
Biomarkers of Relapse in Cocaine Use Disorder: A Narrative Review

 , , , , and
, , , , and
Abstract
:1. Introduction
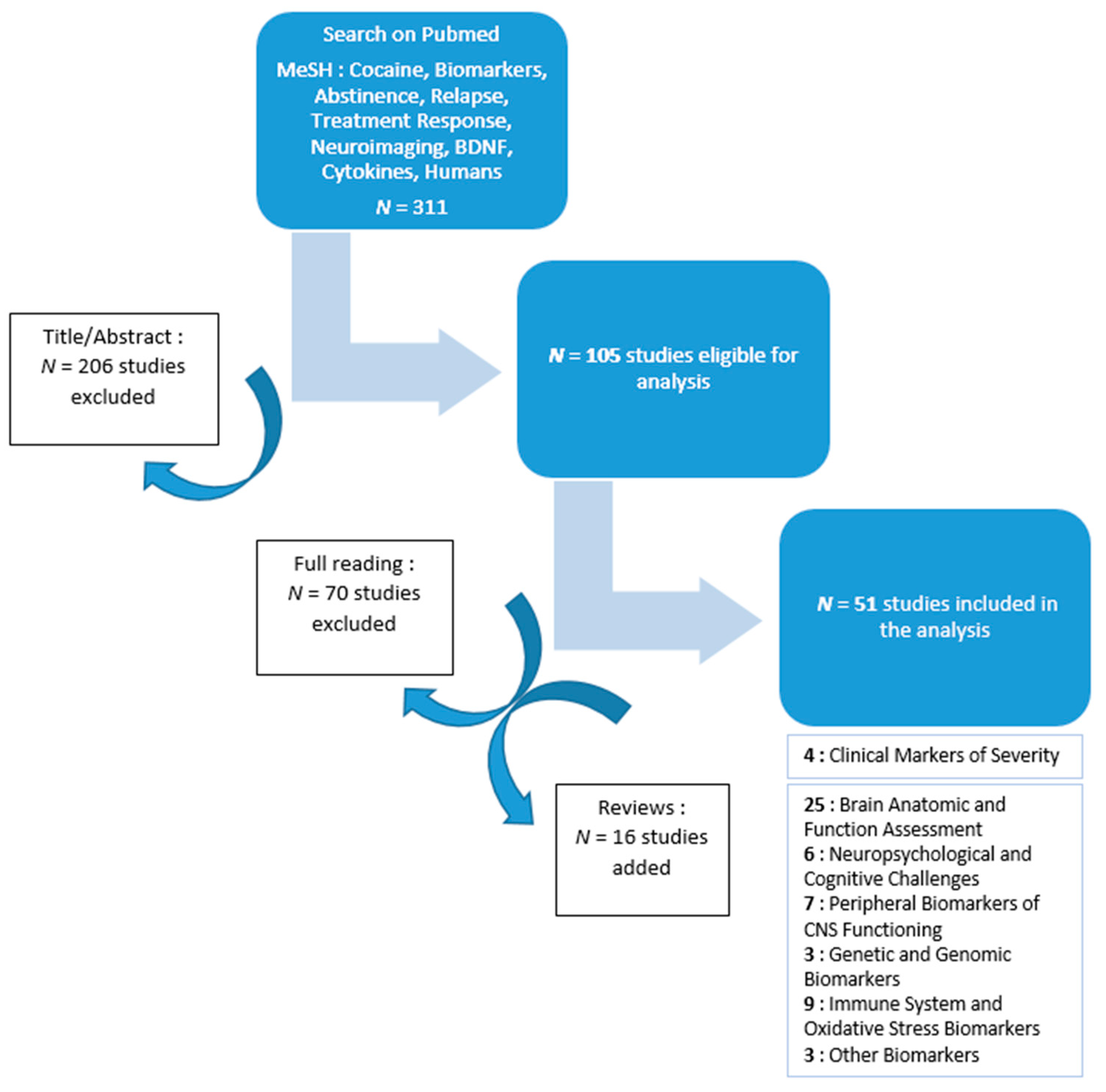
2. Methods
3. Results
3.1. Central Nervous System
3.1.1. Brain Anatomic and Function Assessment
3.1.2. Neuropsychological and Cognitive Challenges
3.1.3. Peripheral Biomarkers of CNS Functioning
3.2. Genetic and Genomic Biomarkers
3.3. Immune System and Oxidative Stress Biomarkers
3.4. “Other” Biomarkers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pitchot, W.; Scantamburlo, G.; Pinto, E.; Karila, L. Cocaine Addiction. Rev. Med. Liege 2013, 68, 294–297. [Google Scholar]
- Wouldes, T.A.; Lester, B.M. Stimulants: How big is the problem and what are the effects of prenatal exposure? Semin. Fetal Neonatal Med. 2019, 24, 155–160. [Google Scholar] [CrossRef]
- Clergue-Duval, V.; Nicolas-Sacy, L.; Karsinti, E.; Zerdazi, E.-H.; Laplanche, J.-L.; Brousse, G.; Marees, A.T.; Derks, E.M.; Henry, P.; Bellivier, F.; et al. Risk and Protective Factors of Lifetime Cocaine-Associated Chest Pain. Front. Psychiatry 2021, 12, 704276. [Google Scholar] [CrossRef] [PubMed]
- Chychula, N.M.; Okore, C. The cocaine epidemic: A comprehensive review of use, abuse and dependence. Nurse Pract. 1990, 15, 31–39. [Google Scholar] [CrossRef]
- Vorspan, F.; Brousse, G.; Bloch, V.; Bellais, L.; Romo, L.; Guillem, E.; Coeuru, P.; Lépine, J.-P. Cocaine-induced psychotic symptoms in French cocaine addicts. Psychiatry Res. 2012, 200, 1074–1076. [Google Scholar] [CrossRef] [PubMed]
- Vorspan, F.; de Witt, P.; Zerdazi, E.-H.; Karsinti, E.; Ksouda, K.; Icick, R.; Bellivier, F.; Marie, N.; Brousse, G.; Bloch, V. Chronic exposure to cocaine is associated with persistent behavioral disturbances. A cross-sectional dimensional study in outpatients with multiple substance use disorders. Psychopharmacology 2020, 237, 3399–3407. [Google Scholar] [CrossRef]
- Goldstein, R.Z.; Tomasi, D.; Alia-Klein, N.; Zhang, L.; Telang, F.; Volkow, N.D. The effect of practice on a sustained attention task in cocaine abusers. NeuroImage 2007, 35, 194–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Block, R.I.; Erwin, W.J.; Ghoneim, M. Chronic drug use and cognitive impairments. Pharmacol. Biochem. Behav. 2002, 73, 491–504. [Google Scholar] [CrossRef]
- Wagner, F.A.; Anthony, J.C. From First Drug Use to Drug Dependence Developmental Periods of Risk for Dependence upon Marijuana, Cocaine, and Alcohol. Neuropsychopharmacology 2002, 26, 479–488. [Google Scholar] [CrossRef]
- Vorspan, F.; Fortias, M.; Zerdazi, E.-H.; Karsinti, E.; Bloch, V.; Lépine, J.-P.; Bellivier, F.; Brousse, G.; van den Brink, W.; Derks, E. Self-reported cue-induced physical symptoms of craving as an indicator of cocaine dependence. Am. J. Addict. 2015, 24, 740–743. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, H. Clinical and laboratory assessment of the subjective experience of drug craving. Clin. Psychol. Rev. 2009, 29, 519–534. [Google Scholar] [CrossRef] [PubMed]
- Paliwal, P.; Hyman, S.M.; Sinha, R. Craving predicts time to cocaine relapse: Further validation of the now and brief versions of the cocaine craving questionnaire. Drug Alcohol Depend. 2008, 93, 252–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kampman, K.M. The treatment of cocaine use disorder. Sci. Adv. 2019, 5, eaax1532. [Google Scholar] [CrossRef] [Green Version]
- Bough, K.J.; Amur, S.; Lao, G.; Hemby, S.E.; Tannu, N.S.; Kampman, K.M.; Schmitz, J.M.; Martinez, D.; Merchant, K.M.; Green, C.E.; et al. Biomarkers for the Development of New Medications for Cocaine Dependence. Neuropsychopharmacology 2014, 39, 202–219. [Google Scholar] [CrossRef] [Green Version]
- Corominas-Roso, M.; Roncero, C.; Daigre, C.; Grau-López, L.; Ros-Cucurull, E.; Rodríguez-Cintas, L.; Sànchez-Mora, C.; Lopez, M.V.; Ribases, M.; Casas, M. Changes in brain-derived neurotrophic factor (BDNF) during abstinence could be associated with relapse in cocaine-dependent patients. Psychiatry Res. 2015, 225, 309–314. [Google Scholar] [CrossRef]
- von Diemen, L.; Kapczinski, F.; Sordi, A.O.; de Magalhães Narvaez, J.C.; Guimarães, L.S.P.; Kessler, F.H.P.; Pfaffenseller, B.; de Aguiar, B.W.; de Moura Gubert, C.; Pechansky, F. Increase in brain-derived neurotrophic factor expression in early crack cocaine withdrawal. Int. J. Neuropsychopharmacol. 2013, 17, 33–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lima, D.R.; Gonçalves, P.D.; Ometto, M.; Malbergier, A.; Amaral, R.A.; dos Santos, B.; Cavallet, M.; Chaim-Avancini, T.; Serpa, M.H.; Ferreira, L.R.K.; et al. The role of neurocognitive functioning, substance use variables and the DSM-5 severity scale in cocaine relapse: A prospective study. Drug Alcohol Depend. 2019, 197, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Bell, R.P.; Garavan, H.; Foxe, J.J. Neural correlates of craving and impulsivity in abstinent former cocaine users: Towards biomarkers of relapse risk. Neuropharmacology 2014, 85, 461–470. [Google Scholar] [CrossRef]
- McHugh, M.J.; Demers, C.H.; Esalmeron, B.J.; Devous, M.D.S.; Stein, E.A.; Eadinoff, B. Cortico-Amygdala Coupling as a Marker of Early Relapse Risk in Cocaine-Addicted Individuals. Front. Psychiatry 2014, 5, 16. [Google Scholar] [CrossRef] [Green Version]
- Clark, V.P.; Beatty, G.K.; Anderson, R.E.; Kodituwakku, P.; Phillips, J.P.; Lane, T.D.; Kiehl, K.A.; Calhoun, V.D. Reduced fMRI activity predicts relapse in patients recovering from stimulant dependence. Hum. Brain Mapp. 2012, 35, 414–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moeller, F.G.; Dougherty, D.M.; Barratt, E.S.; Schmitz, J.M.; Swann, A.C.; Grabowski, J. The impact of impulsivity on cocaine use and retention in treatment. J. Subst. Abus. Treat. 2001, 21, 193–198. [Google Scholar] [CrossRef]
- Hser, Y.-I.; Shen, H.; Grella, C.; Anglin, M.D. Lifetime Severity Index for Cocaine Use Disorder (LSI-Cocaine): A Predictor of Treatment Outcomes. J. Nerv. Ment. Dis. 1999, 187, 742–750. [Google Scholar] [CrossRef]
- Volkow, N.D.; Koob, G. Brain disease model of addiction: Why is it so controversial? Lancet Psychiatry 2015, 2, 677–679. [Google Scholar] [CrossRef] [Green Version]
- Vorspan, F.; Marie-Claire, C.; Bellivier, F.; Bloch, V. Biomarkers to predict staging and treatment response in opioid dependence: A narrative review. Drug Dev. Res. 2021, 82, 668–677. [Google Scholar] [CrossRef] [PubMed]
- McGorry, P.; Keshavan, M.; Goldstone, S.; Amminger, P.; Allott, K.; Berk, M.; Lavoie, S.; Pantelis, C.; Yung, A.; Wood, S.; et al. Biomarkers and clinical staging in psychiatry. World Psychiatry 2014, 13, 211–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balodis, I.M.; Kober, H.; Worhunsky, P.D.; Stevens, M.C.; Pearlson, G.D.; Carroll, K.M.; Potenza, M.N. Neurofunctional Reward Processing Changes in Cocaine Dependence During Recovery. Neuropsychopharmacology 2016, 41, 2112–2121. [Google Scholar] [CrossRef] [PubMed]
- Brewer, J.A.; Worhunsky, P.D.; Carroll, K.M.; Rounsaville, B.J.; Potenza, M.N. Pretreatment Brain Activation During Stroop Task Is Associated with Outcomes in Cocaine-Dependent Patients. Biol. Psychiatry 2008, 64, 998–1004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Claus, E.D.; Shane, M.S. dACC response to presentation of negative feedback predicts stimulant dependence diagnosis and stimulant use severity. NeuroImage Clin. 2018, 20, 16–23. [Google Scholar] [CrossRef]
- Connolly, C.G.; Foxe, J.J.; Nierenberg, J.; Shpaner, M.; Garavan, H. The neurobiology of cognitive control in successful cocaine abstinence. Drug Alcohol Depend. 2012, 121, 45–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia, Z.; Worhunsky, P.D.; Carroll, K.M.; Rounsaville, B.J.; Stevens, M.; Pearlson, G.D.; Potenza, M.N. An Initial Study of Neural Responses to Monetary Incentives as Related to Treatment Outcome in Cocaine Dependence. Biol. Psychiatry 2011, 70, 553–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosten, T.R.; Scanley, B.E.; Tucker, K.A.; Oliveto, A.; Prince, C.; Sinha, R.; Potenza, M.N.; Skudlarski, P.; Wexler, B.E. Cue-Induced Brain Activity Changes and Relapse in Cocaine-Dependent Patients. Neuropsychopharmacology 2006, 31, 644–650. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, M.R.; Balodis, I.M.; Devito, E.E.; Lacadie, C.M.; Yeston, J.; Scheinost, D.; Constable, R.T.; Carroll, K.M.; Potenza, M.N. A preliminary investigation of Stroop-related intrinsic connectivity in cocaine dependence: Associations with treatment outcomes. Am. J. Drug Alcohol Abus. 2013, 39, 392–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moeller, F.G.; Steinberg, J.L.; Schmitz, J.M.; Ma, L.; Liu, S.; Kjome, K.L.; Rathnayaka, N.; Kramer, L.A.; Narayana, P.A. Working memory fMRI activation in cocaine-dependent subjects: Association with treatment response. Psychiatry Res. 2010, 181, 174–182. [Google Scholar] [CrossRef] [Green Version]
- Prisciandaro, J.J.; Myrick, H.; Henderson, S.; McRae-Clark, A.L.; Brady, K.T. Prospective associations between brain activation to cocaine and no-go cues and cocaine relapse. Drug Alcohol Depend. 2013, 131, 44–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Regier, P.S.; Jagannathan, K.; Franklin, T.R.; Wetherill, R.R.; Langleben, D.D.; Gawyrsiak, M.; Kampman, K.M.; Childress, A.R. Sustained brain response to repeated drug cues is associated with poor drug-use outcomes. Addict. Biol. 2021, 26, e13028. [Google Scholar] [CrossRef]
- Zhang, S.; Hu, S.; Bednarski, S.R.; Erdman, E.; Li, C.-S.R. Error-related functional connectivity of the thalamus in cocaine dependence. NeuroImage Clin. 2014, 4, 585–592. [Google Scholar] [CrossRef] [Green Version]
- Adinoff, B.; Gu, H.; Merrick, C.; McHugh, M.; Jeon-Slaughter, H.; Lu, H.; Yang, Y.; Stein, E.A. Basal Hippocampal Activity and Its Functional Connectivity Predicts Cocaine Relapse. Biol. Psychiatry 2015, 78, 496–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camchong, J.; MacDonald, A.W.; Mueller, B.A.; Nelson, B.; Specker, S.; Slaymaker, V.; Lim, K.O. Changes in resting functional connectivity during abstinence in stimulant use disorder: A preliminary comparison of relapsers and abstainers. Drug Alcohol Depend. 2014, 139, 145–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, H.; Salmeron, B.J.; Ross, T.J.; Geng, X.; Zhan, W.; Stein, E.A.; Yang, Y. Mesocorticolimbic circuits are impaired in chronic cocaine users as demonstrated by resting-state functional connectivity. NeuroImage 2010, 53, 593–601. [Google Scholar] [CrossRef] [Green Version]
- Zhai, T.; Salmeron, B.J.; Gu, H.; Adinoff, B.; Stein, E.A.; Yang, Y. Functional connectivity of dorsolateral prefrontal cortex predicts cocaine relapse: Implications for neuromodulation treatment. Brain Commun. 2021, 3, fcab120. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; DeVito, E.E.; Worhunsky, P.D.; Carroll, K.M.; Rounsaville, B.J.; Potenza, M.N. White Matter Integrity is Associated with Treatment Outcome Measures in Cocaine Dependence. Neuropsychopharmacology 2010, 35, 1541–1549. [Google Scholar] [CrossRef] [PubMed]
- Abé, C.; Mon, A.; Durazzo, T.C.; Pennington, D.L.; Schmidt, T.P.; Meyerhoff, D.J. Polysubstance and alcohol dependence: Unique abnormalities of magnetic resonance-derived brain metabolite levels. Drug Alcohol Depend. 2012, 130, 30–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abé, C.; Mon, A.; Hoefer, M.E.; Durazzo, T.C.; Pennington, D.L.; Schmidt, T.P.; Meyerhoff, D.J. Metabolic abnormalities in lobar and subcortical brain regions of abstinent polysubstance users: Magnetic resonance spectroscopic imaging. Alcohol Alcohol. 2013, 48, 543–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez, D.; Carpenter, K.M.; Liu, F.; Slifstein, M.; Broft, A.; Friedman, A.C.; Kumar, D.; Van Heertum, R.; Kleber, H.D.; Nunes, E. Imaging Dopamine Transmission in Cocaine Dependence: Link Between Neurochemistry and Response to Treatment. Am. J. Psychiatry 2011, 168, 634–641. [Google Scholar] [CrossRef] [PubMed]
- Ide, J.S.; Zhang, S.; Hu, S.; Sinha, R.; Mazure, C.M.; Li, C.-S.R. Cerebral gray matter volumes and low-frequency fluctuation of BOLD signals in cocaine dependence: Duration of use and gender difference. Drug Alcohol Depend. 2013, 134, 51–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, J.; Kober, H.; Wang, X.; DeVito, E.E.; Carroll, K.M.; Potenza, M.N. Hippocampal volume mediates the relationship between measures of pre-treatment cocaine use and within-treatment cocaine abstinence. Drug Alcohol Depend. 2014, 143, 74–80. [Google Scholar] [CrossRef] [Green Version]
- Parvaz, M.A.; Moeller, S.J.; Goldstein, R.Z. Incubation of Cue-Induced Craving in Adults Addicted to Cocaine Measured by Electroencephalography. JAMA Psychiatry 2016, 73, 1127–1134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Floresco, S.B. The Nucleus Accumbens: An Interface between Cognition, Emotion, and Action. Annu. Rev. Psychol. 2015, 66, 25–52. [Google Scholar] [CrossRef]
- Anastasio, N.C.; Liu, S.; Maili, L.; Swinford, S.E.; Lane, S.D.; Fox, R.G.; Hamon, S.C.; Nielsen, D.A.; Cunningham, K.A.; Moeller, F.G. Variation within the serotonin (5-HT) 5-HT2C receptor system aligns with vulnerability to cocaine cue reactivity. Transl. Psychiatry 2014, 4, e369. [Google Scholar] [CrossRef] [Green Version]
- Fox, H.C.; Jackson, E.D.; Sinha, R. Elevated cortisol and learning and memory deficits in cocaine dependent individuals: Relationship to relapse outcomes. Psychoneuroendocrinology 2009, 34, 1198–1207. [Google Scholar] [CrossRef] [Green Version]
- Streeter, C.C.; Terhune, D.B.; Whitfield, T.H.; Gruber, S.; Sarid-Segal, O.; Silveri, M.M.; Tzilos, G.; Afshar, M.; Rouse, E.D.; Tian, H.; et al. Performance on the Stroop Predicts Treatment Compliance in Cocaine-Dependent Individuals. Neuropsychopharmacology 2007, 33, 827–836. [Google Scholar] [CrossRef] [PubMed]
- Peng, S.; Li, W.; Lv, L.; Zhang, Z.; Zhan, X. BDNF as a biomarker in diagnosis and evaluation of treatment for schizophrenia and depression. Discov. Med. 2018, 26, 127–136. [Google Scholar] [PubMed]
- D’Sa, C.; Fox, H.C.; Hong, A.K.; Dileone, R.J.; Sinha, R. Increased Serum Brain-Derived Neurotrophic Factor Is Predictive of Cocaine Relapse Outcomes: A Prospective Study. Biol. Psychiatry 2011, 70, 706–711. [Google Scholar] [CrossRef] [Green Version]
- Hilburn, C.; Nejtek, V.A.; Underwood, W.A.; Singh, M.; Patel, G.; Gangwani, P.; Forster, M.J. Is serum brain-derived neurotrophic factor related to craving for or use of alcohol, cocaine, or methamphetamine? Neuropsychiatr. Dis. Treat. 2011, 7, 357–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirsch, G.E.; Jaskulski, M.; Hamerski, H.M.; Porto, F.G.; da Silva, B.; Aita, C.A.M.; Kroker, K.; de Bem Silveira, G.; Silveira, P.C.L.; Santos, G.T.; et al. Evaluation of oxidative stress and brain-derived neurotrophic factor levels related to crack-use detoxification. Neurosci. Lett. 2018, 670, 62–68. [Google Scholar] [CrossRef]
- Patkar, A.A.; Rozen, S.; Mannelli, P.; Matson, W.; Pae, C.-U.; Krishnan, K.R.; Kaddurah-Daouk, R. Alterations in tryptophan and purine metabolism in cocaine addiction: A metabolomic study. Psychopharmacology 2009, 206, 479–489. [Google Scholar] [CrossRef]
- Scherer, J.N.; Schuch, S.; Ornell, F.; Sordi, A.O.; Bristot, G.; Pfaffenseller, B.; Kapczinski, F.; Kessler, F.H.; Fumagalli, F.; Pechansky, F.; et al. High levels of brain-derived neurotrophic factor are associated with treatment adherence among crack-cocaine users. Neurosci. Lett. 2016, 630, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Sordi, A.O.; Pechansky, F.; Kessler, F.H.P.; Kapczinski, F.; Pfaffenseller, B.; Gubert, C.; de Aguiar, B.W.; de Magalhães Narvaez, J.C.; Ornell, F.; von Diemen, L. Oxidative stress and BDNF as possible markers for the severity of crack cocaine use in early withdrawal. Psychopharmacology 2014, 231, 4031–4039. [Google Scholar] [CrossRef] [PubMed]
- Gelernter, J.; Sherva, R.; Koesterer, R.; Almasy, L.; Zhao, H.; Kranzler, H.R.; Farrer, L. Genome-wide association study of cocaine dependence and related traits: FAM53B identified as a risk gene. Mol. Psychiatry 2013, 19, 717–723. [Google Scholar] [CrossRef] [Green Version]
- Forget, B.; Icick, R.; Robert, J.; Correia, C.; Prevost, M.S.; Gielen, M.; Corringer, P.-J.; Bellivier, F.; Vorspan, F.; Besson, M.; et al. Alterations in nicotinic receptor alpha5 subunit gene differentially impact early and later stages of cocaine addiction: A translational study in transgenic rats and patients. Prog. Neurobiol. 2020, 197, 101898. [Google Scholar] [CrossRef]
- Viola, T.W.; Heberle, B.A.; Zaparte, A.; Sanvicente-Vieira, B.; Wainer, L.M.; Fries, G.R.; Walss-Bass, C.; Grassi-Oliveira, R. Peripheral blood microRNA levels in females with cocaine use disorder. J. Psychiatr. Res. 2019, 114, 48–54. [Google Scholar] [CrossRef]
- Prinz, M.; Priller, J. The role of peripheral immune cells in the CNS in steady state and disease. Nat. Neurosci. 2017, 20, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.H.; Chen, P.S. Inflammatory Biomarkers for Mood Disorders—A Brief Narrative Review. Curr. Pharm. Des. 2020, 26, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Araos, P.; Pedraz, M.; Serrano, A.; Lucena, M.; Barrios, V.; García-Marchena, N.; Campos-Cloute, R.; Ruiz, J.J.; Romero, P.; Suárez, J.; et al. Plasma profile of pro-inflammatory cytokines and chemokines in cocaine users under outpatient treatment: Influence of cocaine symptom severity and psychiatric co-morbidity: Inflammation and Cocaine Addiction. Addict. Biol. 2014, 20, 756–772. [Google Scholar] [CrossRef]
- Araos, P.; Vidal, R.; O’Shea, E.; Pedraz, M.; García-Marchena, N.; Serrano, A.; Suárez, J.; Castilla-Ortega, E.; Ruiz, J.J.; Campos-Cloute, R.; et al. Serotonin is the main tryptophan metabolite associated with psychiatric comorbidity in abstinent cocaine-addicted patients. Sci. Rep. 2019, 9, 16842. [Google Scholar] [CrossRef]
- Levandowski, M.L.; Viola, T.W.; Wearick-Silva, L.E.; Wieck, A.; Tractenberg, S.G.; Brietzke, E.; Bauer, M.E.; Teixeira, A.L.; Grassi-Oliveira, R. Early life stress and tumor necrosis factor superfamily in crack cocaine withdrawal. J. Psychiatr. Res. 2014, 53, 180–186. [Google Scholar] [CrossRef]
- Levandowski, M.L.; Hess, A.R.B.; Grassi-Oliveira, R.; de Almeida, R.M.M. Plasma interleukin-6 and executive function in crack cocaine-dependent women. Neurosci. Lett. 2016, 628, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Ligabue, K.P.; Schuch, J.B.; Scherer, J.N.; Ornell, F.; Roglio, V.S.; Assunção, V.; Rebelatto, F.P.; Hildalgo, M.P.; Pechansky, F.; Kessler, F.; et al. Increased cortisol levels are associated with low treatment retention in crack cocaine users. Addict. Behav. 2019, 103, 106260. [Google Scholar] [CrossRef] [PubMed]
- Sampedro-Piquero, P.; Vicario, S.; Pérez-Rivas, A.; Venero, C.; Baliyan, S.; Santín, L.J. Salivary Cortisol Levels Are Associated with Craving and Cognitive Performance in Cocaine-Abstinent Subjects: A Pilot Study. Brain Sci. 2020, 10, 682. [Google Scholar] [CrossRef] [PubMed]
- Stamatovich, S.N.; Lopez-Gamundi, P.; Suchting, R.; Colpo, G.D.; Walss-Bass, C.; Lane, S.D.; Schmitz, J.M.; Wardle, M.C. Plasma pro- and anti-inflammatory cytokines may relate to cocaine use, cognitive functioning, and depressive symptoms in cocaine use disorder. Am. J. Drug Alcohol Abus. 2021, 47, 52–64. [Google Scholar] [CrossRef]
- Escobar, M.; Scherer, J.N.; Ornell, F.; Bristot, G.; Soares, C.M.; Guimarães, L.S.P.; Von Diemen, L.; Pechansky, F. Leptin levels and its correlation with crack-cocaine use severity: A preliminary study. Neurosci. Lett. 2018, 671, 56–59. [Google Scholar] [CrossRef]
- Levandowski, M.; Viola, T.; Tractenberg, S.G.; Teixeira, A.L.; Brietzke, E.; Bauer, M.E.; Grassi-Oliveira, R. Adipokines during early abstinence of crack cocaine in dependent women reporting childhood maltreatment. Psychiatry Res. 2013, 210, 536–540. [Google Scholar] [CrossRef]
- Patkar, A.A.; Hill, K.P.; Sterling, R.C.; Gottheil, E.; Berrettini, W.H.; Weinstein, S.P. Serum prolactin and response to treatment among cocaine-dependent individuals. Addict. Biol. 2002, 7, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Mavridis, I. The role of the nucleus accumbens in psychiatric disorders. Psychiatriki 2015, 25, 282–294. [Google Scholar]
- Bracht, T.; Soravia, L.; Moggi, F.; Stein, M.; Grieder, M.; Federspiel, A.; Tschümperlin, R.; Batschelet, H.M.; Wiest, R.; Denier, N. The role of the orbitofrontal cortex and the nucleus accumbens for craving in alcohol use disorder. Transl. Psychiatry 2021, 11, 267. [Google Scholar] [CrossRef]
- Lee, J.H.; Ribeiro, E.A.; Kim, J.; Ko, B.; Kronman, H.; Jeong, Y.H.; Kim, J.K.; Janak, P.H.; Nestler, E.J.; Koo, J.W.; et al. Dopaminergic Regulation of Nucleus Accumbens Cholinergic Interneurons Demarcates Susceptibility to Cocaine Addiction. Biol. Psychiatry 2020, 88, 746–757. [Google Scholar] [CrossRef] [PubMed]
- Huang, A.S.; Mitchell, J.A.; Haber, S.N.; Alia-Klein, N.; Goldstein, R.Z. The thalamus in drug addiction: From rodents to humans. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2018, 373, 20170028. [Google Scholar] [CrossRef] [PubMed]
- Hampton, W.H.; Hanik, I.M.; Olson, I.R. Substance abuse and white matter: Findings, limitations, and future of diffusion tensor imaging research. Drug Alcohol Depend. 2019, 197, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, C.E.; Clifford, J.; Ling, J.; Mayer, A.R.; Bigelow, R.; Bogenschutz, M.P.; Tonigan, J.S. Stroop-related cerebellar and temporal activation is correlated with negative affect and alcohol use disorder severity. Brain Imaging Behav. 2019, 14, 586–598. [Google Scholar] [CrossRef]
- Christiansen, P.; Schoenmakers, T.M.; Field, M. Less than meets the eye: Reappraising the clinical relevance of attentional bias in addiction. Addict. Behav. 2015, 44, 43–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghitza, U.E.; Zhai, H.; Wu, P.; Airavaara, M.; Shaham, Y.; Lu, L. Role of BDNF and GDNF in drug reward and relapse: A review. Neurosci. Biobehav. Rev. 2010, 35, 157–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becker, J.B.; Chartoff, E. Sex differences in neural mechanisms mediating reward and addiction. Neuropsychopharmacology 2018, 44, 166–183. [Google Scholar] [CrossRef] [Green Version]
- Boulanger, L.M. Immune Proteins in Brain Development and Synaptic Plasticity. Neuron 2009, 64, 93–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leclercq, S.; Cani, P.D.; Neyrinck, A.M.; Stärkel, P.; Jamar, F.; Mikolajczak, M.; Delzenne, N.M.; De Timary, P. Role of intestinal permeability and inflammation in the biological and behavioral control of alcohol-dependent subjects. Brain Behav. Immun. 2012, 26, 911–918. [Google Scholar] [CrossRef] [PubMed]
- Fox, H.C.; D’Sa, C.; Kimmerling, A.; Siedlarz, K.M.; Tuit, K.L.; Stowe, R.; Sinha, R. Immune system inflammation in cocaine dependent individuals: Implications for medications development: Inflammation in cocaine dependent individuals. Hum. Psychopharmacol. Clin. Exp. 2012, 27, 156–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Participants | Study Design | Article | |
|---|---|---|---|
| Task-based fMRI: | |||
| Biomarker of: | |||
| ↗ abstinence: ↗ midbrain activity during a MIDT ↘ abstinence: ↗ ventral striatum and NAcc activity during a MIDT ↘ craving: ↗ ventral striatum activity during a MIDT | N = 57 | Prospective | Balodis et al., 2016 [26] |
| ↗ cue-induced craving: ↗ right ventral striatum activity during a CCQ-N | N = 20 | Cross-sectional | Bell et al., 2014 [18] |
| ↗ abstinence: ↘ dlPFC and left PCC activity during a Stroop Task ↘ abstinence: ↘ right striatum activity during a Stroop Task | N = 22 | Prospective | Brewer et al., 2008 [27] |
| ↗ abstinence: ↗ PCC activity during an Odball Task | N = 45 | Prospective | Clark et al., 2014 [20] |
| ↘ lifetime stimulant use: ↘ dACC activity during a reaction time task | N = 87 | Cross-sectional | Claus et al., 2018 [28] |
| ↗ abstinence: ↗ PFC activity during a response inhibition task | N = 27 | Cross-sectional | Connolly et al., 2012 [29] |
| ↘ abstinence: ↗ thalamus, right caudate and culmen activity during a MIDT ↘ treatment retention: ↗ left amygdala and left PHG activity during a MIDT | N = 20 | Prospective | Jia et al., 2011 [30] |
| ↗ relapse: ↗ PrG, PCC, STG, LiG, and IOG activity during exposure to cocaine-related cues | N = 17 | Prospective | Kosten et al., 2006 [31] |
| ↗ abstinence: ↘ intrinsic connectivity in ventral striatum, right insula, left hippocampus, substantia nigra, and thalamus during a Stroop Task | N = 16 | Prospective | Mitchell et al., 2013 [32] |
| ↘ abstinence: ↘ thalamus activity during a working memory task | N = 19 | Cross-sectional | Moeller et al., 2010 [33] |
| ↘ abstinence: ↗ right putamen, insula, and bilateral occipital regions during exposure to cocaine-related cues | N = 30 | Prospective | Prisciandaro et al., 2013 [34] |
| ↗ abstinence: ↘ amygdala, FuG and PHG activity during exposure to cocaine-related cues | N = 73 | Prospective | Regier et al., 2021 [35] |
| ↗ cocaine use in the prior month: ↘ thalamus and vmPFC during a reaction time task | N = 54 | Cross-sectional | Zhang et al., 2014 [36] |
| Resting-state: | |||
| Biomarker of: | |||
| ↗ relapse: ↗ rsFC between PCC and precuneus | N = 40 | Prospective | Adinoff et al., 2015 [37] |
| ↗ relapse: ↗ rsFC between NAcc and FPC, ↗ rsFC between NAcc and posterior cingulate gyrus, ↗ rsFC between subgenual ACC and left PFC | N = 18 | Prospective | Camchong et al., 2014 [38] |
| ↗ years of cocaine use: ↘ rsFC between VTA and thalamus, lentiform nucleus and NAcc | N = 39 | Cross-sectional | Gu et al., 2010 [39] |
| ↗ relapse: ↘ rsFC between left corticomedial amygdala and vmPFC and rACC ↗ abstinence: ↘ rsFC between bilateral amygdala and lingual gyrus and cuneus | N = 45 | Prospective | McHugh et al., 2014 [19] |
| ↘ relapse: ↗ rsFC in the executive control network, ↗ rsFC between bilateral dlPFC, IFG, right IPL, dmPFC, and left vlPFC ↗ relapse: ↗ rsFC in the default mode network, ↗ rsFC between bilateral precuneus and amygdala and hippocampus, ↗ rsFC between bilateral cuneus, visual cortex, vmOFC, thalamus, FuG, and left precuneus | N = 43 | Prospective | Zhai et al., 2021 [40] |
| Diffusion Tensor Imaging (DTI): | |||
| Biomarker of: | |||
| ↗ abstinence: ↗ WM integrity in frontal, parietal, and occipital lobes and rostral corpus callosum, cerebellum, and rostral midbrain | N = 16 | Prospective | Xu et al., 2010 [41] |
| Positron Emission Tomography (PET-SCAN): | |||
| Biomarker of: | |||
| ↗ abstinence: ↗ creatine levels in frontal and parietal GM and frontal WM, ↗ choline-containing metabolites levels in parietal GM, ↗ myo-inositol levels in thalamus | N = 18 | Cross-sectional | Abé et al., 2013 [42] |
| ↗ cocaine use: ↘ GABA levels in ACC, N-acetylaspartate levels in cortical GM | N = 28 | Cross-sectional | Abé et al., 2013 [43] |
| ↗ abstinence: ↗ dopamine signaling in the limbic striatum | N = 25 | Prospective | Martinez et al., 2011 [44] |
| Anatomical MRI: | |||
| Biomarker of: | |||
| ↗ years of cocaine use: ↘ GM volume in cingulate cortex and bilateral superior frontal gyri | N = 84 | Cross-sectional | Ide et al., 2014 [45] |
| ↘ abstinence: ↗ WM volume in hippocampus | N = 23 | Prospective | Xu et al., 2014 [46] |
| Electroencephalography: | |||
| Biomarker of: | |||
| ↗ craving: ↗ cue-induced LPP at 1 and 6 months of abstinence | N = 76 | Cross-sectional | Parvaz et al., 2016 [47] |
| Participants | Study Design | Article | |
|---|---|---|---|
| Biomarker of: | |||
| ↗ cocaine reactivity: ↗ attentional bias during a cocaine-word Stroop Task | N = 114 | Cross-sectional | Anastasio et al., 2014 [49] |
| ↗ treatment retention: ↘ Stroop interference effect | N = 22 | Prospective | Brewer et al., 2008 [32] |
| ↗ relapse: ↘ cognitive flexibility scores on the WCST | N = 45 | Prospective | Clark et al., 2014 [20] |
| ↗ relapse: ↘ memory score on the RAVLT | N = 36 | Prospective | Fox et al., 2009 [50] |
| ↗ abstinence: ↗ Stroop interference effect | N = 13 | Prospective | Mitchell et al., 2013 [32] |
| ↗ treatment dropout: ↗ attentional bias during a Stroop Task | N = 74 | Prospective | Streeter et al., 2008 [51] |
| Participants | Study design | Article | |
|---|---|---|---|
| Biomarker of: | |||
| ↗ abstinence: ↘ BDNF levels | N = 40 | Prospective | Corominas-Roso et al., 2015 [15] |
| ↘ abstinence: ↗ BDNF levels | N = 35 | Prospective | D’Sa et al., 2011 [53] |
| ↗ abstinence: ↗ BDNF levels | N = 22 | Cross-sectional | Hilburn et al., 2011 [54] |
| ↗ abstinence: ↘ BDNF levels between entry and 2 weeks of detoxification | N = 31 | Prospective | Hirsch et al., 2018 [55] |
| ↗ severity of CUD: ↗ n-methylserotonin levels, ↘ xanthine levels | N = 18 | Cross-sectional | Patkar et al., 2009 [56] |
| ↗ abstinence: ↗ BDNF levels | N = 47 | Prospective | Scherer et al., 2016 [57] |
| ↗ severity of CUD: ↘ BDNF levels | N = 49 | Prospective | Sordi et al., 2014 [58] |
| Participants | Study Design | Article | |
|---|---|---|---|
| Biomarker of: | |||
| ↗ cocaine cue reactivity: carrying the SER23 variation of the 5-HT2C receptor | N = 114 | Cross-sectional | Anastasio et al., 2014 [49] |
| ↘ time before relapse: variation in the βnAC subunit that possibly alters CHRNA5 gene expression | N = 581 | Cross-sectional | Forget et al., 2021 [60] |
| ↗ severity of CUD: upregulation of miR-181 | N = 30 | Cross-sectional | Viola et al., 2019 [61] |
| Participants | Study Design | Article | |
|---|---|---|---|
| Biomarker of: | |||
| ↗ abstinence: ↘ TNF-α, MCP-1 and SDF-1 levels ↗ severity of CUD: ↗ IL-1β, fraktaline and SDF-1 levels | N = 82 | Cross-sectional | Araos et al., 2015 [64] |
| ↗ lifetime dependence: ↘ kynurenic acid levels | N = 100 | Cross-sectional | Araos et al., 2019 [65] |
| ↗ CUD duration: ↗ glutathione levels between entry and 3 weeks of detoxification | N = 31 | Prospective | Hirsch et al., 2018 [55] |
| ↗ abstinence symptoms severity: ↗ TNF-α levels | N = 44 | Prospective | Levandowski et al., 2014 [66] |
| ↘ cognitive flexibility: ↗ IL-6 levels | N = 42 | Cross-sectional | Levandowski et al., 2016 [67] |
| ↘ treatment retention: ↗ entry cortisol levels | N = 44 | Prospective | Ligabue et al., 2020 [68] |
| ↗ craving: ↗ morning cortisol levels | N = 14 | Cross-sectional | Sampedro-Piquero et al., 2020 [69] |
| ↗ severity of CUD: ↗ TBARS levels (lipid oxidation) | N = 49 | Prospective | Sordi et al., 2014 [58] |
| ↗ years of cocaine use: ↘ IL-29 and IL-20 levels | N = 85 | Cross-sectional | Stamatovich et al., 2021 [70] |
| Participants | Study Design | Article | |
|---|---|---|---|
| Biomarker of: | |||
| ↗ severity of CUD: ↘ leptin plasmatic levels | N = 40 | Cross-sectional | Escobar et al., 2018 [71] |
| ↗ withdrawal symptoms: ↗ plasmatic adipokine levels | N = 104 | Cross-sectional | Levandowski et al., 2013 [72] |
| ↘ abstinence: ↗ prolactin plasmatic levels | N = 86 | Prospective | Patkar et al., 2002 [73] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poireau, M.; Milpied, T.; Maillard, A.; Delmaire, C.; Volle, E.; Bellivier, F.; Icick, R.; Azuar, J.; Marie-Claire, C.; Bloch, V.; et al. Biomarkers of Relapse in Cocaine Use Disorder: A Narrative Review. Brain Sci. 2022, 12, 1013. https://doi.org/10.3390/brainsci12081013
Poireau M, Milpied T, Maillard A, Delmaire C, Volle E, Bellivier F, Icick R, Azuar J, Marie-Claire C, Bloch V, et al. Biomarkers of Relapse in Cocaine Use Disorder: A Narrative Review. Brain Sciences. 2022; 12(8):1013. https://doi.org/10.3390/brainsci12081013
Chicago/Turabian StylePoireau, Margaux, Thomas Milpied, Angéline Maillard, Christine Delmaire, Emmanuelle Volle, Frank Bellivier, Romain Icick, Julien Azuar, Cynthia Marie-Claire, Vanessa Bloch, and et al. 2022. "Biomarkers of Relapse in Cocaine Use Disorder: A Narrative Review" Brain Sciences 12, no. 8: 1013. https://doi.org/10.3390/brainsci12081013