

Can Presurgical Interhemispheric EEG Connectivity Predict Outcome in Hemispheric Surgery? A Brain Machine Learning Approach
 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Patients
- -
- Available pre-surgical clinical and EEG data during wakefulness and sleep;
- -
- Electroclinic concordance: unilateral seizure onset concordant with side of the lesion at brain MR;
- -
- Absence of signal or morphological abnormalities within the contralateral hemisphere on pre-surgical MR;
- -
- Complete disconnection evaluated at post-surgical brain MR, after multidisciplinary re-evaluation;
- -
- At least two years of post-surgical follow-up;
- -
- No previous surgeries for the treatment of epilepsy.
2.2. Presurgical Assessment
2.3. EEG Data Recording, Acquisition and Processing
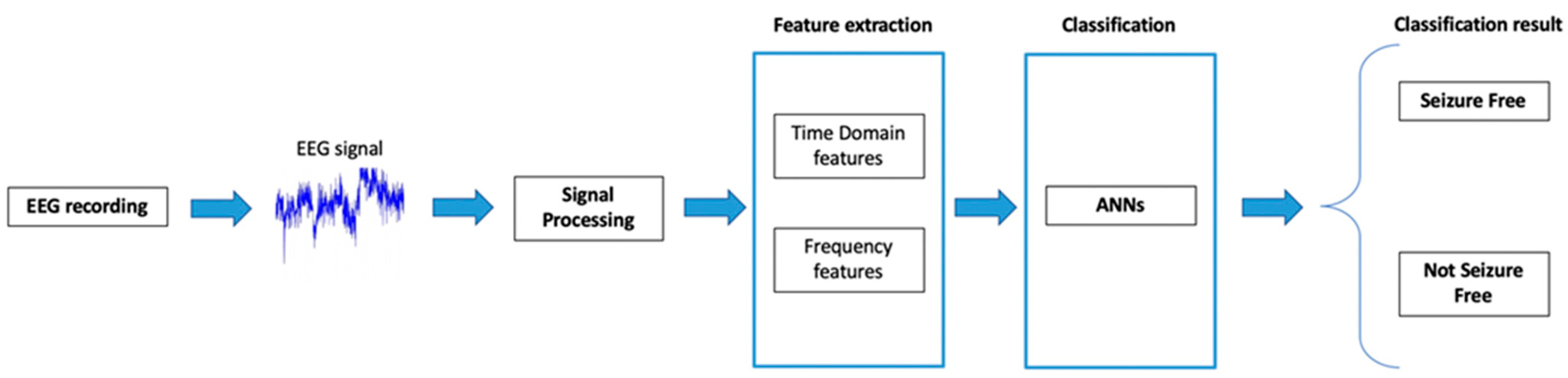
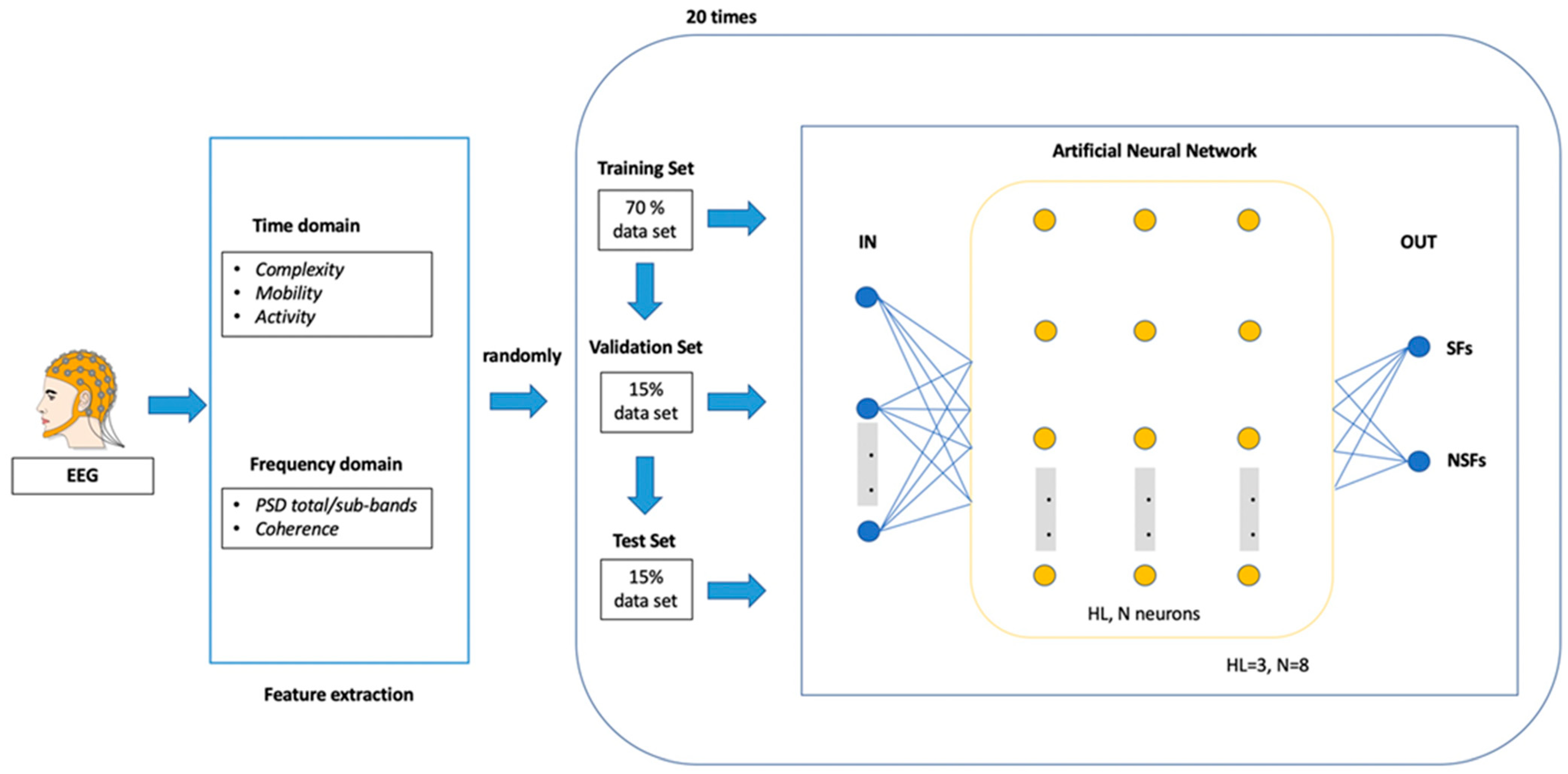
2.4. EEG Features Extraction and Classification through Artificial Neural Network (ANN)
- Dataset 1: all features;
- Dataset 2: all features calculated only in the total band frequency [0.5–45 Hz];
- Dataset 3: frequency-domain features (PSD) for every signal band;
- Dataset 4: time-domain features (Hjorth parameters) for every band;
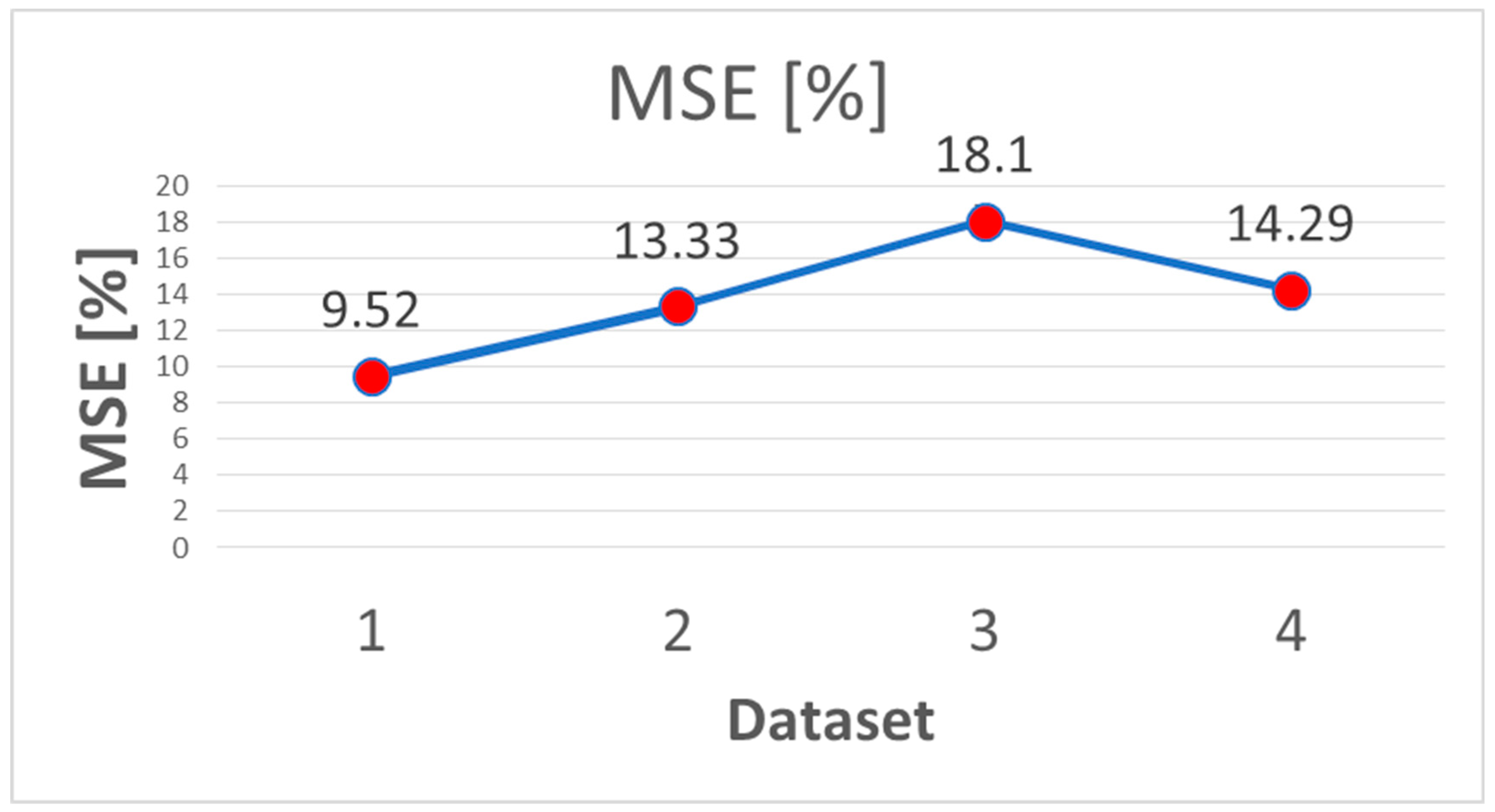
- The Mean Square Error (MSE) was calculated to select the most accurate training set.
3. Results
3.1. Clinical Results
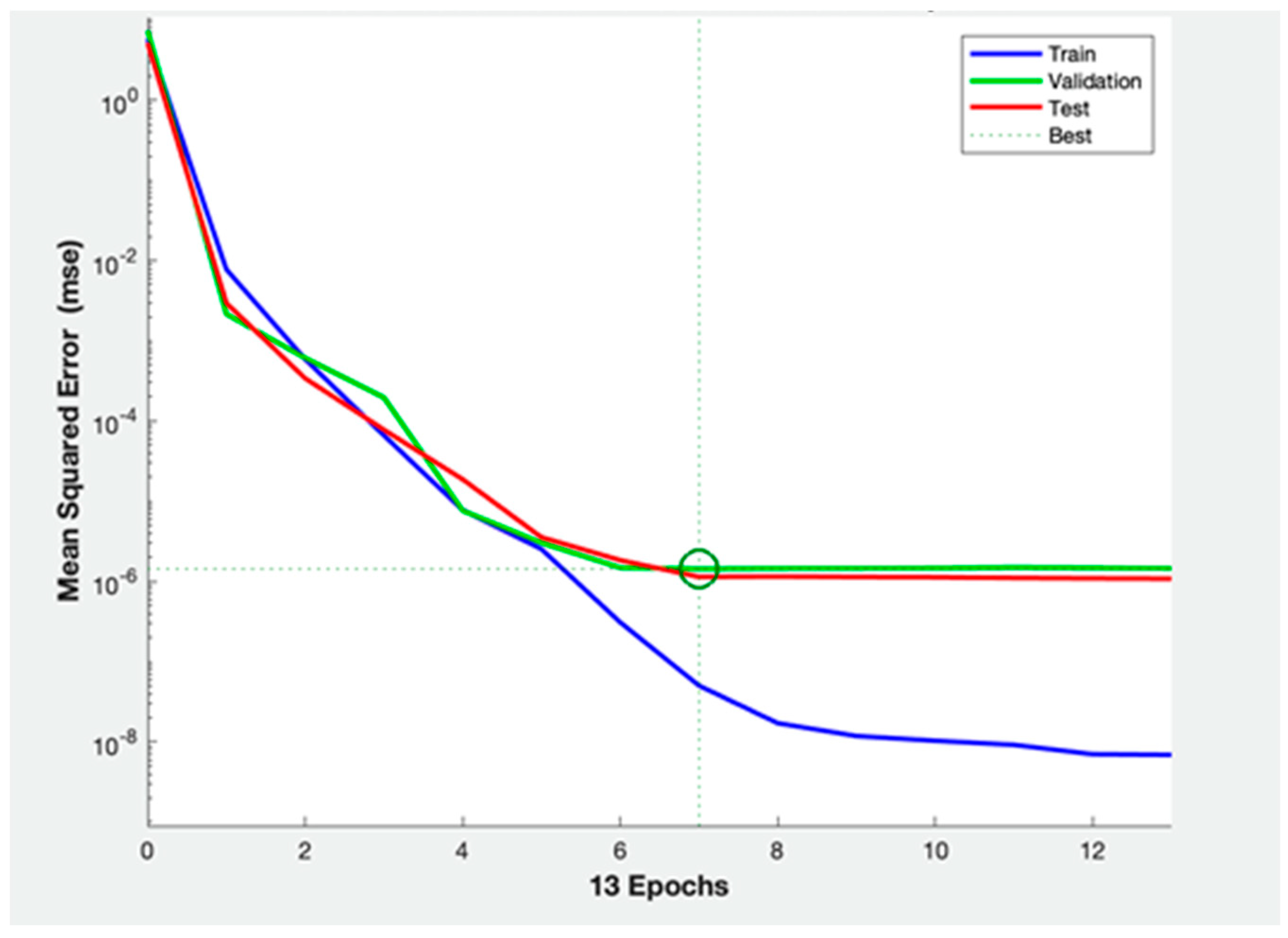
3.2. ANNs Performance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- De Ribaupierre, S.; Delalande, O. Hemispherotomy and other disconnective techniques. Neurosurg. Focus 2008, 25, E14. [Google Scholar] [CrossRef]
- Moritani, T.; Smoker, W.; Lee, H.K.; Sato, Y. Differential Diagnosis of Cerebral Hemispheric Pathology. Clin. Neuroradiol. 2011, 21, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Hu, W.-H.; Zhang, C.; Zhang, K.; Shao, X.-Q.; Zhang, J.-G. Hemispheric surgery for refractory epilepsy: A systematic review and meta-analysis with emphasis on seizure predictors and outcomes. J. Neurosurg. 2016, 124, 952–961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basheer, S.N.; Connolly, M.B.; Lautzenhiser, A.; Sherman, E.M.S.; Hendson, G.; Steinbok, P. Hemispheric Surgery in Children with Refractory Epilepsy: Seizure Outcome, Complications, and Adaptive Function. Epilepsia 2007, 48, 133–140. [Google Scholar] [CrossRef]
- Kim, J.-S.; Park, E.-K.; Shim, K.-W.; Kim, D.S. Hemispherotomy and Functional Hemispherectomy: Indications and Outcomes. J. Epilepsy Res. 2018, 8, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Moosa, A.N.; Gupta, A.; Jehi, L.; Marashly, A.; Cosmo, G.; Lachhwani, D.; Wyllie, E.; Kotagal, P.; Bingaman, W. Longitudinal seizure outcome and prognostic predictors after hemispherectomy in 170 children. Neurology 2012, 80, 253–260. [Google Scholar] [CrossRef]
- Bulteau, C.; Otsuki, T.; Delalande, O. Epilepsy surgery for hemispheric syndromes in infants: Hemimegalencepahly and hemispheric cortical dysplasia. Brain Dev. 2013, 35, 742–747. [Google Scholar] [CrossRef] [PubMed]
- Delalande, O.; Bulteau, C.; Dellatolas, G.; Fohlen, M.; Jalin, C.; Buret, V.; Viguier, D.; Dorfmüller, G.; Jambaqué, I. Vertical Parasagittal Hemispherotomy: Surgical Procedures And Clinical Long-Term Outcomes in A Population Of 83 Children. Oper. Neurosurg. 2007, 60, 19–32. [Google Scholar] [CrossRef] [PubMed]
- Marras, C.E.; Granata, T.; Franzini, A.; Freri, E.; Villani, F.; Casazza, M.; De Curtis, M.; Ragona, F.; Ferroli, P.; D’Incerti, L.; et al. Hemispherotomy and functional hemispherectomy: Indications and outcome. Epilepsy Res. 2010, 89, 104–112. [Google Scholar] [CrossRef]
- Griessenauer, C.J.; Salam, S.; Hendrix, P.; Patel, D.M.; Tubbs, R.S.; Blount, J.P.; Winkler, P.A. Hemispherectomy for treatment of refractory epilepsy in the pediatric age group: A systematic review. J. Neurosurgery: Pediatr. 2015, 15, 34–44. [Google Scholar] [CrossRef]
- Kossoff, E.H.; Vining, E.P.; Pillas, D.J.; Pyzik, P.L.; Avellino, A.M.; Carson, B.S.; Freeman, J.M. Hemispherectomy for intractable unihemispheric epilepsy Etiology vs outcome. Neurology 2003, 61, 887–890. [Google Scholar] [CrossRef] [PubMed]
- De Palma, L.; Pietrafusa, N.; Gozzo, F.; Barba, C.; Carfi-Pavia, G.; Cossu, M.; De Benedictis, A.; Genitori, L.; Giordano, F.; Russo, G.L.; et al. Outcome after hemispherotomy in patients with intractable epilepsy: Comparison of techniques in the Italian experience. Epilepsy Behav. 2019, 93, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Panigrahi, M.; Krishnan, S.S.; Vooturi, S.; Vadapalli, R.; Somayajula, S.; Jayalakshmi, S. An observational study on outcome of hemispherotomy in children with refractory epilepsy. Int. J. Surg. 2016, 36, 477–482. [Google Scholar] [CrossRef]
- Tripathi, M.; Chandra, P.S.; Padma, V.M.; Shailesh, G.; Chandreshekar, B.; Sarkar, C. Hemispherotomy for intractable epilepsy. Neurol. India 2008, 56, 127. [Google Scholar] [CrossRef] [Green Version]
- Weil, A.G.; Lewis, E.C.; Ibrahim, G.M.; Kola, O.; Tseng, C.; Zhou, X.; Lin, K.; Cai, L.; Liu, Q.; Lin, J.; et al. Hemispherectomy Outcome Prediction Scale: Development and validation of a seizure freedom prediction tool. Epilepsia 2021, 62, 1064–1073. [Google Scholar] [CrossRef] [PubMed]
- Carmant, L.; Kramer, U.; Riviello, J.; Helmers, S.; Mikati, M.; Madsen, J.; Black, P.; Lombroso, C.; Holmes, G. EEG prior to hemispherectomy: Correlation with outcome and pathology. Electroencephalogr. Clin. Neurophysiol. 1995, 94, 265–270. [Google Scholar] [CrossRef]
- Ramantani, G.; Strobl, K.; Stathi, A.; Brandt, A.; Schubert-Bast, S.; Wiegand, G.; Korinthenberg, R.; Stephani, U.; van Velthoven, V.; Zentner, J.; et al. Reoperation for Refractory Epilepsy in Childhood: A second chance for selected patients. Neurosurgery 2013, 73, 695–704. [Google Scholar] [CrossRef]
- Lew, S.M.; Koop, J.I.; Mueller, W.M.; Matthews, A.E.; Mallonee, J.C. Fifty Consecutive Hemispherectomies: Outcomes, evolution of technique, complications, and lessons learned. Neurosurgery 2014, 74, 182–195. [Google Scholar] [CrossRef] [Green Version]
- Bai, X.; Guo, J.; Killory, B.; Vestal, M.; Berman, R.; Negishi, M.; Danielson, N.; Novotny, E.J.; Constable, R.T.; Blumenfeld, H. Resting functional connectivity between the hemispheres in childhood absence epilepsy. Neurology 2011, 76, 1960–1967. [Google Scholar] [CrossRef] [Green Version]
- Masterton, R.A.; Carney, P.W.; Jackson, G.D. Cortical and thalamic resting-state functional connectivity is altered in childhood absence epilepsy. Epilepsy Res. 2012, 99, 327–334. [Google Scholar] [CrossRef]
- Varotto, G.; Visani, E.; Canafoglia, L.; Franceschetti, S.; Avanzini, G.; Panzica, F. Enhanced frontocentral EEG connectivity in photosensitive generalized epilepsies: A partial directed coherence study. Epilepsia 2011, 53, 359–367. [Google Scholar] [CrossRef] [PubMed]
- Gotman, J. Interhemispheric Relations During Bilateral Spike-and-Wave Activity. Epilepsia 1981, 22, 453–466. [Google Scholar] [CrossRef] [PubMed]
- Kawano, T.; Hattori, N.; Uno, Y.; Hatakenaka, M.; Yagura, H.; Fujimoto, H.; Yoshioka, T.; Nagasako, M.; Otomune, H.; Kitajo, K.; et al. Electroencephalographic Phase Synchrony Index as a Biomarker of Poststroke Motor Impairment and Recovery. Neurorehabilit. Neural Repair 2020, 34, 711–722. [Google Scholar] [CrossRef] [PubMed]
- Steinmann, S.; Leicht, G.; Mulert, C. The interhemispheric miscommunication theory of auditory verbal hallucinations in schizophrenia. Int. J. Psychophysiol. 2019, 145, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Isler, J.; Martien, K.; Grieve, P.; Stark, R.; Herbert, M. Reduced functional connectivity in visual evoked potentials in children with autism spectrum disorder. Clin. Neurophysiol. 2010, 121, 2035–2043. [Google Scholar] [CrossRef]
- Youh, J.; Hong, J.S.; Han, D.H.; Chung, U.S.; Min, K.J.; Lee, Y.S.; Kim, S.M. Comparison of Electroencephalography (EEG) Coherence between Major Depressive Disorder (MDD) without Comorbidity and MDD Comorbid with Internet Gaming Disorder. J. Korean Med. Sci. 2017, 32, 1160–1165. [Google Scholar] [CrossRef]
- Libbrecht, M.W.; Noble, W.S. Machine learning applications in genetics and genomics. Nat. Rev. Genet. 2015, 16, 321–332. [Google Scholar] [CrossRef] [Green Version]
- Kerr, W.T.; Anderson, A.; Lau, E.P.; Cho, A.Y.; Xia, H.; Bramen, J.; Douglas, P.K.; Braun, E.S.; Stern, J.M.; Cohen, M.S. Automated diagnosis of epilepsy using EEG power spectrum. Epilepsia 2012, 53, e189–e192. [Google Scholar] [CrossRef] [Green Version]
- Paul, Y. Various epileptic seizure detection techniques using biomedical signals: A review. Brain Inform. 2018, 5, 6. [Google Scholar] [CrossRef] [Green Version]
- Kerr, W.T.; Nguyen, S.T.; Cho, A.Y.; Lau, E.P.; Silverman, D.H.; Douglas, P.K.; Reddy, N.M.; Anderson, A.; Bramen, J.; Salamon, N.; et al. Computer-Aided Diagnosis and Localization of Lateralized Temporal Lobe Epilepsy Using Interictal FDG-PET. Front. Neurol. 2013, 4, 31. [Google Scholar] [CrossRef]
- Keihaninejad, S.; Heckemann, R.; Gousias, I.S.; Hajnal, J.; Duncan, J.S.; Aljabar, P.; Rueckert, D.; Hammers, A. Classification and Lateralization of Temporal Lobe Epilepsies with and without Hippocampal Atrophy Based on Whole-Brain Automatic MRI Segmentation. PLoS ONE 2012, 7, e33096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gleichgerrcht, E.; Munsell, B.; Bhatia, S.; Vandergrift, W.A.; Rorden, C.; McDonald, C.; Edwards, J.; Kuzniecky, R.; Bonilha, L. Deep learning applied to whole-brain connectome to determine seizure control after epilepsy surgery. Epilepsia 2018, 59, 1643–1654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Memarian, N.; Kim, S.; Dewar, S.; Engel, J.; Staba, R.J. Multimodal data and machine learning for surgery outcome prediction in complicated cases of mesial temporal lobe epilepsy. Comput. Biol. Med. 2015, 64, 67–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dian, J.A.; Colic, S.; Chinvarun, Y.; Carlen, P.L.; Bardakjian, B.L. Identification of brain regions of interest for epilepsy surgery planning using support vector machines. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 6590–6593. [Google Scholar] [CrossRef]
- Bernhardt, B.C.; Hong, S.-J.; Bernasconi, A.; Bernasconi, N. Magnetic resonance imaging pattern learning in temporal lobe epilepsy: Classification and prognostics. Ann. Neurol. 2015, 77, 436–446. [Google Scholar] [CrossRef]
- Armañanzas, R.; Alonso-Nanclares, L.; DeFelipe-Oroquieta, J.; Kastanauskaite, A.; De Sola, R.G.; Defelipe, J.; Bielza, C.; Larrañaga, P. Machine Learning Approach for the Outcome Prediction of Temporal Lobe Epilepsy Surgery. PLoS ONE 2013, 8, e62819. [Google Scholar] [CrossRef] [Green Version]
- Fisher, R.S.; Cross, J.H.; French, J.A.; Higurashi, N.; Hirsch, E.; Jansen, F.E.; Lagae, L.; Moshé, S.L.; Peltola, J.; Perez, E.R.; et al. Operational classification of seizure types by the International League Against Epilepsy: Position Paper of the ILAE Commission for Classification and Terminology. Epilepsia 2017, 58, 522–530. [Google Scholar] [CrossRef] [Green Version]
- Engel, J.; Van Ness, P.C.; Rasmussen, T.B.O.L. Outcome with respect to epileptic seizures. In Surgical Treatment of the Epilepsies, 2nd ed.; Engel, J., Ed.; Press NYR: New York, NY, USA, 1993; pp. 609–621. [Google Scholar]
- Bandarabadi, M.; Teixeira, C.A.; Rasekhi, J.; Dourado, A. Epileptic seizure prediction using relative spectral power features. Clin. Neurophysiol. 2015, 126, 237–248. [Google Scholar] [CrossRef]
- Faust, O.; Acharya, U.R.; Min, L.C.; Sputh, B.H.C. Automatic identification of epileptic and background eeg signals using frequency domain parameters. Int. J. Neural Syst. 2010, 20, 159–176. [Google Scholar] [CrossRef] [Green Version]
- Oh, S.-H.; Lee, Y.-R.; Kim, H.-N. A Novel EEG Feature Extraction Method Using Hjorth Parameter. Int. J. Electron. Electr. Eng. 2014, 2, 106–110. [Google Scholar] [CrossRef]
- Yotov, K.; Hadzhikolev, E.; Hadzhikoleva, S. Determining the Number of Neurons in Artificial Neural Networks for Approximation, Trained with Algorithms Using the Jacobi Matrix. TEM J. 2020, 9, 1320–1329. [Google Scholar] [CrossRef]
- Demuru, M.; La Cava, S.M.; Pani, S.M.; Fraschini, M. A comparison between power spectral density and network metrics: An EEG study. Biomed. Signal Process. Control. 2019, 57, 101760. [Google Scholar] [CrossRef]
- Harpale, V.K.; Bairagi, V.K. Time and frequency domain analysis of EEG signals for seizure detection: A review. In Proceedings of the 2016 International Conference on Microelectronics, Computing and Communications (MicroCom), Durgapur, India, 23–25 January 2016. [Google Scholar] [CrossRef]
- Vidaurre, C.; Krämer, N.; Blankertz, B.; Schlögl, A. Time Domain Parameters as a feature for EEG-based Brain–Computer Interfaces. Neural Netw. 2009, 22, 1313–1319. [Google Scholar] [CrossRef] [PubMed]
- Feis, D.-L.; Schoene-Bake, J.-C.; Elger, C.; Wagner, J.; Tittgemeyer, M.; Weber, B. Prediction of post-surgical seizure outcome in left mesial temporal lobe epilepsy. NeuroImage Clin. 2013, 2, 903–911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parker, C.S.; Clayden, J.D.; Cardoso, M.J.; Rodionov, R.; Duncan, J.S.; Scott, C.; Diehl, B.; Ourselin, S. Structural and effective connectivity in focal epilepsy. NeuroImage Clin. 2018, 17, 943–952. [Google Scholar] [CrossRef] [PubMed]
- Antony, A.R.; Alexopoulos, A.V.; Gonzalez-Martinez, J.A.; Mosher, J.C.; Jehi, L.; Burgess, R.C.; So, N.K.; Galán, R.F. Functional Connectivity Estimated from Intracranial EEG Predicts Surgical Outcome in Intractable Temporal Lobe Epilepsy. PLoS ONE 2013, 8, e77916. [Google Scholar] [CrossRef] [PubMed]
- Tomlinson, S.B.; Porter, B.E.; Marsh, E.D. Interictal network synchrony and local heterogeneity predict epilepsy surgery outcome among pediatric patients. Epilepsia 2017, 58, 402–411. [Google Scholar] [CrossRef] [Green Version]
- Abbasi, B.; Goldenholz, D.M. Machine learning applications in epilepsy. Epilepsia 2019, 60, 2037–2047. [Google Scholar] [CrossRef]
- Grigsby, J.; Kramer, R.E.; Schneiders, J.L.; Gates, J.R.; Smith, W.B. Predicting Outcome of Anterior Temporal Lobectomy Using Simulated Neural Networks. Epilepsia 1998, 39, 61–66. [Google Scholar] [CrossRef]
- Arle, J.E.; Perrine, K.; Devinsky, O.; Doyle, W.K. Neural network analysis of preoperative variables and outcome in epilepsy surgery. J. Neurosurg. 1999, 90, 998–1004. [Google Scholar] [CrossRef] [Green Version]
- Rasheed, K.; Qayyum, A.; Qadir, J.; Sivathamboo, S.; Kwan, P.; Kuhlmann, L.; O’Brien, T.; Razi, A. Machine Learning for Predicting Epileptic Seizures Using EEG Signals: A Review. IEEE Rev. Biomed. Eng. 2021, 14, 139–155. [Google Scholar] [CrossRef]
- Kerr, W.T.; Douglas, P.K.; Anderson, A.; Cohen, M.S. The utility of data-driven feature selection: Re: Chu et al. 2012. Neuroimage 2014, 84, 1107–1110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirchi, N.; Warsi, N.M.; Zhang, F.; Wong, S.M.; Suresh, H.; Mithani, K.; Erdman, L.; Ibrahim, G.M. Decoding Intracranial EEG With Machine Learning: A Systematic Review. Front. Hum. Neurosci. 2022, 16, 399. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type | Name | Description |
|---|---|---|
| Time Domain | Complexity | Hjorth parameters quantify the dynamical properties of signal |
| Mobility | ||
| Activity | ||
| Frequency Domain | Power Spectrum (PSD) | PSD quantify the signal power associated to specific frequency range |
| ANNs | HL [1,2,3] | N | Architecture |
|---|---|---|---|
| I | 1 | 8 | 8 |
| II | 2 | 8 × 2 | 8 + 8 |
| III | 3 | 5 | 5 |
| IV | 1 | 5 × 2 | 5 + 5 |
| V | 2 | 4 | 4 |
| VI | 3 | 4 × 2 | 4 + 4 |
| VII | 1 | 3 | 3 |
| VIII | 2 | 3 × 2 | 3 + 3 |
| IX | 3 | 2 | 2 |
| Patient | Age at Surgery | Etiology | Histology | Outcome | Follow-Up (Years) |
|---|---|---|---|---|---|
| 1 | 1.3 | HME | FCD Ic | IA | 12.6 |
| 2 | 14.8 | Rasmussen | Inflammatory infiltrate | IV | 10.1 |
| 3 | 4.7 | Perinatal ischemic injury | Gliosis | IA | 4.8 |
| 4 | 17.7 | Rasmussen | Gliosis | IA | 7.6 |
| 5 | 2.9 | HME | FCD IIa | IA | 5.7 |
| 6 | 0.2 | HME | FCD IIa | IA | 5.8 |
| 7 | 4.5 | Ischemic injury | Gliosis | IA | 7.3 |
| 8 | 16.8 | Vascular congenital abnormality | Gliosis | II | 5.7 |
| 9 | 17.0 | Perinatal ischemic injury | Gliosis | IV | 7.5 |
| 10 | 7.0 | Perinatal ischemic injury | Gliosis | IA | 6.8 |
| 11 | 4.1 | Hemispheric MCD | FCD Ic | III | 4.4 |
| 12 | 0.2 | HME | FCD IIa | IA | 5.1 |
| 13 | 12.0 | Post-infectious ischemic injury | Gliosis | IA | 5.3 |
| 14 | 11.7 | Perinatal ischemic injury | Gliosis | ID | 4.9 |
| 15 | 7.0 | Rasmussen | Inflammatory infiltrate | IA | 4.8 |
| 16 | 8.8 | Rasmussen | Inflammatory infiltrate | IA | 2.3 |
| 17 | 17.9 | Rasmussen | Inflammatory infiltrate | IA | 2.9 |
| 18 | 0.7 | Perinatal ischemic injury | Gliosis | IA | 2.9 |
| 19 | 3.6 | Rasmussen | Inflammatory infiltrate | ID | 2.4 |
| 20 | 2.0 | Hemispheric MCD | Neuronal heterotopia | IA | 2.4 |
| 21 | 11.1 | Rasmussen | Inflammatory infiltrate | IA | 2.3 |
| Architecture | Accuracy (P%) | Specificity (%) | Sensitivity (%) |
|---|---|---|---|
| I | 43.333 ± 14.91 | 61.000 ± 29.66 | 10.000 ± 22.36 |
| II | 73.333 ± 22.36 | 40.000 ± 54.77 | 40.000 ± 41.83 |
| III | 63.333 ± 29.81 | 86.667 ± 29.81 | 36.667 ± 41.50 |
| IV | 53.333 ± 18.26 | 83.333 ± 23.57 | 11.667 ± 16.24 |
| V | 66.667 ± 11.79 | 82.000 ± 20.49 | 20.000 ± 29.81 |
| VI | 63.333 ± 13.94 | 76.000 ± 43.36 | 25.000 ± 27.64 |
| VII | 63.333 ± 7.45 | 74.667 ± 25.56 | 40.000 ± 43.46 |
| VIII | 63.333 ± 24.72 | 63.333 ± 22.85 | 40.000 ± 54.77 |
| IX | 56.667 ± 9.13 | 65.667 ± 15.44 | 26.667 ± 43.46 |
| Mean of Iteration | |||
|---|---|---|---|
| ANNs | SF (%) | NSF (%) | |
| II | SF | 85 | 60 |
| NSF | 15 | 40 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pepi, C.; Mercier, M.; Carfì Pavia, G.; de Benedictis, A.; Vigevano, F.; Rossi-Espagnet, M.C.; Falcicchio, G.; Marras, C.E.; Specchio, N.; de Palma, L. Can Presurgical Interhemispheric EEG Connectivity Predict Outcome in Hemispheric Surgery? A Brain Machine Learning Approach. Brain Sci. 2023, 13, 71. https://doi.org/10.3390/brainsci13010071
Pepi C, Mercier M, Carfì Pavia G, de Benedictis A, Vigevano F, Rossi-Espagnet MC, Falcicchio G, Marras CE, Specchio N, de Palma L. Can Presurgical Interhemispheric EEG Connectivity Predict Outcome in Hemispheric Surgery? A Brain Machine Learning Approach. Brain Sciences. 2023; 13(1):71. https://doi.org/10.3390/brainsci13010071
Chicago/Turabian StylePepi, Chiara, Mattia Mercier, Giusy Carfì Pavia, Alessandro de Benedictis, Federico Vigevano, Maria Camilla Rossi-Espagnet, Giovanni Falcicchio, Carlo Efisio Marras, Nicola Specchio, and Luca de Palma. 2023. "Can Presurgical Interhemispheric EEG Connectivity Predict Outcome in Hemispheric Surgery? A Brain Machine Learning Approach" Brain Sciences 13, no. 1: 71. https://doi.org/10.3390/brainsci13010071