

Phenomenological Changes Associated with Deep Brain Stimulation for Obsessive Compulsive Disorder: A Cognitive Appraisal Model of Recovery

Abstract
:1. Introduction
1.1. The Cognitive Mechanisms of OCD Psychopathology Are Complex
1.2. The Assessment of DBS Efficacy Is Too Narrow
1.3. DBS Neuroethical Concerns Lack Empirical Evidence
1.4. The DBS Scientific Literature Lacks the Patient Perspective
2. Methods
2.1. Participants
2.2. Procedure
2.3. Analysis
3. Results
3.1. Lived Experiences Prior to DBS and Major Changes
3.2. Phenomenological Themes
3.2.1. Psychopathological Theme 1: More Alive
3.2.2. Psychopathological Theme 2: Improved Cognitive-Affective Control
3.2.3. Psychopathological Theme 3: Greater Engagement
3.2.4. Psychopathological Theme 4: Able to Manage the OCD
3.2.5. Self and Identity Theme 1: Self-Actualization
3.2.6. Self and Identity Theme 2: Prioritization of the Self
3.2.7. Self and Identity Theme 3: Changed Role in Life
3.2.8. Carer Theme 1. Changed Outlook
3.2.9. Carer Theme 2: Able to Be Their True Self
3.2.10. Carer Theme 3: Enriched Experiences and Relationships
3.2.11. Carer Theme 4: Enabled to Take Control of Life
3.3. Difficulties Experienced through Recovery
3.3.1. Burden of Normality
3.3.2. Grief for Lost Time
3.3.3. Difficulties of Charging Batteries
3.3.4. Changes Experiences by Carers
4. Discussion
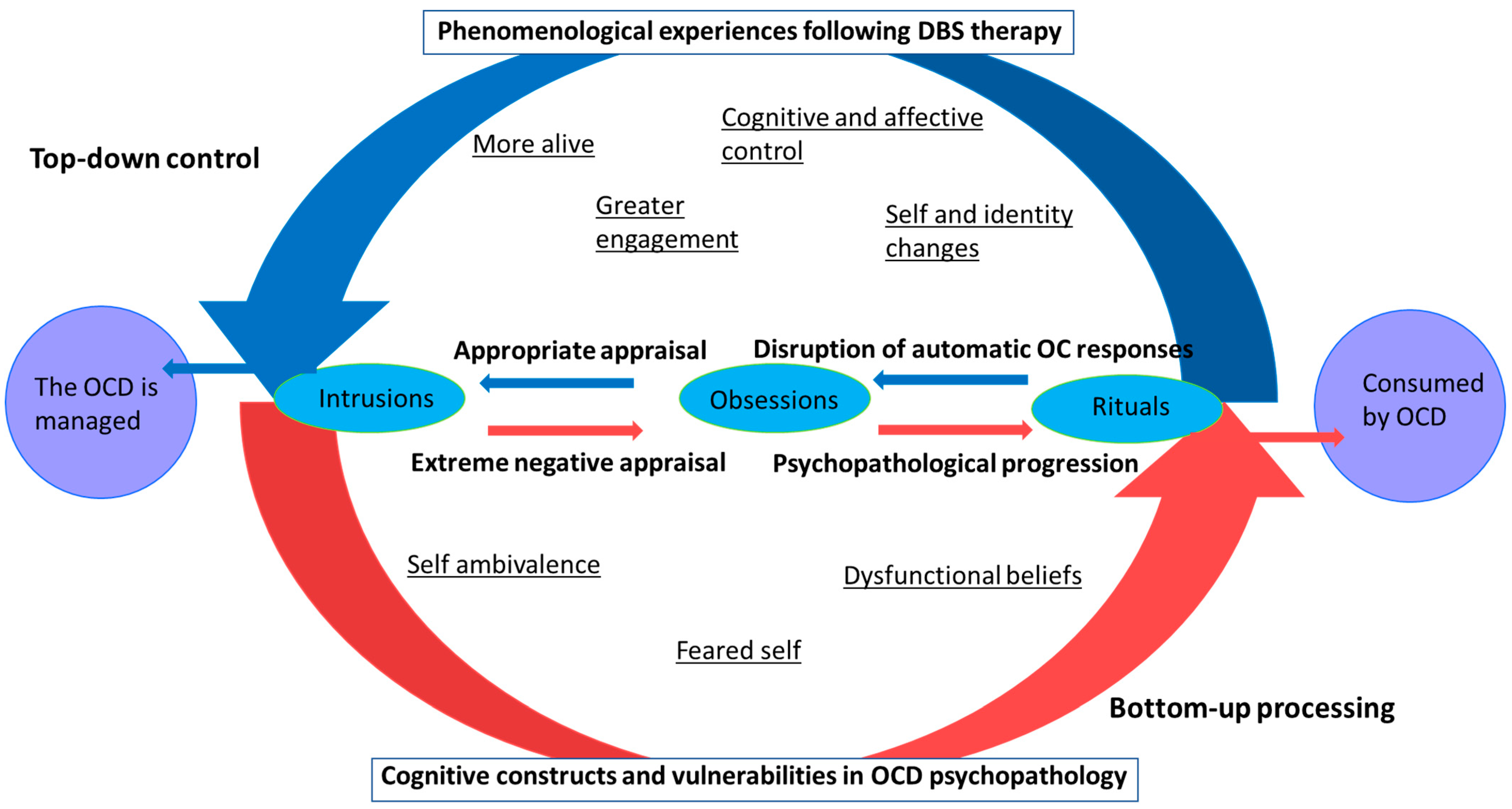
4.1. Conceptual Framework: Phenomenological Model of DBS Induced Changes
4.2. Proposed Cognitive Model of Changes in the Cognitive Appraisal of Obsessional Intrusions
4.3. Changes to the Self
4.4. Clinical Relevance of Findings
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Widge, A.S.; Deckersbach, T.; Eskandar, E.N.; Dougherty, D.D. Deep Brain Stimulation for Treatment-Resistant Psychiatric Illnesses: What Has Gone Wrong and What Should We Do Next? Biol. Psychiatry 2016, 79, e9–e10. [Google Scholar] [CrossRef] [PubMed]
- Thomson, C.; Carter, A. Ethical issues in experimental treatments for psychiatric disorders: Lessons from deep brain stimulation. Transl. Issues Psychol. Sci. 2020, 6, 240–246. [Google Scholar] [CrossRef]
- De Haan, S.; Rietveld, E.; Stokhof, M.; Denys, D. The phenomenology of deep brain stimulation-induced changes in OCD: An enactive affordance-based model. Front. Hum. Neurosci. 2013, 7, 653. [Google Scholar] [CrossRef] [PubMed]
- Abramowitz, J.S.; McKay, D.; Storch, E.A. The Wiley Handbook of Obsessive Compulsive Disorders; John Wiley & Sons: Hoboken, NJ, USA, 2017. [Google Scholar]
- Bosanac, P.; Hamilton, B.E.; Lucak, J.; Castle, D. Identity challenges and ‘burden of normality’ after DBS for severe OCD: A narrative case study. BMC Psychiatry 2018, 18, 186. [Google Scholar] [CrossRef] [PubMed]
- De Haan, S.; Rietveld, E.; Stokhof, M.; Denys, D. Effects of Deep Brain Stimulation on the Lived Experience of Obsessive-Compulsive Disorder Patients: In-Depth Interviews with 18 Patients. PLoS ONE 2015, 10, e0135524. [Google Scholar] [CrossRef] [PubMed]
- De Haan, S.; Rietveld, E.; Stokhof, M.; Denys, D. Becoming more oneself? Changes in personality following DBS treatment for psychiatric disorders: Experiences of OCD patients and general considerations. PLoS ONE 2017, 12, e0175748. [Google Scholar] [CrossRef] [PubMed]
- Mataix-Cols, D.; de la Cruz, L.F.; Nordsletten, A.E.; Lenhard, F.; Isomura, K.; Simpson, H.B. Towards an international expert consensus for defining treatment response, remission, recovery and relapse in obsessive-compulsive disorder. World Psychiatry 2016, 15, 80. [Google Scholar] [CrossRef]
- Synofzik, M.; Schlaepfer, T.E. Stimulating personality: Ethical criteria for deep brain stimulation in psychiatric patients and for enhancement purposes. Biotechnol. J. 2008, 3, 1511–1520. [Google Scholar] [CrossRef]
- Thomson, C.J.; Segrave, R.A.; Carter, A. Changes in Personality Associated with Deep Brain Stimulation: A Qualitative Evaluation of Clinician Perspectives. Neuroethics 2021, 14, 109–124. [Google Scholar] [CrossRef]
- Temel, Y.; Kessels, A.; Tan, S.; Topdag, A.; Boon, P.; Visser-Vandewalle, V. Behavioural changes after bilateral subthalamic stimulation in advanced Parkinson disease: A systematic review. Park. Relat. Disord. 2006, 12, 265–272. [Google Scholar] [CrossRef]
- Van Westen, M.; Rietveld, E.; Denys, D. Effective Deep Brain Stimulation for Obsessive-Compulsive Disorder Requires Clinical Expertise. Front. Psychol. 2019, 10, 2294. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Alase, A. The interpretative phenomenological analysis (IPA): A guide to a good qualitative research approach. Int. J. Educ. Lit. Stud. 2017, 5, 9–19. [Google Scholar] [CrossRef]
- Bengtsson, M. How to plan and perform a qualitative study using content analysis. NursingPlus Open 2016, 2, 8–14. [Google Scholar] [CrossRef]
- Skapinakis, P.; Caldwell, D.M.; Hollingworth, W.; Bryden, P.; Fineberg, N.A.; Salkovskis, P.; Welton, N.J.; Baxter, H.; Kessler, D.; Churchill, R.; et al. Pharmacological and psychotherapeutic interventions for management of obsessive-compulsive disorder in adults: A systematic review and network meta-analysis. Lancet Psychiatry 2016, 3, 730–739. [Google Scholar] [CrossRef] [PubMed]
- Rachman, S. A cognitive theory of obsessions. In Behavior and Cognitive Therapy Today; Elsevier: Amsterdam, The Netherlands, 1998; pp. 209–222. [Google Scholar]
- Obsessive Compulsive Cognitions Working Group. Cognitive assessment of obsessive-compulsive disorder. Behav. Res. Ther. 1997, 35, 667–681. [Google Scholar] [CrossRef] [PubMed]
- Obsessive Compulsive Cognitions Working Group. Psychometric validation of the obsessive belief questionnaire and interpretation of intrusions inventory—Part 2: Factor analyses and testing of a brief version. Behav. Res. Ther. 2005, 43, 1527–1542. [Google Scholar] [CrossRef]
- Aardema, F.; Moulding, R.; Radomsky, A.S.; Doron, G.; Allamby, J.; Souki, E. Fear of self and obsessionality: Development and validation of the Fear of Self Questionnaire. J. Obs. Compuls. Relat. Disord. 2013, 2, 306–315. [Google Scholar] [CrossRef]
- Bhar, S.S.; Kyrios, M. An investigation of self-ambivalence in obsessive-compulsive disorder. Behav. Res. Ther. 2007, 45, 1845–1857. [Google Scholar] [CrossRef]
- Kyrios, M.; Nelson, B.; Ahern, C.; Fuchs, T.; Parnas, J. The Self in Psychopathology. Psychopathology 2015, 48, 275–277. [Google Scholar] [CrossRef] [PubMed]
- Doron, G.; Kyrios, M. Obsessive compulsive disorder: A review of possible specific internal representations within a broader cognitive theory. Clin. Psychol. Rev. 2005, 25, 415–432. [Google Scholar] [CrossRef] [PubMed]
- Purdon, C.; Clark, D.A. Metacognition and obsessions. Clin. Psychol. Psychother. Int. J. Theory Pract. 1999, 6, 102–110. [Google Scholar] [CrossRef]
- Baumeister, R.F. Self and identity: A brief overview of what they are, what they do, and how they work. Ann. N. Y. Acad. Sci. 2011, 1234, 48–55. [Google Scholar] [CrossRef]
- Van Westen, M.; Rietveld, E.; Bergfeld, I.O.; de Koning, P.; Vullink, N.; Ooms, P.; Graat, I.; Liebrand, L.; van den Munckhof, P.; Schuurman, R.; et al. Optimizing Deep Brain Stimulation Parameters in Obsessive–Compulsive Disorder. Neuromodulation Technol. Neural Interface 2020, 24, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Holland, M.T.; Trapp, N.T.; McCormick, L.M.; Jareczek, F.J.; Zanaty, M.; Close, L.N.; Beeghly, J.; Greenlee, J.D.W. Deep Brain Stimulation for Obsessive-Compulsive Disorder: A Long Term Naturalistic Follow Up Study in a Single Institution. Front. Psychiatry 2020, 11, 55. [Google Scholar] [CrossRef] [PubMed]
- Acevedo, N.; Castle, D.; Groves, C.; Bosanac, P.; Mosley, P.E.; Rossell, S. Clinical recommendations for the care of people with treatment-refractory obsessive-compulsive disorder when undergoing deep brain stimulation. Aust. N. Z. J. Psychiatry 2022, 56, 1219–1225. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Themes | Sub-Themes | Extract |
|---|---|---|
| More alive | Feeling of lightness and being carefree | “I just felt lighter, there was just this feeling in me, and something inside me felt lighter” “Immediately I felt better, I just felt better, I don’t know how to explain it” “You could just see in my eyes… there was no one there… but yeah I have more life I guess” |
| More present | “A completely different ability, to have that capacity to be in the moment, and to have the ability to enjoy life” “I noticed was the ability to be in the moment…so when I’m just sitting and watching the sunset over the trees or something” “You focus on the real world so to speak” | |
| Changed outlook and approach to life | “I always try and look on the bright side, try and stay positive, but my mood [before DBS] would always just be dark” “Anything is possible, if I put my mind to it anything is possible, I could try and do anything if I wanted to, nothing is out of my reach” “I started to turn my life around” | |
| Appreciation for life | “I am just so grateful… you just can’t put it into words” “It’s just been joyous, to feel as if life can be wonderful and exciting and interesting and doable” | |
| Life has been saved | “I wouldn’t be here without the DBS, that’s for sure” “I felt more alive” “It can change the way you think feel and react and change your life, the DBS has been a lifesaver for me, a life changer” “My life had been a misery, I was done, finished. Luckily DBS was there…now I’m functioning” | |
| Improved cognitive-affective control | Greater mental clarity | “All the clouds had been lifted” “I couldn’t do this, sit down and have a conversation with someone, I would just be so much in my head, if you asked me a question, I would have to ask you 2 or 3 times to repeat the question” “Before DBS I would look at a situation in 10 thousand different ways and angles and stress about it, I have noticed I just let it be” “DBS gave me an ability to think, when I didn’t have DBS I couldn’t think, I couldn’t stop and think” “Now when I have a thought come in that’s stressful, I don’t divert to OCD thinking, that doesn’t happen anymore” |
| Implementation of cognitive control strategies | “It’s given me the capacity, to have the confidence, to have the cognitive capabilities, to do the work.” “ERP [exposure response and prevention] was impossible to do without the DBS” “Before the DBS I would have all these steps and now I can sort of, instead of doing every step I can generalise it and just say a word that would sum up everything, for all those steps” | |
| Improved self-regulation | “I’m better at not reacting… at saying, what do I want to get out of this situation” “There’s been so much that I’ve had to be flexible for, and I’ve just done it, and I’ve smiled all the way through it” “The stress component in my brain doesn’t seem to trigger” | |
| Greater engagement | Expanding perimeter of opportunities | “My worlds gotten bigger… there’s more opportunity” “Before I had no lust for life…. the world has opened up for me, there are opportunities, there are things out there” “I had no opportunities and no way to engage in them before DBS” “I go out and do things that I have never done before” “I feel like the world out there isn’t just for other people anymore…that is just amazing” |
| Able to experience the beauty and joy in the world | “I found pleasure in finding lost things that I used to enjoy” “It gets to the point where you think…would you prefer to be walking down next to the creek where the birds are chirping and that or would you rather be in a hospital within white walls. So, you got to help yourself” | |
| Enriched experiences | “I like to explore and discover things, art, painting, writing” “Social events are really easy- used to be hard, you wouldn’t do it, make up some excuse” “Just being able to have a conversation, hear what they say and take it in… being present, and being part of the friendship or relationship” “I hadn’t hugged my parents for 5–6 years, so I could start to hugging people” | |
| Able to manage OCD | Reduced intensity | “It [OCD] had the punch taken out of it, the strength taken out of….it was like the monster had been depleted.” “It’s not nearly as strong anymore… it doesn’t come into the room and fill it anymore” “Still have about 25% of days where it can creep in, 50% where I can function and 25% where it’s really happy days, whereas before it was virtually 90% shitty days” |
| Took control of OCD | “It gave me the power to change things… to say I’m the boss, the OCD is not the boss… I have a choice if I do something 10 times or if I do it once.” “Defeating is a good word, but it [OCD] will bark back sometimes” “I got rid of 99% of my rituals and compulsions, but there was always 1% left…and then I ticked it off” | |
| New relationship to OCD | “Rituals made me feel safe… definitely a sense of grieving… it was like an enemy, I guess a frenemy, so grieving like a friend of the time” “I’m not trying to cure it anymore, it’s there, I manage it” “You can’t kill OCD, but you can manage it, DBS has definitely helped me manage it” | |
| Enhanced resilience and strength | “My resilience is a lot better” “When the OCD comes on strong, I am able to sort of shrug it off more easily” “When I am operating at low stress, virtually no [intrusive] thoughts come through and end up as rituals, but when my stress levels are high, the thoughts come through that filter” “I am able to see the bad days don’t last” | |
| On a journey to recovery | “Still have a way to go, but compared to where I was, much better” “There are good days and bad days, but it’s a work in progress… it’s definitely an upward trajectory” “It’s like a reverse mountain climb, instead of looking at how far you have to go, you look at how far you have come… it’s a work in progress” |
| Themes | Sub-Themes | Extract |
|---|---|---|
| Self-actualisation | Discovery of the self | “Before DBS I wasn’t able to have a personality, have a sense of self, because my sense of self was my illness, I was my illness. Now I view myself as someone that can do things, not everything, but I can do enough” “I am growing into who I am supposed to be, well not who I am supposed to be, but who I am” “It’s actually a discovery of identity. It’s finding out new things and rediscovering what you enjoy” |
| Able to appreciate one’s place in the world | “Now I view myself as, I am a part of society I am a part of the people that do stuff, when your sick you only see sickness and you don’t see ahead” “It [DBS] has given me the ability to start thinking about things other than OCD… to start studying, and a career, and my daughter” “I feel like I’m offering something to the world I couldn’t have done prior to the surgery” | |
| Existential thoughts | “I have had big picture problems arise where I’ve wanted answers, and I can’t get any answers…what’s going to happen in 30 years” “To feel life is so hard, and when is it going to end, here’s me worrying oh I’ve only got 40 years at the most, where as I used to be- how many more years to go…I wish I had more years to go” | |
| Prioritisation of the self | Greater self-worth and self-love | “I just feel more comfortable within myself, like who I am” “I am getting more comfortable with telling myself, that I’m an okay person, that I am actually a good person” “I am proud of myself, and I am very happy that I was able to overcome the illness, to a degree” “Before DBS I felt terrible and I evaluated myself as not functioning, not functioning, not part of society, not contributing to anything, just useless. Now I feel the opposite” |
| Pursuing own wants and needs | “The more I do and the more I achieve and the more I feel connected with people, the better I feel, the better that gets and the quieter the critic gets” “I am now doing what I want to do, this is always what I have wanted to do” “It’s about rediscovering and more focus on me” | |
| Changed role in life | Improved theory of mind | “I feel like I have given my dad his life back… and then started my own” “She only had half a mum… now I know doing the best I can is actually a really good effort…I’m proud of the way I am bringing her up” |
| Gained independence | “The thoughts that were there before DBS, I couldn’t have a girlfriend, I couldn’t live alone, I couldn’t have a child… all those milestones were hard to reach but I reached those milestones” | |
| Engaged in supporting others | “I wasn’t really in tune with her [daughter], now I feel I want to do something, I want to help her achieve a productive but happy life” “The lived experience work I’m doing… is just incredible…people value what you have been through… it makes you feel really good about yourself” |
| Themes | Sub-Themes | Extract |
|---|---|---|
| Changed outlook | More present | “It was as though a layer of the cloud had lifted” “It [DBS] enables a person to look at life differently, and able to have a bit more control over your feelings and what you’re doing” “After having DBS I think she is more in the moment, less worried about things that are going to happen in the future, it’s a more kind of normal state of thinking” |
| Acceptance and resilience | “I think they did obviously realise that they still had to challenge the OCD all the time, everyday” “Much more accepting of who people are” “If she hadn’t had OCD their life would have been incredibly different, but they have learnt to be incredibly positive about what is in her life now” | |
| Able to be their true self | No longer defined by OCD | “I think it has just allowed her to be the person that she always has been” “She’s definitely more confident out in the world, there’s no question of that, definitely, definitely!” “If the DBS has done anything in terms of her personality it has allowed it to come through” “It’s more like he has an outward focus of 60–70%, but the OCD is still there” |
| Improved self -regulation and self-awareness | “She knows sometimes she will feel like not going and still make the effort to go, other times she will say I need to step away from that on this occasion” “It has been a gradual process since the DBS of adjusting to what she can do, and she’s gotten very good at recognising what she can do, but also recognising what she doesn’t want to do” | |
| More vibrant and expressive | “If she was depressed, she would be sleeping all day or on the coach all day…she’s more awake, she’s more alert, she has more energy” “She’s become more relaxed, more herself and more decisive about things, and yeah, it’s really great to see, she is calm, relaxed, decisive, happy, vibrant, much more outgoing, not bogged down in her thoughts” | |
| Enriched experiences and relationships | Experiences joy and happiness | “She just seems a lot happier, in the moment, if something bad happens she is like- oh well” “She can go off and go out for the evening with her friends and enjoy that, rather than lying in bed and obsessing about different scenarios” |
| More engaged in the world | “Well she’s engaged in what is going on in the world, she has a variety of thing, she’s interested in…so she has the headspace now to be interested in that” “I think exercise is a great thing, and he was so motivated, and I loved to hear, when I would ring him, he would tell me, I’ve done this, I am going to rest now and meditate” “She [participant] said …I have been cured from my OCD, I just want to go out and live my life” “It was like a switch, he was doing things, driving around going to places, having mini breaks, stuff like that” “I am happy he has had it done, it has helped him in a lot of ways, he does get out more. Before he was just housebound, before DBS he couldn’t get out of bed, he wasn’t showering” | |
| Enabled to take control of life | Reduced hyperarousal and depression | “Well the DBS has enabled her to keep the OCD under control and to just engage with life in a much more meaningful way” “DBS isn’t an instantaneous cure for these things, but it seems to bring the parameters of the depth of depression and volcanic effect of anxiety, it seems to suppress the upper and lower level” “They felt a reduction in this chronic ambient hyperarousal state” |
| On a defined path | “I wouldn’t say by any means she is free of it [OCD]… she has learnt to manage it incredible well” “There have been set back but on the whole it has been a very positive journey, there is no question about it” “What it does, is it re-enables people” “The DBS has allowed her to incrementally take much more control of her life” “She is flourishing and doing more now than she has ever done, and she is working things out” “I’m more hopeful for his future, and I think we can get there, slow and steady but we can get there” | |
| Changed role | “I think we have a very good relationship, because she has embraced being much more independent” “It kind of made me feel like I was living with a stranger, which I don’t know how to… she changed for the better and I got to see more of the good side of her, which were far and in between but now it is more constant” “I think I’m a bit closer to him then I was before, I felt a bit alienated, it was more, I felt like I was, not a slave, but a go getter boy, or a fix it, whereas now, it’s not as much, he tries to do things himself” | |
| Personal development with appropriate support | “I think she has matured quite a lot, she has without a doubt, there is no doubt about that, when you are constantly in a state of high anxiety, that undermines any capacity you have for maturing from a child to a teenager to an adult” “Since the DBS he has been able to move on, he left home. he has a partner, and they have a baby, to even have a baby, is a bit of a miracle” “I think that without the DBS I wouldn’t be sitting here talking to you about his family and his achievements that he has made in that period of time” “I can see small changes but I was hoping for a lot more, you know, bigger changes in him” | |
| Themes related to carers | Burden is lifted | “I am much more happier and content now that she’s much more stable” “So it has been a life-saving, a major major event, there is no doubt about it” “It has been a great joy, to see her life enlarging, and her enjoying things, and the relationship she has been able to build with [daughter], which is terrific” “The burden on me is less, less strain, saying you know, does he have enough to eat, does he have his medication, so he takes care of that himself…it has become a blessing, in a way” |
| No longer stuck in OCD loop | “We are not in the OCD loop anymore, she manages her OCD I know it’s still there, but we are not part of it anymore, she’s just part of the family, whereas OCD was sitting in on our shoulder all the time” “It has given our lives back to a great extent too” “It’s different now I don’t see the attacks like I used to” |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Acevedo, N.; Castle, D.; Bosanac, P.; Rossell, S. Phenomenological Changes Associated with Deep Brain Stimulation for Obsessive Compulsive Disorder: A Cognitive Appraisal Model of Recovery. Brain Sci. 2023, 13, 1444. https://doi.org/10.3390/brainsci13101444
Acevedo N, Castle D, Bosanac P, Rossell S. Phenomenological Changes Associated with Deep Brain Stimulation for Obsessive Compulsive Disorder: A Cognitive Appraisal Model of Recovery. Brain Sciences. 2023; 13(10):1444. https://doi.org/10.3390/brainsci13101444
Chicago/Turabian StyleAcevedo, Nicola, David Castle, Peter Bosanac, and Susan Rossell. 2023. "Phenomenological Changes Associated with Deep Brain Stimulation for Obsessive Compulsive Disorder: A Cognitive Appraisal Model of Recovery" Brain Sciences 13, no. 10: 1444. https://doi.org/10.3390/brainsci13101444