
Clinical Results of Flow Diverter Treatments for Cerebral Aneurysms under Local Anesthesia

 ,
,  , and
, and
Abstract
:1. Introduction
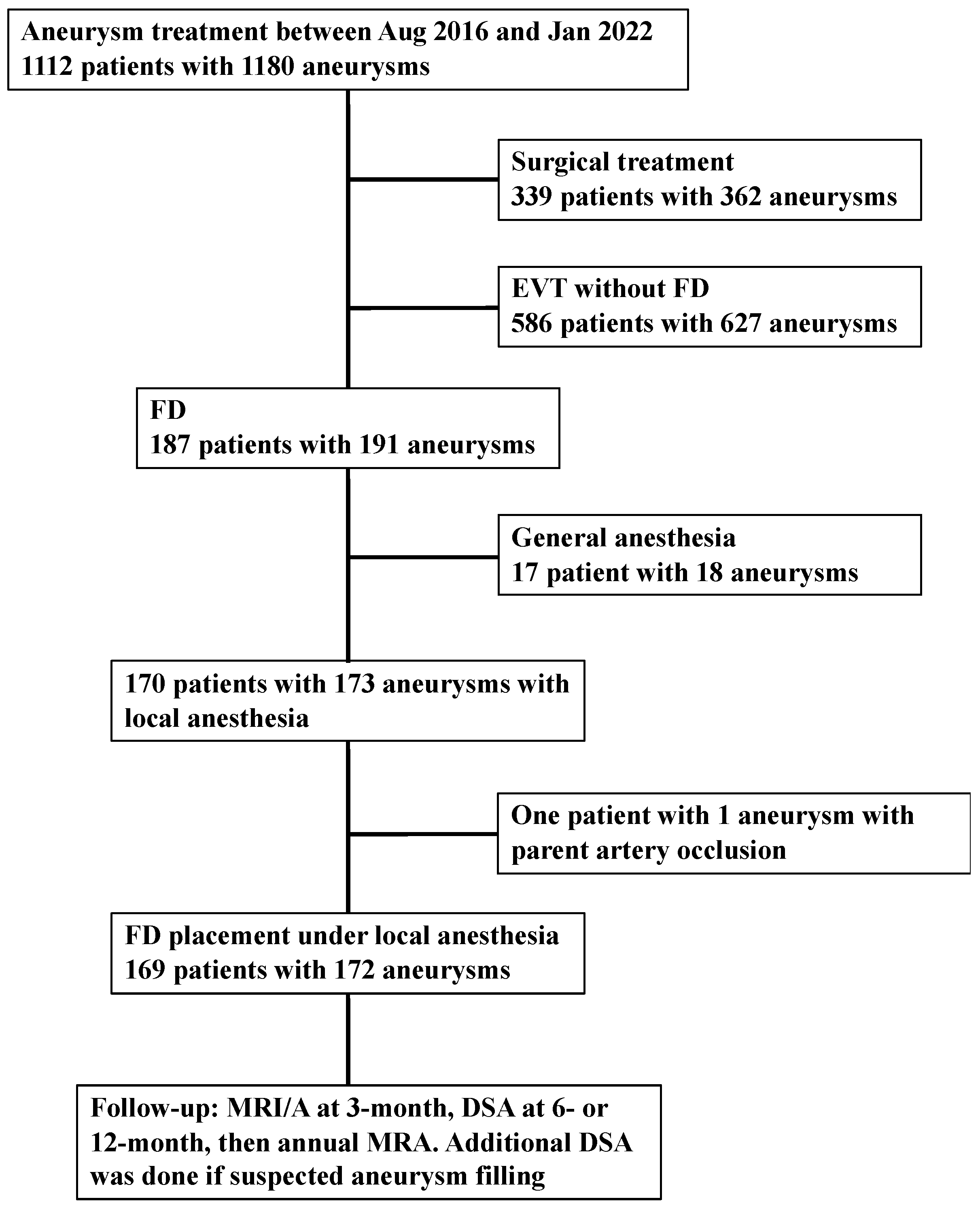
2. Materials and Methods
2.1. Outcomes
2.2. Statistics
3. Results
Outcome
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Briganti, F.; Napoli, M.; Tortora, F.; Solari, D.; Bergui, M.; Boccardi, E.; Cagliari, E.; Castellan, L.; Causin, F.; Ciceri, E.; et al. Italian Multicenter Experience with Flow-Diverter Devices for Intracranial Unruptured Aneurysm Treatment with Periprocedural Complications—A Retrospective Data Analysis. Neuroradiology 2012, 54, 1145–1152. [Google Scholar] [CrossRef] [PubMed]
- Arrese, I.; Sarabia, R.; Pintado, R.; Delgado-Rodriguez, M. Flow-Diverter Devices for Intracranial Aneurysms: Systematic Review and Meta-Analysis. Neurosurgery 2013, 73, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Brinjikji, W.; Murad, M.H.; Lanzino, G.; Cloft, H.J.; Kallmes, D.F. Endovascular Treatment of Intracranial Aneurysms with Flow Diverters: A Meta-Analysis. Stroke 2013, 44, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Abou-Chebl, A.; Lin, R.; Shazam Hussain, M.; Jovin, T.G.; Levy, E.I.; Liebeskind, D.S.; Yoo, A.J.; Hsu, D.P.; Rymer, M.M.; Tayal, A.H.; et al. Conscious Sedation versus General Anesthesia during Endovascular Therapy for Acute Anterior Circulation Stroke: Preliminary Results from a Retrospective, Multicenter Study. Stroke 2010, 41, 1175–1179. [Google Scholar] [CrossRef]
- Brinjikji, W.; Murad, M.H.; Rabinstein, A.A.; Cloft, H.J.; Lanzino, G.; Kallmes, D.F. Conscious Sedation versus General Anesthesia during Endovascular Acute Ischemic Stroke Treatment: A Systematic Review and Meta-Analysis. AJNR. Am. J. Neuroradiol. 2015, 36, 525–529. [Google Scholar] [CrossRef]
- Ito, S.; Iwata, S.; Kondo, I.; Iwade, M.; Ozaki, M.; Ishikawa, T.; Kawamata, T. Esophageal Submucosal Hematoma Developed after Endovascular Surgery for Unruptured Cerebral Aneurysm under General Anesthesia: A Case Report. JA Clin. Rep. 2017, 3, 54. [Google Scholar] [CrossRef]
- Siddiqui, A.H.; Kan, P.; Abla, A.A.; Hopkins, L.N.; Levy, E.I. Complications after Treatment with Pipeline Embolization for Giant Distal Intracranial Aneurysms with or without Coil Embolization. Neurosurgery 2012, 71, E509–E513. [Google Scholar] [CrossRef]
- Chalouhi, N.; Chitale, R.; Starke, R.M.; Jabbour, P.; Tjoumakaris, S.; Dumont, A.S.; Rosenwasser, R.H.; Gonzalez, L.F. Treatment of Recurrent Intracranial Aneurysms with the Pipeline Embolization Device. J. Neurointerv. Surg. 2014, 6, 19–23. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Van Swieten, J.C.; Koudstaal, P.J.; Visser, M.C.; Schouten, H.; Van Gijn, J. Interobserver Agreement for the Assessment of Handicap in Stroke Patients. Stroke 1988, 19, 604–607. [Google Scholar] [CrossRef]
- O’Kelly, C.J.; Krings, T.; Fiorella, D.; Marotta, T.R. A Novel Grading Scale for the Angiographic Assessment of Intracranial Aneurysms Treated Using Flow Diverting Stents. Interv. Neuroradiol. 2010, 16, 133. [Google Scholar] [CrossRef]
- Xiang, S.; Fan, F.; Hu, P.; Yang, K.; Zhai, X.; Geng, J.; Ji, Z.; Lu, J.; Zhang, H. The Sensitivity and Specificity of TOF-MRA Compared with DSA in the Follow-up of Treated Intracranial Aneurysms. J. Neurointerv. Surg. 2021, 13, 1172–1179. [Google Scholar] [CrossRef]
- Becske, T.; Kallmes, D.F.; Saatci, I.; McDougall, C.G.; Szikora, I.; Lanzino, G.; Moran, C.J.; Woo, H.H.; Lopes, D.K.; Berez, A.L.; et al. Pipeline for Uncoilable or Failed Aneurysms: Results from a Multicenter Clinical Trial. Radiology 2013, 267, 858–868. [Google Scholar] [CrossRef]
- Pierot, L.; Spelle, L.; Berge, J.; Januel, A.C.; Herbreteau, D.; Aggour, M.; Piotin, M.; Biondi, A.; Barreau, X.; Mounayer, C.; et al. SAFE Study (Safety and Efficacy Analysis of FRED Embolic Device in Aneurysm Treatment): 1-Year Clinical and Anatomical Results. J. Neurointerv. Surg. 2019, 11, 184–189. [Google Scholar] [CrossRef]
- Nelson, P.K.; Lylyk, P.; Szikora, I.; Wetzel, S.G.; Wanke, I.; Fiorella, D. The Pipeline Embolization Device for the Intracranial Treatment of Aneurysms Trial. AJNR. Am. J. Neuroradiol. 2011, 32, 34–40. [Google Scholar] [CrossRef]
- Becske, T.; Potts, M.B.; Shapiro, M.; Kallmes, D.F.; Brinjikji, W.; Saatci, I.; McDougall, C.G.; Szikora, I.; Lanzino, G.; Moran, C.J.; et al. Pipeline for Uncoilable or Failed Aneurysms: 3-Year Follow-up Results. J. Neurosurg. 2017, 127, 81–88. [Google Scholar] [CrossRef]
- Kallmes, D.F.; Brinjikji, W.; Boccardi, E.; Ciceri, E.; Diaz, O.; Tawk, R.; Woo, H.; Jabbour, P.; Albuquerque, F.; Chapot, R.; et al. Aneurysm Study of Pipeline in an Observational Registry (ASPIRe). Interv. Neurol. 2016, 5, 89–99. [Google Scholar] [CrossRef]
- Kallmes, D.F.; Hanel, R.; Lopes, D.; Boccardi, E.; Bonafé, A.; Cekirge, S.; Fiorella, D.; Jabbour, P.; Levy, E.; McDougall, C.; et al. International Retrospective Study of the Pipeline Embolization Device: A Multicenter Aneurysm Treatment Study. Am. J. Neuroradiol. 2015, 36, 108–115. [Google Scholar] [CrossRef]
- Chiu, A.H.Y.; Cheung, A.K.; Wenderoth, J.D.; De Villiers, L.; Rice, H.; Phatouros, C.C.; Singh, T.P.; Phillips, T.J.; McAuliffe, W. Long-Term Follow-Up Results Following Elective Treatment of Unruptured Intracranial Aneurysms with the Pipeline Embolization Device. AJNR. Am. J. Neuroradiol. 2015, 36, 1728–1734. [Google Scholar] [CrossRef]
- Hanel, R.A.; Kallmes, D.F.; Lopes, D.K.; Nelson, P.K.; Siddiqui, A.; Jabbour, P.; Pereira, V.M.; Szikora István, I.; Zaidat, O.O.; Bettegowda, C.; et al. Prospective Study on Embolization of Intracranial Aneurysms with the Pipeline Device: The PREMIER Study 1 Year Results. J. Neurointerv. Surg. 2020, 12, 62–66. [Google Scholar] [CrossRef]
- Wakhloo, A.K.; Lylyk, P.; De Vries, J.; Taschner, C.; Lundquist, J.; Biondi, A.; Hartmann, M.; Szikora, I.; Pierot, L.; Sakai, N.; et al. Surpass Flow Diverter in the Treatment of Intracranial Aneurysms: A Prospective Multicenter Study. AJNR. Am. J. Neuroradiol. 2015, 36, 98–107. [Google Scholar] [CrossRef]
- Berge, J.; Biondi, A.; Machi, P.; Brunel, H.; Pierot, L.; Gabrillargues, J.; Kadziolka, K.; Barreau, X.; Dousset, V.; Bonafée, A. Flow-Diverter Silk Stent for the Treatment of Intracranial Aneurysms: 1-Year Follow-up in a Multicenter Study. AJNR. Am. J. Neuroradiol. 2012, 33, 1150–1155. [Google Scholar] [CrossRef]
- Meyers, P.M.; Coon, A.L.; Kan, P.T.; Wakhloo, A.K.; Hanel, R.A. SCENT Trial. Stroke 2019, 50, 1473–1479. [Google Scholar] [CrossRef]
- Griessenauer, C.J.; Shallwani, H.; Adeeb, N.; Gupta, R.; Rangel-Castilla, L.; Siddiqui, A.H.; Levy, E.I.; Boone, M.D.; Thomas, A.J.; Ogilvy, C.S. Conscious Sedation Versus General Anesthesia for the Treatment of Cerebral Aneurysms with Flow Diversion: A Matched Cohort Study. World Neurosurg. 2017, 102, 1–5. [Google Scholar] [CrossRef]
- Rangel-Castilla, L.; Cress, M.C.; Munich, S.A.; Sonig, A.; Krishna, C.; Gu, E.Y.; Snyder, K.V.; Hopkins, L.N.; Siddiqui, A.H.; Levy, E.I. Feasibility, Safety, and Periprocedural Complications of Pipeline Embolization for Intracranial Aneurysm Treatment under Conscious Sedation: University at Buffalo Neurosurgery Experience. Clin. Neurosurg. 2015, 11, 426–430. [Google Scholar] [CrossRef]
- Pacheco-Lopez, P.C.; Berkow, L.C.; Hillel, A.T.; Akst, L.M. Complications of Airway ManagementDiscussion. Respir. Care 2014, 59, 1006–1021. [Google Scholar] [CrossRef]
- Takeyama, E.; Wada, A.; Amano, E.; Shibuya, H. Oesophageal Submucosal Hematoma after Flow Diverter Embolization with Favourable Outcome Treated by Discontinuing Postoperative Antiplatelet Therapy for Only Three Days: A Case Report. JA Clin. Rep. 2019, 5, 2. [Google Scholar] [CrossRef]
- Arıcan, Ş.; Bakdık, S.; Hacıbeyoğlu, G.; Yılmaz, R.; Koç, O.; Tavlan, A.; Uzun, S.T. The Effects of Sevoflurane Anesthesia on Hemodynamics and Cerebral Artery Diameters in Endovascular Treatment of Intracranial Aneurysm: A Pilot Study. Ulusal Travma ve Acil Cerrahi Dergisi 2021, 27, 200–206. [Google Scholar] [CrossRef]
- Erickson, K.M.; Cole, D.J. Carotid Artery Disease: Stenting vs Endarterectomy. Br. J. Anaesth. 2010, 105 (Suppl. S1), i34–i49. [Google Scholar] [CrossRef]
- Schönenberger, S.; Uhlmann, L.; Hacke, W.; Schieber, S.; Mundiyanapurath, S.; Purrucker, J.C.; Nagel, S.; Klose, C.; Pfaff, J.; Bendszus, M.; et al. Effect of Conscious Sedation vs General Anesthesia on Early Neurological Improvement Among Patients with Ischemic Stroke Undergoing Endovascular Thrombectomy: A Randomized Clinical Trial. JAMA 2016, 316, 1986–1996. [Google Scholar] [CrossRef]
- Zanaty, M.; Daou, B.; Chalouhi, N.; Starke, R.M.; Samaniego, E.; Derdeyn, C.; Jabbour, P.; Hasan, D. Same-Day Discharge After Treatment with the Pipeline Embolization Device Using Monitored Anesthesia Care. World Neurosurg. 2016, 96, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Hendén, P.L.; Rentzos, A.; Karlsson, J.E.; Rosengren, L.; Leiram, B.; Sundeman, H.; Dunker, D.; Schnabel, K.; Wikholm, G.; Hellström, M.; et al. General Anesthesia Versus Conscious Sedation for Endovascular Treatment of Acute Ischemic Stroke: The AnStroke Trial (Anesthesia During Stroke). Stroke 2017, 48, 1601–1607. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Value |
|---|---|
| Mean age, years (SD) | 61 (11) |
| Female sex, n (%) | 139 (82) |
| Smoking history, n (%) | 64 (38) |
| Alcohol consumption, n (%) | 32 (19) |
| Preoperative mRS 0–2, n (%) | 165 (98) |
| Past medical history, n (%) | |
| Hypertension | 68 (40) |
| Dyslipidemia | 41 (24) |
| Diabetes mellitus | 10 (5.9) |
| Verify Now, median (IQR) | |
| P2Y12 reaction units | 184 (148–217) |
| Base | 248 (219–286) |
| Inhibition | 26 (8–41) |
| Aspirin reaction units | 476 (410–523) |
| Platelet aggregability, median (IQR) | |
| Adenosine diphosphate | 5 (4–5) |
| Collagen | 4 (3–5) |
| Variables | Value |
|---|---|
| Aneurysm shape, n (%) | |
| Saccular | 145 (84) |
| Blister | 3 (1.7) |
| Fusiform | 24 (14) |
| Median maximum aneurysm size, mm (Q1–Q3) | 9.5 (6.1–14) |
| Number of aneurysm measuring ≥10 mm (%) | 94 (52%) |
| Median aneurysm neck, mm (Q1–Q3) | 6.2 (4.4–8.0) |
| Growing aneurysm | 47 (27) |
| Branch from aneurysm sac | 7 (4.1) |
| Thrombosed aneurysm | 15 (8.7) |
| Previous treatment of the same aneurysm, n (%) | 26 (15%) |
| coiling | 11 (6.4) |
| Stent assisted coiling | 3 (1.7) |
| FD | 7 (4.1) |
| Direct surgery | 5 (2.9) |
| Number of FD treatment, n (%) | |
| 1 | 162 (94) |
| 2 | 8 (4.7) |
| 3 | 1 (0.58) |
| Type of FD, n (%) | n = 181 |
| FRED | 103 (57) |
| PED | 78 (43) |
| Balloon angioplasty, n (%) | 66 (38%) |
| Variables | Value |
|---|---|
| Patient outcome | n = 169 |
| mRS 0 to 2 at 90 days (n = 168) | 164 (98) |
| Mortality at discharge | 1 (0.59) |
| Major stroke | 1 (0.59) |
| Steno-occlusive events | 4 (2.4) |
| Aneurysm outcome | n = 172 |
| Satisfactory aneurysm occlusion (n = 160) | 126 (79) |
| Re-treatment | 9 (5.2) |
| Post-treatment rupture | 2 (1.2) |
| Study | Year | Number of Aneurysm (Patient) | Anesthesia | Procedure Time (min) | Hemorrhagic Events | Ischemic Events | Aneurysm Occlusion | Neurologic Morbidity and Mortality |
|---|---|---|---|---|---|---|---|---|
| Current study | 2022 | 172 (169) | LA without CS | 70 (IQR 60–84) | 0.59% | 2.4% | 79% (at median 345 days) | Mortality: 1.2% |
| PITA Nelson et al. [15] | 2011 | 31 (31) | GA | NA | 0% | 6.7% (2/30) | 93.3% (at 6 M) | Morbidity 6.7% |
| PUFS Becske et al. [13,16] | 2013, 2017 | 109 (108) | GA | 124 | 1.9% (2/107) | 6.7% (2/30) | 86.8 % (at 1Y) 95.2% (at 5 Y) | Morbidity 4.7% Mortality 2.8% |
| ASPIRe Kallmes et al. [17] | 2014 | 207 (191) | NA | 112.9 ± 54.9 | 3.7% (7/191) | 1.6% (3/191) | 74.8% (at 7.8 M) | Morbidity 7.4% Mortality 1.6% |
| IntePED Kallmes et al. [18] | 2015 | 906 (793) | NA | 101 ± 50 | 2.4% (19/793) | 4.7% (37/793) | NA | Morbidity 7.4% Mortality 3.8% |
| Australian Registry Chiu et al. [19] | 2015 | 119 (98) | NA | NA | 2.4% (19/793) | 4.7% (37/793) | 93.2% (at 2 Y) | Mortality 0.8% |
| PREMIER Hanel et al. [20] | 2019 | 141 (141) | GA or CS | 78.4 ± 40.3 | 1.4% (2/141) | 0.7% (1/141) | 81.9% (at 1Y) | 2.1% |
| Wakhloo et al. [21] | 2015 | 190 (165) | GA (except in 4: CS) | 79.8 (Average) | 2.5% | 3.7% | 75% (at median, 6 M; range, 1–38) | Morbidity 6% Mortality 2.7% |
| Berge et al. [22] | 2012 | 77 (65) | GA | NA | 6.2% | 4.7% | 84.5% (at 12 M) | Morbidity 7.7% Mortality 3% |
| SAFE Pierot et al. [14] | 2019 | 103 (103) | NA | NA | 1% | 6.8% (4/103) | 73.3% (at 1 Y) | Morbidity 2.9% Mortality 1.9% |
| SCENT Myers et al. [23] | 2019 | 180 (180) | NA | NA | 2.8% | 6.1% (11/180) | 66.1% (at 1 Y) | Total 8.3% Mortality 2.8% |
| Griessenauer et al. [24] | 2017 | CS (199) GA (149) | CS (70 patients); GA (70 patients) | CS (64) GA (83) | 5.7% (CS); 1.4% (GA) | 5.7% (CS); 2.9% (GA) | 75% (CS at 14 M); 82.4% (GA at 7 M) | Morbidity: 1.4% (CS); 3.2% (GA) Mortality: 1.4% (CS); 0% (GA) |
| Rangel-Castilla et al. [25]. | 2015 | 139 (130) | CS | 85 | NA | 3% | NA | Morbidity 3% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rajbhandari, S.; Matsukawa, H.; Uchida, K.; Shirakawa, M.; Yoshimura, S. Clinical Results of Flow Diverter Treatments for Cerebral Aneurysms under Local Anesthesia. Brain Sci. 2022, 12, 1076. https://doi.org/10.3390/brainsci12081076
Rajbhandari S, Matsukawa H, Uchida K, Shirakawa M, Yoshimura S. Clinical Results of Flow Diverter Treatments for Cerebral Aneurysms under Local Anesthesia. Brain Sciences. 2022; 12(8):1076. https://doi.org/10.3390/brainsci12081076
Chicago/Turabian StyleRajbhandari, Saujanya, Hidetoshi Matsukawa, Kazutaka Uchida, Manabu Shirakawa, and Shinichi Yoshimura. 2022. "Clinical Results of Flow Diverter Treatments for Cerebral Aneurysms under Local Anesthesia" Brain Sciences 12, no. 8: 1076. https://doi.org/10.3390/brainsci12081076