
Neurocognitive Artificial Neural Network Models Are Superior to Linear Models at Accounting for Dimensional Psychopathology


Abstract
:1. Introduction
2. Aims and Hypotheses
3. Materials and Methods
3.1. Participants
3.2. Procedure
3.3. Measures
3.4. Analysis
3.4.1. Linear Models
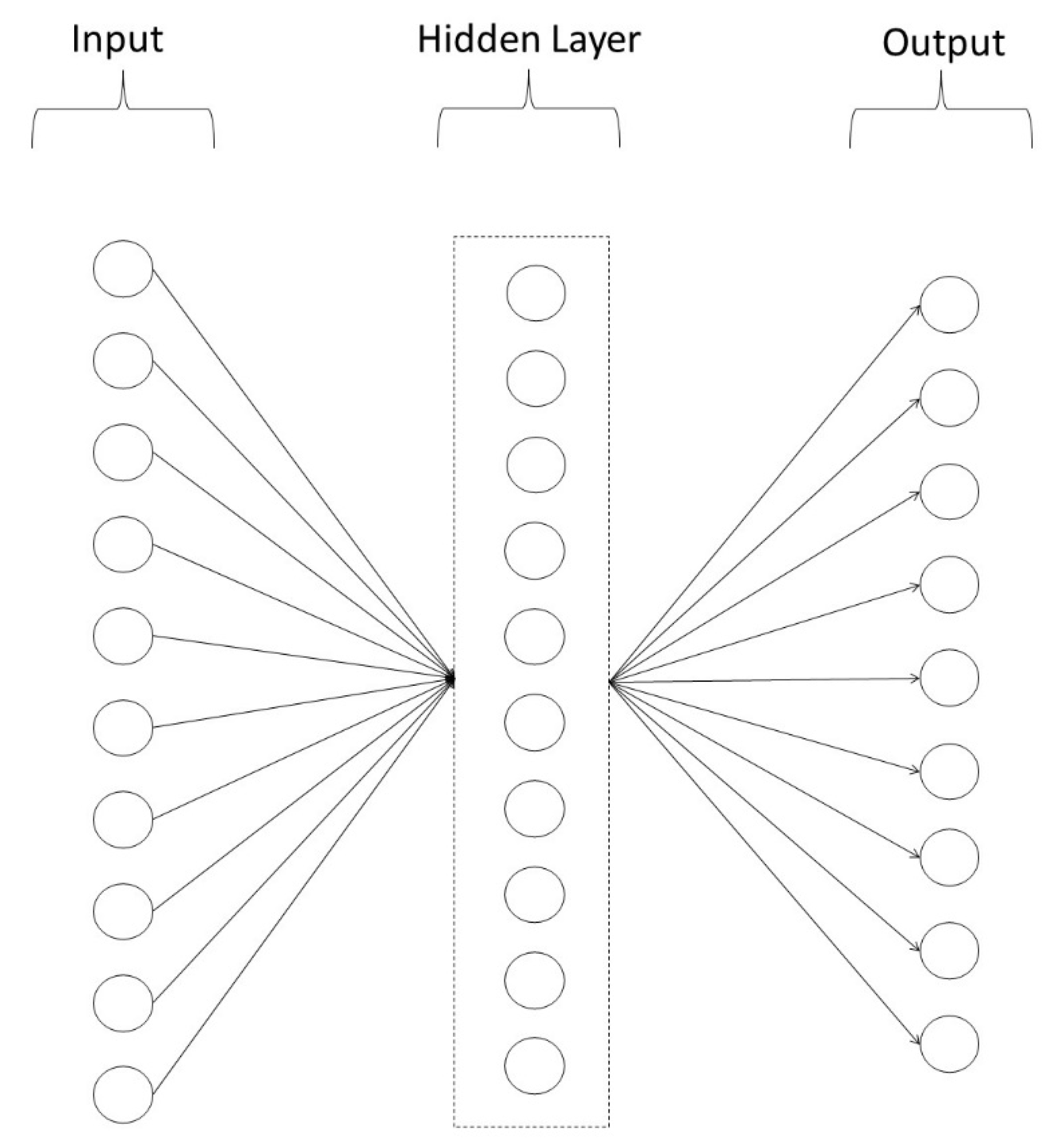
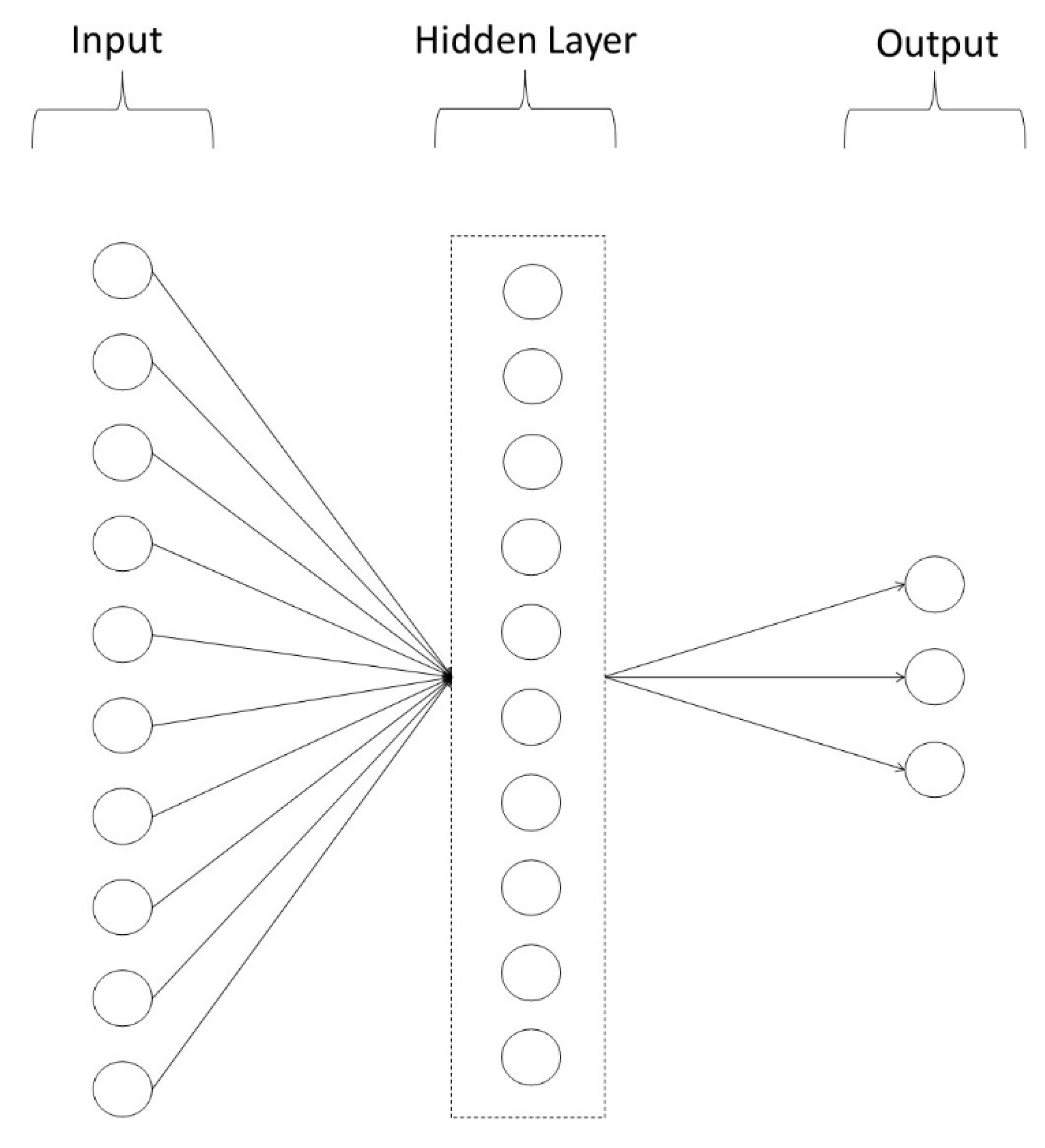
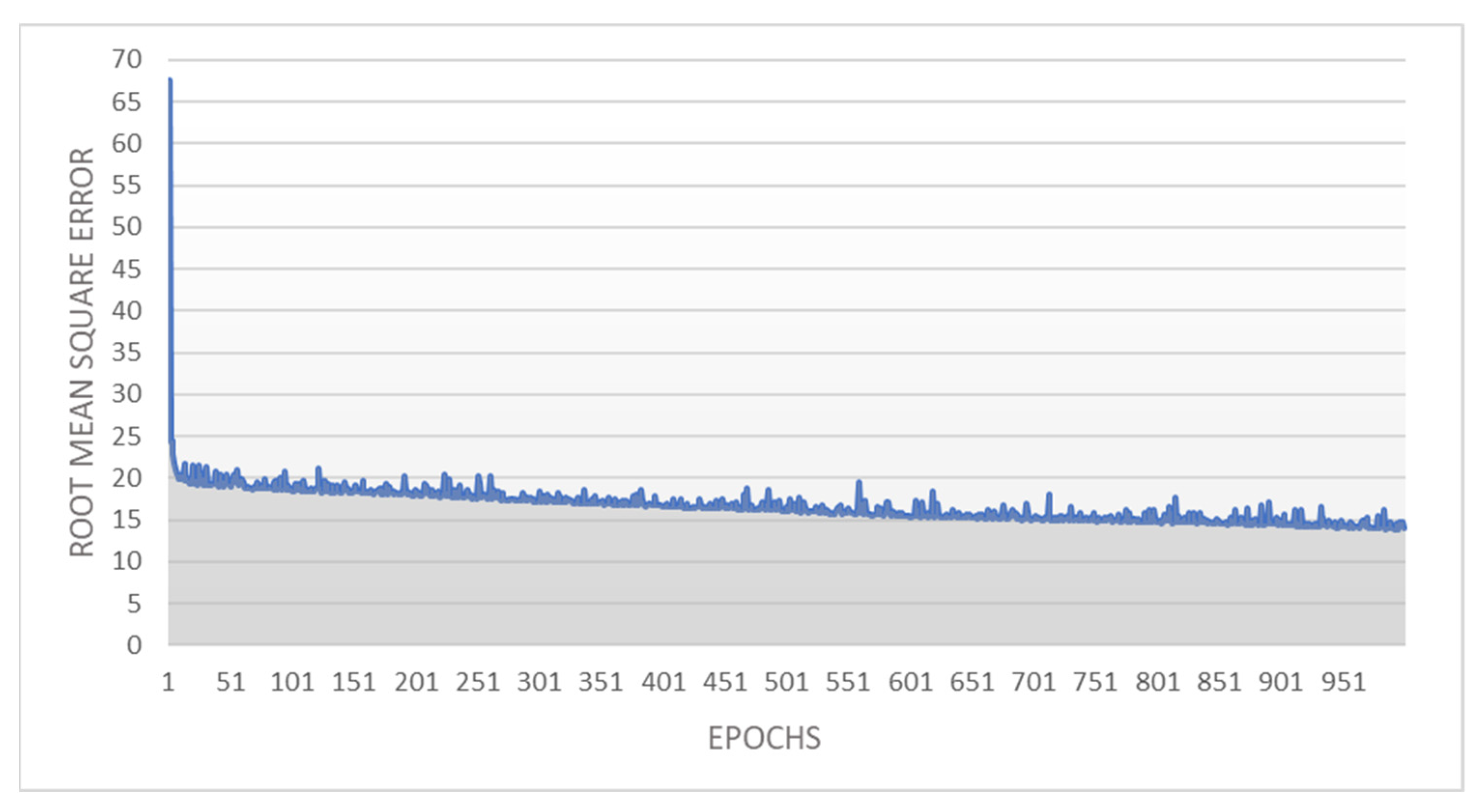
3.4.2. Artificial Neural Network Models
3.4.3. Model Comparison
4. Results
4.1. Linear Models
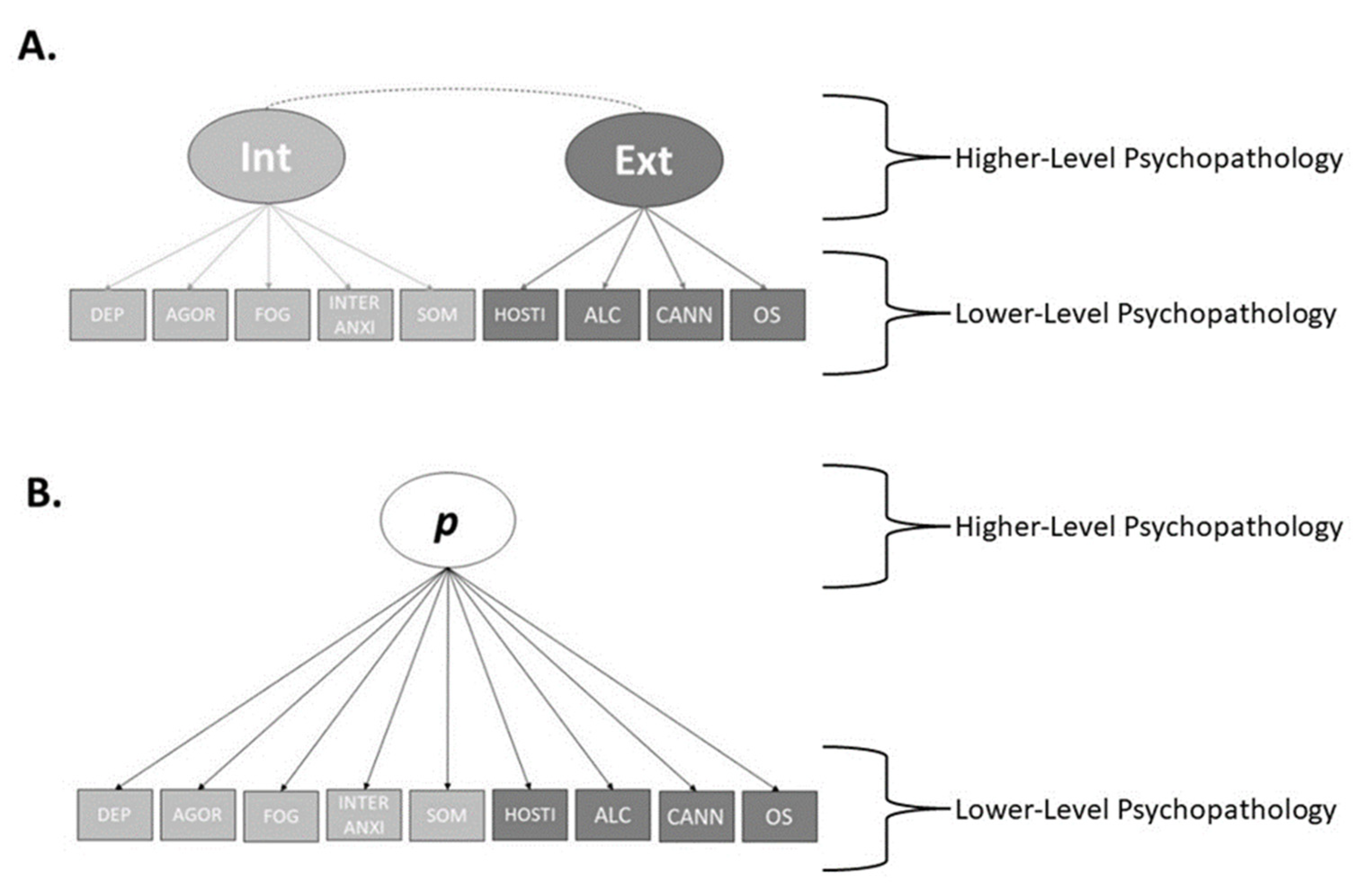
4.1.1. Lower-Level Psychopathology
4.1.2. Higher-Level Psychopathology
4.2. Artificial Neural Network Models
Lower-Level Psychopathology
4.3. Model Comparison
4.3.1. Lower-Level Psychopathology
4.3.2. Higher-Level Psychopathology
5. Discussion
Limitations and Directions for Future Research
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Beck, A.T.; Rector, N.A. Cognitive approaches to schizophrenia: Theory and therapy. Annu. Rev. Clin. Psychol. 2005, 1, 577–606. [Google Scholar] [CrossRef] [PubMed]
- Romer, A.L.; Pizzagalli, D.A. Is executive dysfunction a risk marker or consequence of psychopathology? A test of executive function as a prospective predictor and outcome of general psychopathology in the adolescent brain cognitive development study®. Dev. Cogn. Neurosci. 2021, 51, 100994. [Google Scholar] [CrossRef] [PubMed]
- Tan, E.J.; Rossell, S.L.; Subotnik, K.L.; Ventura, J.; Nuechterlein, K.H. Cognitive heterogeneity in first-episode psychosis and its relationship with premorbid developmental adjustment. Psychol. Med. 2021, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Moritz, S.; Birkner, C.; Kloss, M.; Jahn, H.; Hand, I.; Haasen, C.; Krausz, M. Executive functioning in obsessive–compulsive disorder, unipolar depression, and schizophrenia. Arch. Clin. Neuropsychol. 2002, 17, 477–483. [Google Scholar]
- Carruthers, S.P.; Van Rheenen, T.E.; Gurvich, C.; Sumner, P.J.; Rossell, S.L. Characterising the structure of cognitive heterogeneity in schizophrenia spectrum disorders. A systematic review and narrative synthesis. Neurosci. Biobehav. Rev. 2019, 107, 252–278. [Google Scholar] [CrossRef]
- Carruthers, S.P.; Gurvich, C.T.; Meyer, D.; Bousman, C.; Everall, I.P.; Neill, E.; Pantelis, C.; Sumner, P.J.; Tan, E.J.; Thomas, E.H.X. Exploring heterogeneity on the Wisconsin card sorting test in schizophrenia spectrum disorders: A cluster analytical investigation. J. Int. Neuropsychol. Soc. 2019, 25, 750–760. [Google Scholar] [CrossRef]
- Malcolm, A.; Pikoos, T.; Castle, D.J.; Rossell, S.L. Cross-diagnostic cognitive heterogeneity in body dysmorphic disorder and obsessive-compulsive disorder. J. Behav. Ther. Exp. Psychiatry 2021, 73, 101674. [Google Scholar] [CrossRef]
- Haywood, D.; Baughman, F.D. Multidimensionality in Executive Function Profiles in Schizophrenia: A Computational Approach Using the Wisconsin Card Sorting Task. Comput. Brain Behav. 2021, 4, 381–394. [Google Scholar] [CrossRef]
- Martino, D.J.; Strejilevich, S.A.; Scápola, M.; Igoa, A.; Marengo, E.; Ais, E.D.; Perinot, L. Heterogeneity in cognitive functioning among patients with bipolar disorder. J. Affect. Disord. 2008, 109, 149–156. [Google Scholar] [CrossRef]
- Newman, D.L.; Moffitt, T.E.; Caspi, A.; Silva, P.A. Comorbid mental disorders: Implications for treatment and sample selection. J. Abnorm. Psychol. 1998, 107, 305. [Google Scholar] [CrossRef]
- Hovenkamp-Hermelink, J.H.M.; Riese, H.; Batelaan, N.M.; Penninx, B.W.J.H.; Schoevers, R.A. Low stability of diagnostic classifications of anxiety disorders over time: A six-year follow-up of the NESDA study. J. Affect. Disord. 2016, 190, 310–315. [Google Scholar] [CrossRef] [PubMed]
- Burdick, K.E.; Goldberg, J.F.; Harrow, M.; Faull, R.N.; Malhotra, A.K. Neurocognition as a stable endophenotype in bipolar disorder and schizophrenia. J. Nerv. Ment. Dis. 2006, 194, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Craddock, N.; Owen, M.J.; O’Donovan, M.C. The catechol-O-methyl transferase (COMT) gene as a candidate for psychiatric phenotypes: Evidence and lessons. Mol. Psychiatry 2006, 11, 446–458. [Google Scholar] [CrossRef]
- Lichtenstein, P.; Yip, B.H.; Björk, C.; Pawitan, Y.; Cannon, T.D.; Sullivan, P.F.; Hultman, C.M. Common genetic determinants of schizophrenia and bipolar disorder in Swedish families: A population-based study. Lancet 2009, 373, 234–239. [Google Scholar] [CrossRef]
- Smucny, J.; Lesh, T.A.; Newton, K.; Niendam, T.A.; Ragland, J.D.; Carter, C.S. Levels of cognitive control: A functional magnetic resonance imaging-based test of an RDoC domain across bipolar disorder and schizophrenia. Neuropsychopharmacology 2018, 43, 598–606. [Google Scholar] [CrossRef]
- Cuthbert, B.N. The role of RDoC in future classification of mental disorders. Dialogues Clin. Neurosci. 2020, 22, 81. [Google Scholar] [CrossRef]
- Kotov, R.; Krueger, R.F.; Watson, D.; Cicero, D.C.; Conway, C.C.; DeYoung, C.G.; Eaton, N.R.; Forbes, M.K.; Hallquist, M.N.; Latzman, R.D. The Hierarchical Taxonomy of Psychopathology (HiTOP): A Quantitative Nosology Based on Consensus of Evidence. Annu. Rev. Clin. Psychol. 2021, 17, 83–108. [Google Scholar] [CrossRef]
- Caspi, A.; Houts, R.M.; Belsky, D.W.; Goldman-Mellor, S.J.; Harrington, H.; Israel, S.; Meier, M.H.; Ramrakha, S.; Shalev, I.; Poulton, R. The p factor: One general psychopathology factor in the structure of psychiatric disorders? Clin. Psychol. Sci. 2014, 2, 119–137. [Google Scholar] [CrossRef]
- Lahey, B.B.; Moore, T.M.; Kaczkurkin, A.N.; Zald, D.H. Hierarchical models of psychopathology: Empirical support, implications, and remaining issues. World Psychiatry 2021, 20, 57–63. [Google Scholar] [CrossRef]
- Lahey, B.B.; Applegate, B.; Hakes, J.K.; Zald, D.H.; Hariri, A.R.; Rathouz, P.J. Is there a general factor of prevalent psychopathology during adulthood? J. Abnorm. Psychol. 2012, 121, 971. [Google Scholar] [CrossRef]
- Caspi, A.; Moffitt, T.E. All for one and one for all: Mental disorders in one dimension. Am. J. Psychiatry 2018, 175, 831–844. [Google Scholar] [CrossRef] [PubMed]
- Haywood, D.; Baughman, F.D.; Mullan, B.A.; Heslop, K.R. One p-Factor for All? Exploring the Applicability of Structural Models of Psychopathology within Subgroups of a Population. Int. J. Environ. Res. Public Health 2021, 18, 7108. [Google Scholar] [CrossRef]
- Haywood, D.; Baughman, F.D.; Mullan, B.A.; Heslop, K.R. What Accounts for the Factors of Psychopathology? an Investigation of the Neurocognitive Correlates of Internalising, Externalising, and the P-factor. Brain Sci. 2022, 12, 421. [Google Scholar] [CrossRef] [PubMed]
- Haywood, D.; Baughman, F.D.; Mullan, B.A.; Heslop, K.R. Psychopathology and Neurocognition in the Era of the p-Factor: The Current Landscape and the Road Forward. Psychiatry Int. 2021, 2, 233–249. [Google Scholar] [CrossRef]
- Putnam, H. Representation and Reality; MIT Press: Cambridge, MA, USA, 1988. [Google Scholar]
- Bosia, M.; Bechi, M.; Bosinelli, F.; Politi, E.; Buonocore, M.; Spangaro, M.; Bianchi, L.; Cocchi, F.; Guglielmino, C.; Cavallaro, R. From cognitive and clinical substrates to functional profiles: Disentangling heterogeneity in schizophrenia. Psychiatry Res. 2019, 271, 446–453. [Google Scholar] [CrossRef]
- Tryon, W.W.; Hoffman, J.; McKay, D. Neural networks as explanatory frameworks of psychopathology and its treatment. In Mechanisms of Syndromes and Treatment for Psychological Problems; McKay, D., Abramowitz, J.S., Storch, E., Eds.; Wiley: Chichester, UK, 2017. [Google Scholar]
- Wei, Y.; Womer, F.Y.; Sun, K.; Zhu, Y.; Sun, D.; Duan, J.; Zhang, R.; Wei, S.; Jiang, X.; Zhang, Y. Applying dimensional psychopathology: Transdiagnostic prediction of executive cognition using brain connectivity and inflammatory biomarkers. Psychol. Med. 2022, 1–11. [Google Scholar] [CrossRef]
- Haywood, D.; Lawrence, B.J.; Baughman, F.D.; Mullan, B.A. A Conceptual Model of Long-Term Weight Loss Maintenance: The Importance of Cognitive, Empirical and Computational Approaches. Int. J. Environ. Res. Public Health 2021, 18, 635. [Google Scholar] [CrossRef]
- Simeoli, R.; Milano, N.; Rega, A.; Marocco, D. Using Technology to Identify Children With Autism Through Motor Abnormalities. Front. Psychol. 2021, 1710. [Google Scholar] [CrossRef]
- Dolce, P.; Marocco, D.; Maldonato, M.N.; Sperandeo, R. Toward a machine learning predictive-oriented approach to complement explanatory modeling. an application for evaluating psychopathological traits based on affective neurosciences and phenomenology. Front. Psychol. 2020, 11, 446. [Google Scholar] [CrossRef]
- Baughman, F.D.; Thomas, M.S.C. Specific Impairments in Cognitive Development: A Dynamical Systems Approach. In Proceedings of the 30th Annual Conference of the Cognitive Science Society; Love, B.C., McRae, K., Sloutsky, V.M., Eds.; Cognitive Science Society: Austin, TX, USA, 2008. [Google Scholar]
- Thomas, M.S.C.; McClelland, J.L.; Richardson, F.M.; Schapiro, A.C.; Baughman, F. Dynamical and connectionist approaches to development: Toward a future of mutually beneficial co-evolution. In Toward a Unified Theory of Development; Spencer, J., Ed.; Oxford University Press: New York, NY, USA, 2009; pp. 337–353. [Google Scholar]
- Vetter, T.R.; Schober, P. Regression: The apple does not fall far from the tree. Anesth. Analg. 2018, 127, 277–283. [Google Scholar] [CrossRef]
- Palan, S.; Schitter, C. Prolific. ac—A subject pool for online experiments. J. Behav. Exp. Financ. 2018, 17, 22–27. [Google Scholar] [CrossRef]
- Derogatis, L.R.; Melisaratos, N. The brief symptom inventory: An introductory report. Psychol. Med. 1983, 13, 595–605. [Google Scholar] [CrossRef] [PubMed]
- WHO. The alcohol, smoking and substance involvement screening test (ASSIST): Development, reliability and feasibility. Addiction 2002, 97, 1183–1194. [Google Scholar] [CrossRef]
- Cowen, P.J. Neuroendocrine and neurochemical processes in depression. Psychopathol. Rev. 2016, 3, 3–15. [Google Scholar] [CrossRef]
- Kimberg, D.Y.; Aguirre, G.K.; D’Esposito, M. Modulation of task-related neural activity in task-switching: An fMRI study. Cogn. Brain Res. 2000, 10, 189–196. [Google Scholar] [CrossRef]
- Wilson, R.C.; Niv, Y. Inferring relevance in a changing world. Front. Hum. Neurosci. 2012, 5, 189. [Google Scholar] [CrossRef]
- MacLeod, C.M. The Stroop task: The” gold standard” of attentional measures. J. Exp. Psychol. Gen. 1992, 121, 12. [Google Scholar] [CrossRef]
- Nosek, B.A.; Banaji, M.R. The go/no-go association task. Soc. Cogn. 2001, 19, 625–666. [Google Scholar] [CrossRef]
- Anderson, M.; Reid, C.; Nelson, J. Developmental changes in inspection time: What a difference a year makes. Intelligence 2001, 29, 475–486. [Google Scholar] [CrossRef]
- Schwannauer, M.; Chetwynd, P. The Brief Symptom Inventory: A validity study in two independent Scottish samples. Clin. Psychol. Psychother. Int. J. Theory Pract. 2007, 14, 221–228. [Google Scholar] [CrossRef]
- Soper, D. Significance of the Difference between Two Correlations Calculator [Software]. Available online: https://www.danielsoper.com/statcalc (accessed on 1 January 2022).
- Hauke, J.; Kossowski, T. Comparison of values of Pearson’s and Spearman’s correlation coefficients on the same sets of data. Quaest. Geogr. 2011, 30, 87. [Google Scholar] [CrossRef]
- Warner, B.; Misra, M. Understanding neural networks as statistical tools. Am. Stat. 1996, 50, 284–293. [Google Scholar]
- Danielsson, H.; Henry, L.; Messer, D.; Rönnberg, J. Strengths and weaknesses in executive functioning in children with intellectual disability. Res. Dev. Disabil. 2012, 33, 600–607. [Google Scholar] [CrossRef] [PubMed]
- Kleinhans, N.; Akshoomoff, N.; Delis, D.C. Executive functions in autism and Asperger’s disorder: Flexibility, fluency, and inhibition. Dev. Neuropsychol. 2005, 27, 379–401. [Google Scholar] [CrossRef] [PubMed]
- Egger, J.I.M.; De Mey, H.R.A.; Janssen, G.T.L. Assessment of Executive Functioning in Psychiatric Disorders: Functional Diagnosis as the Ouverture of Treatment. Clin. Neuropsychiatr. 2007, 4, 111–116. [Google Scholar]
- Johnson, B.P.; Dayan, E.; Censor, N.; Cohen, L.G. Crowdsourcing in cognitive and systems neuroscience. Neuroscientist 2021. [Google Scholar] [CrossRef]
- Crump, M.J.C.; McDonnell, J.V.; Gureckis, T.M. Evaluating Amazon’s Mechanical Turk as a tool for experimental behavioral research. PLoS ONE 2013, 8, e57410. [Google Scholar] [CrossRef]
- Merz, Z.C.; Lace, J.W.; Eisenstein, A.M. Examining broad intellectual abilities obtained within an mTurk internet sample. Curr. Psychol. 2020, 1–9. [Google Scholar] [CrossRef]
- Uittenhove, K.; Jeanneret, S.; Vergauwe, E. From Lab-Based to Web-Based Behavioural Research: Who You Test is more Important than How You Test. Psyarxiv 2022. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dependent Variable | Parameter | B | Β | Sig. |
|---|---|---|---|---|
| Depression | Age | −0.024 | −0.396 | <0.001 ** |
| Gender | 0.275 | 0.137 | 0.007 ** | |
| Digit Span | −0.051 | −0.091 | 0.067 | |
| Visual WM | 0.002 | 0.014 | 0.790 | |
| Inferring Relevance | 117.25 | 0.030 | 0.598 | |
| Shape-Number | 155.76 | 0.046 | 0.410 | |
| Stroop | −337.60 | −0.049 | 0.334 | |
| Go/NoGo | −512.58 | −0.030 | 0.550 | |
| Simple RT | −2866.43 | −0.059 | 0.250 | |
| IT | 0.003 | 0.068 | 0.177 | |
| Agoraphobia | Age | −0.015 | −0.241 | <0.001 ** |
| Gender | 0.221 | 0.111 | 0.007 ** | |
| Digit Span | −0.002 | −0.004 | 0.913 | |
| Visual WM | −0.002 | −0.018 | 0.673 | |
| Inferring Relevance | −65.82 | −0.017 | 0.714 | |
| Shape-Number | −84.80 | −0.025 | 0.578 | |
| Stroop | 100.15 | 0.014 | 0.722 | |
| Go/NoGo | −709.85 | −0.042 | 0.305 | |
| Simple RT | −3372.44 | −0.070 | 0.094 | |
| IT | 0.002 | 0.038 | 0.342 | |
| Hostility | Age | −0.015 | −0.238 | <0.001 ** |
| Gender | 0.036 | 0.018 | 0.566 | |
| Digit Span | 0.018 | 0.032 | 0.306 | |
| Visual WM | 0.000 | −0.004 | 0.905 | |
| Inferring Relevance | 61.31 | 0.016 | 0.659 | |
| Shape-Number | −39.83 | −0.012 | 0.736 | |
| Stroop | 96.77 | 0.014 | 0.657 | |
| Go/NoGo | −293.64 | −0.017 | 0.584 | |
| Simple RT | −5504.99 | −0.114 | <0.001 ** | |
| IT | 0.002 | 0.050 | 0.112 | |
| Mental Fog | Age | −0.025 | −0.410 | <0.001 ** |
| Gender | 0.348 | 0.174 | <0.001 ** | |
| Digit Span | −0.029 | −0.051 | 0.245 | |
| Visual WM | −0.002 | −0.017 | 0.718 | |
| Inferring Relevance | 35.30 | 0.009 | 0.859 | |
| Shape-Number | −37.12 | −0.011 | 0.825 | |
| Stroop | 22.51 | 0.003 | 0.942 | |
| Go/NoGo | −1498.37 | −0.089 | 0.050 | |
| Simple RT | −1794.27 | −0.037 | 0.419 | |
| IT | 0.004 | 0.081 | 0.071 | |
| Interpersonal Anxiety | Age | −0.022 | −0.358 | <0.001 ** |
| Gender | 0.214 | 0.107 | 0.007 ** | |
| Digit Span | −0.007 | −0.012 | 0.747 | |
| Visual WM | −0.003 | −0.027 | 0.522 | |
| Inferring Relevance | 40.08 | 0.010 | 0.817 | |
| Shape-Number | −143.92 | −0.043 | 0.329 | |
| Stroop | −271.37 | −0.039 | 0.319 | |
| Go/NoGo | 53.71 | 0.003 | 0.936 | |
| Simple RT | −4043.57 | −0.083 | 0.038 * | |
| IT | 0.004 | 0.081 | 0.038 * | |
| Somatisation | Age | −0.014 | −0.228 | <0.001 ** |
| Gender | 0.272 | 0.136 | <0.001 ** | |
| Digit Span | −0.005 | −0.008 | 0.776 | |
| Visual WM | 0.000 | 0.002 | 0.941 | |
| Inferring Relevance | −89.74 | −0.023 | 0.501 | |
| Shape-Number | 107.08 | 0.032 | 0.345 | |
| Stroop | −57.52 | −0.008 | 0.783 | |
| Go/NoGo | −766.38 | −0.045 | 0.136 | |
| Simple RT | −5405.81 | −0.112 | <0.001 ** | |
| IT | 0.003 | 0.070 | 0.020 * | |
| Alcohol | Age | −0.029 | −0.468 | 0.223 |
| Gender | −1.62 | −0.811 | 0.022 ** | |
| Digit Span | 0.240 | 0.430 | 0.214 | |
| Visual WM | −0.041 | −0.356 | 0.343 | |
| Inferring Relevance | −297.26 | −0.076 | 0.848 | |
| Shape-Number | −393.96 | −0.117 | 0.765 | |
| Stroop | −682.54 | −0.099 | 0.779 | |
| Go/NoGo | 8663.47 | 0.513 | 0.149 | |
| Simple RT | −69,091.17 | −10.426 | <0.001 ** | |
| IT | 0.021 | 0.461 | 0.188 | |
| Cannabis | Age | −0.052 | −0.857 | 0.005 ** |
| Gender | −0.646 | −0.323 | 0.252 | |
| Digit Span | −0.183 | −0.328 | 0.234 | |
| Visual WM | 0.012 | 0.106 | 0.722 | |
| Inferring Relevance | 1064.69 | 0.273 | 0.389 | |
| Shape-Number | −295.90 | −0.088 | 0.778 | |
| Stroop | 861.75 | 0.124 | 0.657 | |
| Go/NoGo | 4069.70 | 0.241 | 0.394 | |
| Simple RT | −34,946.23 | −0.721 | 0.012 * | |
| IT | 0.002 | 0.046 | 0.868 | |
| Other Substances | Age | 0.014 | 0.223 | 0.648 |
| Gender | −0.332 | −0.166 | 0.712 | |
| Digit Span | 0.533 | 0.954 | 0.031 * | |
| Visual WM | −0.112 | −0.980 | 0.040 * | |
| Inferring Relevance | 1196.78 | 0.307 | 0.545 | |
| Shape-Number | 1123.99 | 0.335 | 0.503 | |
| Stroop | 5111.74 | 0.738 | 0.100 | |
| Go/NoGo | 475.96 | 0.028 | 0.950 | |
| Simple RT | −61,098.64 | −1.261 | 0.006 ** | |
| IT | 0.024 | 0.525 | 0.238 |
| Predictors | Internalising | Externalising | p-Factor | ||||||
|---|---|---|---|---|---|---|---|---|---|
| B | β | p | B | β | p | B | β | p | |
| Age | −0.027 | −0.433 | <0.001 ** | −0.026 | −0.346 | <0.001 ** | −0.398 | −0.434 | <0.001 ** |
| Gender | 0.360 | 0.174 | <0.001 ** | 0.007 | 0.003 | 0.951 | 4.68 | 0.156 | 0.001 ** |
| Digit Span | −0.024 | −0.041 | 0.360 | 0.036 | 0.054 | 0.249 | −0.251 | −0.030 | 0.505 |
| Vis WM | −0.002 | −0.013 | 0.783 | −0.003 | −0.022 | 0.669 | −0.026 | −0.015 | 0.758 |
| Infer. Rel. | 13.03 | 0.003 | 0.950 | 149.99 | 0.032 | 0.555 | 415.57 | 0.007 | 0.891 |
| Shape-Num | −9.37 | −0.003 | 0.958 | −61.02 | −0.015 | 0.778 | −214.33 | −0.004 | 0.934 |
| Stroop | −182.03 | −0.025 | 0.578 | 264.25 | 0.031 | 0.664 | −1916.14 | −0.018 | 0.686 |
| Go/NoGo | −840.70 | −0.048 | 0.297 | −203.95 | −0.010 | 0.835 | −11,229.5 | −0.044 | 0.336 |
| Simple RT | −4973.28 | −0.099 | 0.034 * | −12,291.5 | −0.209 | <0.001 ** | −84,882.8 | −0.117 | 0.012 * |
| IT | 0.004 | 0.094 | 0.040 * | 0.005 | 0.082 | 0.083 | 0.064 | 0.095 | 0.037 * |
| LM-Dep | ANN-Dep | LM-Agor | ANN-Agor | LM-Host | ANN-Host | LM-Fog | ANN-Fog | LM-Int. Anx | ANN-Int. Anx | LM-Soma | ANN-Soma | LM-Alc | ANN-Alc | LM-Cann | ANN-Cann | LM-Other | ANN-Other | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Dep | 0.435 | 0.648 | ||||||||||||||||
| Agor | 0.331 | 0.577 | ||||||||||||||||
| Host | 0.414 | 0.655 | ||||||||||||||||
| Fog | 0.476 | 0.711 | ||||||||||||||||
| Int. Anx | 0.449 | 0.675 | ||||||||||||||||
| Soma | 0.469 | 0.710 | ||||||||||||||||
| Alc | 0.268 | 0.338 | ||||||||||||||||
| Cann | 0.235 | 0.413 | ||||||||||||||||
| Other | 0.243 | 0.552 |
| LM-Int | ANN-Int | LM-Ext | ANN-Ext | LM-p | ANN-p | |
|---|---|---|---|---|---|---|
| Internalising | 0.488 | 0.661 | ||||
| Externalising | 0.421 | 0.619 | ||||
| p-factor | 0.486 | 0.666 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haywood, D.; Baughman, F.D.; Mullan, B.A.; Heslop, K.R. Neurocognitive Artificial Neural Network Models Are Superior to Linear Models at Accounting for Dimensional Psychopathology. Brain Sci. 2022, 12, 1060. https://doi.org/10.3390/brainsci12081060
Haywood D, Baughman FD, Mullan BA, Heslop KR. Neurocognitive Artificial Neural Network Models Are Superior to Linear Models at Accounting for Dimensional Psychopathology. Brain Sciences. 2022; 12(8):1060. https://doi.org/10.3390/brainsci12081060
Chicago/Turabian StyleHaywood, Darren, Frank D. Baughman, Barbara A. Mullan, and Karen R. Heslop. 2022. "Neurocognitive Artificial Neural Network Models Are Superior to Linear Models at Accounting for Dimensional Psychopathology" Brain Sciences 12, no. 8: 1060. https://doi.org/10.3390/brainsci12081060