
A Review of the Measurement of the Neurology of Gait in Cognitive Dysfunction or Dementia, Focusing on the Application of fNIRS during Dual-Task Gait Assessment

 , and
, and 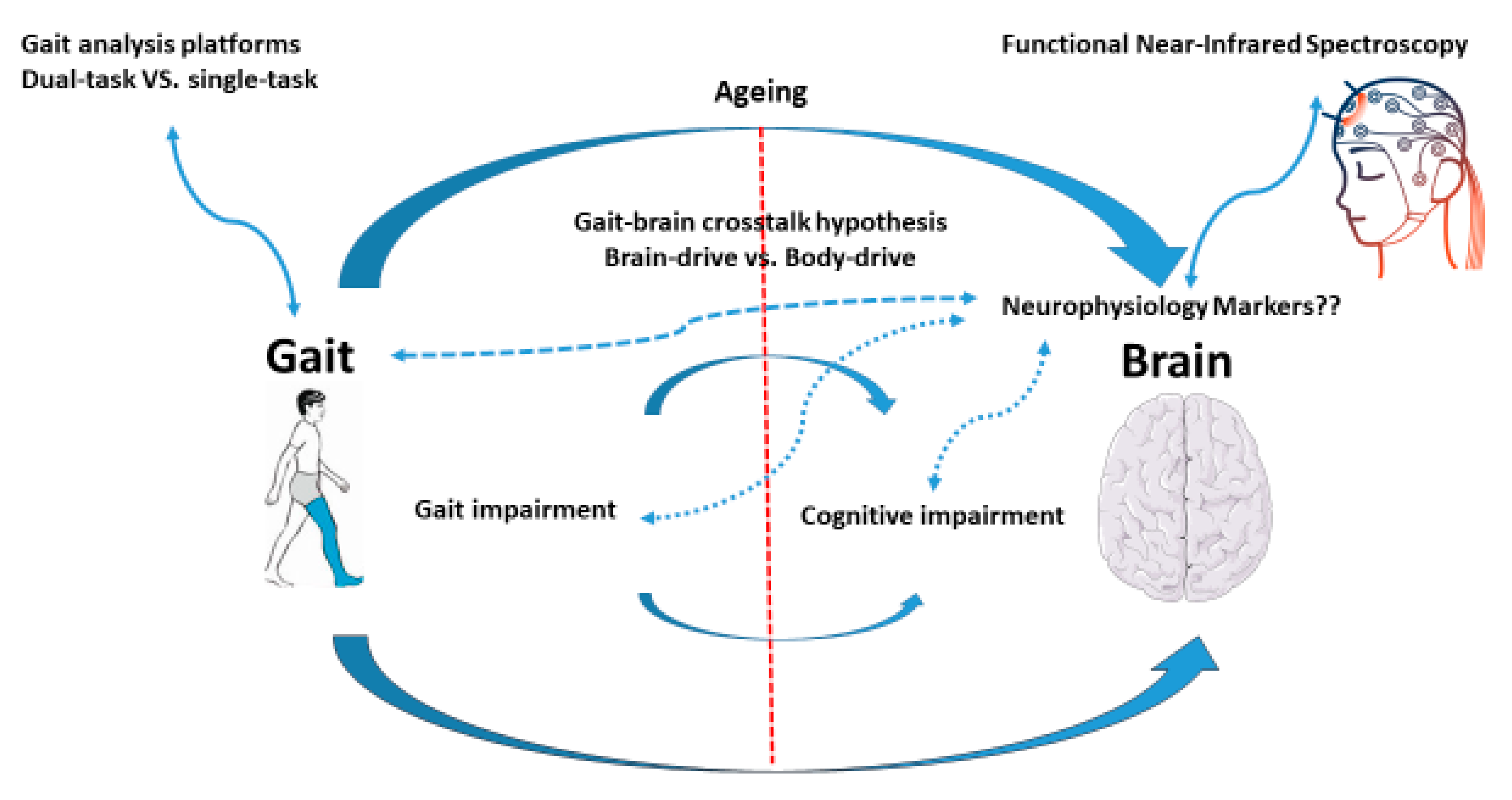{kind=link}
Abstract
:1. Gait and Brain
Criteria and Searching Protocol
2. Gait, Cognitive Dysfunction, and Dementia
3. Dual-Task Gait Performance, Cognitive Dysfunction, and Dementia
4. Neurophysiological Biomarkers
4.1. fNIRS, Dual-Task Gait, and Ageing
4.2. fNIRS, Dual-Task Gait, Neurological Disorders
4.3. fNIRS, Dual-Task Gait, Cognitive Dysfunction, Dementia
5. Brain–Drive Hypothesis
6. Research Gap and Future Directions
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
References
- Cohen, J.A.; Verghese, J. Gait and dementia. Handb. Clin. Neurol. 2019, 167, 419–427. [Google Scholar] [PubMed]
- Giladi, N.; Horak, F.B.; Hausdorff, J.M. Classification of gait disturbances: Distinguishing between continuous and episodic changes. Mov. Disord. 2013, 28, 1469–1473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulas, I.; Putzu, V.; Asoni, G.; Viale, D.; Mameli, I.; Pau, M. Clinical assessment of gait and functional mobility in Italian healthy and cognitively impaired older persons using wearable inertial sensors. Aging Clin. Exp. Res. 2021, 33, 1853–1864. [Google Scholar] [CrossRef]
- Valkanova, V.; Ebmeier, K.P. What can gait tell us about dementia? Review of epidemiological and neuropsychological evidence. Gait Posture 2017, 53, 215–223. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Pavasini, R.; Guralnik, J.; Brown, J.C.; di Bari, M.; Cesari, M.; Landi, F.; Vaes, B.; Legrand, D.; Verghese, J.; Wang, C.; et al. Short Physical Performance Battery and all-cause mortality: Systematic review and meta-analysis. BMC Med. 2016, 14, 215. [Google Scholar] [CrossRef] [Green Version]
- Lipkin, D.P.; Scriven, A.J.; Crake, T.; Poole-Wilson, P.A. Six minute walking test for assessing exercise capacity in chronic heart failure. Br. Med. J. (Clin. Res. Ed.) 1986, 292, 653–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freire, A.N.; Guerra, R.O.; Alvarado, B.; Guralnik, J.M.; Zunzunegui, M.V. Validity and reliability of the short physical performance battery in two diverse older adult populations in Quebec and Brazil. J. Aging Health 2012, 24, 863–878. [Google Scholar] [CrossRef]
- Perracini, M.R.; Mello, M.; de Oliveira Máximo, R.; Bilton, T.L.; Ferriolli, E.; Lustosa, L.P.; da Silva Alexandre, T. Diagnostic Accuracy of the Short Physical Performance Battery for Detecting Frailty in Older People. Phys. Ther. 2020, 100, 90–98. [Google Scholar] [CrossRef]
- Hausdorff, J.M. Gait dynamics in Parkinson’s disease: Common and distinct behavior among stride length, gait variability, and fractal-like scaling. Chaos 2009, 19, 026113. [Google Scholar] [CrossRef] [Green Version]
- Amboni, M.; Barone, P.; Hausdorff, J.M. Cognitive contributions to gait and falls: Evidence and implications. Mov. Disord. 2013, 28, 1520–1533. [Google Scholar] [CrossRef] [PubMed]
- Bahureksa, L.; Najafi, B.; Saleh, A.; Sabbagh, M.; Coon, D.; Mohler, M.J.; Schwenk, M. The Impact of Mild Cognitive Impairment on Gait and Balance: A Systematic Review and Meta-Analysis of Studies Using Instrumented Assessment. Gerontology 2017, 63, 67–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Roberts, R.; Knopman, D.S. Classification and Epidemiology of MCI. Clin. Geriatr. Med. 2013, 29, 753–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, P.-J.; Zhong, Y.; Fillit, H.M.; Chen, E.; Neumann, P.J. Medicare Expenditures of Individuals with Alzheimer’s Disease and Related Dementias or Mild Cognitive Impairment Before and After Diagnosis. J. Am. Geriatr. Soc. 2016, 64, 1549–1557. [Google Scholar] [CrossRef]
- Batty, G.D.; Deary, I.J.; Zaninotto, P. Association of cognitive function with cause-specific mortality in middle and older age: Follow-up of participants in the English Longitudinal Study of Ageing. Am. J. Epidemiol. 2016, 183, 183–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaufman, Y.; Anaki, D.; Binns, M.; Freedman, M. Cognitive decline in Alzheimer disease. Impact Spiritual. Relig. QOL 2007, 68, 1509–1514. [Google Scholar]
- Sui, S.X.; Williams, L.J.; Holloway-Kew, K.L.; Hyde, N.K.; Pasco, J.A. Skeletal muscle health and cognitive function: A narrative review. Int. J. Mol. Sci. 2020, 22, 255. [Google Scholar] [CrossRef]
- Pasco, J.A.; Stuart, A.L.; Sui, S.X.; Holloway-Kew, K.L.; Hyde, N.K.; Tembo, M.C.; Rufus-Membere, P.; Kotowicz, M.A.; Williams, L.J. Dynapenia and low Cognition: A cross-sectional association in postmenopausal women. J. Clin. Med. 2021, 10, 173. [Google Scholar] [CrossRef]
- Sui, S.X.; Holloway-Kew, K.L.; Hyde, N.K.; Williams, L.J.; Leach, S.; Pasco, J.A. Muscle strength and gait speed rather than lean mass are better indicators for poor cognitive function in older men. Sci. Rep. 2020, 10, 10367. [Google Scholar] [CrossRef]
- Sui, S.X.; Holloway-Kew, K.L.; Hyde, N.K.; Williams, L.J.; Tembo, M.C.; Mohebbi, M.; Gojanovic, M.; Leach, S.; Pasco, J.A. Handgrip strength and muscle quality in Australian women: Cross-sectional data from the Geelong Osteoporosis Study. J. Cachexia Sarcopenia Muscle 2020, 11, 690–697. [Google Scholar] [CrossRef]
- Sui, S.X.; Williams, L.J.; Holloway-Kew, K.L.; Hyde, N.K.; Anderson, K.B.; Tembo, M.C.; Addinsall, A.B.; Leach, S.; Pasco, J.A. Skeletal Muscle Density and Cognitive Function: A Cross-Sectional Study in Men. Calcif. Tissue Int. 2021, 108, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Kueper, J.K.; Lizotte, D.J.; Montero-Odasso, M.; Speechley, M. Cognition and motor function: The gait and cognition pooled index. PLoS ONE 2020, 15, e0238690. [Google Scholar] [CrossRef] [PubMed]
- Darweesh, S.K.L.; Licher, S.; Wolters, F.J.; Koudstaal, P.J.; Ikram, M.K.; Ikram, M.A. Quantitative gait, cognitive decline, and incident dementia: The Rotterdam Study. Alzheimers Dement. 2019, 15, 1264–1273. [Google Scholar] [CrossRef] [Green Version]
- Montero-Odasso, M.; Speechley, M.; Muir-Hunter, S.W.; Pieruccini-Faria, F.; Sarquis-Adamson, Y.; Hachinski, V.; Bherer, L.; Borrie, M.; Wells, J.; Garg, A.X. Dual decline in gait speed and cognition is associated with future dementia: Evidence for a phenotype. Age Ageing 2020, 49, 995–1002. [Google Scholar] [CrossRef] [PubMed]
- Mc Ardle, R.; Morris, R.; Wilson, J.; Galna, B.; Thomas, A.J.; Rochester, L. What Can Quantitative Gait Analysis Tell Us about Dementia and Its Subtypes? A Structured Review. J. Alzheimers Dis. 2017, 60, 1295–1312. [Google Scholar] [CrossRef]
- De Cock, A.M.; Fransen, E.; Perkisas, S.; Verhoeven, V.; Beauchet, O.; Vandewoude, M.; Remmen, R. Comprehensive Quantitative Spatiotemporal Gait Analysis Identifies Gait Characteristics for Early Dementia Subtyping in Community Dwelling Older Adults. Front. Neurol. 2019, 10, 313. [Google Scholar] [CrossRef] [Green Version]
- Allali, G.; Launay, C.P.; Blumen, H.M.; Callisaya, M.L.; de Cock, A.n.; Kressig, R.W.; Srikanth, V.; Steinmetz, J.e.; Verghese, J.; Beauchet, O.; et al. Falls, Cognitive Impairment, and Gait Performance: Results From the GOOD Initiative. J. Am. Med. Dir. Assoc. 2017, 18, 335–340. [Google Scholar] [CrossRef] [Green Version]
- Bayot, M.; Dujardin, K.; Tard, C.; Defebvre, L.; Bonnet, C.T.; Allart, E.; Delval, A. The interaction between cognition and motor control: A theoretical framework for dual-task interference effects on posture, gait initiation, gait and turning. Neurophysiol. Clin. 2018, 48, 361–375. [Google Scholar] [CrossRef]
- Goh, J.O.; Park, D.C. Neuroplasticity and cognitive aging: The scaffolding theory of aging and cognition. Restor. Neurol. Neurosci. 2009, 27, 391–403. [Google Scholar] [CrossRef]
- Kelly, V.E.; Eusterbrock, A.J.; Shumway-Cook, A. A review of dual-task walking deficits in people with Parkinson’s disease: Motor and cognitive contributions, mechanisms, and clinical implications. Parkinsons Dis. 2012, 2012, 918719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrigna, L.; Gentile, A.; Mani, D.; Pajaujiene, S.; Zanotto, T.; Thomas, E.; Paoli, A.; Palma, A.; Bianco, A. Dual-Task Conditions on Static Postural Control in Older Adults: A Systematic Review and Meta-Analysis. J. Aging Phys. Act. 2021, 29, 162–177. [Google Scholar] [CrossRef]
- Strobach, T. The dual-task practice advantage: Empirical evidence and cognitive mechanisms. Psychon. Bull. Rev. 2020, 27, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Sui, S.X.; Hordacre, B.; Pasco, J.A. Are sarcopenia and cognitive dysfunction comorbid after stroke in the context of brain-muscle crosstalk? Biomedicines 2021, 9, 223. [Google Scholar] [CrossRef] [PubMed]
- Montero-Odasso, M.M.; Sarquis-Adamson, Y.; Speechley, M.; Borrie, M.J.; Hachinski, V.C.; Wells, J.; Riccio, P.M.; Schapira, M.; Sejdic, E.; Camicioli, R.M.; et al. Association of Dual-Task Gait With Incident Dementia in Mild Cognitive Impairment: Results From the Gait and Brain Study. JAMA Neurol. 2017, 74, 857–865. [Google Scholar] [CrossRef]
- Ansai, J.H.; Andrade, L.P.; Rossi, P.G.; Takahashi, A.C.M.; Vale, F.A.C.; Rebelatto, J.R. Gait, dual task and history of falls in elderly with preserved cognition, mild cognitive impairment, and mild Alzheimer’s disease. Braz. J. Phys. Ther. 2017, 21, 144–151. [Google Scholar] [CrossRef]
- Lowe, D.A.; MacAulay, R.K.; Szeles, D.M.; Milano, N.J.; Wagner, M.T. Dual-Task Gait Assessment in a Clinical Sample: Implications for Improved Detection of Mild Cognitive Impairment. J. Gerontol. B Psychol. Sci. Soc. Sci. 2020, 75, 1372–1381. [Google Scholar] [CrossRef]
- Boettcher, L.N.; Hssayeni, M.; Rosenfeld, A.; Tolea, M.I.; Galvin, J.E.; Ghoraani, B. Dual-Task Gait Assessment and Machine Learning for Early-detection of Cognitive Decline. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2020, 2020, 3204–3207. [Google Scholar]
- Varma, V.R.; Ghosal, R.; Hillel, I.; Volfson, D.; Weiss, J.; Urbanek, J.; Hausdorff, J.M.; Zipunnikov, V.; Watts, A. Continuous gait monitoring discriminates community-dwelling mild Alzheimer’s disease from cognitively normal controls. Alzheimers Dement. 2021, 7, e12131. [Google Scholar] [CrossRef]
- Belghali, M.; Chastan, N.; Davenne, D.; Decker, L.M. Improving Dual-Task Walking Paradigms to Detect Prodromal Parkinson’s and Alzheimer’s Diseases. Front. Neurol. 2017, 8, 207. [Google Scholar] [CrossRef] [Green Version]
- Sakurai, R.; Bartha, R.; Montero-Odasso, M. Entorhinal Cortex Volume Is Associated With Dual-Task Gait Cost Among Older Adults With MCI: Results From the Gait and Brain Study. J. Gerontol. A Biol. Sci. Med. Sci. 2019, 74, 698–704. [Google Scholar] [CrossRef] [Green Version]
- Annweiler, C.; Beauchet, O.; Bartha, R.; Wells, J.L.; Borrie, M.J.; Hachinski, V.; Montero-Odasso, M. Motor cortex and gait in mild cognitive impairment: A magnetic resonance spectroscopy and volumetric imaging study. Brain 2013, 136 Pt 3, 859–871. [Google Scholar] [CrossRef] [Green Version]
- Doi, T.; Blumen, H.M.; Verghese, J.; Shimada, H.; Makizako, H.; Tsutsumimoto, K.; Hotta, R.; Nakakubo, S.; Suzuki, T. Gray matter volume and dual-task gait performance in mild cognitive impairment. Brain Imaging Behav. 2017, 11, 887–898. [Google Scholar] [CrossRef] [PubMed]
- Rosso, A.L.; Verghese, J.; Metti, A.L.; Boudreau, R.M.; Aizenstein, H.J.; Kritchevsky, S.; Harris, T.; Yaffe, K.; Satterfield, S.; Studenski, S.; et al. Slowing gait and risk for cognitive impairment: The hippocampus as a shared neural substrate. Neurology 2017, 89, 336–342. [Google Scholar] [CrossRef]
- Wilson, J.; Allcock, L.; Mc Ardle, R.; Taylor, J.P.; Rochester, L. The neural correlates of discrete gait characteristics in ageing: A structured review. Neurosci. Biobehav. Rev. 2019, 100, 344–369. [Google Scholar] [CrossRef] [PubMed]
- Bürki, C.N.; Bridenbaugh, S.A.; Reinhardt, J.; Stippich, C.; Kressig, R.W.; Blatow, M. Imaging gait analysis: An fMRI dual task study. Brain Behav. 2017, 7, e00724. [Google Scholar] [CrossRef] [PubMed]
- Scarapicchia, V.; Brown, C.; Mayo, C.; Gawryluk, J.R. Functional Magnetic Resonance Imaging and Functional Near-Infrared Spectroscopy: Insights from Combined Recording Studies. Front. Hum. Neurosci. 2017, 11, 419. [Google Scholar] [CrossRef]
- Bonilauri, A.; Sangiuliano Intra, F.; Pugnetti, L.; Baselli, G.; Baglio, F. A Systematic Review of Cerebral Functional Near-Infrared Spectroscopy in Chronic Neurological Diseases-Actual Applications and Future Perspectives. Diagnostics 2020, 10, 581. [Google Scholar] [CrossRef]
- Kim, H.Y.; Seo, K.; Jeon, H.J.; Lee, U.; Lee, H. Application of Functional Near-Infrared Spectroscopy to the Study of Brain Function in Humans and Animal Models. Mol. Cells 2017, 40, 523–532. [Google Scholar] [CrossRef] [Green Version]
- Beurskens, R.; Helmich, I.; Rein, R.; Bock, O. Age-related changes in prefrontal activity during walking in dual-task situations: A fNIRS study. Int. J. Psychophysiol. 2014, 92, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Guidotti Breting, L.M.; Tuminello, E.R.; Duke Han, S. Functional neuroimaging studies in normal aging. Curr. Top. Behav. Neurosci. 2012, 10, 91–111. [Google Scholar] [PubMed]
- Chen, M.; Pillemer, S.; England, S.; Izzetoglu, M.; Mahoney, J.R.; Holtzer, R. Neural correlates of obstacle negotiation in older adults: An fNIRS study. Gait Posture 2017, 58, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Wagshul, M.E.; Lucas, M.; Ye, K.; Izzetoglu, M.; Holtzer, R. Multi-modal neuroimaging of dual-task walking: Structural MRI and fNIRS analysis reveals prefrontal grey matter volume moderation of brain activation in older adults. Neuroimage 2019, 189, 745–754. [Google Scholar] [CrossRef] [PubMed]
- Salzman, T.; Aboualmagd, A.; Badawi, H.; Tobón-Vallejo, D.; Kim, H.; Dahroug, L.; Laamarti, F.; El Saddik, A.; Fraser, S. Prefrontal Cortex Involvement during Dual-Task Stair Climbing in Healthy Older Adults: An fNIRS Study. Brain Sci. 2021, 11, 71. [Google Scholar] [CrossRef] [PubMed]
- Salzman, T.; Tobón Vallejo, D.; Polskaia, N.; Michaud, L.; St-Amant, G.; Lajoie, Y.; Fraser, S. Hemodynamic and behavioral changes in older adults during cognitively demanding dual tasks. Brain Behav. 2021, 11, e02021. [Google Scholar] [CrossRef]
- Pelicioni, P.H.S.; Tijsma, M.; Lord, S.R.; Menant, J. Prefrontal cortical activation measured by fNIRS during walking: Effects of age, disease and secondary task. PeerJ 2019, 7, e6833. [Google Scholar] [CrossRef] [Green Version]
- Bishnoi, A.; Holtzer, R.; Hernandez, M.E. Brain Activation Changes While Walking in Adults with and without Neurological Disease: Systematic Review and Meta-Analysis of Functional Near-Infrared Spectroscopy Studies. Brain Sci. 2021, 11, 291. [Google Scholar] [CrossRef]
- Teo, W.P.; Rantalainen, T.; Nuzum, N.; Valente, L.; Macpherson, H. Altered prefrontal cortex responses in older adults with subjective memory complaints and dementia during dual-task gait: An fNIRS study. Eur. J. Neurosci. 2021, 53, 1324–1333. [Google Scholar] [CrossRef]
- Bloom, G.S. Amyloid-β and tau: The trigger and bullet in Alzheimer disease pathogenesis. JAMA Neurol. 2014, 71, 505–508. [Google Scholar] [CrossRef] [Green Version]
- Muurling, M.; Rhodius-Meester, H.F.M.; Pärkkä, J.; van Gils, M.; Frederiksen, K.S.; Bruun, M.; Hasselbalch, S.G.; Soininen, H.; Herukka, S.-K.; Hallikainen, M.; et al. Gait Disturbances are Associated with Increased Cognitive Impairment and Cerebrospinal Fluid Tau Levels in a Memory Clinic Cohort. J. Alzheimers Dis. 2020, 76, 1061–1070. [Google Scholar] [CrossRef]
- Wennberg, A.M.V.; Lesnick, T.G.; Schwarz, C.G.; Savica, R.; Hagen, C.E.; Roberts, R.O.; Knopman, D.S.; Hollman, J.H.; Vemuri, P.; Jack, C.R., Jr.; et al. Longitudinal Association Between Brain Amyloid-Beta and Gait in the Mayo Clinic Study of Aging. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 1244–1250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nadkarni, N.K.; Perera, S.; Snitz, B.E.; Mathis, C.A.; Price, J.; Williamson, J.; DeKosky, S.T.; Klunk, W.E. Association of Brain Amyloid-β With Slow Gait in Elderly Individuals Without Dementia: Influence of Cognition and Apolipoprotein E ε4 Genotype. JAMA Neurol. 2017, 74, 82–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitson, H.E.; Potter, G.G.; Feld, J.A.; Plassman, B.L.; Reynolds, K.; Sloane, R.; Welsh-Bohmer, K.A. Dual-Task Gait and Alzheimer’s Disease Genetic Risk in Cognitively Normal Adults: A Pilot Study. J. Alzheimers Dis. 2018, 64, 1137–1148. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sui, S.X.; Hendy, A.M.; Teo, W.-P.; Moran, J.T.; Nuzum, N.D.; Pasco, J.A. A Review of the Measurement of the Neurology of Gait in Cognitive Dysfunction or Dementia, Focusing on the Application of fNIRS during Dual-Task Gait Assessment. Brain Sci. 2022, 12, 968. https://doi.org/10.3390/brainsci12080968
Sui SX, Hendy AM, Teo W-P, Moran JT, Nuzum ND, Pasco JA. A Review of the Measurement of the Neurology of Gait in Cognitive Dysfunction or Dementia, Focusing on the Application of fNIRS during Dual-Task Gait Assessment. Brain Sciences. 2022; 12(8):968. https://doi.org/10.3390/brainsci12080968
Chicago/Turabian StyleSui, Sophia X., Ashlee M. Hendy, Wei-Peng Teo, Joshua T. Moran, Nathan D. Nuzum, and Julie A. Pasco. 2022. "A Review of the Measurement of the Neurology of Gait in Cognitive Dysfunction or Dementia, Focusing on the Application of fNIRS during Dual-Task Gait Assessment" Brain Sciences 12, no. 8: 968. https://doi.org/10.3390/brainsci12080968