
Functional Connectivity Increases in Response to High-Definition Transcranial Direct Current Stimulation in Patients with Chronic Disorder of Consciousness


Abstract
:Highlights
- Functional connectivity induced by HD-tDCS in DLPFC has different trends in CRS-R score improvers and non-improvers.
- An increase in theta PLV in the left frontal–parietooccipital region was significantly associated with CRS-R changes.
- DOC patients with increased PLV of the alpha band in the intra-bifrontal region have a better prognosis than those without.
Abstract
1. Introduction
2. Experimental Procedures
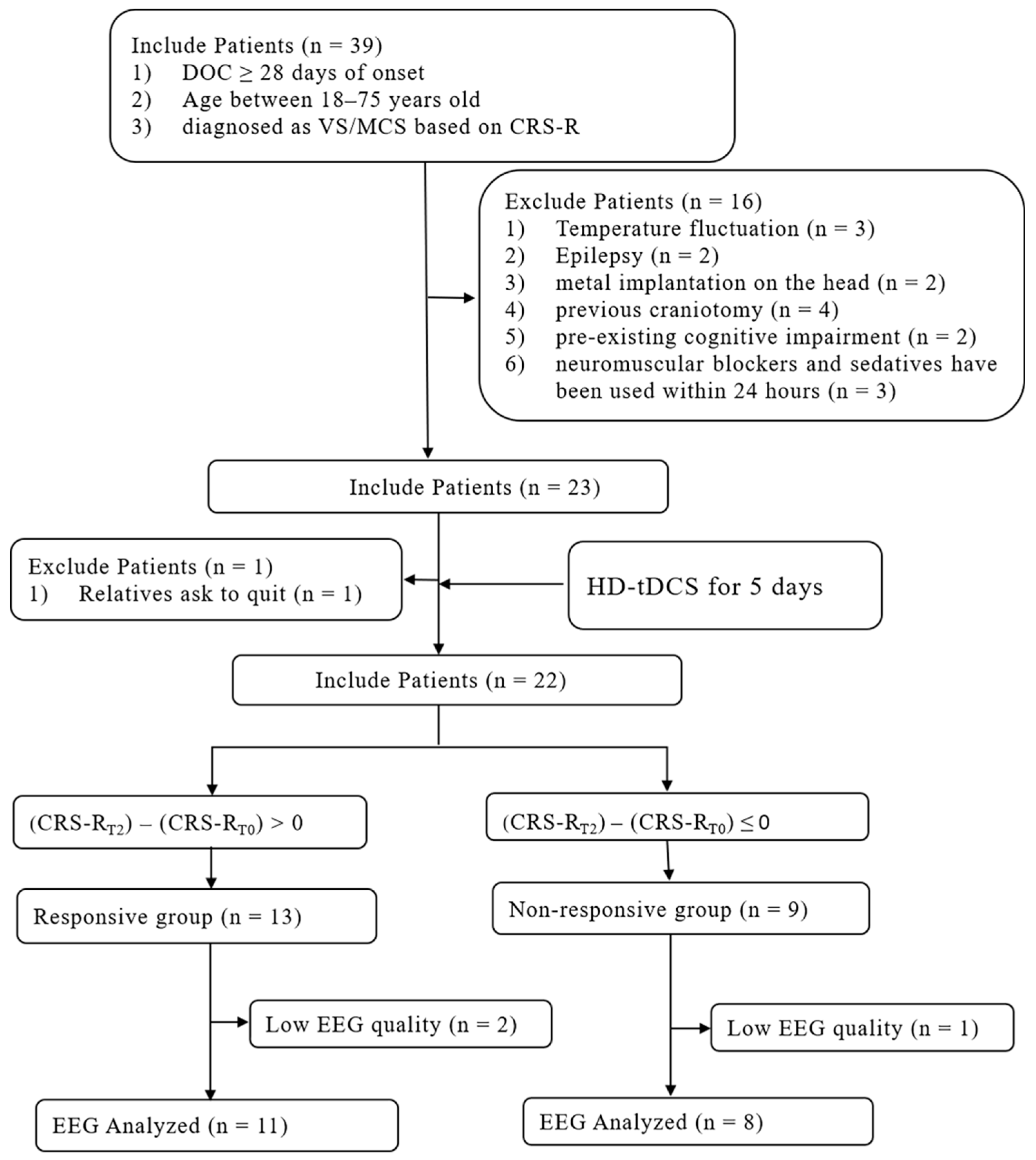
2.1. Patients
2.2. Behavior
2.3. Stimulation Protocol
2.4. EEG Recordings and Pre-Processing
2.5. EEG Analysis of the Phase Locking Value (PLV)
2.6. Statistical Analysis
3. Results
3.1. Demographic and Clinical Behavioral Outcomes
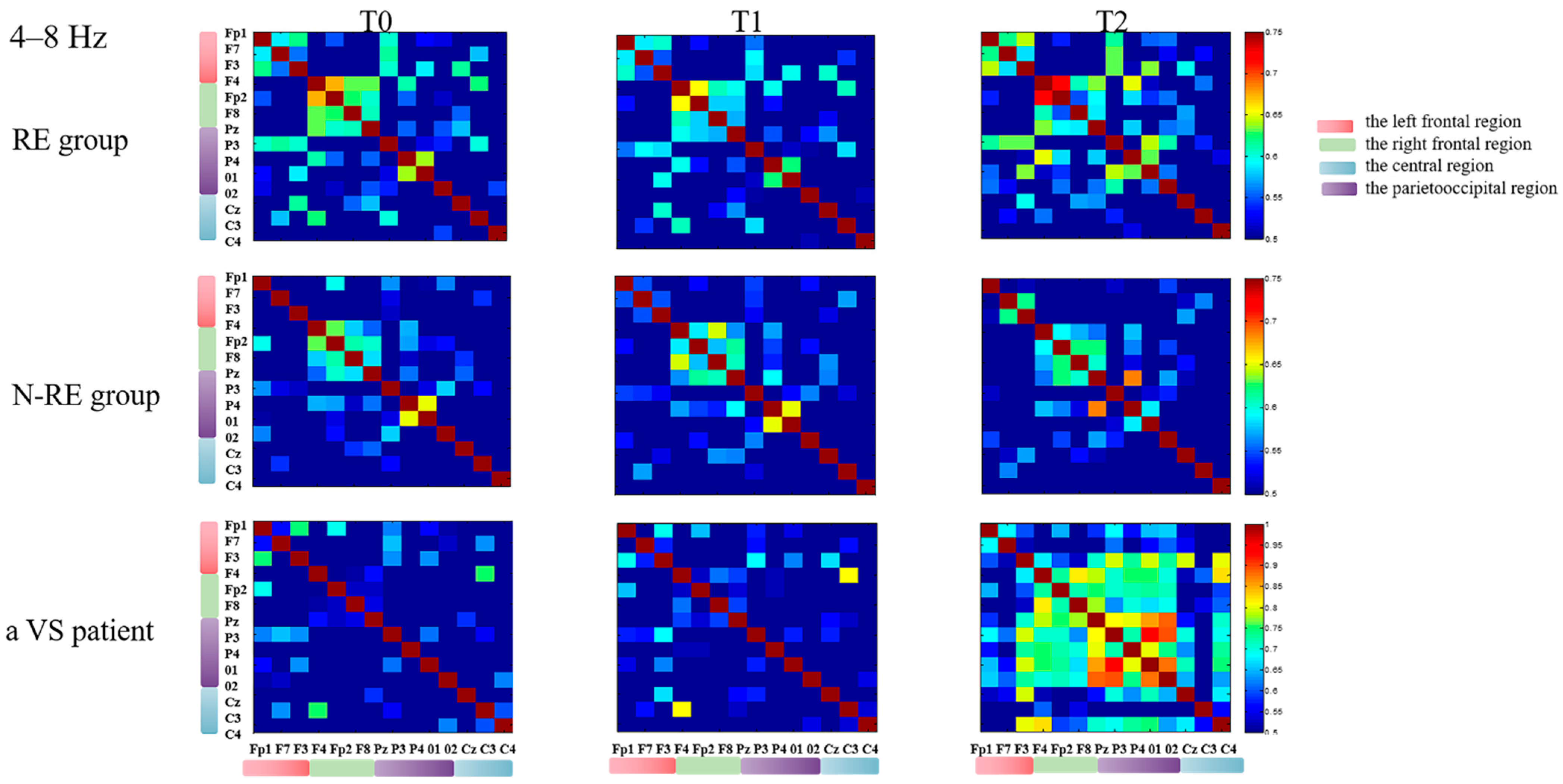
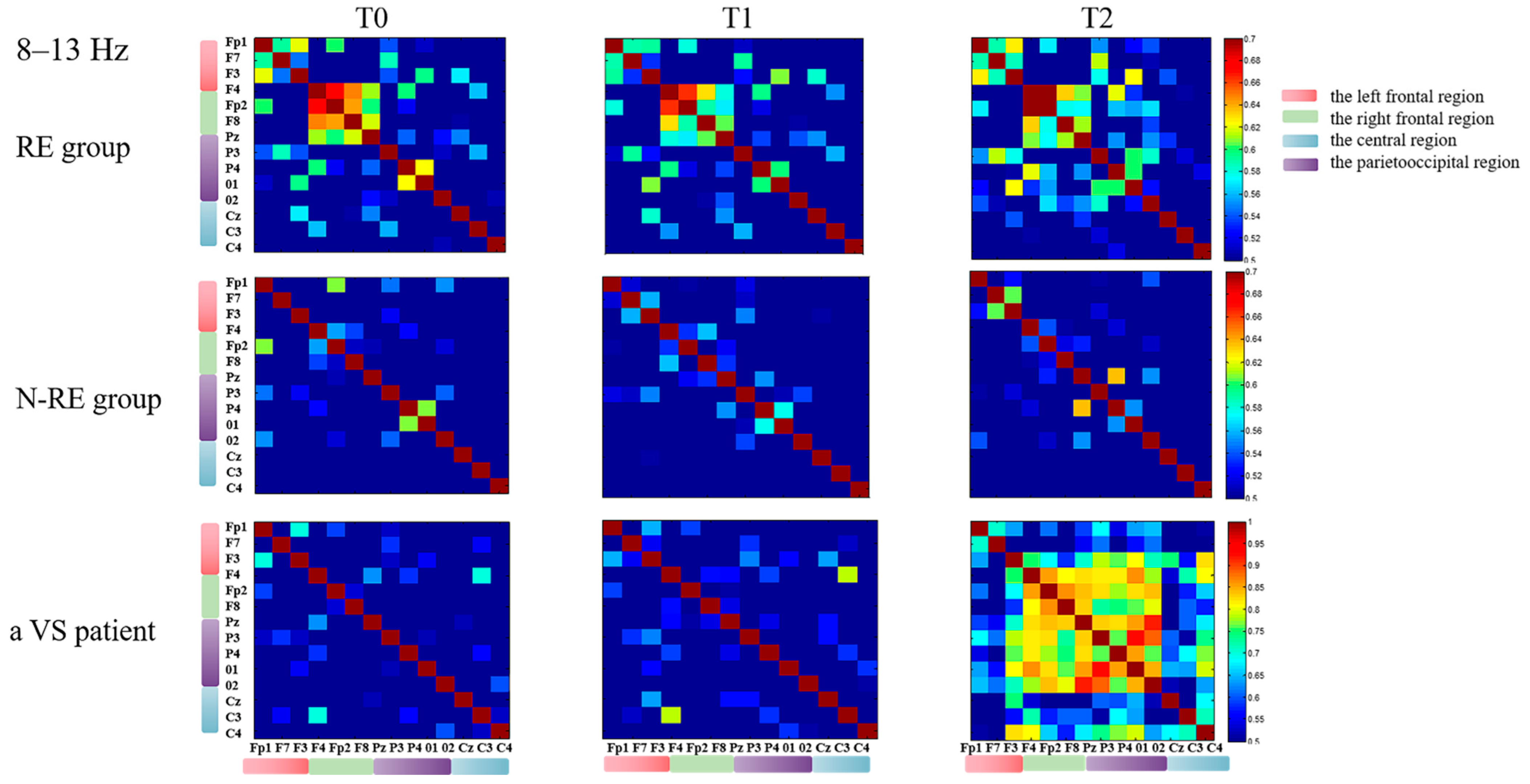
3.2. Electroencephalographic Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethics Statement
References
- Sitt, J.D.; King, J.-R.; El Karoui, I.; Rohaut, B.; Faugeras, F.; Gramfort, A.; Cohen, L.; Sigman, M.; Dehaene, S.; Naccache, L. Large scale screening of neural signatures of consciousness in patients in a vegetative or minimally conscious state. Brain 2014, 137, 2258–2270. [Google Scholar] [CrossRef] [PubMed]
- Thul, A.; Lechinger, J.; Donis, J.; Michitsch, G.; Pichler, G.; Kochs, E.F.; Jordan, D.; Ilg, R.; Schabus, M. EEG entropy measures indicate decrease of cortical information processing in Disorders of Consciousness. Clin. Neurophysiol. 2016, 127, 1419–1427. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J. Disorders of Consciousness in China. Neurosci. Bull. 2018, 34, 605–614. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, M.J.; Giacino, J.T.; Katz, D.I.; Schiff, N.D.; Whyte, J.; Ashman, E.J.; Ashwal, S.; Barbano, R.; Hammond, F.M.; Laureys, S.; et al. Author response: Practice guideline update recommendations summary: Disorders of consciousness: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology; the American Congress of Rehabilitation Medicine; and the National Institute on Disability, Independent Living, and Rehabilitation Research. Neurology 2018, 92, 1164. [Google Scholar]
- Lefaucheur, J.-P.; Antal, A.; Ayache, S.S.; Benninger, D.H.; Brunelin, J.; Cogiamanian, F.; Cotelli, M.; De Ridder, D.; Ferrucci, R.; Langguth, B.; et al. Evidence-based guidelines on the therapeutic use of transcranial direct current stimulation (tDCS). Clin. Neurophysiol. 2017, 128, 56–92. [Google Scholar] [CrossRef]
- Thibaut, A.; Bruno, M.-A.; LeDoux, D.; Demertzi, A.; Laureys, S. tDCS in patients with disorders of consciousness: Sham-controlled randomized double-blind study. Neurology 2014, 82, 1112–1118. [Google Scholar] [CrossRef]
- Han, J.; Chen, C.; Zheng, S.; Yan, X.; Wang, C.; Wang, K.; Hu, Y. High-Definition Transcranial Direct Current Stimulation of the Dorsolateral Prefrontal Cortex Modulates the Electroencephalography Rhythmic Activity of Parietal Occipital Lobe in Patients With Chronic Disorders of Consciousness. Front. Hum. Neurosci. 2022, 16, 889023. [Google Scholar] [CrossRef]
- Datta, A.; Bansal, V.; Diaz, J.; Patel, J.; Reato, D.; Bikson, M. Gyri-precise head model of transcranial direct current stimulation: Improved spatial focality using a ring electrode versus conventional rectangular pad. Brain Stimul. 2009, 2, 201–207.e1. [Google Scholar] [CrossRef]
- Dmochowski, J.P.; Datta, A.; Bikson, M.; Su, Y.; Parra, L.C. Optimized multi-electrode stimulation increases focality and intensity at target. J. Neural Eng. 2011, 8, 046011. [Google Scholar] [CrossRef]
- Shekhawat, G.S.; Vanneste, S. High-definition transcranial direct current stimulation of the dorsolateral prefrontal cortex for tinnitus modulation: A preliminary trial. J. Neural Transm. 2018, 125, 163–171. [Google Scholar] [CrossRef]
- Hummel, F.C.; Cohen, L.G. Non-invasive brain stimulation: A new strategy to improve neurorehabilitation after stroke? Lancet Neurol. 2006, 5, 708–712. [Google Scholar] [CrossRef]
- O’Reilly, J.X.; Beckmann, C.F.; Tomassini, V.; Ramnani, N.; Johansen-Berg, H. Distinct and overlapping functional zones in the cerebellum defined by resting state functional connectivity. Cereb. Cortex 2010, 20, 953–965. [Google Scholar] [CrossRef] [PubMed]
- Martens, G.; Kroupi, E.; Bodien, Y.; Frasso, G.; Annen, J.; Cassol, H.; Barra, A.; Martial, C.; Gosseries, O.; Lejeune, N.; et al. Behavioral and electrophysiological effects of network-based frontoparietal tDCS in patients with severe brain injury: A randomized controlled trial. NeuroImage Clin. 2020, 28, 102426. [Google Scholar] [CrossRef] [PubMed]
- Thibaut, A.; Chennu, S.; Chatelle, C.; Martens, G.; Annen, J.; Cassol, H.; Laureys, S. Theta network centrality correlates with tDCS response in disorders of consciousness. Brain Stimul. 2018, 11, 1407–1409. [Google Scholar] [CrossRef]
- Thibaut, A.; Schiff, N.; Giacino, J.; Laureys, S.; Gosseries, O. Therapeutic interventions in patients with prolonged disorders of consciousness. Lancet Neurol. 2019, 18, 600–614. [Google Scholar] [CrossRef]
- Zhang, R.; Zhang, L.; Guo, Y.; Shi, L.; Gao, J.; Wang, X.; Hu, Y. Effects of High-Definition Transcranial Direct-Current Stimulation on Resting-State Functional Connectivity in Patients With Disorders of Consciousness. Front. Hum. Neurosci. 2020, 14, 560586. [Google Scholar] [CrossRef]
- El-Hagrassy, M.M.; Duarte, D.; Lu, J.; Uygur-Kucukseymen, E.; Münger, M.; Thibaut, A.; Lv, P.; Morales-Quezada, L.; Fregni, F. EEG modulation by different transcranial direct current stimulation (tDCS) montages: A randomized double-blind sham-control mechanistic pilot trial in healthy participants. Expert Rev. Med. Devices 2020, 18, 107–120. [Google Scholar] [CrossRef]
- Bagnato, S.; Boccagni, C.; Prestandrea, C.; Sant’Angelo, A.; Castiglione, A.; Galardi, G. Prognostic value of standard EEG in traumatic and non-traumatic disorders of consciousness following coma. Clin. Neurophysiol. 2010, 121, 274–280. [Google Scholar] [CrossRef]
- Miller, E.K.; Cohen, J.D. An integrative theory of prefrontal cortex function. Annu. Rev. Neurosci. 2001, 24, 167–202. [Google Scholar] [CrossRef]
- Lafontaine, M.P.; Théoret, H.; Gosselin, F.; Lippé, S. Transcranial direct current stimulation of the dorsolateral prefrontal cortex modulates repetition suppression to unfamiliar faces: An ERP study. PLoS ONE 2013, 8, e81721. [Google Scholar] [CrossRef]
- Zhang, Y.; Song, W.; Du, J.; Huo, S.; Shan, G.; Li, R. Transcranial Direct Current Stimulation in Patients with Prolonged Disorders of Consciousness: Combined Behavioral and Event-Related Potential Evidence. Front. Neurol. 2017, 8, 620. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Xia, X.; Wang, Y.; Guo, Y.; Yang, Y.; He, J.; Li, X. Fronto-parietal coherence response to tDCS modulation in patients with disorders of consciousness. Int. J. Neurosci. 2018, 128, 587–594. [Google Scholar] [CrossRef] [PubMed]
- Angelakis, E.; Liouta, E.; Andreadis, N.; Korfias, S.; Ktonas, P.; Stranjalis, G.; Sakas, D.E. Transcranial direct current stimulation effects in disorders of consciousness. Arch. Phys. Med. Rehabil. 2014, 95, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Golland, Y.; Bentin, S.; Gelbard, H.; Benjamini, Y.; Heller, R.; Nir, Y.; Hasson, U.; Malach, R. Extrinsic and intrinsic systems in the posterior cortex of the human brain revealed during natural sensory stimulation. Cereb. Cortex 2007, 17, 766–777. [Google Scholar] [CrossRef]
- Fox, M.D.; Snyder, A.Z.; Vincent, J.L.; Corbetta, M.; Van Essen, D.C.; Raichle, M.E. From The Cover: The human brain is intrinsically organized into dynamic, anticorrelated functional networks. Proc. Natl. Acad. Sci. USA 2005, 102, 9673–9678. [Google Scholar] [CrossRef]
- Tononi, G.; Koch, C. The neural correlates of consciousness: An update. Ann. N. Y. Acad. Sci. 2008, 1124, 239–261. [Google Scholar] [CrossRef]
- Monti, M.M.; Rosenberg, M.; Finoia, P.; Kamau, E.; Pickard, J.D.; Owen, A.M. Thalamo-frontal connectivity mediates top-down cognitive functions in disorders of consciousness. Neurology 2014, 84, 167–173. [Google Scholar] [CrossRef]
- Schiff, N.D.; Nauvel, T.; Victor, J.D. Large-scale brain dynamics in disorders of consciousness. Curr. Opin. Neurobiol. 2014, 25, 7–14. [Google Scholar] [CrossRef]
- Boly, M.B.; Faymonville, M.; Peigneux, P.; Lambermont, B.; Damas, P.; del Fiore, G.; Degueldre, C.; Franck, G.; Luxen, A.; Lamy, M.; et al. Auditory processing in severely brain injured patients: Differences between the minimally conscious state and the persistent vegetative state. Arch. Neurol. 2004, 61, 233–238. [Google Scholar]
- Laureys, S.; Boly, M.; Maquet, P. Tracking the recovery of consciousness from coma. J. Clin. Investig. 2006, 116, 1823–1825. [Google Scholar] [CrossRef]
- Giacino, J.T.; Kalmar, K.; Whyte, J. The JFK Coma Recovery Scale-Revised: Measurement characteristics and diagnostic utility. Arch. Phys. Med. Rehabil. 2004, 85, 2020–2029. [Google Scholar] [CrossRef] [PubMed]
- Bagnato, S.; Boccagni, C.; Sant’Angelo, A.; Prestandrea, C.; Mazzilli, R.; Galardi, G. EEG predictors of outcome in patients with disorders of consciousness admitted for intensive rehabilitation. Clin. Neurophysiol. 2015, 126, 959–966. [Google Scholar] [CrossRef] [PubMed]
- Gerrard, P.; Zafonte, R.; Giacino, J.T. Coma recovery scale–revised: Evidentiary support for hierarchical grading of level of consciousness. Arch. Phys. Med. Rehabil. 2014, 95, 2335–2341. [Google Scholar] [CrossRef]
- Bruno, M.-A.; Vanhaudenhuyse, A.; Thibaut, A.; Moonen, G.; Laureys, S. From unresponsive wakefulness to minimally conscious PLUS and functional locked-in syndromes: Recent advances in our understanding of disorders of consciousness. J. Neurol. 2011, 258, 1373–1384. [Google Scholar] [CrossRef] [PubMed]
- Gosseries, O.; Vanhaudenhuyse, A.; Bruno, M.-A.; Demertzi, A.; Schnakers, C.; Boly, M.M.; Maudoux, A.; Moonen, G.; Laureys, S. Disorders of Consciousness: Coma, Vegetative and Minimally Conscious States. In The Frontiers Collection; Springer: Berlin/Heidelberg, Germany, 2011; pp. 29–55. [Google Scholar]
- Gui, P.; Jiang, Y.; Zang, D.; Qi, Z.; Tan, J.; Tanigawa, H.; Jiang, J.; Wen, Y.; Xu, L.; Zhao, J.; et al. Assessing the depth of language processing in patients with disorders of consciousness. Nat. Neurosci. 2020, 23, 761–770. [Google Scholar] [CrossRef]
- Jung, T.-P.; Makeig, S.; Westerfield, M.; Townsend, J.; Courchesne, E.; Sejnowski, T.J. Removal of eye activity artifacts from visual event-related potentials in normal and clinical subjects. Clin. Neurophysiol. 2000, 111, 1745–1758. [Google Scholar] [CrossRef]
- He, R.; Fan, J.; Wang, H.; Zhong, Y.; Ma, J. Differentiating Responders and Non-responders to rTMS Treatment for Disorder of Consciousness Using EEG After-Effects. Front. Neurol. 2020, 11, 583268. [Google Scholar] [CrossRef]
- WWu, M.; Yu, Y.; Luo, L.; Wu, Y.; Gao, J.; Ye, X.; Luo, B. Efficiency of Repetitive Transcranial Direct Current Stimulation of the Dorsolateral Prefrontal Cortex in Disorders of Consciousness: A Randomized Sham-Controlled Study. Neural Plast. 2019, 2019, 7089543. [Google Scholar]
- Bai, Y.; Xia, X.; Liang, Z.; Wang, Y.; Yang, Y.; He, J.; Li, X. Frontal Connectivity in EEG Gamma (30-45 Hz) Respond to Spinal Cord Stimulation in Minimally Conscious State Patients. Front. Cell. Neurosci. 2017, 11, 177. [Google Scholar] [CrossRef]
- Sauseng, P.; Klimesch, W.; Freunberger, R.; Pecherstorfer, T.; Hanslmayr, S.; Doppelmayr, M. Relevance of EEG alpha and theta oscillations during task switching. Exp. Brain Res. 2006, 170, 295–301. [Google Scholar] [CrossRef]
- Lehembre, R.; Marie-Aurélie, B.; Vanhaudenhuyse, A.; Chatelle, C.; Cologan, V.; Leclercq, Y.; Soddu, A.; Macq, B.; Laureys, S.; Noirhomme, Q. Resting-state EEG study of comatose patients: A connectivity and frequency analysis to find differences between vegetative and minimally conscious states. Funct. Neurol. 2012, 27, 41–47. [Google Scholar] [PubMed]
- Jensen, O.; Tesche, C.D. Frontal theta activity in humans increases with memory load in a working memory task. Eur. J. Neurosci. 2002, 15, 1395–1399. [Google Scholar] [CrossRef] [PubMed]
- Pupíková, M.; Šimko, P.; Gajdoš, M.; Rektorová, I. Modulation of Working Memory and Resting-State fMRI by tDCS of the Right Frontoparietal Network. Neural Plast. 2021, 2021, 5594305. [Google Scholar] [CrossRef]
- Keeser, D.; Meindl, T.; Bor, J.; Palm, U.; Pogarell, O.; Mulert, C.; Brunelin, J.; Möller, H.-J.; Reiser, M.; Padberg, F. Prefrontal transcranial direct current stimulation changes connectivity of resting-state networks during fMRI. J. Neurosci. 2011, 31, 15284–15293. [Google Scholar] [CrossRef]
- Liang, Z.; Li, J.; Xia, X.; Wang, Y.; Li, X.; He, J.; Bai, Y. Long-Range Temporal Correlations of Patients in Minimally Conscious State Modulated by Spinal Cord Stimulation. Front. Physiol. 2018, 9, 1511. [Google Scholar] [CrossRef] [PubMed]
- Rosenblum, M.; Pikovsky, A.; Kurths, J.; Schäfer, C.; Tass, P. Chapter 9 Phase synchronization: From theory to data analysis. Handb. Biol. Phys. 2001, 4, 279–321. [Google Scholar]
- Vlisides, P.; Bel-Bahar, T.; Nelson, A.; Chilton, K.; Smith, E.; Janke, E.; Tarnal, V.; Picton, P.; Harris, R.; Mashour, G. Subanaesthetic ketamine and altered states of consciousness in humans. Br. J. Anaesth. 2018, 121, 249–259. [Google Scholar] [CrossRef]
- Chennu, S.; Annen, J.; Wannez, S.; Thibaut, A.; Chatelle, C.; Cassol, H.; Martens, G.; Schnakers, C.; Gosseries, O.; Menon, D.; et al. Brain networks predict metabolism, diagnosis and prognosis at the bedside in disorders of consciousness. Brain 2017, 140, 2120–2132. [Google Scholar] [CrossRef]
- D’Esposito, M.; Postle, B.R. The cognitive neuroscience of working memory. Annu. Rev. Psychol. 2015, 66, 115–142. [Google Scholar] [CrossRef]
- Hermann, B.; Raimondo, F.; Hirsch, L.; Huang, Y.; Denis-Valente, M.; Pérez, P.; Engemann, D.; Faugeras, F.; Weiss, N.; Demeret, S.; et al. Combined behavioral and electrophysiological evidence for a direct cortical effect of prefrontal tDCS on disorders of consciousness. Sci. Rep. 2020, 10, 4323. [Google Scholar] [CrossRef]
- Huang, H.; Niu, Z.; Liu, G.; Jiang, M.; Jia, Q.; Li, X.; Su, Y. Early Consciousness Disorder in Acute Large Hemispheric Infarction: An Analysis Based on Quantitative EEG and Brain Network Characteristics. Neurocritical Care 2020, 33, 376–388. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Zou, Q.; Hu, J.; Tang, W.; Mao, Y.; Gao, L.; Zhu, J.; Jin, Y.; Lu, L.; Zhang, Y.; et al. Intrinsic Functional Connectivity Patterns Predict Consciousness Level and Recovery Outcome in Acquired Brain Injury. J. Neurosci. 2015, 35, 12932–12946. [Google Scholar] [CrossRef]
- Vanhaudenhuyse, A.; Demertzi, A.; Schabus, M.; Noirhomme, Q.; Bredart, S.; Boly, M.; Phillips, C.; Soddu, A.; Luxen, A.; Moonen, G.; et al. Two distinct neuronal networks mediate the awareness of environment and of self. J. Cogn. Neurosci. 2011, 23, 570–578. [Google Scholar] [CrossRef] [PubMed]
- Cavaliere, C.; Aiello, M.; Di Perri, C.; Amico, E.; Martial, C.; Thibaut, A.; Laureys, S.; Soddu, A. Functional Connectivity Substrates for tDCS Response in Minimally Conscious State Patients. Front. Cell. Neurosci. 2016, 10, 257. [Google Scholar] [CrossRef] [PubMed]
- Cavinato, M.; Genna, C.; Formaggio, E.; Gregorio, C.; Storti, S.F.; Manganotti, P.; Casanova, E.; Piperno, R.; Piccione, F. Behavioural and electrophysiological effects of tDCS to prefrontal cortex in patients with disorders of consciousness. Clin. Neurophysiol. 2019, 130, 231–238. [Google Scholar] [CrossRef]
- Chennu, S.; Finoia, P.; Kamau, E.; Allanson, J.; Williams, G.B.; Monti, M.M.; Noreika, V.; Arnatkeviciute, A.; Canales-Johnson, A.; Olivares, F.; et al. Spectral signatures of reorganised brain networks in disorders of consciousness. PLoS Comput. Biol. 2014, 10, e1003887. [Google Scholar] [CrossRef]
- Demertzi, A.; Antonopoulos, G.; Heine, L.; Voss, H.U.; Crone, J.S.; Angeles, C.D.L.; Bahri, M.A.; Di Perri, C.; Vanhaudenhuyse, A.; Charland-Verville, V.; et al. Intrinsic functional connectivity differentiates minimally conscious from unresponsive patients. Brain 2015, 138, 2619–2631. [Google Scholar] [CrossRef]
- Giacino, J.T.; Sherer, M.; Christoforou, A.; Maurer-Karattup, P.; Hammond, F.M.; Long, D.; Bagiella, E. Behavioral Recovery and Early Decision Making in Patients with Prolonged Disturbance in Consciousness after Traumatic Brain Injury. J. Neurotrauma 2020, 37, 357–365. [Google Scholar] [CrossRef]
- Hirschberg, R.; Giacino, J.T. The vegetative and minimally conscious states: Diagnosis, prognosis and treatment. Neurol. Clin. 2011, 29, 773–786. [Google Scholar] [CrossRef]
- Rivera-Lillo, G.; Stamatakis, E.A.; Bekinschtein, T.A.; Menon, D.K.; Chennu, S. Delta band activity contributes to the identification of command following in disorder of consciousness. Sci. Rep. 2021, 11, 16267. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | Sex | Age | Etiology | Days Post- Injury | T0 (CRS-R) (A-Vi-M-Ve-C-Ar) | T0—Clinical Diagnosis | T1 (CRS-R) (A-Vi-M-Ve-C-Ar) | T1—Clinical Diagnosis | T2 (CRS-R) (A-Vi-M-Ve-C-Ar) | T2—Clinical Diagnosis | Follow-Up at 3 Months (CRS-R) (A-Vi-M-Ve-C-Ar) | Follow-Up at 3 Months—Clinical Diagnosis |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| RE1 | M | 52 | Trauma | 84 | 11(1/3/4/1/1/1) | MCS+ | 11(1/3/4/1/1/1) | MCS+ | 12(2/3/4/1/1/1) | MCS+ | 18(3/4/6/1/1/3) | EMCS |
| RE2 | F | 49 | HIE | 30 | 6(1/1/3/0/0/1) | MCS- | 7(2/1/3/0/0/1) | MCS- | 15(3/3/5/2/1/1) | MCS+ | 20(3/4/5/3/2/3) | EMCS |
| RE3 | M | 53 | Trauma | 34 | 5(0/0/5/0/0/0) | MCS- | 7(0/0/5/1/0/1) | MCS- | 14(3/2/5/2/1/1) | MCS+ | 23(4/5/6/3/2/3) | EMCS |
| RE4 | F | 74 | Hemorrhage | 101 | 11(2/3/3/0/1/2) | MCS+ | 11(2/3/3/0/1/2) | MCS+ | 15(3/4/5/0/1/2) | MCS+ | / | Dead |
| RE5 | M | 49 | Hemorrhage | 50 | 5(1/1/1/0/0/2) | VS | 6(1/1/1/1/0/2) | VS | 7(1/1/2/1/0/2) | VS | 8(1/2/2/1/0/2) | VS |
| RE6 | M | 55 | Trauma | 302 | 6(1/2/1/0/0/2) | VS | 6(1/2/1/0/0/2) | VS | 8(2/3/1/0/0/2) | MCS- | 8(2/3/1/0/0/2) | MCS- |
| RE7 | M | 72 | Cerebral infarction | 42 | 5(1/3/0/0/0/1) | MCS- | 5(1/3/0/0/0/1) | MCS- | 9(2/3/0/2/1/1) | MCS+ | 13(3/3/0/3/1/3) | MCS+ |
| RE8 | M | 47 | Hemorrhage | 29 | 6(1/1/2/1/0/1) | VS | 6(1/1/2/1/0/1) | VS | 12(2/3/3/1/1/2) | MCS+ | 14(2/4/3/1/1/3) | MCS+ |
| RE9 | M | 58 | Trauma | 53 | 9(2/3/2/0/0/2) | MCS- | 9(2/3/2/0/0/2) | MCS- | 10(2/3/2/1/0/2) | MCS- | 22(4/4/6/3/2/3) | EMCS |
| RE10 | F | 68 | Hemorrhage | 30 | 8(2/1/3/0/0/2) | MCS- | 9(3/1/3/0/0/2) | MCS+ | 15(3/4/5/0/0/3) | MCS+ | 18(3/4/5/2/1/3) | MCS+ |
| RE11 | M | 59 | Cerebral infarction | 68 | 5(2/1/0/0/0/2) | VS | 5(2/1/0/0/0/2) | VS | 6(3/1/0/0/0/2) | MCS+ | 15(4/3/5/0/1/2) | MCS+ |
| RE12 # | M | 37 | HIE | 35 | 10(1/2/5/0/1/1) | MCS+ | 10(1/2/5/0/1/1) | MCS+ | 11(2/2/5/0/1/1) | MCS+ | 18(3/5/6/0/2/2) | EMCS |
| RE13 # | M | 72 | Cerebral infarction | 200 | 2(1/1/0/0/0/0) | VS | 2(1/1/0/0/0/0) | VS | 4(1/1/1/0/0/1) | VS | 5(1/2/1/0/0/1) | VS |
| N-RE1 | M | 54 | Hemorrhage | 73 | 6(1/1/2/0/0/2) | VS | 6(1/1/2/0/0/2) | VS | 6(1/1/2/0/0/2) | VS | 6(1/1/2/0/0/2) | VS |
| N-RE2 | M | 56 | HIE | 41 | 2(0/0/0/0/0/2) | VS | 2(0/0/0/0/0/2) | VS | 2(0/0/0/0/0/2) | VS | 4(0/0/1/1/0/2) | VS |
| N-RE3 | F | 39 | HIE | 128 | 4(0/0/2/0/0/2) | VS | 4(0/0/2/0/0/2) | VS | 4(0/0/2/0/0/2) | VS | 5(1/0/2/0/0/2) | VS |
| N-RE4 | M | 18 | Disseminated cerebrospinalmeningits | 48 | 4(1/1/0/0/0/2) | VS | 4(1/1/0/0/0/2) | VS | 4(1/1/0/0/0/2) | VS | 7(2/2/0/1/0/2) | MCS- |
| N-RE5 | M | 56 | Hemorrhage | 88 | 3(0/0/1/0/0/2) | VS | 3(0/0/1/0/0/2) | VS | 3(0/0/1/0/0/2) | VS | 5(1/1/1/0/0/2) | VS |
| N-RE6 | M | 64 | Hemorrhage | 34 | 10(1/1/5/0/1/2) | MCS- | 10(1/1/5/0/1/2) | MCS- | 10(1/1/5/0/1/2) | MCS- | 12(2/1/5/0/1/3) | MCS+ |
| N-RE7 | F | 70 | Cerebral infarction | 58 | 4(1/1/0/1/0/1) | VS | 4(1/1/0/1/0/1) | VS | 4(1/1/0/1/0/1) | VS | 7(1/1/0/2/1/2) | MCS- |
| N-RE8 | F | 39 | HIE | 215 | 3(0/0/0/1/0/2) | VS | 3(0/0/0/1/0/2) | VS | 3(0/0/0/1/0/2) | VS | 4(1/0/0/1/0/2) | VS |
| N-RE9 # | M | 57 | Hemorrhage | 52 | 6(1/1/2/0/0/2) | VS | 6(1/1/2/0/0/2) | VS | 6(1/1/2/0/0/2) | VS | 14(2/2/4/2/1/3) | MCS+ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, J.; Chen, C.; Zheng, S.; Zhou, T.; Hu, S.; Yan, X.; Wang, C.; Wang, K.; Hu, Y. Functional Connectivity Increases in Response to High-Definition Transcranial Direct Current Stimulation in Patients with Chronic Disorder of Consciousness. Brain Sci. 2022, 12, 1095. https://doi.org/10.3390/brainsci12081095
Han J, Chen C, Zheng S, Zhou T, Hu S, Yan X, Wang C, Wang K, Hu Y. Functional Connectivity Increases in Response to High-Definition Transcranial Direct Current Stimulation in Patients with Chronic Disorder of Consciousness. Brain Sciences. 2022; 12(8):1095. https://doi.org/10.3390/brainsci12081095
Chicago/Turabian StyleHan, Jinying, Chen Chen, Shuang Zheng, Ting Zhou, Shunyin Hu, Xiaoxiang Yan, Changqing Wang, Kai Wang, and Yajuan Hu. 2022. "Functional Connectivity Increases in Response to High-Definition Transcranial Direct Current Stimulation in Patients with Chronic Disorder of Consciousness" Brain Sciences 12, no. 8: 1095. https://doi.org/10.3390/brainsci12081095