
Serum microRNA miR-491-5p/miR-206 Is Correlated with Poor Outcomes/Spontaneous Hemorrhagic Transformation after Ischemic Stroke: A Case Control Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Baseline Data Collection
2.3. Blood Sampling
2.4. Selection and Assessment of Candidate MMP-9-Related MiRNAs
2.5. Extraction of miRNAs, Reverse Transcription and qRT–PCR
2.6. Outcome Measures
2.7. Statistical Analyses
3. Results
3.1. Baseline Information
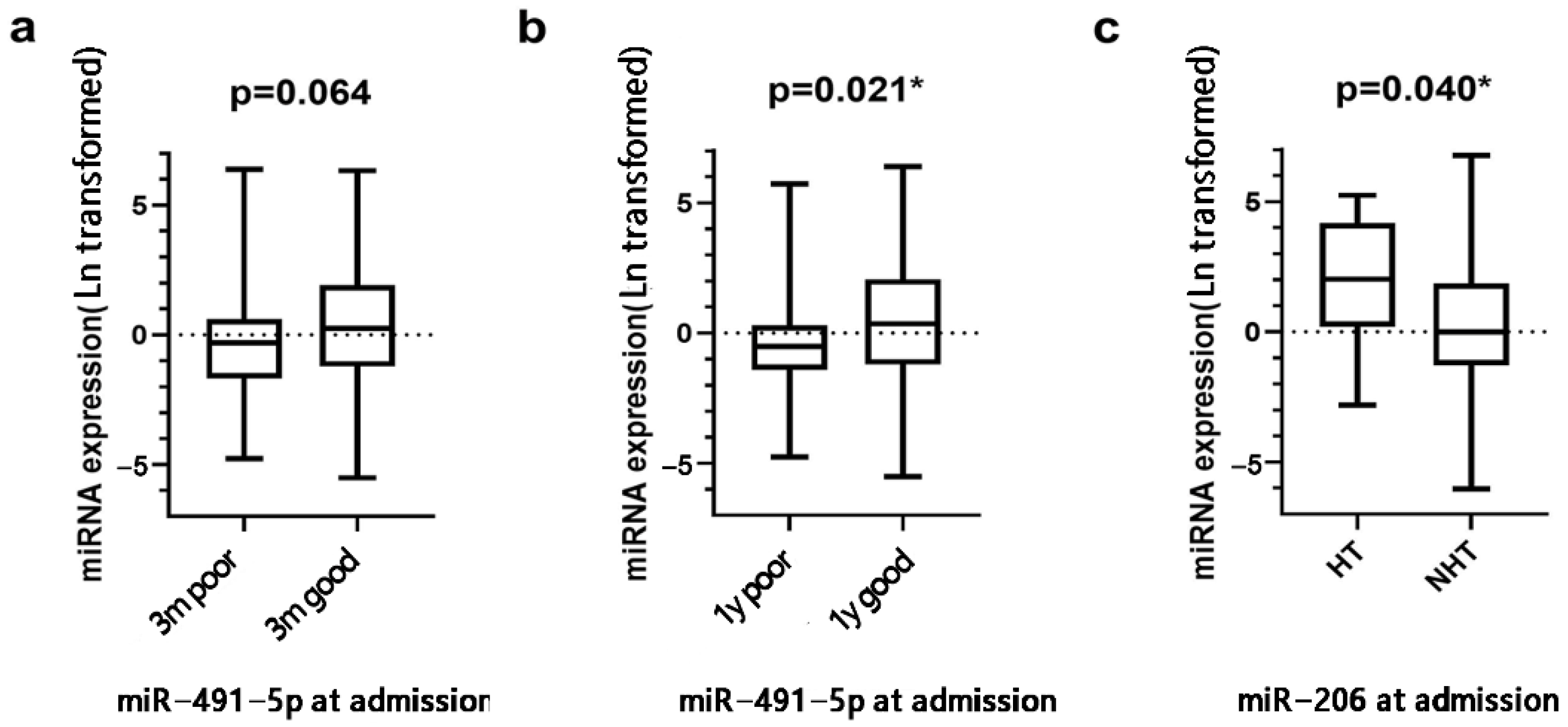
3.2. Correlation between miRNA Expression Levels and Functional Outcomes
3.3. Correlation between miRNA Expression Levels and Spontaneous HT
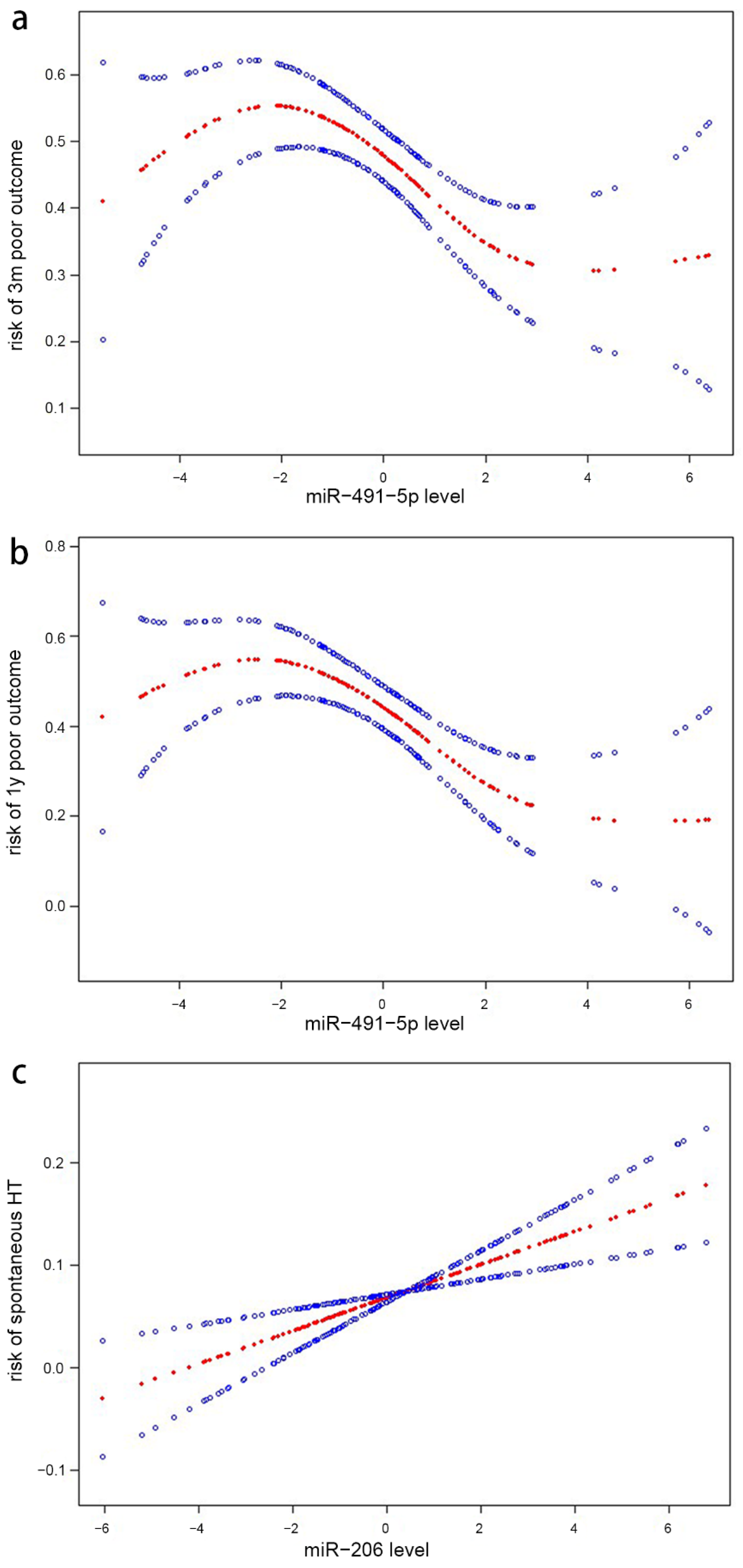
3.4. Analyses of the Nonlinear Correlation between microRNA Levels and Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wu, S.; Wu, B.; Liu, M.; Chen, Z.; Wang, W.; Anderson, C.S.; Sandercock, P.; Wang, Y.; Huang, Y.; Cui, L.; et al. Stroke in China: Advances and challenges in epidemiology, prevention, and management. Lancet. Neurol. 2019, 18, 394–405. [Google Scholar] [CrossRef]
- Wang, W.; Jiang, B.; Sun, H.; Ru, X.; Sun, D.; Wang, L.; Wang, L.; Jiang, Y.; Li, Y.; Wang, Y.; et al. Prevalence, Incidence, and Mortality of Stroke in China: Results from a Nationwide Population-Based Survey of 480 687 Adults. Circulation 2017, 135, 759–771. [Google Scholar] [CrossRef] [PubMed]
- Fullerton, J.L.; Thomas, J.M.; Gonzalez-Trueba, L.; Trivett, C.; van Kralingen, J.C.; Allan, S.M.; Quinn, T.J.; Work, L.M. Systematic review: Association between circulating microRNA expression & stroke. J. Cereb. Blood Flow Metab. 2022, 42, 935–951. [Google Scholar] [CrossRef]
- Volný, O.; Kašičková, L.; Coufalová, D.; Cimflová, P.; Novák, J. microRNAs in Cerebrovascular Disease. Adv. Exp. Med. Biol. 2015, 888, 155–195. [Google Scholar] [CrossRef] [PubMed]
- Castellanos, M.; Sobrino, T.; Millán, M.; García, M.; Arenillas, J.; Nombela, F.; Brea, D.; de la Ossa, N.P.; Serena, J.; Vivancos, J.; et al. Serum cellular fibronectin and matrix metalloproteinase-9 as screening biomarkers for the prediction of parenchymal hematoma after thrombolytic therapy in acute ischemic stroke: A multicenter confirmatory study. Stroke 2007, 38, 1855–1859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaturvedi, M.; Kaczmarek, L. Mmp-9 inhibition: A therapeutic strategy in ischemic stroke. Mol. Neurobiol. 2014, 49, 563–573. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Wei, C.; Deng, L.; Wang, Z.; Song, M.; Xiong, Y.; Liu, M. The Accuracy of Serum Matrix Metalloproteinase-9 for Predicting Hemorrhagic Transformation After Acute Ischemic Stroke: A Systematic Review and Meta-Analysis. J. Stroke Cereb. Dis. 2018, 27, 1653–1665. [Google Scholar] [CrossRef] [PubMed]
- Zheng, L.; Xiong, Y.; Liu, J.; Yang, X.; Wang, L.; Zhang, S.; Liu, M.; Wang, D. MMP-9-Related microRNAs as Prognostic Markers for Hemorrhagic Transformation in Cardioembolic Stroke Patients. Front. Neurol. 2019, 10, 945. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.P., Jr.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E., 3rd. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devaux, Y.; Dankiewicz, J.; Salgado-Somoza, A.; Stammet, P.; Collignon, O.; Gilje, P.; Gidlöf, O.; Zhang, L.; Vausort, M.; Hassager, C.; et al. Association of Circulating MicroRNA-124-3p Levels With Outcomes After Out-of-Hospital Cardiac Arrest: A Substudy of a Randomized Clinical Trial. JAMA Cardiol. 2016, 1, 305–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hacke, W.; Kaste, M.; Fieschi, C.; Toni, D.; Lesaffre, E.; von Kummer, R.; Boysen, G.; Bluhmki, E.; Höxter, G.; Mahagne, M.H.; et al. Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke. The European Cooperative Acute Stroke Study (ECASS). JAMA 1995, 274, 1017–1025. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B (Methodol.) 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Wang, C.; Deng, L.; Qiu, S.; Bian, H.; Wang, L.; Li, Y.; Liu, M.; Wu, B. Serum Albumin is negatively associated with hemorrhagic transformation in acute ischemic stroke patients. Cereb. Dis. 2019, 47, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Qi, L. miR-124 is downregulated in serum of acute cerebral infarct patients and shows diagnostic and prognostic value. Clin. Appl. Thromb. Hemost. 2021, 27, 10760296211035446. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.Z.; Wang, J.; Xu, F. Circulating miR-29b and miR-424 as Prognostic Markers in Patients with Acute Cerebral Infarction. Clin. Lab. 2017, 63, 1667–1674. [Google Scholar] [CrossRef]
- Rainer, T.H.; Leung, L.Y.; Chan, C.P.Y.; Leung, Y.K.; Abrigo, J.M.; Wang, D.; Graham, C.A. Plasma miR-124-3p and miR-16 concentrations as prognostic markers in acute stroke. Clin. Biochem. 2016, 49, 663–668. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Song, Y.; Huang, J.; Qu, M.; Zhang, Y.; Geng, J.; Zhang, Z.; Liu, J.; Yang, G.Y. Increased Circulating Exosomal miRNA-223 Is Associated with Acute Ischemic Stroke. Front. Neurol. 2017, 8, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scherrer, N.; Fays, F.; Mueller, B.; Luft, A.; Fluri, F.; Christ-Crain, M.; Devaux, Y.; Katan, M. MicroRNA 150-5p Improves Risk Classification for Mortality within 90 Days after Acute Ischemic Stroke. J. Stroke 2017, 19, 323–332. [Google Scholar] [CrossRef] [Green Version]
- Suofu, Y.; Wang, X.; He, Y.; Li, F.; Zhang, Y.; Carlisle, D.L.; Friedlander, R.M. Mir-155 knockout protects against ischemia/reperfusion-induced brain injury and hemorrhagic transformation. Neuroreport 2020, 31, 235–239. [Google Scholar] [CrossRef]
- Ramos-Fernandez, M.; Bellolio, M.F.; Stead, L.G. Matrix metalloproteinase-9 as a marker for acute ischemic stroke: A systematic review. J. Stroke Cereb. Dis. 2011, 20, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Deng, L.; Yuan, R.; Liu, J.; Li, Y.; Liu, M. Association of Matrix Metalloproteinase 9 and Cellular Fibronectin and Outcome in Acute Ischemic Stroke: A Systematic Review and Meta-Analysis. Front. Neurol. 2020, 11, 523506. [Google Scholar] [CrossRef]
- Yuan, R.; Tan, S.; Wang, D.; Wu, S.; Cao, X.; Zhang, S.; Wu, B.; Liu, M. Predictive value of plasma matrix metalloproteinase-9 concentrations for spontaneous haemorrhagic transformation in patients with acute ischaemic stroke: A cohort study in Chinese patients. J. Clin. Neurosci. 2018, 58, 108–112. [Google Scholar] [CrossRef]
- Ro, S.; Park, C.; Young, D.; Sanders, K.M.; Yan, W. Tissue-dependent paired expression of miRNAs. Nucleic Acids Res. 2007, 35, 5944–5953. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Zhang, G.; Yu, K.; Zhang, X.; Jiang, A. Circ_0003204 knockdown protects endothelial cells against oxidized low-density lipoprotein-induced injuries by targeting the miR-491-5p-ICAM1 pathway. J. Thromb. Thrombolysis 2022, 53, 302–312. [Google Scholar] [CrossRef]
- Meng, W.; Cao, X.; Sun, W.; Zheng, L.; Fan, B.; Zhou, S.; Liu, H.; Wang, H.; Wang, W.; Liu, X. A functional polymorphism at the miR-491-5p binding site in the 3′-untranslated region of the MMP-9 gene increases the risk of developing ventilator-associated pneumonia. Int. J. Mol. Med. 2021, 48, 217. [Google Scholar] [CrossRef]
- Liao, Y.; Zhu, E.; Zhou, W. Ox-LDL Aggravates the Oxidative Stress and Inflammatory Responses of THP-1 Macrophages by Reducing the Inhibition Effect of miR-491-5p on MMP-9. Front. Cardiovasc. Med. 2021, 8, 697236. [Google Scholar] [CrossRef]
- Yuan, M.; Zhan, Q.; Duan, X.; Song, B.; Zeng, S.; Chen, X.; Yang, Q.; Xia, J. A functional polymorphism at miR-491-5p binding site in the 3′-UTR of MMP-9 gene confers increased risk for atherosclerotic cerebral infarction in a Chinese population. Atherosclerosis 2013, 226, 447–452. [Google Scholar] [CrossRef]
- McCarthy, J.J. MicroRNA-206: The skeletal muscle-specific myomiR. Biochim. Biophys. Acta 2008, 1779, 682–691. [Google Scholar] [CrossRef] [Green Version]
- He, X.W.; Shi, Y.H.; Zhao, R.; Liu, Y.S.; Li, G.F.; Hu, Y.; Chen, W.; Cui, G.H.; Su, J.J.; Liu, J.R. Plasma Levels of miR-125b-5p and miR-206 in Acute Ischemic Stroke Patients After Recanalization Treatment: A Prospective Observational Study. J. Stroke Cereb. Dis. 2019, 28, 1654–1661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, F.; Xing, J. Circulating pro-angiogenic and anti-angiogenic microRNA expressions in patients with acute ischemic stroke and their association with disease severity. Neurol. Sci. 2017, 38, 2015–2023. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.J.; Lim, K.Y.; Kaur, P.; Sepramaniam, S.; Armugam, A.; Wong, P.T.; Jeyaseelan, K. microRNAs Involved in Regulating Spontaneous Recovery in Embolic Stroke Model. PLoS ONE 2013, 8, e66393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, R.; Hu, Y.; Song, G.; Hao, C.J.; Cui, Y.; Xia, H.F.; Ma, X. MiR-206 regulates neural cells proliferation and apoptosis via Otx2. Cell. Physiol. Biochem. 2012, 29, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Stahlhut, C.; Suárez, Y.; Lu, J.; Mishima, Y.; Giraldez, A.J. miR-1 and miR-206 regulate angiogenesis by modulating VegfA expression in zebrafish. Development 2012, 139, 4356–4364. [Google Scholar] [CrossRef] [Green Version]
- Fu, X.; Zeng, L.; Liu, Z.; Ke, X.; Lei, L.; Li, G. MicroRNA-206 regulates the secretion of inflammatory cytokines and MMP9 expression by targeting TIMP3 in Mycobacterium tuberculosis-infected THP-1 human macrophages. Biochem. Biophys. Res. Commun. 2016, 477, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Serena, J.; Blanco, M.; Castellanos, M.; Silva, Y.; Vivancos, J.; Moro, M.A.; Leira, R.; Lizasoain, I.; Castillo, J.; Dávalos, A. The prediction of malignant cerebral infarction by molecular brain barrier disruption markers. Stroke 2005, 36, 1921–1926. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Overall (n = 215) | Poor 3 m Outcome (n = 106) | Good 3 m Outcome (n = 109) | p Value | Poor 1 y Outcome (n = 88) | Good 1 y Outcome (n = 127) | p Value | ||
|---|---|---|---|---|---|---|---|---|
| Age, years, mean (SD) | 66.69 (14.52) | 69.93 (13.91) | 63.53 (14.46) | 0.001 * | 71.08 (11.53) | 61.21 (15.65) | 0.001 * | |
| Female, n (%) | 83 (38.6) | 44 (41.5) | 39 (35.8) | 0.47 | 50 (56.8) | 82 (64.6) | 0.315 | |
| Onset to admission, h, median [IQR] | 21.00 [5.00, 45.00] | 21.00 [4.63, 45.00] | 21.00 [6.50, 45.00] | 0.290 | 21.00 [2.25, 45.00] | 21.00 [8.00, 45.00] | 0.280 | |
| Onset to blood sampling, h, median [IQR] | 25.68 [5.75, 43.08] | 21.20 [7.41, 41.27] | 27.07 [4.91, 45.22] | 0.526 | 20.94 [4.32, 41.84] | 26.64 [7.88, 44.58] | 0.228 | |
| GCS on admission, median [IQR] | 15.00 [13.00, 15.00] | 14.00 [10.25, 15.00] | 15.00 [14.00, 15.00] | <0.001 * | 13.00 [10.00, 15.00] | 15.00 [14.00, 15.00] | <0.001 * | |
| NIHSS on admission, median [IQR] | 6.00 [3.00, 12.00] | 11.00 [4.00, 15.75] | 4.00 [2.00, 7.00] | <0.001 * | 12.00 [6.00, 16.25] | 4.00 [2.00, 7.00] | <0.001 * | |
| Axillary temperature, °C, mean (SD) | 36.53 (0.44) | 36.64 (0.05) | 36.40 (0.03) | <0.001 * | 36.67 (0.06) | 36.41 (0.03) | <0.001 * | |
| History of risk factors | ||||||||
| Hypertension, n (%) | 124 (57.7) | 60 (56.6) | 64 (58.7) | 0.861 | 54 (61.4) | 70 (55.1) | 0.441 | |
| DM, n (%) | 53 (24.7) | 29 (27.4) | 24 (22.0) | 0.453 | 28 (31.8) | 25 (19.7) | 0.062 | |
| Hyperlipidemia, n (%) | 8 (3.7) | 3 (2.8) | 5 (4.6) | 0.749 | 4 (4.5) | 4 (3.1) | 0.869 | |
| AF, n (%) | 31 (14.4) | 18 (17.0) | 13 (11.9) | 0.389 | 17 (19.3) | 14 (11.0) | 0.132 | |
| Acute myocardial infarction, n (%) | 4 (1.9) | 4 (3.8) | 0 (0.0) | 0.123 | 4 (4.5) | 0 (0.0) | 0.056 | |
| Valvular heart disease, n (%) | 11 (5.1) | 6 (5.7) | 5 (4.6) | 0.962 | 6 (6.8) | 5 (3.9) | 0.53 | |
| Transient ischemic attack, n (%) | 6 (2.8) | 3 (2.8) | 3 (2.8) | 1 | 2 (2.3) | 4 (3.1) | 1 | |
| AIS, n (%) | 43 (20.0) | 23 (21.7) | 20 (18.3) | 0.658 | 23 (26.1) | 20 (15.7) | 0.089 | |
| Hemorrhagic stroke, n (%) | 3 (1.4) | 1 (0.9) | 2 (1.8) | 1 | 2 (2.3) | 1 (0.8) | 0.748 | |
| Therapies before admission | ||||||||
| Antiplatelet therapy, n (%) | 28 (13.0) | 14 (13.2) | 14 (12.8) | 1 | 13 (14.8) | 15 (11.8) | 0.668 | |
| Lipid lowering, n (%) | 19 (8.8) | 8 (7.5) | 11 (10.1) | 0.677 | 7 (8.0) | 12 (9.4) | 0.892 | |
| Anticoagulant therapy, n (%) | 10 (4.7) | 3 (2.8) | 7 (6.4) | 0.354 | 4 (4.5) | 6 (4.7) | 1 | |
| TOAST classification, n (%) | 0.089 | 0.005 * | ||||||
| LAA | 62 (28.8) | 33 (31.1) | 29 (26.6) | 28 (31.8) | 34 (26.8) | |||
| SAO | 49 (22.8) | 16 (15.1) | 33 (30.3) | 10 (11.4) | 39 (30.7) | |||
| CE | 58 (27.0) | 34 (32.1) | 24 (22.0) | 32 (36.4) | 26 (20.5) | |||
| SOE | 5 (2.3) | 3 (2.8) | 2 (1.8) | 1 (1.1) | 4 (3.1) | |||
| SUE | 41 (19.1) | 20 (18.9) | 21 (19.3) | 17 (19.3) | 24 (18.9) | |||
| ECASS classification, n (%) | 0.27 | 0.762 | ||||||
| No | 200 (93.0) | 95 (89.6) | 105 (96.3) | 80 (90.9) | 120 (94.5) | |||
| HI1 | 6 (2.8) | 4 (3.8) | 2 (1.8) | 3 (3.4) | 3 (2.4) | |||
| HI2 | 5 (2.3) | 4 (3.8) | 1 (0.9) | 3 (3.4) | 2 (1.6) | |||
| PH1 | 4 (1.9) | 3 (2.8) | 1 (0.9) | 2 (2.3) | 2 (1.6) | |||
| PH2 | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |||
| Levels of miRNA expression, fold difference | ||||||||
| miR-21-5p, median [IQR] | 0.82 [0.18, 4.10] | 0.89 [0.17, 4.66] | 0.77 [0.21, 2.53] | 0.635 | 0.69 [0.17, 2.23] | 0.88 [0.17, 6.10] | 0.363 | |
| miR-491-5p, median [IQR]) | 0.98 [0.29, 2.45] | 0.72 [0.21, 1.62] | 1.25 [0.30, 4.98] | 0.064 | 0.60 [0.27, 1.33] | 1.43 [0.31, 7.45] | 0.021 * | |
| miR-3123, median [IQR] | 1.60 [0.08, 12.26] | 1.11 [0.04, 15.79] | 1.92 [0.15, 10.71] | 0.755 | 0.78 [0.02, 9.23] | 1.98 [0.09, 14.37] | 0.326 | |
| miR-206, median [IQR] | 1.15 [0.29, 7.57] | 1.51 [0.35, 7.47] | 0.84 [0.25, 9.00] | 0.476 | 1.75 [0.36, 9.85] | 1.95 [0.51, 26.62] | 0.414 | |
| 3 Months | |||||||
|---|---|---|---|---|---|---|---|
| Unadjusted | Model 1 | Model 2 | |||||
| OR (95% CI) | p Value | OR (95% CI) | p Value | OR (95% CI) | p Value | Corrected p Value # | |
| miR-21-5p † | 1.01 (0.92–1.12) | 0.785 | 1.00 (0.95–1.06) | 0.947 | 1.00 (0.95–1.05) | 0.992 | 0.992 |
| miR-491-5p † | 0.90 (0.77–1.05) | 0.177 | 0.93 (0.85–1.02) | 0.145 | 0.93 (0.85–1.03) | 0.147 | 0.588 |
| miR-3123 † | 0.97 (0.88–1.07) | 0.545 | 1.00 (0.95–1.04) | 0.901 | 1.00 (0.95–1.05) | 0.958 | 0.992 |
| miR-206 † | 1.03 (0.91–1.16) | 0.684 | 1.01 (0.96–1.07) | 0.640 | 1.01 (0.95–1.07) | 0.783 | 0.992 |
| 1 Year | |||||||
| Unadjusted | Model 1 | Model 2 | |||||
| OR (95% CI) | p Value | OR (95% CI) | p Value | OR (95% CI) | p Value | Corrected p Value # | |
| miR-21-5p † | 0.99 (0.900–1.100) | 0.921 | 0.98 (0.93–1.03) | 0.499 | 0.98 (0.93–1.03) | 0.456 | 0.347 |
| miR-491-5p † | 0.84 (0.71–0.99) | 0.036 * | 0.90 (0.82–0.98) | 0.012 * | 0.90 (0.82–0.98) | 0.014 * | 0.044 * |
| miR-3123 † | 0.93 (0.84–1.03) | 0.167 | 0.97 (0.92–1.02) | 0.282 | 0.98 (0.93–1.03) | 0.348 | 0.347 |
| miR-206 † | 0.98 (0.87–1.10) | 0.712 | 0.98 (0.92–1.05) | 0.570 | 0.98 (0.84–1.15) | 0.476 | 0.347 |
| Unadjusted | Model 1 | ||||
|---|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | ||
| miR-21-5p † | 0.98 (0.81–1.19) | 0.848 | 0.93 (0.76–1.13) | 0.463 | |
| miR-491-5p † | 1.05 (0.80–1.38) | 0.725 | 1.01 (0.76–1.34) | 0.932 | |
| miR-3123 † | 0.91 (0.75–1.09) | 0.289 | 0.91 (0.76–1.09) | 0.324 | |
| miR-206† | 1.25 (1.00–1.57) | 0.048 * | 1.45 (1.09–1.94) | 0.012 * | |
| Model 2 | Model 3 | ||||
| OR (95% CI) | p Value | OR (95% CI) | p Value | Corrected p Value # | |
| miR-21-5p † | 0.88 (0.71–1.09) | 0.259 | 0.85 (0.67–1.07) | 0.165 | 0.330 |
| miR-491-5p † | 1.04 (0.77–1.42) | 0.784 | 1.08 (0.78–1.49) | 0.649 | 0.649 |
| miR-3123 † | 0.91 (0.76–1.10) | 0.338 | 0.93 (0.77–1.13) | 0.466 | 0.621 |
| miR-206† | 1.61 (1.16–2.23) | 0.004 * | 1.64 (1.17–2.30) | 0.004 * | 0.016 * |
| Inflection Points of miRNA Level † | OR (95% CI) | p Value |
|---|---|---|
| miR-491-5p # | 3-month poor outcome | |
| <2.10 | 0.97 (0.95–0.99) | 0.017 * |
| >2.10 | 0.99 (0.94, 1.04) | 0.641 |
| miR-491-5p # | 1-year poor outcome | |
| <2.18 | 0.90 (0.86, 0.95) | <0.001 * |
| >2.18 | 1.01 (0.94, 1.08) | 0.892 |
| miR-206 § | Spontaneous HT | |
| <2.04 | 1.02 (1.01, 1.03) | 0.009 * |
| >2.04 | 1.01 (0.99, 1.04) | 0.384 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, X.; Liu, J.; Wang, Y.; Zheng, L.; Liu, M. Serum microRNA miR-491-5p/miR-206 Is Correlated with Poor Outcomes/Spontaneous Hemorrhagic Transformation after Ischemic Stroke: A Case Control Study. Brain Sci. 2022, 12, 999. https://doi.org/10.3390/brainsci12080999
Song X, Liu J, Wang Y, Zheng L, Liu M. Serum microRNA miR-491-5p/miR-206 Is Correlated with Poor Outcomes/Spontaneous Hemorrhagic Transformation after Ischemic Stroke: A Case Control Study. Brain Sciences. 2022; 12(8):999. https://doi.org/10.3390/brainsci12080999
Chicago/Turabian StyleSong, Xindi, Junfeng Liu, Yanan Wang, Lukai Zheng, and Ming Liu. 2022. "Serum microRNA miR-491-5p/miR-206 Is Correlated with Poor Outcomes/Spontaneous Hemorrhagic Transformation after Ischemic Stroke: A Case Control Study" Brain Sciences 12, no. 8: 999. https://doi.org/10.3390/brainsci12080999