
Endovascular Treatment of ICAS Patients: Targeting Reperfusion Rather than Residual Stenosis

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
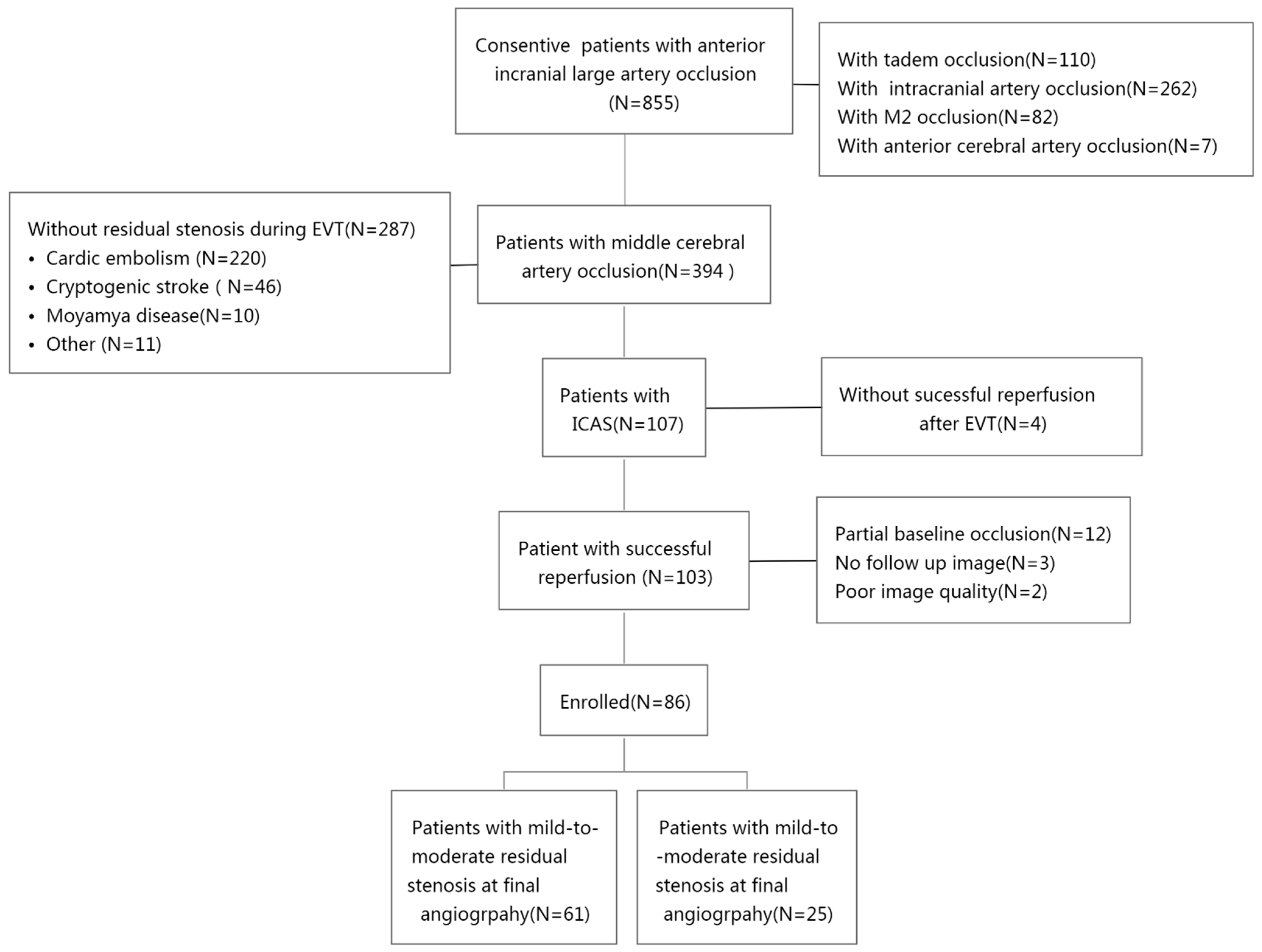
2.2. Patients
2.3. Endovascular Procedures
2.4. Tirofiban Administration and Antiplatelet Regime
2.5. Definitions of ICAS
2.6. Evaluation of Angiographic Images
2.7. Outcomes
2.8. Statistical Analysis
3. Results
3.1. Patients
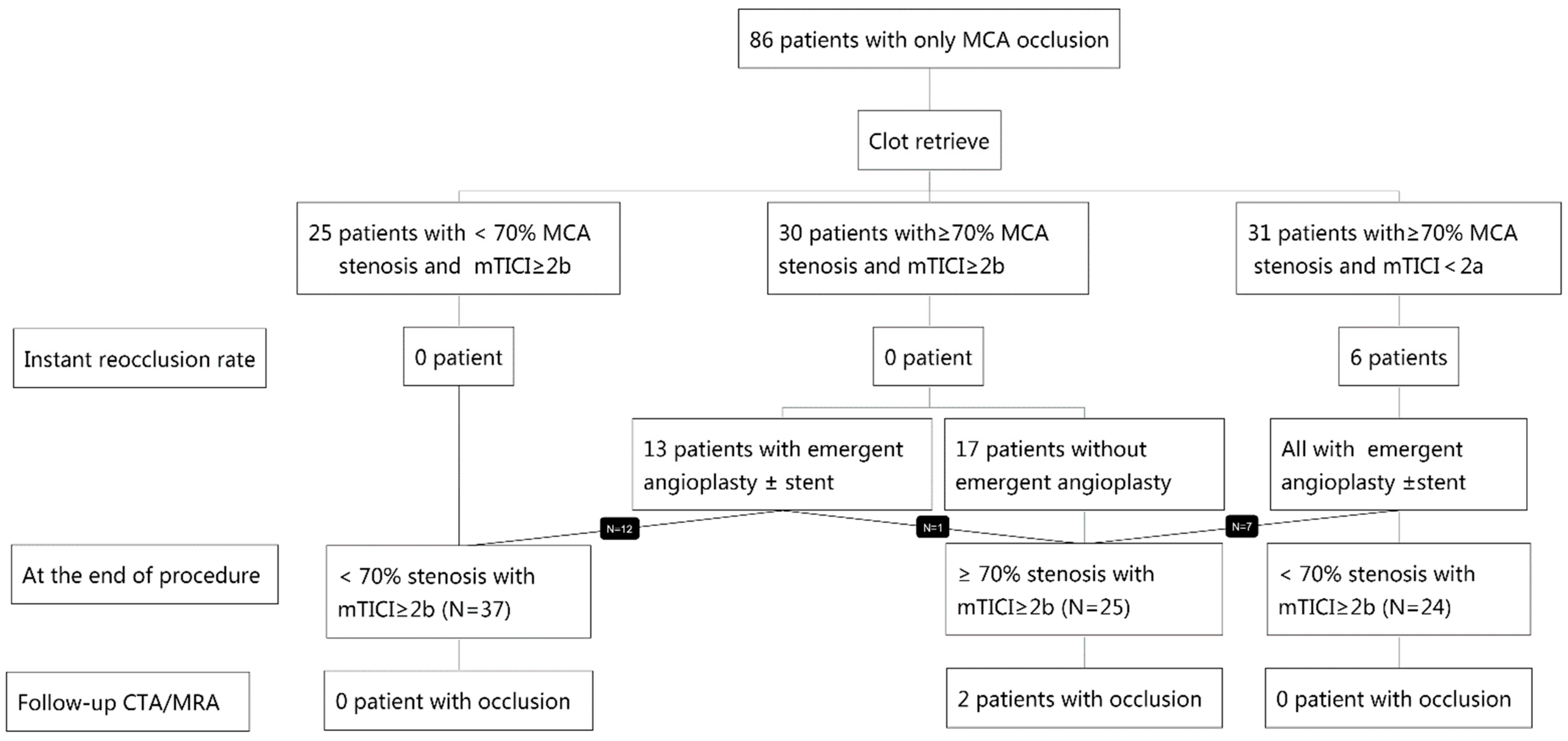
3.2. ICAS Classification Validation
3.2.1. Step 1 Analysis: Intraprocedural Reocclusion
3.2.2. Step 2 Analysis: Delayed Occlusion
3.3. Subgroup Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. 2018 Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2018, 49, e46–e110. [Google Scholar] [CrossRef] [PubMed]
- Langhorne, P.; Ramachandra, S. Organised Inpatient (Stroke Unit) Care for Stroke: Network Meta-Analysis. Cochrane Database Syst. Rev. 2020, 2020, CD000197. [Google Scholar]
- Mosimann, P.J.; Kaesmacher, J.; Gautschi, D.; Bellwald, S.; Panos, L.; Piechowiak, E.; Dobrocky, T.; Zibold, F.; Mordasini, P.; El-Koussy, M.; et al. Predictors of Unexpected Early Reocclusion after Successful Mechanical Thrombectomy in Acute Ischemic Stroke Patients. Stroke 2018, 49, 2643–2651. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.E.; Yoon, W.; Kim, S.K.; Kim, B.C.; Heo, T.W.; Baek, B.H.; Lee, Y.Y.; Yim, N.Y. Incidence and Clinical Significance of Acute Reocclusion after Emergent Angioplasty or Stenting for Underlying Intracranial Stenosis in Patients with Acute Stroke. Am. J. Neuroradiol. 2016, 37, 1690–1695. [Google Scholar] [CrossRef] [Green Version]
- Kang, D.-H.; Kim, Y.-W.; Hwang, Y.-H.; Park, S.-P.; Kim, Y.-S.; Baik, S.K. Instant Reocclusion Following Mechanical Thrombectomy of in Situ Thromboocclusion and the Role of Low-Dose Intra-Arterial Tirofiban. Cerebrovasc. Dis. 2014, 37, 350–355. [Google Scholar] [CrossRef]
- Heo, J.H.; Lee, K.Y.; Kim, S.H.; Kim, D.I. Immediate Reocclusion Following a Successful Thrombolysis in Acute Stroke: A Pilot Study. Neurology 2003, 60, 1684–1687. [Google Scholar] [CrossRef]
- Jame, S.; Barnes, G. Stroke and Thromboembolism Prevention in Atrial Fibrillation. Heart 2020, 106, 10–17. [Google Scholar] [CrossRef]
- Yi, T.Y.; Chen, W.H.; Wu, Y.M.; Zhang, M.F.; Chen, Y.H.; Wu, Z.Z.; Shi, Y.C.; Chen, B.L. Special Endovascular Treatment for Acute Large Artery Occlusion Resulting From Atherosclerotic Disease. World Neurosurg. 2017, 103, 65–72. [Google Scholar] [CrossRef]
- Liang, W.; Wang, Y.; Du, Z.; Mang, J.; Wang, J. Intraprocedural Angiographic Signs Observed During Endovascular Thrombectomy in Patients With Acute Ischemic Stroke: A Systematic Review. Neurology 2021, 96, 1080–1090. [Google Scholar] [CrossRef]
- Lee, J.S.; Hong, J.M.; Lee, K.S.; Suh, H.I.; Demchuk, A.M.; Hwang, Y.H.; Kim, B.M.; Kim, J.S. Endovascular Therapy of Cerebral Arterial Occlusions: Intracranial Atherosclerosis versus Embolism. J. Stroke Cerebrovasc. Dis. 2015, 24, 2074–2080. [Google Scholar] [CrossRef]
- Yi, T.Y.; Chen, W.H.; Wu, Y.M.; Zhang, M.F.; Zhan, A.L.; Chen, Y.H.; Wu, Z.Z.; Shi, Y.C.; Chen, B.L. Microcatheter “First-Pass Effect” Predicts Acute Intracranial Artery Atherosclerotic Disease-Related Occlusion. Neurosurgery 2018, 84, 1296–1305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, W.H.; Yi, T.Y.; Zhan, A.L.; Wu, Y.M.; Lu, Y.Y.; Li, Y.M.; Pan, Z.N.; Lin, D.L.; Lin, X.H. Stent-Unsheathed Effect Predicts Acute Distal Middle Cerebral Artery Atherosclerotic Disease-Related Occlusion. J. Neurol. Sci. 2020, 416, 116957. [Google Scholar] [CrossRef] [PubMed]
- Zaidat, O.O.; Yoo, A.J.; Khatri, P.; Tomsick, T.A.; Von Kummer, R.; Saver, J.L.; Marks, M.P.; Prabhakaran, S.; Kallmes, D.F.; Fitzsimmons, B.F.M.; et al. Recommendations on Angiographic Revascularization Grading Standards for Acute Ischemic Stroke: A Consensus Statement. Stroke 2013, 44, 2650–2663. [Google Scholar] [CrossRef] [Green Version]
- López-Cancio, E.; Matheus, M.G.; Romano, J.G.; Liebeskind, D.S.; Prabhakaran, S.; Turan, T.N.; Cotsonis, G.A.; Lynn, M.J.; Rumboldt, Z.; Chimowitz, M.I.; et al. Infarct Patterns, Collaterals and Likely Causative Mechanisms of Stroke in Symptomatic Intracranial Atherosclerosis. Cerebrovasc. Dis. 2014, 37, 417–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rocco, A.; Sallustio, F.; Toschi, N.; Rizzato, B.; Legramante, J.; Ippoliti, A.; Marchetti, A.A.; Pampana, E.; Gandini, R.; Diomedi, M. Carotid Artery Stent Placement and Carotid Endarterectomy: A Challenge for Urgent Treatment after Stroke—Early and 12-Month Outcomes in a Comprehensive Stroke Center. J. Vasc. Interv. Radiol. 2018, 29, 1254–1261. [Google Scholar] [CrossRef]
- Hwang, Y.H.; Kim, Y.W.; Kang, D.H.; Kim, Y.S.; Liebeskind, D.S. Impact of Target Arterial Residual Stenosis on Outcome after Endovascular Revascularization. Stroke 2016, 47, 1850–1857. [Google Scholar] [CrossRef] [Green Version]
- Yan, Z.; Shi, Z.; Wang, Y.; Zhang, C.; Cao, J.; Ding, C.; Qu, M.; Xia, Y.; Cai, J.; Zhang, X.; et al. Efficacy and Safety of Low-Dose Tirofiban for Acute Intracranial Atherosclerotic Stenosis Related Occlusion with Residual Stenosis after Endovascular Treatment. J. Stroke Cerebrovasc. Dis. 2020, 29, 104619. [Google Scholar] [CrossRef]
- Yang, J.; Wu, Y.; Gao, X.; Bivard, A.; Levi, C.R.; Parsons, M.W.; Lin, L. Intraarterial Versus Intravenous Tirofiban as an Adjunct to Endovascular Thrombectomy for Acute Ischemic Stroke. Stroke 2020, 51, 2925–2933. [Google Scholar] [CrossRef]
- Al Hasan, M.; Murugan, R. Stenting versus Aggressive Medical Therapy for Intracranial Arterial Stenosis: More Harm than Good. Crit. Care. 2012, 16, 310. [Google Scholar] [CrossRef] [Green Version]
- Wakhloo, A.; Gupta, R.; Kirshner, H.; Megerian, J.T.; Lesko, J.; Pitzer, P. Effect of a Balloon-Expandable Intracranial Stent vs Medical Therapy on Risk of Stroke in Patients With Symptomatic Intracranial Stenosis. VISSIT Randomized Clin. Trial 2015, 53226, 1240–1248. [Google Scholar]
- Alexander, M.J.; Zauner, A.; Chaloupka, J.C.; Baxter, B.; Callison, R.C.; Gupta, R.; Song, S.S.; Yu, W.; WEAVE Trial Investigators. WEAVE Trial: Final results in 152 on-label patients. Stroke 2019, 50, 889–894. [Google Scholar] [CrossRef] [PubMed]
- Dumont, T.M.; Kan, P.; Snyder, K.V.; Hopkins, L.N.; Siddiqui, A.H.; Levy, E.I. Revisiting Angioplasty without Stenting for Symptomatic Intracranial Atherosclerotic Stenosis after the Stenting and Aggressive Medical Management for Preventing Recurrent Stroke in Intracranial Stenosis (SAMMPRIS) Study. Neurosurgery 2012, 71, 1103–1110. [Google Scholar] [CrossRef] [PubMed]
- Piccardi, B.; Arba, F.; Nesi, M.; Palumbo, V.; Nencini, P.; Giusti, B.; Sereni, A.; Gadda, D.; Moretti, M.; Fainardi, E.; et al. Reperfusion Injury after Ischemic Stroke Study (RISKS): Single-Centre (Florence, Italy), Prospective Observational Protocol Study. BMJ Open 2018, 5, e021183. [Google Scholar]
- Khatri, R.; McKinney, A.M.; Swenson, B.; Janardhan, V. Blood-Brain Barrier, Reperfusion Injury, and Hemorrhagic Transformation in Acute Ischemic Stroke. Neurology 2012, 79, S52–S57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bath, P.M.; Woodhouse, L.J.; Appleton, J.P.; Beridze, M.; Christensen, H.; Dineen, R.A.; Duley, L.; England, T.J.; Flaherty, K.; Havard, D.; et al. Antiplatelet Therapy with Aspirin, Clopidogrel, and Dipyridamole versus Clopidogrel Alone or Aspirin and Dipyridamole in Patients with Acute Cerebral Ischaemia (TARDIS): A Randomised, Open-Label, Phase 3 Superiority Trial. Lancet 2018, 391, 850–859. [Google Scholar] [CrossRef] [Green Version]
- Lescher, S.; Czeppan, K.; Porto, L.; Singer, O.C.; Berkefeld, J. Acute Stroke and Obstruction of the Extracranial Carotid Artery Combined with Intracranial Tandem Occlusion: Results of Interventional Revascularization. Cardiovasc. Intervent. Radiol. 2015, 38, 304–313. [Google Scholar] [CrossRef] [PubMed]
- CChang, Y.; Kim, B.M.; Bang, O.Y.; Baek, J.H.; Heo, J.H.; Nam, H.S.; Kim, Y.D.; Yoo, J.; Kim, D.J.; Jeon, P.; et al. Rescue Stenting for Failed Mechanical Thrombectomy in Acute Ischemic Stroke a Multicenter Experience. Stroke 2018, 49, 958–964. [Google Scholar] [CrossRef]
- Wu, C.; Chang, W.; Wu, D.; Wen, C.; Zhang, J.; Xu, R.; Liu, X.; Lian, Y.; Xie, N.; Li, C.; et al. Angioplasty and/or Stenting after Thrombectomy in Patients with Underlying Intracranial Atherosclerotic Stenosis. Neuroradiology 2019, 61, 1073–1081. [Google Scholar] [CrossRef]
- Tsang, A.C.O.; Orru, E.; Klostranec, J.M.; Yang, I.H.; Lau, K.K.; Tsang, F.C.P.; Lui, W.M.; Pereira, V.M.; Krings, T. Thrombectomy Outcomes of Intracranial Atherosclerosis-Related Occlusions: A Systematic Review and Meta-Analysis. Stroke 2019, 50, 1460–1466. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Group 1a: mTICI ≥ 2b + Stenosis < 70% (N = 25) | Group 2a: mTICI ≥ 2b + Stenosis ≥ 70% (N = 30) | Group 3a: mTICI < 2b + Stenosis ≥ 70% (N = 31) | p-Value | |
|---|---|---|---|---|
| Male Sex, N (%) | 18 (72%) | 22 (73.3%) | 22 (71.0%) | 0.979 |
| Age (mean, years) | 64 ± 15 | 66 ± 10 | 62 ± 12 | 0.497 |
| Smoker | 10 (40%) | 16 (51.6%) | 17 (56.7%) | 0.457 |
| Hypertension, N (%) | 16 (72.7%) | 24 (80.0%) | 26 (86.7%) | 0.454 |
| DM N (%) | 7 (28.0%) | 8 (26.7%) | 9 (29.0%) | 0.979 |
| Atrial fibrillation N (%) | 0 (0%) | 1 (3.3%) | 0 (0%) | 0.389 |
| TIA N (%) | 1 (4.0%) | 1 (3.3%) | 0 (0%) | 0.554 |
| Admission NIHSS (median, IQR) | 14 (11,18) | 13(11,17) | 14 (11,18) | 0.332 |
| Onset-to-puncture time N (%) | 0.022 | |||
| Within 8 h | 18 (72%) | 20 (66.7%) | 12 (38.7%) | |
| 8–24 h | 7 (28%) | 10 (33.3%) | 19 (61.3%) | |
| Good collateral flow, N (%) | ||||
| ASITN ≥ 3 | 14 (56.0%) | 24 (77.4%) | 15 (50.0%) | 0.070 |
| Instant reocclusion | 0 (0%) | 0 (0%) | 6 (19.4%) | 0.03 |
| Group 1b: mTICI ≥ 2b + Stenosis < 70% (N = 61) | Group 2b: mTICI ≥ 2b + Stenosis ≥ 70% (N = 25) | p-Value | |
|---|---|---|---|
| Male Sex N (%) | 45 (73.8%) | 17 (68.0%) | 0.588 |
| Age (mean, years) | 63 ± 13 | 65 ± 12 | 0.434 |
| Smoker N (%) | 30 (50.8%) | 12 (48.0%) | 0.811 |
| Hypertension, N (%) | 45 (78.9%) | 21 (84.0%) | 0.595 |
| DM N (%) | 17 (29.3%) | 7 (28.0%) | 0.904 |
| Atrial fibrillation N (%) | 0 (0%) | 1 (4.0%) | 0.291 |
| TIA N (%) | 1 (1.6%) | 1 (4.0%) | 0.499 |
| Admission NIHSS (median, IQR) | 14 (11,17) | 14 (10,20) | 0.681 |
| Onset-to-puncture time N (%) | 0.982 | ||
| Within 8 h | 35 (57.4%) | 15 (60.0%) | |
| 8–24 h | 26 (42.6%) | 10 (40.0%) | |
| Good collateral flow, N (%) | 0.627 | ||
| ASITN ≥ 3 | 35 (58.3%) | 16 (64.0%) | |
| sICH N (%) | 0 (0%) | 1 (4.0%) | 0.298 |
| Good prognosis N (%) | 41 (67.2%) | 16 (64.0%) | 0.805 |
| Mortality N (%) | 0 (0%) | 1 (4.0%) | 0.291 |
| Delayed reocclusion N (%) | 0 (0%) | 2 (8.0%) | 0.082 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yi, T.; Zhan, A.; Wu, Y.; Li, Y.; Zheng, X.; Lin, D.; Lin, X.; Pan, Z.; Chen, R.; Parsons, M.; et al. Endovascular Treatment of ICAS Patients: Targeting Reperfusion Rather than Residual Stenosis. Brain Sci. 2022, 12, 966. https://doi.org/10.3390/brainsci12080966
Yi T, Zhan A, Wu Y, Li Y, Zheng X, Lin D, Lin X, Pan Z, Chen R, Parsons M, et al. Endovascular Treatment of ICAS Patients: Targeting Reperfusion Rather than Residual Stenosis. Brain Sciences. 2022; 12(8):966. https://doi.org/10.3390/brainsci12080966
Chicago/Turabian StyleYi, Tingyu, Alai Zhan, Yanmin Wu, Yimin Li, Xiufen Zheng, Dinglai Lin, Xiaohui Lin, Zhinan Pan, Rongcheng Chen, Mark Parsons, and et al. 2022. "Endovascular Treatment of ICAS Patients: Targeting Reperfusion Rather than Residual Stenosis" Brain Sciences 12, no. 8: 966. https://doi.org/10.3390/brainsci12080966