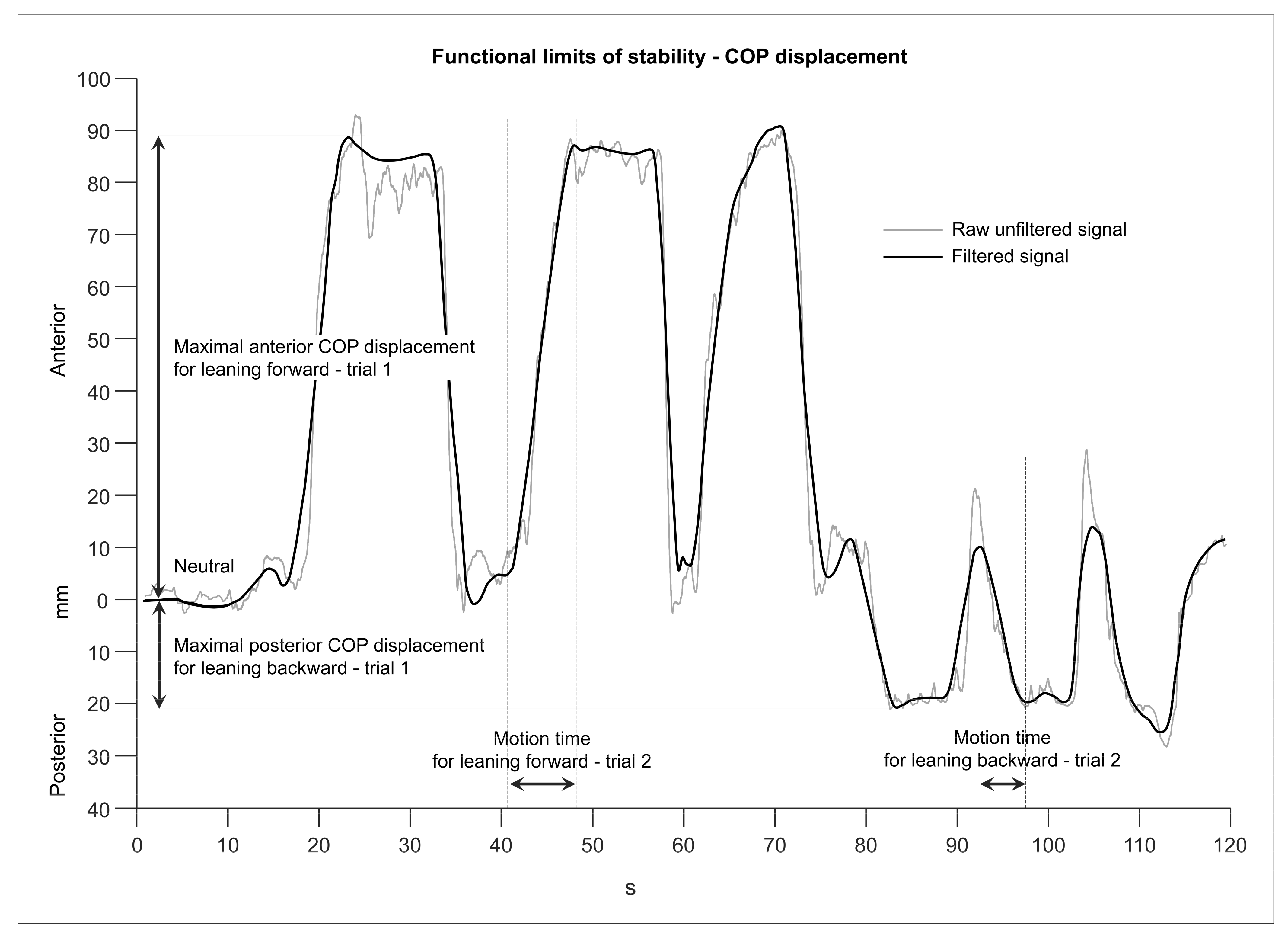
Functional Limits of Stability
Gait
2.3.2. Plantar Cutaneous Vibration Perception
2.4. Statistical Analysis
3. Results
3.1. Demographic and Clinical Data
3.2. Motor Performance
3.2.1. Quiescent Bipedal Stance
- Inter-Group Comparisons
- Intra-Group Comparisons
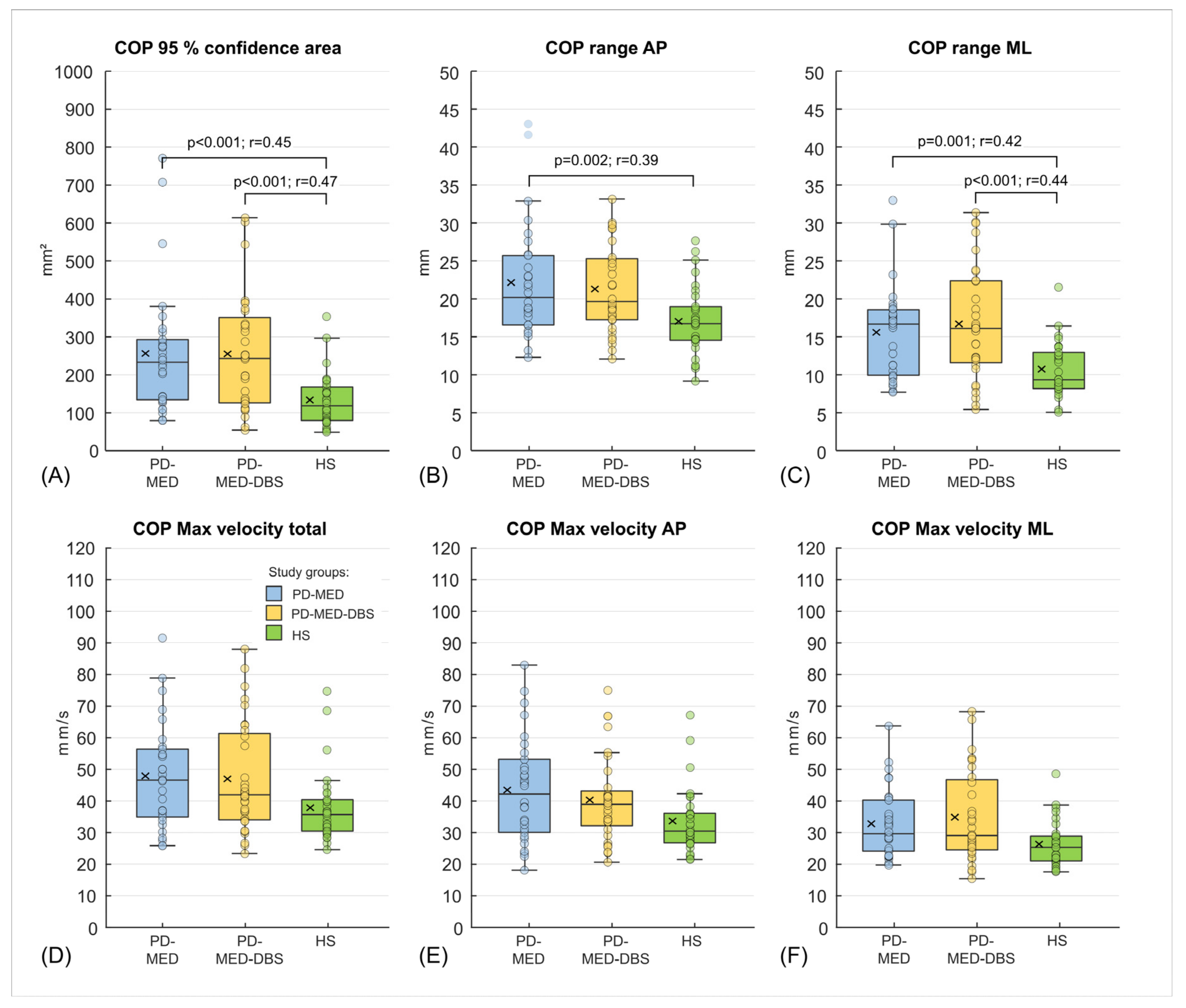
3.2.2. Functional Limits of Stability
- Inter-Group Comparisons
- Intra-Group Comparisons
3.2.3. Gait
- Inter-Group Comparisons
- Intra-Group Comparisons
3.3. Plantar Cutaneous Vibration Perception
- Inter-Group Comparisons
- Intra-Group Comparisons
4. Discussion
4.1. Motor Performance
4.1.1. Quiescent Bipedal Stance
4.1.2. Functional Limits of Stability
4.1.3. Gait
4.2. Plantar Cutaneous Vibration Perception
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Weerasak, M.; Aju, M.; Hiroyuki, H.; Seidel, D. A systematic review of the worldwide prevalence and incidence of Parkinson’s disease. J. Med. Assoc. Thail. 2011, 94, 19–55. [Google Scholar]
- Tysnes, O.-B.; Storstein, A. Epidemiology of Parkinson’s disease. J. Neural Transm. 2017, 124, 901–905. [Google Scholar] [CrossRef]
- Ou, Z.; Pan, J.; Tang, S.; Duan, D.; Yu, D.; Nong, H.; Wang, Z. Global Trends in the Incidence, Prevalence, and Years Lived with Disability of Parkinson’s Disease in 204 Countries/Territories From 1990 to 2019. Front. Public Health 2021, 9, 776847. [Google Scholar] [CrossRef]
- Berardelli, A. Neurophysiology of basal ganglia diseases. In Parkinson’s Disease and Related Disorders, Part I; Elsevier: Amsterdam, The Netherlands, 2007; pp. 67–75. ISBN 9780444519009. [Google Scholar]
- Agid, Y. Parkinson’s disease: Pathophysiology. Lancet 1991, 337, 1321–1324. [Google Scholar] [CrossRef] [PubMed]
- Blandini, F.; Nappi, G.; Tassorelli, C.; Martignoni, E. Functional changes of the basal ganglia circuitry in Parkinson’s disease. Prog. Neurobiol. 2000, 62, 63–88. [Google Scholar] [CrossRef] [PubMed]
- Poewe, W.; Seppi, K.; Tanner, C.M.; Halliday, G.M.; Brundin, P.; Volkmann, J.; Schrag, A.-E.; Lang, A.E. Parkinson disease. Nat. Rev. Dis. Primers 2017, 3, 17013. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.D.; Allen, N.E.; Canning, C.G.; Fung, V.S.C. Postural instability in patients with Parkinson’s disease. Epidemiology, pathophysiology and management. CNS Drugs 2013, 27, 97–112. [Google Scholar] [CrossRef] [PubMed]
- Sveinbjornsdottir, S. The clinical symptoms of Parkinson’s disease. J. Neurochem. 2016, 139 (Suppl. 1), 318–324. [Google Scholar] [CrossRef] [PubMed]
- Schapira, A.H. Science, medicine, and the future: Parkinson’s disease. BMJ 1999, 318, 311–314. [Google Scholar] [CrossRef] [PubMed]
- Shahed, J.; Jankovic, J. Motor symptoms in Parkinson’s disease. In Parkinson’s Disease and Related Disorders, Part I; Elsevier: Amsterdam, The Netherlands, 2007; pp. 329–342. ISBN 9780444519009. [Google Scholar]
- Benatru, I.; Vaugoyeau, M.; Azulay, J.-P. Postural disorders in Parkinson’s disease. Neurophysiol. Clin. 2008, 38, 459–465. [Google Scholar] [CrossRef]
- Del Din, S.; Godfrey, A.; Coleman, S.; Galna, B.; Lord, S.; Rochester, L. Time-dependent changes in postural control in early Parkinson’s disease: What are we missing? Med. Biol. Eng. Comput. 2016, 54, 401–410. [Google Scholar] [CrossRef]
- Martin, W.R.W.; Wieler, M. Treatment of Parkinson’s disease. Can. J. Neurol. Sci. 2003, 30 (Suppl. 1), S27–S33. [Google Scholar] [CrossRef]
- May, D.S.; van Dillen, L.R.; Earhart, G.M.; Rawson, K.S.; Perlmutter, J.S.; Duncan, R.P. Effects of Subthalamic Nucleus Deep Brain Stimulation and Levodopa on Balance in People with Parkinson’s Disease: A Cross Sectional Study. Brain Sci. 2020, 10, 693. [Google Scholar] [CrossRef]
- Jellinger, K.A. Neuropathobiology of non-motor symptoms in Parkinson disease. J. Neural Transm. 2015, 122, 1429–1440. [Google Scholar] [CrossRef]
- Chaudhuri, K.R.; Schapira, A.H.V. Non-motor symptoms of Parkinson’s disease: Dopaminergic pathophysiology and treatment. Lancet Neurol. 2009, 8, 464–474. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, R.F.; Bodis-Wollner, I. Parkinsons Disease and Nonmotor Dysfunction; Springer: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- Hogg, E.; Wertheimer, J.; Graner, S.; Tagliati, M. Deep Brain Stimulation and Nonmotor Symptoms. Int. Rev. Neurobiol. 2017, 134, 1045–1089. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, N.; Maas, K.C.; Shah, V.V.; Carlson-Kuhta, P.; Nutt, J.G.; Horak, F.B.; Asaka, T.; Mancini, M. Functional limits of stability and standing balance in people with Parkinson’s disease with and without freezing of gait using wearable sensors. Gait Posture 2021, 87, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.; Nilsson, M.H.; Rehncrona, S.; Tjernström, F.; Magnusson, M.; Johansson, R.; Fransson, P.-A. Strategic alterations of posture are delayed in Parkinson’s disease patients during deep brain stimulation. Sci. Rep. 2021, 11, 23550. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.; Nilsson, M.H.; Rehncrona, S.; Tjernström, F.; Magnusson, M.; Johansson, R.; Fransson, P.-A. Effects of Deep Brain Stimulation on Postural Control in Parkinson’s Disease. Comput. Biol. Med. 2020, 122, 103828. [Google Scholar] [CrossRef] [PubMed]
- Palakurthi, B.; Burugupally, S.P. Postural Instability in Parkinson’s Disease: A Review. Brain Sci. 2019, 9, 239. [Google Scholar] [CrossRef]
- Vitale, C.; Marcelli, V.; Furia, T.; Santangelo, G.; Cozzolino, A.; Longo, K.; Allocca, R.; Amboni, M.; Marciano, E.; Barone, P. Vestibular impairment and adaptive postural imbalance in parkinsonian patients with lateral trunk flexion. Mov. Disord. 2011, 26, 1458–1463. [Google Scholar] [CrossRef]
- Bertolini, G.; Wicki, A.; Baumann, C.R.; Straumann, D.; Palla, A. Impaired tilt perception in Parkinson’s disease: A central vestibular integration failure. PLoS ONE 2015, 10, e0124253. [Google Scholar] [CrossRef]
- Park, J.-H.; Kang, Y.-J.; Horak, F.B. What Is Wrong with Balance in Parkinson’s Disease? J. Mov. Disord. 2015, 8, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Horak, F.B.; Dimitrova, D.; Nutt, J.G. Direction-specific postural instability in subjects with Parkinson’s disease. Exp. Neurol. 2005, 193, 504–521. [Google Scholar] [CrossRef] [PubMed]
- Termoz, N.; Halliday, S.E.; Winter, D.A.; Frank, J.S.; Patla, A.E.; Prince, F. The control of upright stance in young, elderly and persons with Parkinson’s disease. Gait Posture 2008, 27, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, M.G.; Bloem, B.R. Postural control in Parkinson patients: A proprioceptive problem? Exp. Neurol. 2011, 227, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, L.; e Souza, T.M.; Bizarro, L.; Oliveira, A. Proprioceptive deficits in Parkinson’s disease: From clinical data to animal experimentation. Psychol. Neurosci. 2011, 4, 235–244. [Google Scholar] [CrossRef]
- Vaugoyeau, M.; Viel, S.; Amblard, B.; Azulay, J.P.; Assaiante, C. Proprioceptive contribution of postural control as assessed from very slow oscillations of the support in healthy humans. Gait Posture 2008, 27, 294–302. [Google Scholar] [CrossRef] [PubMed]
- Sabourin, S.; Khazen, O.; DiMarzio, M.; Staudt, M.D.; Williams, L.; Gillogly, M.; Durphy, J.; Hanspal, E.K.; Adam, O.R.; Pilitsis, J.G. Effect of Directional Deep Brain Stimulation on Sensory Thresholds in Parkinson’s Disease. Front. Hum. Neurosci. 2020, 14, 217. [Google Scholar] [CrossRef]
- Belasen, A.; Rizvi, K.; Gee, L.E.; Yeung, P.; Prusik, J.; Ramirez-Zamora, A.; Hanspal, E.; Paiva, P.; Durphy, J.; Argoff, C.E.; et al. Effect of low-frequency deep brain stimulation on sensory thresholds in Parkinson’s disease. J. Neurosurg. 2017, 126, 397–403. [Google Scholar] [CrossRef]
- de Andrade, D.C.; Lefaucheur, J.-P.; Galhardoni, R.; Ferreira, K.S.; Paiva, A.R.B.; Bor-Seng-Shu, E.; Alvarenga, L.; Myczkowski, M.L.; Marcolin, M.A.; de Siqueira, S.R.; et al. Subthalamic deep brain stimulation modulates small fiber-dependent sensory thresholds in Parkinson’s disease. Pain 2012, 153, 1107–1113. [Google Scholar] [CrossRef] [PubMed]
- Zia, S.; Cody, F.W.J.; O’Boyle, D.J. Identification of unilateral elbow-joint position is impaired by Parkinson’s disease. Clin. Anat. 2002, 15, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Aman, J.E.; Abosch, A.; Bebler, M.; Lu, C.-H.; Konczak, J. Subthalamic nucleus deep brain stimulation improves somatosensory function in Parkinson’s disease. Mov. Disord. 2014, 29, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Gierthmühlen, J.; Arning, P.; Binder, A.; Herzog, J.; Deuschl, G.; Wasner, G.; Baron, R. Influence of deep brain stimulation and levodopa on sensory signs in Parkinson’s disease. Mov. Disord. 2010, 25, 1195–1202. [Google Scholar] [CrossRef] [PubMed]
- Maschke, M.; Tuite, P.J.; Krawczewski, K.; Pickett, K.; Konczak, J. Perception of heaviness in Parkinson’s disease. Mov. Disord. 2006, 21, 1013–1018. [Google Scholar] [CrossRef]
- Zia, S.; Cody, F.; O’Boyle, D. Joint position sense is impaired by Parkinson’s disease. Ann. Neurol. Off. J. Am. Neurol. Assoc. Child Neurol. Soc. 2000, 47, 218–228. [Google Scholar] [CrossRef]
- Day, B.L.; Fitzpatrick, R.C. The vestibular system. Curr. Biol. 2005, 15, R583–R586. [Google Scholar] [CrossRef]
- Novak, P.; Novak, V. Effect of step-synchronized vibration stimulation of soles on gait in Parkinson’s disease: A pilot study. J. Neuroeng. Rehabil. 2006, 3, 9. [Google Scholar] [CrossRef]
- Viseux, F.J. The sensory role of the sole of the foot: Review and update on clinical perspectives. Neurophysiol. Clin. 2020, 50, 55–68. [Google Scholar] [CrossRef]
- Phuenpathom, W.; Panyakaew, P.; Vateekul, P.; Surangsrirat, D.; Hiransuthikul, A.; Bhidayasiri, R. Vibratory and plantar pressure stimulation: Steps to improve freezing of gait in Parkinson’s disease. Park. Relat. Disord. 2022, 105, 43–51. [Google Scholar] [CrossRef]
- Qiu, F.; Cole, M.H.; Davids, K.W.; Hennig, E.M.; Silburn, P.A.; Netscher, H.; Kerr, G.K. Effects of textured insoles on balance in people with Parkinson’s disease. PLoS ONE 2013, 8, e83309. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, M.E.; Almeida, Q.J.; Spaulding, S.J.; van Oostveen, R.B.; Holmes, J.D.; Johnson, A.M.; Perry, S.D. Plantar cutaneous sensory stimulation improves single-limb support time, and EMG activation patterns among individuals with Parkinson’s disease. Park. Relat. Disord. 2009, 15, 697–702. [Google Scholar] [CrossRef]
- Germano, A.M.C.; Heß, T.; Schmidt, D.; Milani, T.L. Effects of plantar hypothermia on quasi-static balance: Two different hypothermic procedures. Gait Posture 2018, 60, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Heß, T.; Milani, T.L.; Meixensberger, J.; Krause, M. Postural performance and plantar cutaneous vibration perception in patients with idiopathic normal pressure hydrocephalus. Heliyon 2021, 7, e05811. [Google Scholar] [CrossRef] [PubMed]
- McKeown, M.D.; Peters, R.M.; Pasman, E.P.; McKeown, M.J.; Carpenter, M.G.; Inglis, J.T. Plantar cutaneous function in Parkinson’s disease patients ON and OFF L-dopa. Neurosci. Lett. 2016, 629, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Meyer, P.F.; Oddsson, L.I.E.; de Luca, C.J. The role of plantar cutaneous sensation in unperturbed stance. Exp. Brain Res. 2004, 156, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Nurse, M.A.; Nigg, B.M. The effect of changes in foot sensation on plantar pressure and muscle activity. Clin. Biomech. 2001, 16, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Perry, S.D.; Santos, L.C.; Patla, A.E. Contribution of vision and cutaneous sensation to the control of centre of mass (COM) during gait termination. Brain Res. 2001, 913, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Perry, S.D.; McIlroy, W.E.; Maki, B.E. The role of plantar cutaneous mechanoreceptors in the control of compensatory stepping reactions evoked by unpredictable, multi-directional perturbation. Brain Res. 2000, 877, 401–406. [Google Scholar] [CrossRef]
- McKeon, P.O.; Hertel, J. Diminished Plantar Cutaneous Sensation and Postural Control. Percept Mot Ski. 2007, 104, 56–66. [Google Scholar] [CrossRef]
- McKeon, P.O.; Hertel, J. Plantar hypoesthesia alters time-to-boundary measures of postural control. Somatosens. Mot. Res. 2007, 24, 171–177. [Google Scholar] [CrossRef]
- Song, K.; Kang, T.K.; Wikstrom, E.A.; Jun, H.-p.; Lee, S.Y. Effects of reduced plantar cutaneous sensation on static postural control in individuals with and without chronic ankle instability. J. Sci. Med. Sport 2017, 20, 910–914. [Google Scholar] [CrossRef] [PubMed]
- Germano, A.M.C.; Schmidt, D.; Milani, T.L. Effects of hypothermically reduced plantar skin inputs on anticipatory and compensatory balance responses. BMC Neurosci. 2016, 17, 41. [Google Scholar] [CrossRef] [PubMed]
- Jellinger, K. The role of α-synuclein in neurodegeneration—An update. Transl. Neurosci. 2012, 3, 1015. [Google Scholar] [CrossRef]
- Bennett, M.C. The role of α-synuclein in neurodegenerative diseases. Pharmacol. Ther. 2005, 105, 311–331. [Google Scholar] [CrossRef] [PubMed]
- Beach, T.G.; Adler, C.H.; Lue, L.; Sue, L.I.; Bachalakuri, J.; Henry-Watson, J.; Sasse, J.; Boyer, S.; Shirohi, S.; Brooks, R.; et al. Unified staging system for Lewy body disorders: Correlation with nigrostriatal degeneration, cognitive impairment and motor dysfunction. Acta Neuropathol. 2009, 117, 613–634. [Google Scholar] [CrossRef]
- Kovacs, G.G.; Milenkovic, I.J.; Preusser, M.; Budka, H. Nigral burden of alpha-synuclein correlates with striatal dopamine deficit. Mov. Disord. 2008, 23, 1608–1612. [Google Scholar] [CrossRef]
- Gold, A.; Turkalp, Z.T.; Munoz, D.G. Enteric alpha-synuclein expression is increased in Parkinson’s disease but not Alzheimer’s disease. Mov. Disord. 2013, 28, 237–240. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.K.; Zhang, Y.; Lim, K.L.; Tanaka, Y.; Huang, H.; Gao, J.; Ross, C.A.; Dawson, V.L.; Dawson, T.M. Parkin ubiquitinates the alpha-synuclein-interacting protein, synphilin-1: Implications for Lewy-body formation in Parkinson disease. Nat. Med. 2001, 7, 1144–1150. [Google Scholar] [CrossRef]
- Ikemura, M.; Saito, Y.; Sengoku, R.; Sakiyama, Y.; Hatsuta, H.; Kanemaru, K.; Sawabe, M.; Arai, T.; Ito, G.; Iwatsubo, T.; et al. Lewy body pathology involves cutaneous nerves. J. Neuropathol. Exp. Neurol. 2008, 67, 945–953. [Google Scholar] [CrossRef]
- Nolano, M.; Provitera, V.; Estraneo, A.; Selim, M.M.; Caporaso, G.; Stancanelli, A.; Saltalamacchia, A.M.; Lanzillo, B.; Santoro, L. Sensory deficit in Parkinson’s disease: Evidence of a cutaneous denervation. Brain 2008, 131, 1903–1911. [Google Scholar] [CrossRef]
- Braak, H.; Tredici, K.D. Nervous system pathology in sporadic Parkinson disease. Neurology 2008, 70, 1916–1925. [Google Scholar] [CrossRef]
- Braak, H.; Tredici, K.D.; Rüb, U.; de Vos, R.A.; Jansen Steur, E.N.; Braak, E. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol. Aging 2003, 24, 197–211. [Google Scholar] [CrossRef]
- Wakabayashi, K.; Mori, F.; Tanji, K.; Orimo, S.; Takahashi, H. Involvement of the peripheral nervous system in synucleinopathies, tauopathies and other neurodegenerative proteinopathies of the brain. Acta Neuropathol. 2010, 120, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Beach, T.G.; Adler, C.H.; Sue, L.I.; Vedders, L.; Lue, L.; White Iii, C.L.; Akiyama, H.; Caviness, J.N.; Shill, H.A.; Sabbagh, M.N.; et al. Multi-organ distribution of phosphorylated alpha-synuclein histopathology in subjects with Lewy body disorders. Acta Neuropathol. 2010, 119, 689–702. [Google Scholar] [CrossRef] [PubMed]
- Beudel, M.; Macerollo, A.; Brown, M.J.N.; Chen, R. Editorial: The Role of the Basal Ganglia in Somatosensory-Motor Interactions: Evidence from Neurophysiology and Behavior. Front. Hum. Neurosci. 2019, 13, 451. [Google Scholar] [CrossRef] [PubMed]
- Nagy, A.; Eördegh, G.; Paróczy, Z.; Márkus, Z.; Benedek, G. Multisensory integration in the basal ganglia. Eur. J. Neurosci. 2006, 24, 917–924. [Google Scholar] [CrossRef] [PubMed]
- Colder, B. The basal ganglia select the expected sensory input used for predictive coding. Front. Comput. Neurosci. 2015, 9, 119. [Google Scholar] [CrossRef]
- Peller, M.; Zeuner, K.E.; Munchau, A.; Quartarone, A.; Weiss, M.; Knutzen, A.; Hallett, M.; Deuschl, G.; Siebner, H.R. The basal ganglia are hyperactive during the discrimination of tactile stimuli in writer’s cramp. Brain 2006, 129, 2697–2708. [Google Scholar] [CrossRef] [PubMed]
- Boecker, H.; Ceballos-Baumann, A.; Bartenstein, P.; Weindl, A.; Siebner, H.R.; Fassbender, T.; Munz, F.; Schwaiger, M.; Conrad, B. Sensory processing in Parkinson’s and Huntington’s disease: Investigations with 3D H215O-PET. Brain 1999, 122 Pt 9, 1651–1665. [Google Scholar] [CrossRef]
- Korsun, O.; Renvall, H.; Nurminen, J.; Mäkelä, J.P.; Pekkonen, E. Modulation of sensory cortical activity by deep brain stimulation in advanced Parkinson’s disease. Eur. J. Neurosci. 2022, 56, 3979–3990. [Google Scholar] [CrossRef] [PubMed]
- Schneider, J.S.; Morse, J.R.; Lidsky, T.I. Somatosensory properties of globus pallidus neurons in awake cats. Exp. Brain Res. 1982, 46, 311–314. [Google Scholar] [CrossRef]
- Rothblat, D.S.; Schneider, J.S. Alterations in pallidal neuronal responses to peripheral sensory and striatal stimulation in symptomatic and recovered Parkinsonian cats. Brain Res. 1995, 705, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Rothblat, D.S.; Schneider, J.S. Response of caudate neurons to stimulation of intrinsic and peripheral afferents in normal, symptomatic, and recovered MPTP-treated cats. J. Neurosci. 1993, 13, 4372–4378. [Google Scholar] [CrossRef]
- Seitz, R.J.; Roland, P.E. Vibratory stimulation increases and decreases the regional cerebral blood flow and oxidative metabolism: A positron emission tomography (PET) study. Acta Neurol. Scand. 1992, 86, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Schneider, J.S.; Diamond, S.G.; Markham, C.H. Parkinson’s disease: Sensory and motor problems in arms and hands. Neurology 1987, 37, 951–956. [Google Scholar] [CrossRef]
- Sathian, K.; Zangaladze, A.; Green, J.; Vitek, J.L.; DeLong, M.R. Tactile spatial acuity and roughness discrimination: Impairments due to aging and Parkinson’s disease. Neurology 1997, 49, 168–177. [Google Scholar] [CrossRef] [PubMed]
- Zia, S.; Cody, F.W.J.; O’Boyle, D.J. Discrimination of bilateral differences in the loci of tactile stimulation is impaired in subjects with Parkinson’s disease. Clin. Anat. 2003, 16, 241–247. [Google Scholar] [CrossRef]
- Weder, B.J.; Leenders, K.L.; Vontobel, P.; Nienhusmeier, M.; Keel, A.; Zaunbauer, W.; Vonesch, T.; Ludin, H.-P. Impaired somatosensory discrimination of shape in Parkinson’s disease: Association with caudate nucleus dopaminergic function. Hum. Brain Mapp. 1999, 8, 1–12. [Google Scholar] [CrossRef]
- Cury, R.G.; Galhardoni, R.; Fonoff, E.T.; Perez Lloret, S.; Dos Santos Ghilardi, M.G.; Barbosa, E.R.; Teixeira, M.J.; Ciampi de Andrade, D. Sensory abnormalities and pain in Parkinson disease and its modulation by treatment of motor symptoms. Eur. J. Pain 2016, 20, 151–165. [Google Scholar] [CrossRef]
- Conte, A.; Khan, N.; Defazio, G.; Rothwell, J.C.; Berardelli, A. Pathophysiology of somatosensory abnormalities in Parkinson disease. Nat. Rev. Neurol. 2013, 9, 687–697. [Google Scholar] [CrossRef]
- Conte, A.; Modugno, N.; Lena, F.; Dispenza, S.; Gandolfi, B.; Iezzi, E.; Fabbrini, G.; Berardelli, A. Subthalamic nucleus stimulation and somatosensory temporal discrimination in Parkinson’s disease. Brain 2010, 133, 2656–2663. [Google Scholar] [CrossRef]
- Hammond, C.; Bergman, H.; Brown, P. Pathological synchronization in Parkinson’s disease: Networks, models and treatments. Trends Neurosci. 2007, 30, 357–364. [Google Scholar] [CrossRef]
- Ikeda, K.; Deguchi, K.; Kume, K.; Kamada, M.; Touge, T.; Masaki, T. Assessment of sensory perception and processing using current perception threshold in Parkinson’s disease. Neurol. Clin. Neurosci. 2013, 1, 209–213. [Google Scholar] [CrossRef]
- Prätorius, B.; Kimmeskamp, S.; Milani, T. The sensitivity of the sole of the foot in patients with Morbus Parkinson. Neurosci. Lett. 2003, 346, 173–176. [Google Scholar] [CrossRef] [PubMed]
- Doty, R.L.; Gandhi, S.S.; Osman, A.; Hurtig, H.I.; Pawasarat, I.; Beals, E.; Chung, I.; Dubroff, J.; Newberg, A.; Ying, G.-S.; et al. Point pressure sensitivity in early stage Parkinson’s disease. Physiol. Behav. 2015, 138, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Cury, R.G.; Galhardoni, R.; Teixeira, M.J.; Dos Santos Ghilardi, M.G.; Silva, V.; Myczkowski, M.L.; Marcolin, M.A.; Barbosa, E.R.; Fonoff, E.T.; Ciampi de Andrade, D. Subthalamic deep brain stimulation modulates conscious perception of sensory function in Parkinson’s disease. Pain 2016, 157, 2758–2765. [Google Scholar] [CrossRef] [PubMed]
- Cury, R.G.; Galhardoni, R.; Fonoff, E.T.; Dos Santos Ghilardi, M.G.; Fonoff, F.; Arnaut, D.; Myczkowski, M.L.; Marcolin, M.A.; Bor-Seng-Shu, E.; Barbosa, E.R.; et al. Effects of deep brain stimulation on pain and other nonmotor symptoms in Parkinson disease. Neurology 2014, 83, 1403–1409. [Google Scholar] [CrossRef] [PubMed]
- Dogru Huzmeli, E.; Yilmaz, A.; Okuyucu, E. Analysis of the effects of subthalamic nucleus deep brain stimulation on somatosensation in Parkinson’s disease patients. Neurol. Sci. 2020, 41, 925–931. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.-H.; Zhang, L.; Sperry, L.; Olichney, J.; Farias, S.T.; Shahlaie, K.; Chang, N.M.; Liu, Y.; Wang, S.-P.; Wang, C. Target Selection Recommendations Based on Impact of Deep Brain Stimulation Surgeries on Nonmotor Symptoms of Parkinson’s Disease. Chin. Med. J. 2015, 128, 3371–3380. [Google Scholar] [CrossRef] [PubMed]
- Djaldetti, R.; Melamed, E. Sensory symptoms in Parkinson’s disease. In Parkinson’s Disease and Related Disorders, Part I; Elsevier: Amsterdam, The Netherlands, 2007; pp. 377–384. ISBN 9780444519009. [Google Scholar]
- Maruo, T.; Saitoh, Y.; Hosomi, K.; Kishima, H.; Shimokawa, T.; Hirata, M.; Goto, T.; Morris, S.; Harada, Y.; Yanagisawa, T.; et al. Deep brain stimulation of the subthalamic nucleus improves temperature sensation in patients with Parkinson’s disease. Pain 2011, 152, 860–865. [Google Scholar] [CrossRef]
- Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, C.W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov. Disord. 2015, 30, 1591–1601. [Google Scholar] [CrossRef] [PubMed]
- Beuter, A.; Modolo, J. Delayed and lasting effects of deep brain stimulation on locomotion in Parkinson’s disease. Chaos 2009, 19, 26114. [Google Scholar] [CrossRef]
- Castrioto, A.; Lozano, A.M.; Poon, Y.-Y.; Lang, A.E.; Fallis, M.; Moro, E. Ten-year outcome of subthalamic stimulation in Parkinson disease: A blinded evaluation. Arch. Neurol. 2011, 68, 1550–1556. [Google Scholar] [CrossRef]
- Zibetti, M.; Merola, A.; Rizzi, L.; Ricchi, V.; Angrisano, S.; Azzaro, C.; Artusi, C.A.; Arduino, N.; Marchisio, A.; Lanotte, M.; et al. Beyond nine years of continuous subthalamic nucleus deep brain stimulation in Parkinson’s disease. Mov. Disord. 2011, 26, 2327–2334. [Google Scholar] [CrossRef] [PubMed]
- Fasano, A.; Romito, L.M.; Daniele, A.; Piano, C.; Zinno, M.; Bentivoglio, A.R.; Albanese, A. Motor and cognitive outcome in patients with Parkinson’s disease 8 years after subthalamic implants. Brain 2010, 133, 2664–2676. [Google Scholar] [CrossRef] [PubMed]
- Germano, A.M.C.; Schlee, G.; Milani, T.L. Effect of cooling foot sole skin receptors on achilles tendon reflex. Muscle Nerve 2016, 53, 965–971. [Google Scholar] [CrossRef]
- Schlee, G.; Sterzing, T.; Milani, T.L. Foot sole skin temperature affects plantar foot sensitivity. Clin. Neurophysiol. 2009, 120, 1548–1551. [Google Scholar] [CrossRef]
- Nikaido, Y.; Akisue, T.; Kajimoto, Y.; Tucker, A.; Kawami, Y.; Urakami, H.; Iwai, Y.; Sato, H.; Nishiguchi, T.; Hinoshita, T.; et al. Postural instability differences between idiopathic normal pressure hydrocephalus and Parkinson’s disease. Clin. Neurol. Neurosurg. 2018, 165, 103–107. [Google Scholar] [CrossRef]
- Mancini, M.; Rocchi, L.; Horak, F.B.; Chiari, L. Effects of Parkinson’s disease and levodopa on functional limits of stability. Clin. Biomech. 2008, 23, 450–458. [Google Scholar] [CrossRef]
- Schlenstedt, C.; Muthuraman, M.; Witt, K.; Weisser, B.; Fasano, A.; Deuschl, G. Postural control and freezing of gait in Parkinson’s disease. Park. Relat. Disord. 2016, 24, 107–112. [Google Scholar] [CrossRef]
- Ganesan, M.; Pal, P.K.; Gupta, A.; Sathyaprabha, T.N. Dynamic posturography in evaluation of balance in patients of Parkinson’s disease with normal pull test: Concept of a diagonal pull test. Park. Relat. Disord. 2010, 16, 595–599. [Google Scholar] [CrossRef] [PubMed]
- Müller, K.; Fröhlich, S.; Germano, A.M.C.; Kondragunta, J.; Agoitia Hurtado, M.F.D.C.; Rudisch, J.; Schmidt, D.; Hirtz, G.; Stollmann, P.; Voelcker-Rehage, C. Sensor-based systems for early detection of dementia (SENDA): A study protocol for a prospective cohort sequential study. BMC Neurol. 2020, 20, 84. [Google Scholar] [CrossRef]
- Schmidt, D.; Germano, A.M.; Milani, T.L.; Khaiyat, O. Subjective sensitivity data: Considerations to treat heteroscedasticity. Cogent Med. 2019, 6, 1673086. [Google Scholar] [CrossRef]
- Cobo, R.; García-Piqueras, J.; Cobo, J.; Vega, J.A. The Human Cutaneous Sensory Corpuscles: An Update. J. Clin. Med. 2021, 10, 227. [Google Scholar] [CrossRef] [PubMed]
- McGlone, F.; Reilly, D. The cutaneous sensory system. Neurosci. Biobehav. Rev. 2010, 34, 148–159. [Google Scholar] [CrossRef] [PubMed]
- Hagander, L.G.; Midani, H.A.; Kuskowski, M.A.; Parry, G.J. Quantitative sensory testing: Effect of site and pressure on vibration thresholds. Clin. Neurophysiol. 2000, 111, 1066–1069. [Google Scholar] [CrossRef]
- Zippenfennig, C.; Wynands, B.; Milani, T.L. Vibration Perception Thresholds of Skin Mechanoreceptors Are Influenced by Different Contact Forces. J. Clin. Med. 2021, 10, 3083. [Google Scholar] [CrossRef]
- Mildren, R.L.; Strzalkowski, N.D.J.; Bent, L.R. Foot sole skin vibration perceptual thresholds are elevated in a standing posture compared to sitting. Gait Posture 2016, 43, 87–92. [Google Scholar] [CrossRef]
- Holowka, N.B.; Wynands, B.; Drechsel, T.J.; Yegian, A.K.; Tobolsky, V.A.; Okutoyi, P.; Mang’eni Ojiambo, R.; Haile, D.W.; Sigei, T.K.; Zippenfennig, C.; et al. Foot callus thickness does not trade off protection for tactile sensitivity during walking. Nature 2019, 571, 261–264. [Google Scholar] [CrossRef]
- Drechsel, T.J.; Monteiro, R.L.; Zippenfennig, C.; Ferreira, J.S.S.P.; Milani, T.L.; Sacco, I.C.N. Low and High Frequency Vibration Perception Thresholds Can Improve the Diagnosis of Diabetic Neuropathy. J. Clin. Med. 2021, 10, 3073. [Google Scholar] [CrossRef] [PubMed]
- Zippenfennig, C.; Drechsel, T.J.; Monteiro, R.L.; Sacco, I.C.; Milani, T.L. The Mechanoreceptor’s Role in Plantar Skin Changes in Individuals with Diabetes Mellitus. J. Clin. Med. 2021, 10, 2537. [Google Scholar] [CrossRef] [PubMed]
- Gomes Paiva, A.F.; Thoumie, P.; Missaoui, B. How far do stabilometric and clinical parameters correlate in peripheral neuropathies? Gait Posture 2017, 52, 11–14. [Google Scholar] [CrossRef] [PubMed]
- Brehm, M.-A.; Scholtes, V.A.; Dallmeijer, A.J.; Twisk, J.W.; Harlaar, J. The importance of addressing heteroscedasticity in the reliability analysis of ratio-scaled variables: An example based on walking energy-cost measurements. Dev. Med. Child Neurol. 2012, 54, 267–273. [Google Scholar] [CrossRef]
- Winter, D.A. Human balance and posture control during standing and walking. Gait Posture 1995, 3, 193–214. [Google Scholar] [CrossRef]
- Fransson, P.-A.; Nilsson, M.H.; Rehncrona, S.; Tjernström, F.; Magnusson, M.; Johansson, R.; Patel, M. Deep brain stimulation in the subthalamic nuclei alters postural alignment and adaptation in Parkinson’s disease. PLoS ONE 2021, 16, e0259862. [Google Scholar] [CrossRef]
- Schlenstedt, C.; Gavriliuc, O.; Boße, K.; Wolke, R.; Granert, O.; Deuschl, G.; Margraf, N.G. The Effect of Medication and Deep Brain Stimulation on Posture in Parkinson’s Disease. Front. Neurol. 2019, 10, 1254. [Google Scholar] [CrossRef]
- Schlenstedt, C.; Mancini, M.; Horak, F.; Peterson, D. Anticipatory Postural Adjustment During Self-Initiated, Cued, and Compensatory Stepping in Healthy Older Adults and Patients with Parkinson Disease. Arch. Phys. Med. Rehabil. 2017, 98, 1316–1324.e1. [Google Scholar] [CrossRef]
- Barbieri, F.A.; Polastri, P.F.; Baptista, A.M.; Lirani-Silva, E.; Simieli, L.; Orcioli-Silva, D.; Beretta, V.S.; Gobbi, L.T. Effects of disease severity and medication state on postural control asymmetry during challenging postural tasks in individuals with Parkinson’s disease. Hum. Mov. Sci. 2016, 46, 96–103. [Google Scholar] [CrossRef]
- Beretta, V.S.; Gobbi, L.T.B.; Lirani-Silva, E.; Simieli, L.; Orcioli-Silva, D.; Barbieri, F.A. Challenging Postural Tasks Increase Asymmetry in Patients with Parkinson’s Disease. PLoS ONE 2015, 10, e0137722. [Google Scholar] [CrossRef]
- Collomb-Clerc, A.; Welter, M.-L. Effects of deep brain stimulation on balance and gait in patients with Parkinson’s disease: A systematic neurophysiological review. Neurophysiol. Clin. 2015, 45, 371–388. [Google Scholar] [CrossRef]
- DiFrancisco-Donoghue, J.; Jung, M.-K.; Geisel, P.; Werner, W.G. Learning effects of the sensory organization test as a measure of postural control and balance in Parkinson’s disease. Park. Relat. Disord. 2015, 21, 858–861. [Google Scholar] [CrossRef]
- Johnsen, E.L. Gait and postural instability in Parkinson’s disease treated with deep brain stimulation of the subthalamic nucleus. Dan. Med. Bull. 2011, 58, B4334. [Google Scholar] [PubMed]
- Rocchi, L. Effects of deep brain stimulation and levodopa on postural sway in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2002, 73, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Stylianou, A.P.; McVey, M.A.; Lyons, K.E.; Pahwa, R.; Luchies, C.W. Postural sway in patients with mild to moderate Parkinson’s disease. Int. J. Neurosci. 2011, 121, 614–621. [Google Scholar] [CrossRef] [PubMed]
- Diener, C.; Scholz, E.; Guschlbauer, B.; Dichgans, J. Increased shortening reaction in Parkinson’s disease reflects a difficulty in modulating long loop reflexes. Mov. Disord. 1987, 2, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Schieppati, M.; Nardone, A. Free and supported stance in Parkinson’s disease. The effect of posture and ‘postural set’ on leg muscle responses to perturbation, and its relation to the severity of the disease. Brain 1991, 114 Pt 3, 1227–1244. [Google Scholar] [CrossRef]
- Horak, F.B.; Nutt, J.G.; Nashner, L.M. Postural inflexibility in parkinsonian subjects. J. Neurol. Sci. 1992, 111, 46–58. [Google Scholar] [CrossRef]
- Dimitrova, D.; Horak, F.B.; Nutt, J.G. Postural muscle responses to multidirectional translations in patients with Parkinson’s disease. J. Neurophysiol. 2004, 91, 489–501. [Google Scholar] [CrossRef] [PubMed]
- Beretta, V.S.; Carpenter, M.G.; Barbieri, F.A.; Santos, P.C.R.; Orcioli-Silva, D.; Pereira, M.P.; Gobbi, L.T.B. Does the impaired postural control in Parkinson’s disease affect the habituation to non-sequential external perturbation trials? Clin. Biomech. 2021, 85, 105363. [Google Scholar] [CrossRef]
- Carpenter, M.G.; Allum, J.H.J.; Honegger, F.; Adkin, A.L.; Bloem, B.R. Postural abnormalities to multidirectional stance perturbations in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2004, 75, 1245–1254. [Google Scholar] [CrossRef] [PubMed]
- Beretta, V.S.; Vitório, R.; Santos, P.C.R.D.; Orcioli-Silva, D.; Gobbi, L.T.B. Postural control after unexpected external perturbation: Effects of Parkinson’s disease subtype. Hum. Mov. Sci. 2019, 64, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Winter, D.A.; Patla, A.E.; Prince, F.; Ishac, M.; Gielo-Perczak, K. Stiffness control of balance in quiet standing. J. Neurophysiol. 1998, 80, 1211–1221. [Google Scholar] [CrossRef]
- Néstor, G.-J. Parkinson’s Disease. Neurobiol. Dis. 2007, 51–67. [Google Scholar] [CrossRef]
- Rocchi, L.; Chiari, L.; Mancini, M.; Carlson-Kuhta, P.; Gross, A.; Horak, F.B. Step initiation in Parkinson’s disease: Influence of initial stance conditions. Neurosci. Lett. 2006, 406, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Sigward, S.; Fisher, B.; Salem, G.J. Altered Dynamic Postural Control during Step Turning in Persons with Early-Stage Parkinson’s Disease. Parkinsons. Dis. 2012, 2012, 386962. [Google Scholar] [CrossRef]
- Heß, T.; Oehlwein, C.; Milani, T.L. Anticipatory Postural Adjustments and Compensatory Postural Responses to Multidirectional Perturbations—Effects of Medication and Subthalamic Nucleus Deep Brain Stimulation in Parkinson’s Disease. Brain Sci. 2023, 13, 454. [Google Scholar] [CrossRef]
- Błaszczyk, J.W.; Orawiec, R.; Duda-Kłodowska, D.; Opala, G. Assessment of postural instability in patients with Parkinson’s disease. Exp. Brain Res. 2007, 183, 107–114. [Google Scholar] [CrossRef] [PubMed]
- de La Casa-Fages, B.; Alonso-Frech, F.; Grandas, F. Effect of subthalamic nucleus deep brain stimulation on balance in Parkinson’s disease: A static posturographic analysis. Gait Posture 2017, 52, 374–380. [Google Scholar] [CrossRef]
- Mitchell, S.L.; Collins, J.J.; de Luca, C.J.; Burrows, A.; Lipsitz, L.A. Open-loop and closed-loop postural control mechanisms in Parkinson’s disease: Increased mediolateral activity during quiet standing. Neurosci. Lett. 1995, 197, 133–136. [Google Scholar] [CrossRef]
- Visser, J.E.; Oude Nijhuis, L.B.; Janssen, L.; Bastiaanse, C.M.; Borm, G.F.; Duysens, J.; Bloem, B.R. Dynamic posturography in Parkinson’s disease: Diagnostic utility of the “first trial effect”. Neuroscience 2010, 168, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Blenkinsop, G.M.; Pain, M.T.G.; Hiley, M.J. Balance control strategies during perturbed and unperturbed balance in standing and handstand. R. Soc. Open Sci. 2017, 4, 161018. [Google Scholar] [CrossRef]
- Horak, F.B.; Nashner, L.M.; Diener, H.C. Postural strategies associated with somatosensory and vestibular loss. Exp. Brain Res. 1990, 82, 167–177. [Google Scholar] [CrossRef] [PubMed]
- Doná, F.; Aquino, C.C.; Gazzola, J.M.; Borges, V.; Silva, S.; Ganança, F.F.; Caovilla, H.H.; Ferraz, H.B. Changes in postural control in patients with Parkinson’s disease: A posturographic study. Physiotherapy 2015, 102, 272–279. [Google Scholar] [CrossRef] [PubMed]
- Am Grimbergen, Y.; Munneke, M.; Bloem, B.R. Falls in Parkinson’s disease. Curr. Opin. Neurol. 2004, 17, 405–415. [Google Scholar] [CrossRef]
- Bosek, M.; Grzegorzewski, B.; Kowalczyk, A.; Lubiński, I. Degradation of postural control system as a consequence of Parkinson’s disease and ageing. Neurosci. Lett. 2005, 376, 215–220. [Google Scholar] [CrossRef]
- Crenna, P.; Carpinella, I.; Lopiano, L.; Marzegan, A.; Rabuffetti, M.; Rizzone, M.; Lanotte, M.; Ferrarin, M. Influence of basal ganglia on upper limb locomotor synergies. Evidence from deep brain stimulation and L-DOPA treatment in Parkinson’s disease. Brain 2008, 131, 3410–3420. [Google Scholar] [CrossRef]
- Shohamy, D.; Myers, C.E.; Onlaor, S.; Gluck, M.A. Role of the basal ganglia in category learning: How do patients with Parkinson’s disease learn? Behav. Neurosci. 2004, 118, 676–686. [Google Scholar] [CrossRef]
- Maschke, M.; Gomez, C.M.; Tuite, P.J.; Konczak, J. Dysfunction of the basal ganglia, but not the cerebellum, impairs kinaesthesia. Brain 2003, 126, 2312–2322. [Google Scholar] [CrossRef]
- Samadi, P.; Rouillard, C.; Bédard, P.J.; Di Paolo, T. Functional neurochemistry of the basal ganglia. In Parkinson’s Disease and Related Disorders, Part I; Elsevier: Amsterdam, The Netherlands, 2007; pp. 19–66. ISBN 9780444519009. [Google Scholar]
- Takakusaki, K. Functional Neuroanatomy for Posture and Gait Control. J. Mov. Disord. 2017, 10, 1–17. [Google Scholar] [CrossRef]
- Takakusaki, K. Neurophysiology of gait: From the spinal cord to the frontal lobe. Mov. Disord. 2013, 28, 1483–1491. [Google Scholar] [CrossRef]
- Bohnen, N.I.; Frey, K.A.; Studenski, S.; Kotagal, V.; Koeppe, R.A.; Scott, P.J.H.; Albin, R.L.; Müller, M.L.T.M. Gait speed in Parkinson disease correlates with cholinergic degeneration. Neurology 2013, 81, 1611–1616. [Google Scholar] [CrossRef] [PubMed]
- Perez-Lloret, S.; Barrantes, F.J. Deficits in cholinergic neurotransmission and their clinical correlates in Parkinson’s disease. NPJ Park. Dis. 2016, 2, 16001. [Google Scholar] [CrossRef] [PubMed]
- Rinne, J.O.; Ma, S.Y.; Lee, M.S.; Collan, Y.; Röyttä, M. Loss of cholinergic neurons in the pedunculopontine nucleus in Parkinson’s disease is related to disability of the patients. Park. Relat. Disord. 2008, 14, 553–557. [Google Scholar] [CrossRef] [PubMed]
- Karachi, C.; Grabli, D.; Bernard, F.A.; Tandé, D.; Wattiez, N.; Belaid, H.; Bardinet, E.; Prigent, A.; Nothacker, H.-P.; Hunot, S.; et al. Cholinergic mesencephalic neurons are involved in gait and postural disorders in Parkinson disease. J. Clin. Investig. 2010, 120, 2745–2754. [Google Scholar] [CrossRef]
- Bonnet, A.-M.; Loria, Y.; Saint-Hilaire, M.-H.; Lhermitte, F.; Agid, Y. Does long-term aggravation of Parkinson’s disease result from nondopaminergic lesions? Neurology 1987, 37, 1539. [Google Scholar] [CrossRef] [PubMed]
- Pahapill, P.A.; Lozano, A.M. The pedunculopontine nucleus and Parkinson’s disease. Brain 2000, 123 Pt 9, 1767–1783. [Google Scholar] [CrossRef] [PubMed]
- Zweig, R.M.; Jankel, W.R.; Hedreen, J.C.; Mayeux, R.; Price, D.L. The pedunculopontine nucleus in Parkinson’s disease. Ann. Neurol. 1989, 26, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, E.C.; Graybiel, A.M.; Duyckaerts, C.; Javoy-Agid, F. Neuronal loss in the pedunculopontine tegmental nucleus in Parkinson disease and in progressive supranuclear palsy. Proc. Natl. Acad. Sci. USA 1987, 84, 5976–5980. [Google Scholar] [CrossRef]
- Rochester, L.; Yarnall, A.J.; Baker, M.R.; David, R.V.; Lord, S.; Galna, B.; Burn, D.J. Cholinergic dysfunction contributes to gait disturbance in early Parkinson’s disease. Brain 2012, 135, 2779–2788. [Google Scholar] [CrossRef]
- Oz, F.; Yucekeya, B.; Huzmeli, I.; Yilmaz, A. Does subthalamic nucleus deep brain stimulation affect the static balance at different frequencies? Neurocirugía 2023, 34, 60–66. [Google Scholar] [CrossRef]
- Sato, K.; Hokari, Y.; Kitahara, E.; Izawa, N.; Hatori, K.; Honaga, K.; Oyama, G.; Hatano, T.; Iwamuro, H.; Umemura, A.; et al. Short-Term Motor Outcomes in Parkinson’s Disease after Subthalamic Nucleus Deep Brain Stimulation Combined with Post-Operative Rehabilitation: A Pre-Post Comparison Study. Park. Dis. 2022, 2022, 8448638. [Google Scholar] [CrossRef] [PubMed]
- Yin, Z.; Bai, Y.; Zou, L.; Zhang, X.; Wang, H.; Gao, D.; Qin, G.; Ma, R.; Zhang, K.; Meng, F.; et al. Balance response to levodopa predicts balance improvement after bilateral subthalamic nucleus deep brain stimulation in Parkinson’s disease. NPJ Park. Dis. 2021, 7, 47. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Liang, S.; Yu, Y.; Wang, Y.; Cheng, Y.; Yang, H.; Tong, X. Effect of Subthalamic Nucleus Deep Brain Stimulation (STN-DBS) on balance performance in Parkinson’s disease. PLoS ONE 2020, 15, e0238936. [Google Scholar] [CrossRef] [PubMed]
- Szlufik, S.; Kloda, M.; Friedman, A.; Potrzebowska, I.; Gregier, K.; Mandat, T.; Przybyszewski, A.; Dutkiewicz, J.; Figura, M.; Habela, P.; et al. The Neuromodulatory Impact of Subthalamic Nucleus Deep Brain Stimulation on Gait and Postural Instability in Parkinson’s Disease Patients: A Prospective Case Controlled Study. Front. Neurol. 2018, 9, 906. [Google Scholar] [CrossRef]
- Pötter-Nerger, M.; Volkmann, J. Deep brain stimulation for gait and postural symptoms in Parkinson’s disease. Mov. Disord. 2013, 28, 1609–1615. [Google Scholar] [CrossRef]
- Colnat-Coulbois, S. Bilateral subthalamic nucleus stimulation improves balance control in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2005, 76, 780–787. [Google Scholar] [CrossRef]
- St George, R.J.; Carlson-Kuhta, P.; Burchiel, K.J.; Hogarth, P.; Frank, N.; Horak, F.B. The effects of subthalamic and pallidal deep brain stimulation on postural responses in patients with Parkinson disease. J. Neurosurg. 2012, 116, 1347–1356. [Google Scholar] [CrossRef]
- Benabid, A.-L.; Koudsié, A.; Benazzouz, A.; Fraix, V.; Ashraf, A.; Le Bas, J.F.; Chabardes, S.; Pollak, P. Subthalamic Stimulation for Parkinson’s Disease. Arch. Med. Res. 2000, 31, 282–289. [Google Scholar] [CrossRef]
- Maurer, C.; Mergner, T.; Xie, J.; Faist, M.; Pollak, P.; Lucking, C.H. Effect of chronic bilateral subthalamic nucleus (STN) stimulation on postural control in Parkinson’s disease. Brain 2003, 126, 1146–1163. [Google Scholar] [CrossRef]
- McNeely, M.E.; Earhart, G.M. Medication and subthalamic nucleus deep brain stimulation similarly improve balance and complex gait in Parkinson disease. Park. Relat. Disord. 2013, 19, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Rocchi, L.; Carlson-Kuhta, P.; Chiari, L.; Burchiel, K.J.; Hogarth, P.; Horak, F.B. Effects of deep brain stimulation in the subthalamic nucleus or globus pallidus internus on step initiation in Parkinson disease: Laboratory investigation. J. Neurosurg. 2012, 117, 1141–1149. [Google Scholar] [CrossRef] [PubMed]
- Nieuwboer, A.; De Weerdt, W.; Dom, R.; Nuttin, B.; Peeraer, L.; Pattyn, A. Walking ability after implantation of a pallidal stimulator:analysis of plantar force distribution in patients with Parkinson’s disease. Park. Relat. Disord. 1998, 4, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Nantel, J.; McDonald, J.C.; Bronte-Stewart, H. Effect of medication and STN-DBS on postural control in subjects with Parkinson’s disease. Park. Relat. Disord. 2012, 18, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Krishnamurthi, N.; Mulligan, S.; Mahant, P.; Samanta, J.; Abbas, J.J. Deep brain stimulation amplitude alters posture shift velocity in Parkinson’s disease. Cogn. Neurodyn. 2012, 6, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Duncan, P.W.; Weiner, D.K.; Chandler, J.; Studenski, S. Functional reach: A new clinical measure of balance. J. Gerontol. 1990, 45, M192–M197. [Google Scholar] [CrossRef]
- Stack, E.; Ashburn, A.; Jupp, K. Postural instability during reaching tasks in Parkinson’s disease. Physiother. Res. Int. 2005, 10, 146–153. [Google Scholar] [CrossRef]
- Schieppati, M.; Hugon, M.; Grasso, M.; Nardone, A.; Galante, M. The limits of equilibrium in young and elderly normal subjects and in parkinsonians. Electroencephalogr. Clin. Neurophysiol./Evoked Potentials Sect. 1994, 93, 286–298. [Google Scholar] [CrossRef]
- Behrman, A.L.; Light, K.E.; Flynn, S.M.; Thigpen, M.T. Is the functional reach test useful for identifying falls risk among individuals with Parkinson’s disease? Arch. Phys. Med. Rehabil. 2002, 83, 538–542. [Google Scholar] [CrossRef]
- Kelly, V.E.; Hyngstrom, A.S.; Rundle, M.M.; Bastian, A.J. Interaction of levodopa and cues on voluntary reaching in Parkinson’s disease. Mov. Disord. 2002, 17, 38–44. [Google Scholar] [CrossRef]
- Li, H.; Liang, S.; Yu, Y.; Wang, Y.; Cheng, Y.; Yang, H.; Tong, X. Clinical experience of comprehensive treatment on the balance function of Parkinson’s disease. Medicine 2020, 99, e20154. [Google Scholar] [CrossRef] [PubMed]
- St George, R.J.; Carlson-Kuhta, P.; Nutt, J.G.; Hogarth, P.; Burchiel, K.J.; Horak, F.B. The effect of deep brain stimulation randomized by site on balance in Parkinson’s disease. Mov. Disord. 2014, 29, 949–953. [Google Scholar] [CrossRef] [PubMed]
- Schulz-Schaeffer, W.J.; Margraf, N.G.; Munser, S.; Wrede, A.; Buhmann, C.; Deuschl, G.; Oehlwein, C. Effect of neurostimulation on camptocormia in Parkinson’s disease depends on symptom duration. Mov. Disord. 2015, 30, 368–372. [Google Scholar] [CrossRef] [PubMed]
- Gamborg, M.; Hvid, L.G.; Thrue, C.; Johansson, S.; Franzén, E.; Dalgas, U.; Langeskov-Christensen, M. Muscle Strength and Power in People with Parkinson Disease: A Systematic Review and Meta-analysis. J. Neurol. Phys. Ther. 2023, 47, 3–15. [Google Scholar] [CrossRef]
- Wolke, R.; Kuhtz-Buschbeck, J.P.; Deuschl, G.; Margraf, N.G. Insufficiency of trunk extension and impaired control of muscle force in Parkinson’s disease with camptocormia. Clin. Neurophysiol. 2020, 131, 2621–2629. [Google Scholar] [CrossRef]
- Santos, M.J.; Kanekar, N.; Aruin, A.S. The role of anticipatory postural adjustments in compensatory control of posture: 1. Electromyographic analysis. J. Electromyogr. Kinesiol. 2010, 20, 388–397. [Google Scholar] [CrossRef]
- Rougier, P.; Burdet, C.; Farenc, I.; Berger, L. Backward and forward leaning postures modelled by an fBm framework. Neurosci. Res. 2001, 41, 41–50. [Google Scholar] [CrossRef]
- Artieda, J.; Pastor, M.A.; Lacruz, F.; Obeso, J.A. Temporal discrimination is abnormal in Parkinson’s disease. Brain 1992, 115 Pt 1, 199–210. [Google Scholar] [CrossRef]
- Bernardinis, M.; Atashzar, S.F.; Jog, M.S.; Patel, R.V. Differential Temporal Perception Abilities in Parkinson’s Disease Patients Based on Timing Magnitude. Sci. Rep. 2019, 9, 19638. [Google Scholar] [CrossRef]
- Vaugoyeau, M.; Hakam, H.; Azulay, J.-P. Proprioceptive impairment and postural orientation control in Parkinson’s disease. Hum. Mov. Sci. 2011, 30, 405–414. [Google Scholar] [CrossRef]
- Pearson, K.G. Proprioceptive regulation of locomotion. Curr. Opin. Neurobiol. 1995, 5, 786–791. [Google Scholar] [CrossRef]
- Jacobs, J.V.; Horak, F.B. Abnormal proprioceptive-motor integration contributes to hypometric postural responses of subjects with Parkinson’s disease. Neuroscience 2006, 141, 999–1009. [Google Scholar] [CrossRef] [PubMed]
- Konczak, J.; Corcos, D.M.; Horak, F.; Poizner, H.; Shapiro, M.; Tuite, P.; Volkmann, J.; Maschke, M. Proprioception and Motor Control in Parkinson’s Disease. J. Mot. Behav. 2009, 41, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Henderson, J.M.; Watson, S.; Halliday, G.M.; Heinemann, T.; Gerlach, M. Relationships between various behavioural abnormalities and nigrostriatal dopamine depletion in the unilateral 6-OHDA-lesioned rat. Behav. Brain Res. 2003, 139, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Franchignoni, F.; Martignoni, E.; Ferriero, G.; Pasetti, C. Balance and fear of falling in Parkinson’s disease. Park. Relat. Disord. 2005, 11, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Hariz, M.; Blomstedt, P. Deep brain stimulation for Parkinson’s disease. J. Intern. Med. 2022, 292, 764–778. [Google Scholar] [CrossRef]
- Agnesi, F.; Johnson, M.D.; Vitek, J.L. Deep brain stimulation: How does it work? Handb. Clin. Neurol. 2013, 116, 39–54. [Google Scholar] [CrossRef]
- Groiss, S.J.; Wojtecki, L.; Südmeyer, M.; Schnitzler, A. Deep brain stimulation in Parkinson’s disease. Ther. Adv. Neurol. Disord. 2009, 2, 20–28. [Google Scholar] [CrossRef]
- Perlmutter, J.S.; Mink, J.W. Deep brain stimulation. Annu. Rev. Neurosci. 2006, 29, 229–257. [Google Scholar] [CrossRef]
- Bloem, B.R.; Beckley, D.J.; van Dijk, J.G.; Zwinderman, A.H.; Remler, M.P.; Roos, R.A. Influence of dopaminergic medication on automatic postural responses and balance impairment in Parkinson’s disease. Mov. Disord. 1996, 11, 509–521. [Google Scholar] [CrossRef]
- Goetz, C.G.; Poewe, W.; Rascol, O.; Sampaio, C. Evidence-based medical review update: Pharmacological and surgical treatments of Parkinson’s disease: 2001 to 2004. Mov. Disord. 2005, 20, 523–539. [Google Scholar] [CrossRef]
- Bejjani, B.P.; Gervais, D.; Arnulf, I.; Papadopoulos, S.; Demeret, S.; Bonnet, A.M.; Cornu, P.; Damier, P.; Agid, Y. Axial parkinsonian symptoms can be improved: The role of levodopa and bilateral subthalamic stimulation. J. Neurol. Neurosurg. Psychiatry 2000, 68, 595–600. [Google Scholar] [CrossRef]
- Lubik, S.; Fogel, W.; Tronnier, V.; Krause, M.; König, J.; Jost, W.H. Gait analysis in patients with advanced Parkinson disease: Different or additive effects on gait induced by levodopa and chronic STN stimulation. J. Neural Transm. 2006, 113, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Yamada, K.; Goto, S.; Hamasaki, T.; Kuratsu, J.-I. Effect of bilateral subthalamic nucleus stimulation on levodopa-unresponsive axial symptoms in Parkinson’s disease. Acta Neurochir. 2008, 150, discussion 22. [Google Scholar] [CrossRef]
- Benabid, A.L. Deep brain stimulation for Parkinson’s disease. Curr. Opin. Neurobiol. 2003, 13, 696–706. [Google Scholar] [CrossRef] [PubMed]
- Krack, P.; Batir, A.; van Blercom, N.; Chabardes, S.; Fraix, V.; Ardouin, C.; Koudsie, A.; Limousin, P.D.; Benazzouz, A.; LeBas, J.F.; et al. Five-year follow-up of bilateral stimulation of the subthalamic nucleus in advanced Parkinson’s disease. N. Engl. J. Med. 2003, 349, 1925–1934. [Google Scholar] [CrossRef] [PubMed]
- Faist, M. Effect of bilateral subthalamic nucleus stimulation on gait in Parkinson’s disease. Brain 2001, 124, 1590–1600. [Google Scholar] [CrossRef]
- Zanardi, A.P.J.; da Silva, E.S.; Costa, R.R.; Passos-Monteiro, E.; Dos Santos, I.O.; Kruel, L.F.M.; Peyré-Tartaruga, L.A. Gait parameters of Parkinson’s disease compared with healthy controls: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 752. [Google Scholar] [CrossRef]
- Roper, J.A.; Kang, N.; Ben, J.; Cauraugh, J.H.; Okun, M.S.; Hass, C.J. Deep brain stimulation improves gait velocity in Parkinson’s disease: A systematic review and meta-analysis. J. Neurol. 2016, 263, 1195–1203. [Google Scholar] [CrossRef]
- Grabli, D.; Karachi, C.; Welter, M.-L.; Lau, B.; Hirsch, E.C.; Vidailhet, M.; François, C. Normal and pathological gait: What we learn from Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2012, 83, 979–985. [Google Scholar] [CrossRef]
- Stolze, H.; Klebe, S.; Poepping, M.; Lorenz, D.; Herzog, J.; Hamel, W.; Schrader, B.; Raethjen, J.; Wenzelburger, R.; Mehdorn, H.M.; et al. Effects of bilateral subthalamic nucleus stimulation on parkinsonian gait. Neurology 2001, 57, 144–146. [Google Scholar] [CrossRef] [PubMed]
- Stolze, H.; Kuhtz-Buschbeck, J.P.; Drücke, H.; Jöhnk, K.; Illert, M.; Deuschl, G. Comparative analysis of the gait disorder of normal pressure hydrocephalus and Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2001, 70, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Charlett, A.; Weller, C.; Purkiss, A.G.; Dobbs, S.M.; Dobbs, R.J. Breadth of base whilst walking: Effect of ageing and parkinsonism. Age Ageing 1998, 27, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Kirollos, C.; Charlett, A.; O’Neill, C.J.; Kosik, R.; Mozol, K.; Purkiss, A.G.; Bowes, S.G.; Nicholson, P.W.; Hunt, W.B.; Weller, C.; et al. Objective measurement of activation of rigidity: Diagnostic, pathogenetic and therapeutic implications in parkinsonism. Br. J. Clin. Pharmacol. 1996, 41, 557–564. [Google Scholar] [CrossRef]
- Bovonsunthonchai, S.; Vachalathiti, R.; Pisarnpong, A.; Khobhun, F.; Hiengkaew, V. Spatiotemporal gait parameters for patients with Parkinson’s disease compared with normal individuals. Physiother. Res. Int. 2014, 19, 158–165. [Google Scholar] [CrossRef]
- Brinkerhoff, S.A.; Murrah, W.M.; Roper, J.A. All Known Cemeteries of Clayton County, Georgia; Ancestors Unlimited: Jonesboro, Georgia, 1986; ISBN 0123456789. [Google Scholar]
- Bugalho, P.; Alves, L.; Miguel, R. Gait dysfunction in Parkinson’s disease and normal pressure hydrocephalus: A comparative study. J. Neural Transm. 2013, 120, 1201–1207. [Google Scholar] [CrossRef]
- Weller, C.; Humphrey, S.J.; Kirollos, C.; Bowes, S.G.; Charlett, A.; Dobbs, S.M.; Dobbs, R.J. Gait on a shoestring: Falls and foot separation in parkinsonism. Age Ageing 1992, 21, 242–244. [Google Scholar] [CrossRef]
- Johnsen, E.L.; Sunde, N.; Mogensen, P.H.; Ostergaard, K. MRI verified STN stimulation site–gait improvement and clinical outcome. Eur. J. Neurol. 2010, 17, 746–753. [Google Scholar] [CrossRef]
- Navratilova, D.; Krobot, A.; Otruba, P.; Nevrly, M.; Krahulik, D.; Kolar, P.; Kolarova, B.; Kaiserova, M.; Mensikova, K.; Vastik, M.; et al. Deep Brain Stimulation Effects on Gait Pattern in Advanced Parkinson’s Disease Patients. Front. Neurosci. 2020, 14, 814. [Google Scholar] [CrossRef]
- Johnsen, E.L.; Mogensen, P.H.; Sunde, N.A.; Ostergaard, K. Improved asymmetry of gait in Parkinson’s disease with DBS: Gait and postural instability in Parkinson’s disease treated with bilateral deep brain stimulation in the subthalamic nucleus. Mov. Disord. 2009, 24, 588–595. [Google Scholar] [CrossRef]
- Peppe, A.; Chiavalon, C.; Pasqualetti, P.; Crovato, D.; Caltagirone, C. Does gait analysis quantify motor rehabilitation efficacy in Parkinson’s disease patients? Gait Posture 2007, 26, 452–462. [Google Scholar] [CrossRef]
- Allen, N.E.; Canning, C.G.; Sherrington, C.; Fung, V.S.C. Bradykinesia, muscle weakness and reduced muscle power in Parkinson’s disease. Mov. Disord. 2009, 24, 1344–1351. [Google Scholar] [CrossRef]
- Bloem, B.R.; Grimbergen, Y.A.M.; Cramer, M.; Willemsen, M.; Zwinderman, A.H. Prospective assessment of falls in Parkinson’s disease. J. Neurol. 2001, 248, 950–958. [Google Scholar] [CrossRef]
- St George, R.J.; Nutt, J.G.; Burchiel, K.J.; Horak, F.B. A meta-regression of the long-term effects of deep brain stimulation on balance and gait in PD. Neurology 2010, 75, 1292–1299. [Google Scholar] [CrossRef]
- van Nuenen, B.F.L.; Esselink, R.A.J.; Munneke, M.; Speelman, J.D.; van Laar, T.; Bloem, B.R. Postoperative gait deterioration after bilateral subthalamic nucleus stimulation in Parkinson’s disease. Mov. Disord. 2008, 23, 2404–2406. [Google Scholar] [CrossRef] [PubMed]
- Lewek, M.D.; Poole, R.; Johnson, J.; Halawa, O.; Huang, X. Arm swing magnitude and asymmetry during gait in the early stages of Parkinson’s disease. Gait Posture 2010, 31, 256–260. [Google Scholar] [CrossRef]
- Adkin, A.L.; Frank, J.S.; Jog, M.S. Fear of falling and postural control in Parkinson’s disease. Mov. Disord. 2003, 18, 496–502. [Google Scholar] [CrossRef] [PubMed]
- Cakit, B.D.; Saracoglu, M.; Genc, H.; Erdem, H.R.; Inan, L. The effects of incremental speed-dependent treadmill training on postural instability and fear of falling in Parkinson’s disease. Clin. Rehabil. 2007, 21, 698–705. [Google Scholar] [CrossRef] [PubMed]
- Bohnen, N.I.; Müller, M.L.; Kotagal, V.; Koeppe, R.A.; Kilbourn, M.R.; Gilman, S.; Albin, R.L.; Frey, K.A. Heterogeneity of cholinergic denervation in Parkinson’s disease without dementia. J. Cereb. Blood Flow Metab. 2012, 32, 1609–1617. [Google Scholar] [CrossRef] [PubMed]
- Malouin, F.; Richards, C.L.; Jackson, P.L.; Dumas, F.; Doyon, J. Brain activations during motor imagery of locomotor-related tasks: A PET study. Hum. Brain Mapp. 2003, 19, 47–62. [Google Scholar] [CrossRef]
- Jahn, K.; Deutschländer, A.; Stephan, T.; Strupp, M.; Wiesmann, M.; Brandt, T. Brain activation patterns during imagined stance and locomotion in functional magnetic resonance imaging. Neuroimage 2004, 22, 1722–1731. [Google Scholar] [CrossRef]
- Weinberger, M.; Hamani, C.; Hutchison, W.D.; Moro, E.; Lozano, A.M.; Dostrovsky, J.O. Pedunculopontine nucleus microelectrode recordings in movement disorder patients. Exp. Brain Res. 2008, 188, 165–174. [Google Scholar] [CrossRef]
- Lozano, A.M.; Snyder, B.J. Deep brain stimulation for parkinsonian gait disorders. J. Neurol. 2008, 255 (Suppl. 4), 30–31. [Google Scholar] [CrossRef]
- Cossu, G.; Pau, M. Subthalamic nucleus stimulation and gait in Parkinson’s Disease: A not always fruitful relationship. Gait Posture 2017, 52, 205–210. [Google Scholar] [CrossRef]
- Morris, M.E.; Iansek, R.; Matyas, T.A.; Summers, J.J. The pathogenesis of gait hypokinesia in Parkinson’s disease. Brain 1994, 117 Pt 5, 1169–1181. [Google Scholar] [CrossRef]
- Morris, M.E.; Iansek, R.; Matyas, T.A.; Summers, J.J. Ability to modulate walking cadence remains intact in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 1994, 57, 1532–1534. [Google Scholar] [CrossRef]
- Wu, T.; Hallett, M. A functional MRI study of automatic movements in patients with Parkinson’s disease. Brain 2005, 128, 2250–2259. [Google Scholar] [CrossRef]
- Bloem, B.R.; Grimbergen, Y.A.M.; van Dijk, J.G.; Munneke, M. The “posture second” strategy: A review of wrong priorities in Parkinson’s disease. J. Neurol. Sci. 2006, 248, 196–204. [Google Scholar] [CrossRef]
- Morris, M.E.; Iansek, R.; Matyas, T.A.; Summers, J.J. Stride length regulation in Parkinson’s disease. Normalization strategies and underlying mechanisms. Brain 1996, 119 Pt 2, 551–568. [Google Scholar] [CrossRef]
- Aziz, T.Z.; Davies, L.; Stein, J.; France, S. The role of descending basal ganglia connections to the brain stem in parkinsonian akinesia. Br. J. Neurosurg. 1998, 12, 245–249. [Google Scholar] [CrossRef]
- Brozova, H.; Barnaure, I.; Ruzicka, E.; Stochl, J.; Alterman, R.; Tagliati, M. Short- and Long-Term Effects of DBS on Gait in Parkinson’s Disease. Front. Neurol. 2021, 12, 688760. [Google Scholar] [CrossRef] [PubMed]
- Vallabhajosula, S.; Haq, I.U.; Hwynn, N.; Oyama, G.; Okun, M.; Tillman, M.D.; Hass, C.J. Low-frequency Versus High-frequency Subthalamic Nucleus Deep Brain Stimulation on Postural Control and Gait in Parkinson’s Disease: A Quantitative Study. Brain Stimul. 2015, 8, 64–75. [Google Scholar] [CrossRef] [PubMed]
- Mera, T.O.; Filipkowski, D.E.; Riley, D.E.; Whitney, C.M.; Walter, B.L.; Gunzler, S.A.; Giuffrida, J.P. Quantitative analysis of gait and balance response to deep brain stimulation in Parkinson’s disease. Gait Posture 2013, 38, 109–114. [Google Scholar] [CrossRef]
- Brozova, H.; Barnaure, I.; Alterman, R.L.; Tagliati, M. STN-DBS frequency effects on freezing of gait in advanced Parkinson disease. Neurology 2009, 72, 770, author reply 770-1. [Google Scholar] [CrossRef] [PubMed]
- Hausdorff, J.M.; Gruendlinger, L.; Scollins, L.; O’Herron, S.; Tarsy, D. Deep brain stimulation effects on gait variability in Parkinson’s disease. Mov. Disord. 2009, 24, 1688–1692. [Google Scholar] [CrossRef] [PubMed]
- Crenna, P.; Carpinella, I.; Rabuffetti, M.; Rizzone, M.; Lopiano, L.; Lanotte, M.; Ferrarin, M. Impact of subthalamic nucleus stimulation on the initiation of gait in Parkinson’s disease. Exp. Brain Res. 2006, 172, 519–532. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.T.; Dilda, V.; Hakim, B.; MacDougall, H.G. Validation of 24-hour ambulatory gait assessment in Parkinson’s disease with simultaneous video observation. Biomed. Eng. Online 2011, 10, 82. [Google Scholar] [CrossRef]
- Peppe, A.; Pierantozzi, M.; Chiavalon, C.; Marchetti, F.; Caltagirone, C.; Musicco, M.; Stanzione, P.; Stefani, A. Deep brain stimulation of the pedunculopontine tegmentum and subthalamic nucleus: Effects on gait in Parkinson’s disease. Gait Posture 2010, 32, 512–518. [Google Scholar] [CrossRef]
- Xie, J.; Krack, P.; Benabid, A.L.; Pollak, P. Effect of bilateral subthalamic nucleus stimulation on parkinsonian gait. J. Neurol. 2001, 248, 1068–1072. [Google Scholar] [CrossRef]
- Ferrarin, M.; Rizzone, M.; Lopiano, L.; Recalcati, M.; Pedotti, A. Effects of subthalamic nucleus stimulation and l-dopa in trunk kinematics of patients with Parkinson’s disease. Gait Posture 2004, 19, 164–171. [Google Scholar] [CrossRef]
- Ferrarin, M.; Rizzone, M.; Bergamasco, B.; Lanotte, M.; Recalcati, M.; Pedotti, A.; Lopiano, L. Effects of bilateral subthalamic stimulation on gait kinematics and kinetics in Parkinson?: S disease. Exp. Brain Res. 2005, 160, 517–527. [Google Scholar] [CrossRef] [PubMed]
- Bleuse, S.; Delval, A.; Blatt, J.L.; Derambure, P.; Destée, A.; Defebvre, L. Effect of bilateral subthalamic nucleus deep brain stimulation on postural adjustments during arm movement. Clin. Neurophysiol. 2011, 122, 2032–2035. [Google Scholar] [CrossRef] [PubMed]
- Carpinella, I.; Crenna, P.; Marzegan, A.; Rabuffetti, M.; Rizzone, M.; Lopiano, L.; Ferrarin, M. Effect of L-dopa and subthalamic nucleus stimulation on arm and leg swing during gait in Parkinson’s Disease. In Proceedings of the 2007 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 22–26 August 2007; Volume 2007, pp. 6665–6668. [Google Scholar] [CrossRef]
- St George, R.J.; Carlson-Kuhta, P.; King, L.A.; Burchiel, K.J.; Horak, F.B. Compensatory stepping in Parkinson’s disease is still a problem after deep brain stimulation randomized to STN or GPi. J. Neurophysiol. 2015, 114, 1417–1423. [Google Scholar] [CrossRef] [PubMed]
- Weaver, F.M.; Follett, K.A.; Stern, M.; Luo, P.; Harris, C.L.; Hur, K.; Marks, W.J.; Rothlind, J.; Sagher, O.; Moy, C.; et al. Randomized trial of deep brain stimulation for Parkinson disease: Thirty-six-month outcomes. Neurology 2012, 79, 55–65. [Google Scholar] [CrossRef] [PubMed]
- Rizzone, M.; Ferrarin, M.; Pedotti, A.; Bergamasco, B.; Bosticco, E.; Lanotte, M.; Perozzo, P.; Tavella, A.; Torre, E.; Recalcati, M.; et al. High-frequency electrical stimulation of the subthalamic nucleus in Parkinson’s disease: Kinetic and kinematic gait analysis. Neurol. Sci. 2002, 23 (Suppl. 2), S103–S104. [Google Scholar] [CrossRef]
- Krystkowiak, P.; Blatt, J.-L.; Bourriez, J.-L.; Duhamel, A.; Perina, M.; Blond, S.; Guieu, J.-D.; Destée, A.; Defebvre, L. Effects of Subthalamic Nucleus Stimulation and Levodopa Treatment on Gait Abnormalities in Parkinson Disease. Arch. Neurol. 2003, 60, 80–84. [Google Scholar] [CrossRef]
- Moreau, C.; Defebvre, L.; Destée, A.; Bleuse, S.; Clement, F.; Blatt, J.L.; Krystkowiak, P.; Devos, D. STN-DBS frequency effects on freezing of gait in advanced Parkinson disease. Neurology 2008, 71, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Wagle Shukla, A.; Moro, E.; Gunraj, C.; Lozano, A.; Hodaie, M.; Lang, A.; Chen, R. Long-term subthalamic nucleus stimulation improves sensorimotor integration and proprioception. J. Neurol. Neurosurg. Psychiatry 2013, 84, 1020–1028. [Google Scholar] [CrossRef]
- Sailer, A.; Molnar, G.F.; Paradiso, G.; Gunraj, C.A.; Lang, A.E.; Chen, R. Short and long latency afferent inhibition in Parkinson’s disease. Brain 2003, 126, 1883–1894. [Google Scholar] [CrossRef]
- Knight, E.J.; Testini, P.; Min, H.-K.; Gibson, W.S.; Gorny, K.R.; Favazza, C.P.; Felmlee, J.P.; Kim, I.; Welker, K.M.; Clayton, D.A.; et al. Motor and Nonmotor Circuitry Activation Induced by Subthalamic Nucleus Deep Brain Stimulation in Patients with Parkinson Disease: Intraoperative Functional Magnetic Resonance Imaging for Deep Brain Stimulation. Mayo Clin. Proc. 2015, 90, 773–785. [Google Scholar] [CrossRef]
- Vitek, J.L. Deep brain stimulation: How does it work? Cleve. Clin. J. Med. 2008, 75 (Suppl. 2), S59–S65. [Google Scholar] [CrossRef] [PubMed]
- Hamel, W.; Fietzek, U.; Morsnowski, A.; Schrader, B.; Herzog, J.; Weinert, D.; Pfister, G.; Müller, D.; Volkmann, J.; Deuschl, G.; et al. Deep brain stimulation of the subthalamic nucleus in Parkinson’s disease: Evaluation of active electrode contacts. J. Neurol. Neurosurg. Psychiatry 2003, 74, 1036–1046. [Google Scholar] [CrossRef]
- Vitek, J.L. Mechanisms of deep brain stimulation: Excitation or inhibition. Mov Disord. 2002, 17, S69–S72. [Google Scholar] [CrossRef]
- Santaniello, S.; McCarthy, M.M.; Montgomery, E.B.; Gale, J.T.; Kopell, N.; Sarma, S.V. Therapeutic mechanisms of high-frequency stimulation in Parkinson’s disease and neural restoration via loop-based reinforcement. Proc. Natl. Acad. Sci. USA 2015, 112, E586–E595. [Google Scholar] [CrossRef] [PubMed]
- Shine, J.M.; Matar, E.; Ward, P.B.; Bolitho, S.J.; Gilat, M.; Pearson, M.; Naismith, S.L.; Lewis, S.J.G. Exploring the cortical and subcortical functional magnetic resonance imaging changes associated with freezing in Parkinson’s disease. Brain 2013, 136, 1204–1215. [Google Scholar] [CrossRef] [PubMed]
- Deniau, J.-M.; Degos, B.; Bosch, C.; Maurice, N. Deep brain stimulation mechanisms: Beyond the concept of local functional inhibition. Eur. J. Neurosci. 2010, 32, 1080–1091. [Google Scholar] [CrossRef]
- Arai, N.; Yokochi, F.; Ohnishi, T.; Momose, T.; Okiyama, R.; Taniguchi, M.; Takahashi, H.; Matsuda, H.; Ugawa, Y. Mechanisms of unilateral STN-DBS in patients with Parkinson’s disease: A PET study. J. Neurol. 2008, 255, 1236–1243. [Google Scholar] [CrossRef] [PubMed]
- Geday, J.; Østergaard, K.; Johnsen, E.; Gjedde, A. STN-stimulation in Parkinson’s disease restores striatal inhibition of thalamocortical projection. Hum. Brain Mapp. 2009, 30, 112–121. [Google Scholar] [CrossRef]
- Stefani, A.; Lozano, A.M.; Peppe, A.; Stanzione, P.; Galati, S.; Tropepi, D.; Pierantozzi, M.; Brusa, L.; Scarnati, E.; Mazzone, P. Bilateral deep brain stimulation of the pedunculopontine and subthalamic nuclei in severe Parkinson’s disease. Brain 2007, 130, 1596–1607. [Google Scholar] [CrossRef]
- Florio, T.; Scarnati, E.; Confalone, G.; Minchella, D.; Galati, S.; Stanzione, P.; Stefani, A.; Mazzone, P. High-frequency stimulation of the subthalamic nucleus modulates the activity of pedunculopontine neurons through direct activation of excitatory fibres as well as through indirect activation of inhibitory pallidal fibres in the rat. Eur. J. Neurosci. 2007, 25, 1174–1186. [Google Scholar] [CrossRef]
- Hanakawa, T.; Katsumi, Y.; Fukuyama, H.; Honda, M.; Hayashi, T.; Kimura, J.; Shibasaki, H. Mechanisms underlying gait disturbance in Parkinson’s disease: A single photon emission computed tomography study. Brain 1999, 122 Pt 7, 1271–1282. [Google Scholar] [CrossRef]
- Limousin, P.; Greene, J.; Pollak, P.; Rothwell, J.; Benabid, A.L.; Frackowiak, R. Changes in cerebral activity pattern due to subthalamic nucleus or internal pallidum stimulation in Parkinson’s disease. Ann. Neurol. 1997, 42, 283–291. [Google Scholar] [CrossRef]
- Di Biase, L.; Pecoraro, P.M.; Carbone, S.P.; Caminiti, M.L.; Di Lazzaro, V. Levodopa-Induced Dyskinesias in Parkinson’s Disease: An Overview on Pathophysiology, Clinical Manifestations, Therapy Management Strategies and Future Directions. J. Clin. Med. 2023, 12, 4427. [Google Scholar] [CrossRef]
- Rizzone, M.G.; Fasano, A.; Daniele, A.; Zibetti, M.; Merola, A.; Rizzi, L.; Piano, C.; Piccininni, C.; Romito, L.M.; Lopiano, L.; et al. Long-term outcome of subthalamic nucleus DBS in Parkinson’s disease: From the advanced phase towards the late stage of the disease? Park. Relat. Disord. 2014, 20, 376–381. [Google Scholar] [CrossRef]
- Kerr, G.K.; Worringham, C.J.; Cole, M.H.; Lacherez, P.F.; Wood, J.M.; Silburn, P.A. Predictors of future falls in Parkinson disease. Neurology 2010, 75, 116–124. [Google Scholar] [CrossRef]
- Dickson, D.W.; Uchikado, H.; Fujishiro, H.; Tsuboi, Y. Evidence in favor of Braak staging of Parkinson’s disease. Mov. Disord. 2010, 25 (Suppl. 1), S78–S82. [Google Scholar] [CrossRef]
- Kingsbury, A.E.; Bandopadhyay, R.; Silveira-Moriyama, L.; Ayling, H.; Kallis, C.; Sterlacci, W.; Maeir, H.; Poewe, W.; Lees, A.J. Brain stem pathology in Parkinson’s disease: An evaluation of the Braak staging model. Mov. Disord. 2010, 25, 2508–2515. [Google Scholar] [CrossRef]
- Wolters, E.C.; Braak, H. Parkinson’s disease: Premotor clinico-pathological correlations. In Parkinson’s Disease and Related Disorders; Springer: Berlin/Heidelberg, Germany, 2006; pp. 309–319. [Google Scholar] [CrossRef]
- Nakanishi, T.; Tamaki, M.; Mizusawa, H.; Akatsuka, T.; Kinoshita, T. An experimental study for analyzing nerve conduction velocity. Electroencephalogr. Clin. Neurophysiol. 1986, 63, 484–487. [Google Scholar] [CrossRef]
- Rodriguez-Oroz, M.C.; Rodriguez, M.; Guridi, J.; Mewes, K.; Chockkman, V.; Vitek, J.; DeLong, M.R.; Obeso, J.A. The subthalamic nucleus in Parkinson’s disease: Somatotopic organization and physiological characteristics. Brain 2001, 124, 1777–1790. [Google Scholar] [CrossRef]
- Romanelli, P.; Bronte-Stewart, H.; Heit, G.; Schaal, D.W.; Esposito, V. The functional organization of the sensorimotor region of the subthalamic nucleus. Stereotact. Funct. Neurosurg. 2004, 82, 222–229. [Google Scholar] [CrossRef]
- Calvert, G.A.; Thesen, T. Multisensory integration: Methodological approaches and emerging principles in the human brain. J. Physiol. Paris 2004, 98, 191–205. [Google Scholar] [CrossRef]
- Kühn, A.A.; Kupsch, A.; Schneider, G.-H.; Brown, P. Reduction in subthalamic 8–35 Hz oscillatory activity correlates with clinical improvement in Parkinson’s disease. Eur. J. Neurosci. 2006, 23, 1956–1960. [Google Scholar] [CrossRef]
- Kühn, A.A.; Williams, D.; Kupsch, A.; Limousin, P.; Hariz, M.; Schneider, G.-H.; Yarrow, K.; Brown, P. Event-related beta desynchronization in human subthalamic nucleus correlates with motor performance. Brain 2004, 127, 735–746. [Google Scholar] [CrossRef]
- Braak, H.; Del Tredici, K.; Bratzke, H.; Hamm-Clement, J.; Sandmann-Keil, D.; Rüb, U. Staging of the intracerebral inclusion body pathology associated with idiopathic Parkinson’s disease (preclinical and clinical stages). J. Neurol. 2002, 249 (Suppl. 3), iii1–iii5. [Google Scholar] [CrossRef]
- Riederer, P.; Sian-Hülsmann, J. The significance of neuronal lateralisation in Parkinson’s disease. J. Neural Transm. 2012, 119, 953–962. [Google Scholar] [CrossRef]
- Silverdale, M.A.; Kobylecki, C.; Kass-Iliyya, L.; Martinez-Martin, P.; Lawton, M.; Cotterill, S.; Chaudhuri, K.R.; Morris, H.; Baig, F.; Williams, N.; et al. A detailed clinical study of pain in 1957 participants with early/moderate Parkinson’s disease. Park. Relat. Disord. 2018, 56, 27–32. [Google Scholar] [CrossRef]
- O’Suilleabhain, P.; Bullard, J.; Dewey, R.B. Proprioception in Parkinson’s disease is acutely depressed by dopaminergic medications. J. Neurol. Neurosurg. Psychiatry 2001, 71, 607–610. [Google Scholar] [CrossRef]
- Mancini, F.; Comi, C.; Oggioni, G.D.; Pacchetti, C.; Calandrella, D.; Moja, M.C.; Riboldazzi, G.; Tunesi, S.; Fante, M.D.; Manfredi, L.; et al. Prevalence and features of peripheral neuropathy in Parkinson’s disease patients under different therapeutic regimens. Park. Relat. Disord. 2014, 20, 27–31. [Google Scholar] [CrossRef]
- Dellapina, E.; Ory-Magne, F.; Regragui, W.; Thalamas, C.; Lazorthes, Y.; Rascol, O.; Payoux, P.; Brefel-Courbon, C. Effect of subthalamic deep brain stimulation on pain in Parkinson’s disease. Pain 2012, 153, 2267–2273. [Google Scholar] [CrossRef]
- Maschke, M.; Tuite, P.J.; Pickett, K.; Wächter, T.; Konczak, J. The effect of subthalamic nucleus stimulation on kinaesthesia in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2005, 76, 569–571. [Google Scholar] [CrossRef]
- Ortega-Cubero, S.; Clavero, P.; Irurzun, C.; Gonzalez-Redondo, R.; Guridi, J.; Obeso, J.A.; Rodriguez-Oroz, M.C. Effect of deep brain stimulation of the subthalamic nucleus on non-motor fluctuations in Parkinson’s disease: Two-year’ follow-up. Park. Relat. Disord. 2013, 19, 543–547. [Google Scholar] [CrossRef]
- Reich, M.M.; Ray Chaudhuri, K.; Ashkan, K.; Hulse, N.; Costello, A.; Moriarty, J.; Samuel, M. Changes in the non-motor symptom scale in Parkinson’s disease after deep brain stimulation. Basal Ganglia 2011, 1, 131–133. [Google Scholar] [CrossRef]
- Witjas, T.; Kaphan, E.; Régis, J.; Jouve, E.; Chérif, A.A.; Péragut, J.-C.; Azulay, J.P. Effects of chronic subthalamic stimulation on nonmotor fluctuations in Parkinson’s disease. Mov. Disord. 2007, 22, 1729–1734. [Google Scholar] [CrossRef]
- Taktakishvili, O.; Sivan-Loukianova, E.; Kultas-Ilinsky, K.; Ilinsky, I.A. Posterior parietal cortex projections to the ventral lateral and some association thalamic nuclei in Macaca mulatta. Brain Res. Bull. 2002, 59, 135–150. [Google Scholar] [CrossRef]
- Davis, K.D.; Kwan, C.L.; Crawley, A.P.; Mikulis, D.J. Functional MRI Study of Thalamic and Cortical Activations Evoked by Cutaneous Heat, Cold, and Tactile Stimuli. J. Neurophysiol. 1998, 80, 1533–1546. [Google Scholar] [CrossRef]
- Hilker, R.; Voges, J.; Weisenbach, S.; Kalbe, E.; Burghaus, L.; Ghaemi, M.; Lehrke, R.; Koulousakis, A.; Herholz, K.; Sturm, V.; et al. Subthalamic nucleus stimulation restores glucose metabolism in associative and limbic cortices and in cerebellum: Evidence from a FDG-PET study in advanced Parkinson’s disease. J. Cereb. Blood Flow Metab. 2004, 24, 7–16. [Google Scholar] [CrossRef]
- Trost, M.; Su, S.; Su, P.; Yen, R.-F.; Tseng, H.-M.; Barnes, A.; Ma, Y.; Eidelberg, D. Network modulation by the subthalamic nucleus in the treatment of Parkinson’s disease. Neuroimage 2006, 31, 301–307. [Google Scholar] [CrossRef]
- Oswal, A.; Beudel, M.; Zrinzo, L.; Limousin, P.; Hariz, M.; Foltynie, T.; Litvak, V.; Brown, P. Deep brain stimulation modulates synchrony within spatially and spectrally distinct resting state networks in Parkinson’s disease. Brain 2016, 139, 1482–1496. [Google Scholar] [CrossRef] [PubMed]
- Herzog, J.; Weiss, P.H.; Assmus, A.; Wefer, B.; Seif, C.; Braun, P.M.; Pinsker, M.O.; Herzog, H.; Volkmann, J.; Deuschl, G.; et al. Improved sensory gating of urinary bladder afferents in Parkinson’s disease following subthalamic stimulation. Brain 2008, 131, 132–145. [Google Scholar] [CrossRef]
- DiMarzio, M.; Rashid, T.; Hancu, I.; Fiveland, E.; Prusik, J.; Gillogly, M.; Madhavan, R.; Joel, S.; Durphy, J.; Molho, E.; et al. Functional MRI Signature of Chronic Pain Relief from Deep Brain Stimulation in Parkinson Disease Patients. Neurosurgery 2019, 85, E1043–E1049. [Google Scholar] [CrossRef]
- Di Giulio, I.; St George, R.J.; Kalliolia, E.; Peters, A.L.; Limousin, P.; Day, B.L. Maintaining balance against force perturbations: Impaired mechanisms unresponsive to levodopa in Parkinson’s disease. J. Neurophysiol. 2016, 116, 493–502. [Google Scholar] [CrossRef]
- Hartmann, C.J.; Hirschmann, J.; Vesper, J.; Wojtecki, L.; Butz, M.; Schnitzler, A. Distinct cortical responses evoked by electrical stimulation of the thalamic ventral intermediate nucleus and of the subthalamic nucleus. Neuroimage Clin. 2018, 20, 1246–1254. [Google Scholar] [CrossRef] [PubMed]
- Garcia, L.; D’Alessandro, G.; Bioulac, B.; Hammond, C. High-frequency stimulation in Parkinson’s disease: More or less? Trends Neurosci. 2005, 28, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Rubin, J.E.; Terman, D. High frequency stimulation of the subthalamic nucleus eliminates pathological thalamic rhythmicity in a computational model. J. Comput. Neurosci. 2004, 16, 211–235. [Google Scholar] [CrossRef] [PubMed]
- Brown, P.; Oliviero, A.; Mazzone, P.; Insola, A.; Tonali, P.; Di Lazzaro, V. Dopamine dependency of oscillations between subthalamic nucleus and pallidum in Parkinson’s disease. J. Neurosci. 2001, 21, 1033–1038. [Google Scholar] [CrossRef]
- Obeso, J.A.; Rodríguez-Oroz, M.C.; Benitez-Temino, B.; Blesa, F.J.; Guridi, J.; Marin, C.; Rodriguez, M. Functional organization of the basal ganglia: Therapeutic implications for Parkinson’s disease. Mov. Disord. 2008, 23 (Suppl. 3), S548–S559. [Google Scholar] [CrossRef]
- Sudhyadhom, A.; McGregor, K.; Okun, M.S.; Foote, K.D.; Trinastic, J.; Crosson, B.; Bova, F.J. Delineation of motor and somatosensory thalamic subregions utilizing probabilistic diffusion tractography and electrophysiology. J. Magn. Reson. Imaging 2013, 37, 600–609. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PD-MED | PD-MED–DBS | HS | p-Values; r | ||
|---|---|---|---|---|---|
| Demographic data: | n/sex | 37/♂ 29/♀ 8 | 39/♂ 24/♀ 15 | 30/♂ 19/♀ 11 | – |
| age (years) | 68.5 ± 7.5 | 66.2 ± 6.5 b | 70.6 ± 5.7 b | b 0.023; 0.13 | |
| height (cm) | 169.6 ± 13.6 | 168.7 ± 8.1 | 171.3 ± 8.9 | – | |
| Clinical data: | self-rated balance confidence (0–100) (%) | 60.0 ± 20.2 a | 59.8 ± 20.1 b | 80.7 ± 9.4 a b | a <0.001; 0.50 b <0.001; 0.43 |
| self-rated gait confidence (0–100) (%) | 64.0 ± 22.5 a | 63.3 ± 18.3 b | 89.1 ± 8.4 a b | a <0.001; 0.55 b <0.001; 0.54 | |
| MMSE (0–30) | 28.5 ± 1.7 | 28.4 ± 1.6 | – | – | |
| UPDRS III (0–108) | 16.9 ± 7.9 | 15.7 ± 6.6 | – | – | |
| UPDRS total (0–199) | 27.8 ± 13.2 | 29.2 ± 10.7 | – | – | |
| Hoehn and Yahr (0–5) | 2.1 ± 0.5 | 2.1 ± 0.4 | – | – | |
| disease duration since diagnosis (months) | 85.1 ± 65.7 | 189.2 ± 77.6 | – | – | |
| disease-dominant body side | left: 17; right: 20 | left: 15; right: 24 | – | – | |
| time btw last neurological examination and testing (months) | 5.7 ± 15.2 a | 3.5 ± 3.9 a | – | a < 0.001; 0.66 | |
| DBS duration since surgery (months) | 33.1 ± 25.7 | – | – | ||
| self-rated satisfaction with DBS (%) | 80.1 ± 20.6 | – | – |
| PD-MED | PD-MED-DBS | HS | p-Values; r | |
|---|---|---|---|---|
| COP motion time anterior (s) | 7.1 ± 2.6 a | 5.3 ± 2.1 b | 3.0 ± 1.1 a b | a <0.001; 0.68; b 0.002; 0.43 |
| COP motion time posterior (s) | 6.3 ± 2.5 a | 4.7 ± 1.7 | 3.2 ± 1.4 a | a <0.001; 0.56 |
| COP mean motion velocity anterior (mm/s) | 12.9 ± 7.9 a | 19.9 ± 10.9 b | 37.3 ± 14.0 a b | a <0.001; 0.71; b 0.002; 0.43 |
| COP mean motion velocity posterior (mm/s) | 6.2 ± 3.7 a | 8.3 ± 3.2 b | 21.4 ± 11.4 a b | a <0.001; 0.72; b <0.001; 0.49 |
| PD-MED | PD-MED-DBS | HS | p-Values; r | |
|---|---|---|---|---|
| Stride length (cm) | 91.1 ± 18.0 a | 94.3 ± 12.8 b | 118.3 ± 16.1 a b | a <0.001; 0.56; b <0.001; 0.52 |
| Stride width (cm) | 10.7 ± 3.1 | 11.1 ± 3.0 b | 8.3 ± 1.8 b | – b <0.001; 0.29 |
| Stride time (s) | 1.2 ± 0.2 a | 1.2 ± 0.1 | 1.1 ± 0.1 a | a <0.001; 0.39; – |
| Gait velocity (m/s) | 0.8 ± 0.2 a | 0.8 ± 0.2 b | 1.1 ± 0.2 a b | a <0.001; 0.60; b <0.001; 0.49 |
| Cadence (steps/minute) | 49.2 ± 6.0 a | 52.4 ± 5.3 | 55.4 ± 4.6 a | a <0.001; 0.39; – |
| Double support time (%) | 35.3 ± 7.1 a | 32.7 ± 4.6 b | 28.4 ± 3.7 a b | a <0.001; 0.47; b <0.001; 0.35 |
| COP length mean left right (%) | 84.5 ± 6.4 a | 85.8 ± 7.3 | 89.9 ± 6.2 a | a 0.002; 0.31; – |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heß, T.; Themann, P.; Oehlwein, C.; Milani, T.L. Does Impaired Plantar Cutaneous Vibration Perception Contribute to Axial Motor Symptoms in Parkinson’s Disease? Effects of Medication and Subthalamic Nucleus Deep Brain Stimulation. Brain Sci. 2023, 13, 1681. https://doi.org/10.3390/brainsci13121681
Heß T, Themann P, Oehlwein C, Milani TL. Does Impaired Plantar Cutaneous Vibration Perception Contribute to Axial Motor Symptoms in Parkinson’s Disease? Effects of Medication and Subthalamic Nucleus Deep Brain Stimulation. Brain Sciences. 2023; 13(12):1681. https://doi.org/10.3390/brainsci13121681
Chicago/Turabian StyleHeß, Tobias, Peter Themann, Christian Oehlwein, and Thomas L. Milani. 2023. "Does Impaired Plantar Cutaneous Vibration Perception Contribute to Axial Motor Symptoms in Parkinson’s Disease? Effects of Medication and Subthalamic Nucleus Deep Brain Stimulation" Brain Sciences 13, no. 12: 1681. https://doi.org/10.3390/brainsci13121681