
A Comparison of Neuropsychological Outcomes following Responsive Neurostimulation and Anterior Temporal Lobectomy in Drug-Resistant Epilepsy

Abstract
:1. Introduction
2. Methods
2.1. Patient Selection and Eligibility Criteria
2.2. Study Variables
2.3. Statistics
3. Results
3.1. Patient Demographics
3.2. Preoperative Epilepsy and Neuropsychological Characteristics
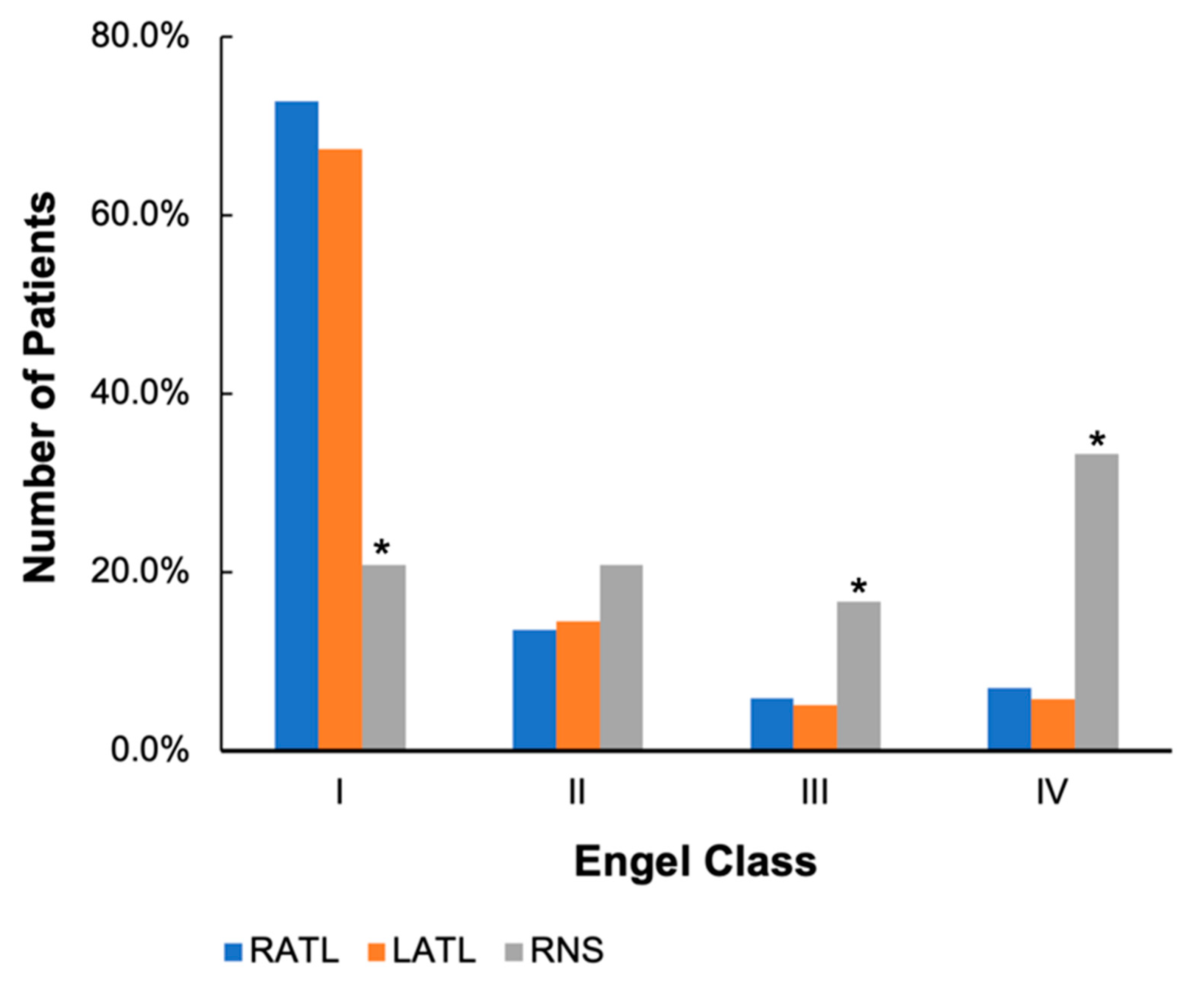
3.3. Post-Intervention Epilepsy Outcomes
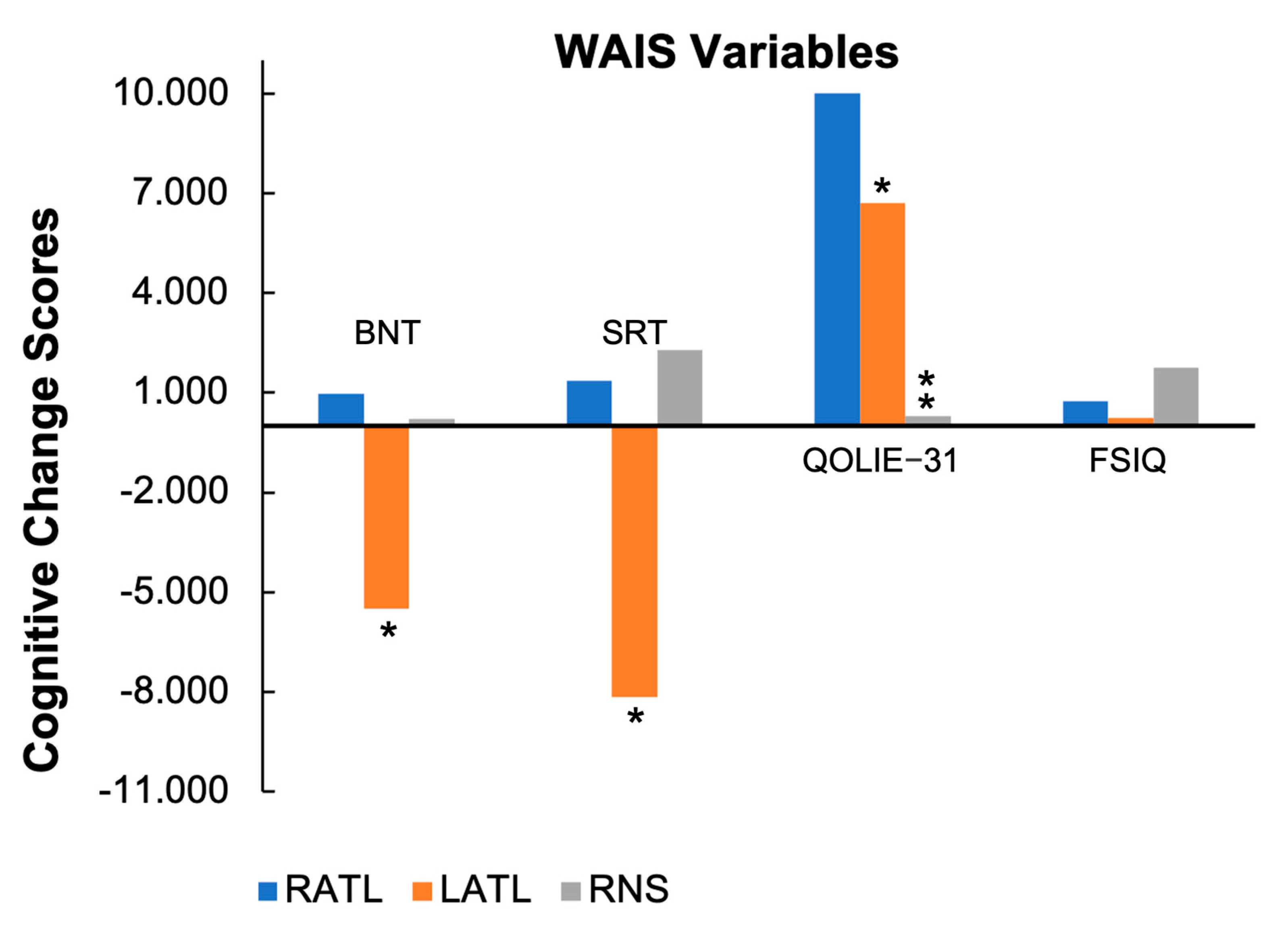
3.4. Post-Intervention Neuropsychological Outcomes

{kind=link}
{kind=link}
| Variables | p-Value (RNS vs. RATL) | RATL (n = 148–160) | RNS (n = 13–21) | LATL (n = 119–132) | p-Value (RNS vs. LATL) |
|---|---|---|---|---|---|
| WAIS | |||||
| FSIQ | 0.631 | 0.744 | 1.750 | 0.239 | 0.475 |
| VCI | 0.525 | 1.131 a | 0.053 | −3.238 a | 0.056 |
| PRI | 0.424 | −0.101 | 2.158 | 1.813 | 0.904 |
| WMI | 0.766 | 0.373 | −0.368 | −0.439 | 0.978 |
| PSI | 0.893 | −0.865 | −0.478 | 1.765 | 0.459 |
| Other assessments | |||||
| BNT | 0.453 | 0.970 a | 0.217 b | −5.508 a,b | 0.005 * |
| SRT | 0.810 | 1.354 a | 2.278 b | −8.160 a,b | 0.008 * |
| WMS- Visual Reproduction | 0.222 | −1.500 | −0.353 | −0.071 | 0.787 |
| COWA | 0.692 | −0.051 | −1.381 | 0.025 | 0.680 |
| Trails B | 0.206 | 1.429 | −3.824 | 1.246 | 0.228 |
| QOLIE-31 | 0.003 * | 10.013 a | 0.308 a,b | 6.712 a,b | 0.050 * |
| MMPI—Scale 2 | 0.547 | 3.556 | 3.327 | 0.750 | 0.341 |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kwan, P.; Arzimanoglou, A.; Berg, A.T.; Brodie, M.J.; Allen Hauser, W.; Mathern, G.; Moshé, S.L.; Perucca, E.; Wiebe, S.; French, J. Definition of Drug Resistant Epilepsy: Consensus Proposal by the Ad Hoc Task Force of the ILAE Commission on Therapeutic Strategies: Definition of Drug Resistant Epilepsy. Epilepsia 2009, 51, 1069–1077. [Google Scholar] [CrossRef]
- Kalilani, L.; Sun, X.; Pelgrims, B.; Noack-Rink, M.; Villanueva, V. The Epidemiology of Drug-Resistant Epilepsy: A Systematic Review and Meta-Analysis. Epilepsia 2018, 59, 2179–2193. [Google Scholar] [CrossRef]
- Sultana, B.; Panzini, M.-A.; Carpentier, A.V.; Comtois, J.; Rioux, B.; Gore, G.; Bauer, P.R.; Kwon, C.-S.; Jetté, N.; Josephson, C.B.; et al. Incidence and Prevalence of Drug-Resistant Epilepsy: A Systematic Review and Meta-Analysis. Neurology 2021, 96, 805–817. [Google Scholar] [CrossRef]
- Chelune, G.J.; Naugle, R.I.; Lüders, H.; Awad, I.A. Prediction of Cognitive Change as a Function of Preoperative Ability Status among Temporal Lobectomy Patients Seen at 6-Month Follow-Up. Neurology 1991, 41, 399–404. [Google Scholar] [CrossRef]
- Hermann, B.P.; Seidenberg, M.; Haltiner, A.; Wyler, A.R. Relationship of Age at Onset, Chronologic Age, and Adequacy of Preoperative Performance to Verbal Memory Change after Anterior Temporal Lobectomy. Epilepsia 1995, 36, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Loring, D.W.; Meador, K.J.; Lee, G.P.; King, D.W.; Nichols, M.E.; Park, Y.D.; Murro, A.M.; Gallagher, B.B.; Smith, J.R. Wada Memory Asymmetries Predict Verbal Memory Decline after Anterior Temporal Lobectomy. Neurology 1995, 45, 1329–1333. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.M.C.; Yip, J.T.H.; Jones-Gotman, M. Memory Deficits after Resection from Left or Right Anterior Temporal Lobe in Humans: A Meta-Analytic Review. Epilepsia 2002, 43, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Morris, G.L.; Mueller, W.M. Long-Term Treatment with Vagus Nerve Stimulation in Patients with Refractory Epilepsy. The Vagus Nerve Stimulation Study Group E01-E05. Neurology 1999, 53, 1731–1735. [Google Scholar] [CrossRef]
- Penry, J.K.; Dean, J.C. Prevention of Intractable Partial Seizures by Intermittent Vagal Stimulation in Humans: Preliminary Results. Epilepsia 1990, 31, S40–S43. [Google Scholar] [CrossRef]
- Tröster, A.I.; Meador, K.J.; Irwin, C.P.; Fisher, R.S. Memory and Mood Outcomes after Anterior Thalamic Stimulation for Refractory Partial Epilepsy. Seizure 2017, 45, 133–141. [Google Scholar] [CrossRef]
- Fisher, R.; Salanova, V.; Witt, T.; Worth, R.; Henry, T.; Gross, R.; Oommen, K.; Osorio, I.; Nazzaro, J.; Labar, D.; et al. Electrical Stimulation of the Anterior Nucleus of Thalamus for Treatment of Refractory Epilepsy: Deep Brain Stimulation of Anterior Thalamus for Epilepsy. Epilepsia 2010, 51, 899–908. [Google Scholar] [CrossRef]
- Burdette, D.; Mirro, E.A.; Lawrence, M.; Patra, S.E. Brain-Responsive Corticothalamic Stimulation in the Pulvinar Nucleus for the Treatment of Regional Neocortical Epilepsy: A Case Series. Epilepsia Open 2021, 6, 611–617. [Google Scholar] [CrossRef]
- Morrell, M.J. RNS System in Epilepsy Study Group Responsive Cortical Stimulation for the Treatment of Medically Intractable Partial Epilepsy. Neurology 2011, 77, 1295–1304. [Google Scholar] [CrossRef]
- Heck, C.N.; King-Stephens, D.; Massey, A.D.; Nair, D.R.; Jobst, B.C.; Barkley, G.L.; Salanova, V.; Cole, A.J.; Smith, M.C.; Gwinn, R.P.; et al. Two-Year Seizure Reduction in Adults with Medically Intractable Partial Onset Epilepsy Treated with Responsive Neurostimulation: Final Results of the RNS System Pivotal Trial. Epilepsia 2014, 55, 432–441. [Google Scholar] [CrossRef]
- Nair, D.R.; Laxer, K.D.; Weber, P.B.; Murro, A.M.; Park, Y.D.; Barkley, G.L.; Smith, B.J.; Gwinn, R.P.; Doherty, M.J.; Noe, K.H.; et al. Nine-Year Prospective Efficacy and Safety of Brain-Responsive Neurostimulation for Focal Epilepsy. Neurology 2020, 95, e1244–e1256. [Google Scholar] [CrossRef] [PubMed]
- Tager, D.; Panjeti-Moore, D.; Yang, J.C.; Rivera-Cruz, A.; Loring, D.W.; Staikova, E.; Block, C.; Bullinger, K.L.; Rodriguez-Ruiz, A.A.; Cabaniss, B.T.; et al. The Effect of Responsive Neurostimulation (RNS) on Neuropsychiatric and Psychosocial Outcomes in Drug-Resistant Epilepsy. Epilepsy Behav. 2023, 142, 109207. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research Electronic Data Capture (REDCap)—A Metadata-Driven Methodology and Workflow Process for Providing Translational Research Informatics Support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Janecek, J.K.; Brett, B.L.; Pillay, S.; Murphy, H.; Binder, J.R.; Swanson, S.J. Cognitive Decline and Quality of Life after Resective Epilepsy Surgery. Epilepsy Behav. 2023, 138, 109005. [Google Scholar] [CrossRef] [PubMed]
- Wechsler, D. Wechsler Adult Intelligence Scale, 4th ed.; PsycTESTS Dataset: Washington, DC, USA, 2008. [Google Scholar] [CrossRef]
- Kaplan, E.; Goodglass, H.; Weintraub, S. Boston Naming Test; Lea & Febiger: Philadelphia, PA, USA, 1983. [Google Scholar]
- Buschke, H. Selective Reminding for Analysis of Memory and Learning. J. Verbal Learn. Verbal Behav. 1973, 12, 543–550. [Google Scholar] [CrossRef]
- Cramer, J.A.; Perrine, K.; Devinsky, O.; Bryant-Comstock, L.; Meador, K.; Hermann, B. Development and Cross-Cultural Translations of a 31-Item Quality of Life in Epilepsy Inventory. Epilepsia 1998, 39, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Reitan, R.M.; Wolfson, D. The Halstead—Reitan Neuropsychological Test Battery: Research Findings and Clinical Application. In Specific Learning Disabilities and Difficulties in Children and Adolescents: Psychological Assessment and Evaluation; Kaufman, A.S., Kaufman, N.L., Eds.; Cambridge Child and Adolescent Psychiatry; Cambridge University Press: Cambridge, UK, 2001; pp. 309–346. ISBN 978-0-521-65840-9. [Google Scholar]
- Guekht, A.B.; Mitrokhina, T.V.; Lebedeva, A.V.; Dzugaeva, F.K.; Milchakova, L.E.; Lokshina, O.B.; Feygina, A.A.; Gusev, E.I. Factors Influencing on Quality of Life in People with Epilepsy. Seizure Eur. J. Epilepsy 2007, 16, 128–133. [Google Scholar] [CrossRef] [PubMed]


| Variables | Thalamic RNS (n = 6) | Non-Thalamic RNS (n = 15) |
|---|---|---|
| Epilepsy diagnosis | ||
| LRE (single focus) | 1 | 14 |
| LRE (multifocal) | 1 | 1 |
| GGE/JME | 3 | 0 |
| LGS | 1 | 0 |
| History of prior resective surgery | ||
| Yes | 1 | 7 |
| No | 5 | 8 |
| Location of RNS electrodes | ||
| LANT | 4 | 0 |
| RANT | 4 | 0 |
| LCM | 2 | 0 |
| RCM | 2 | 0 |
| LFS | 1 | 2 |
| RFS | 0 | 0 |
| LHIP (limbic) | 0 | 11 |
| RHIP (limbic) | 0 | 10 |
| LTS (neocortical) | 0 | 5 |
| RTS (neocortical) | 0 | 0 |
| Variables | RATL (n = 169) | RNS (n = 21) | LATL (n = 138) |
|---|---|---|---|
| Sex (%) | |||
| Male | 40.2 | 29.2 | 48.6 |
| Female | 59.8 | 70.8 | 51.4 |
| Race/Ethnicity (%) | |||
| White | 89.9 | 83.3 | 87.7 |
| Black | 7.7 | 12.5 | 5.8 |
| Hispanic | 2.4 | 4.2 | 5.1 |
| Asian | 0.0 | 0.0 | 0.7 |
| Unknown | 0.0 | 0.0 | 0.7 |
| Marital status (%) | |||
| Married | 36.7 | 37.5 | 42.0 |
| Divorced | 10.7 | 12.5 | 9.4 |
| Separated | 0.6 | 0.0 | 0.7 |
| Never married | 48.5 | 45.8 | 44.9 |
| Widowed | 0.6 | 4.2 | 0.0 |
| Unknown | 3.0 | 0.0 | 2.9 |
| Handedness (%) | |||
| Right | 85.8 | 79.2 | 81.2 |
| Left | 9.5 | 12.5 | 16.7 |
| Mixed | 4.7 | 8.3 | 2.2 |
| Average length of education (years) | 12.96 | 13.29 | 12.70 |
| Variables | p-Value (RNS vs. RATL) | RATL (n = 169) | RNS (n = 21) | LATL (n = 138) | p-Value (RNS vs. LATL) |
|---|---|---|---|---|---|
| Preoperative epilepsy characteristics | |||||
| Seizure frequency (number/month) | 0.010 * | 25 a | 62 a,b | 16 b | 0.002 * |
| Seizure frequency excluding simple partials/auras (number/month) | 0.003 * | 18 a | 59 a,b | 12 b | 0.001 * |
| Age at seizure onset (years) | 0.117 | 15 | 19 a | 14 a | 0.047 * |
| Age at onset of recurrent seizures (years) | 0.441 | 16 | 20 | 17 | 0.258 |
| Disease duration (years) | 0.651 | 20 | 21 | 20 | 0.668 |
| Age at pre-op neuropsychological testing | 0.163 | 37 | 41 | 36 | 0.080 |
| Preoperative neuropsychological characteristics in intellectual testing (WAIS-III—WAIS-IV) | |||||
| Verbal Comprehension Index | 0.007 * | 92.76 a | 83.57 a | 89.57 | 0.083 |
| Perceptual Organizations Index | 0.162 | 93.45 | 89.00 | 94.69 | 0.078 |
| Working Memory Index | 0.170 | 89.41 | 84.40 | 91.06 | 0.071 |
| Processing Speed Index | 0.002 * | 90.64 a | 79.63 a,b | 91.68 b | 0.002 * |
| Full scale IQ | 0.012 * | 90.64 a | 81.84 a,b | 90.07 b | 0.019 * |
| Variables | RATL (n = 153–168) | RNS (n = 21) | LATL (n = 126–128) |
|---|---|---|---|
| Engel scores (%) | |||
| Class I | 72.8 a | 20.8 a,b | 67.4 b |
| Class II | 13.6 | 20.8 | 14.5 |
| Class III | 5.9 a | 16.7 a,b | 5.1 b |
| Class IV | 7.1 a | 33.3 a,b | 5.8 b |
| Reduction in seizure frequency (%) | 63.9 | 60.1 | 80.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
O’Donnell, C.M.; Anderson, C.T.; Oleksy, A.J.; Swanson, S.J. A Comparison of Neuropsychological Outcomes following Responsive Neurostimulation and Anterior Temporal Lobectomy in Drug-Resistant Epilepsy. Brain Sci. 2023, 13, 1628. https://doi.org/10.3390/brainsci13121628
O’Donnell CM, Anderson CT, Oleksy AJ, Swanson SJ. A Comparison of Neuropsychological Outcomes following Responsive Neurostimulation and Anterior Temporal Lobectomy in Drug-Resistant Epilepsy. Brain Sciences. 2023; 13(12):1628. https://doi.org/10.3390/brainsci13121628
Chicago/Turabian StyleO’Donnell, Carly M., Christopher Todd Anderson, Anthony J. Oleksy, and Sara J. Swanson. 2023. "A Comparison of Neuropsychological Outcomes following Responsive Neurostimulation and Anterior Temporal Lobectomy in Drug-Resistant Epilepsy" Brain Sciences 13, no. 12: 1628. https://doi.org/10.3390/brainsci13121628