
Histiocytic Sarcoma Involving Cervical Vertebra: A Case Report and Review of the Literature

 , ,
, ,
Abstract
:1. Introduction
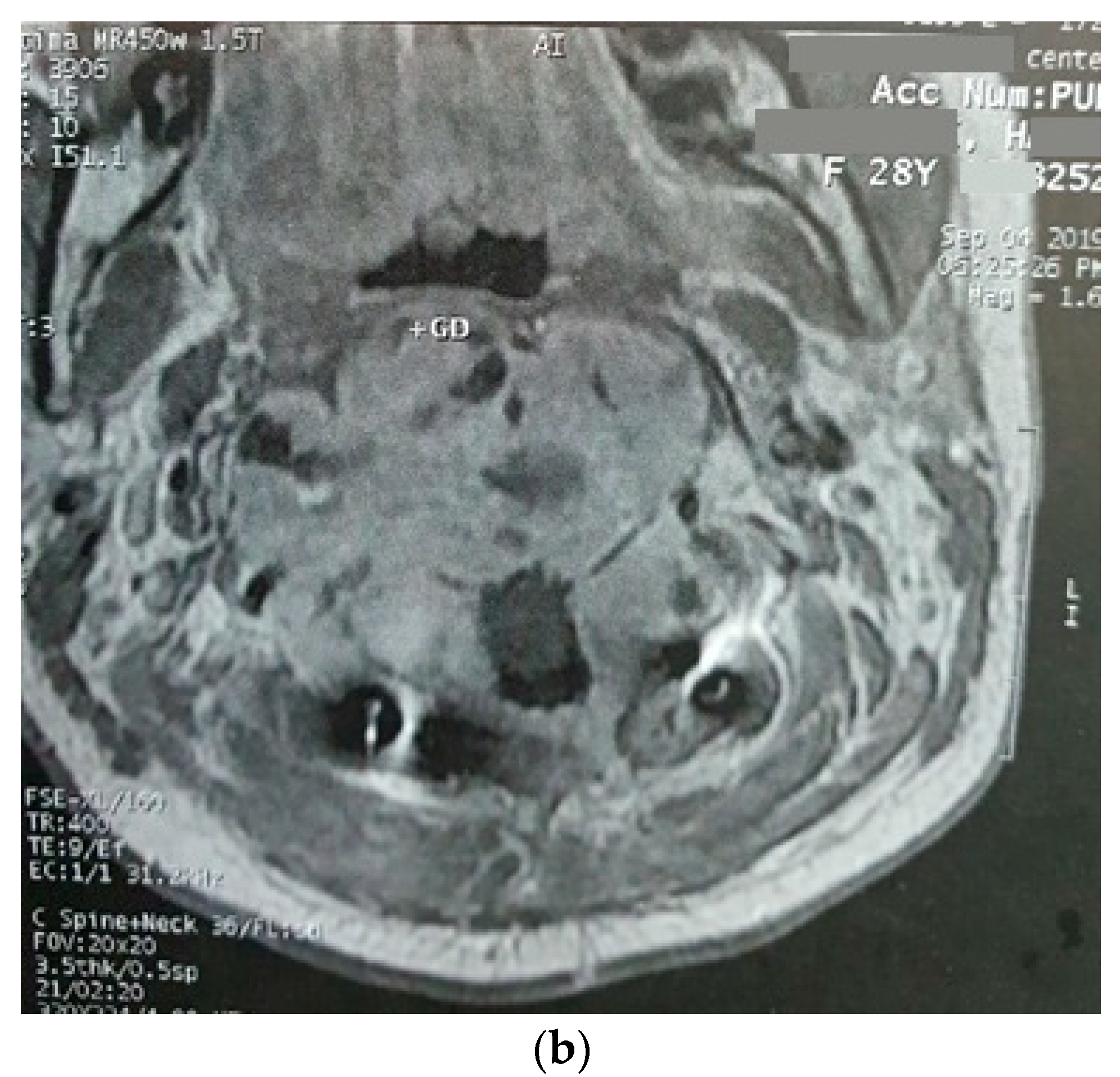
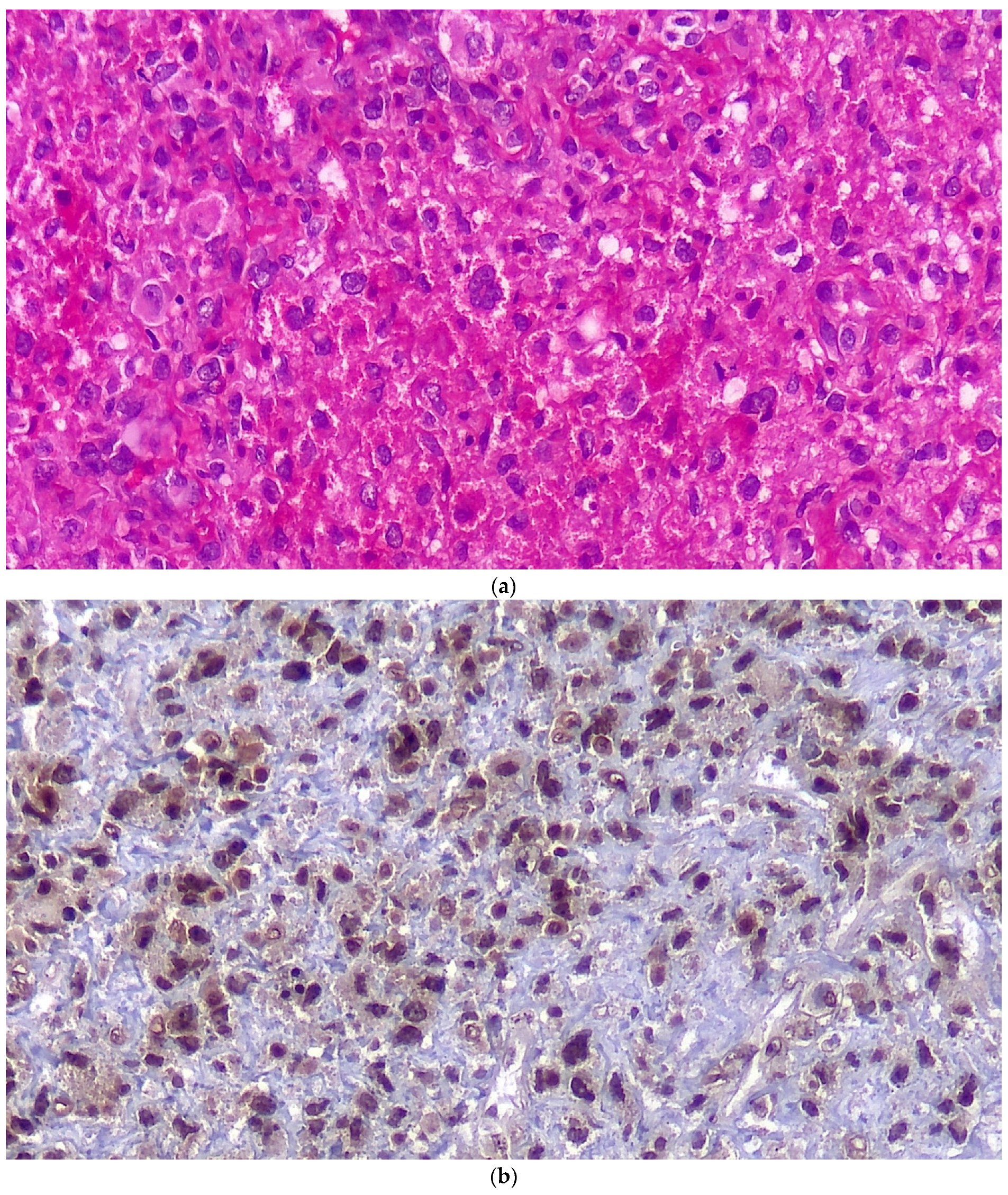
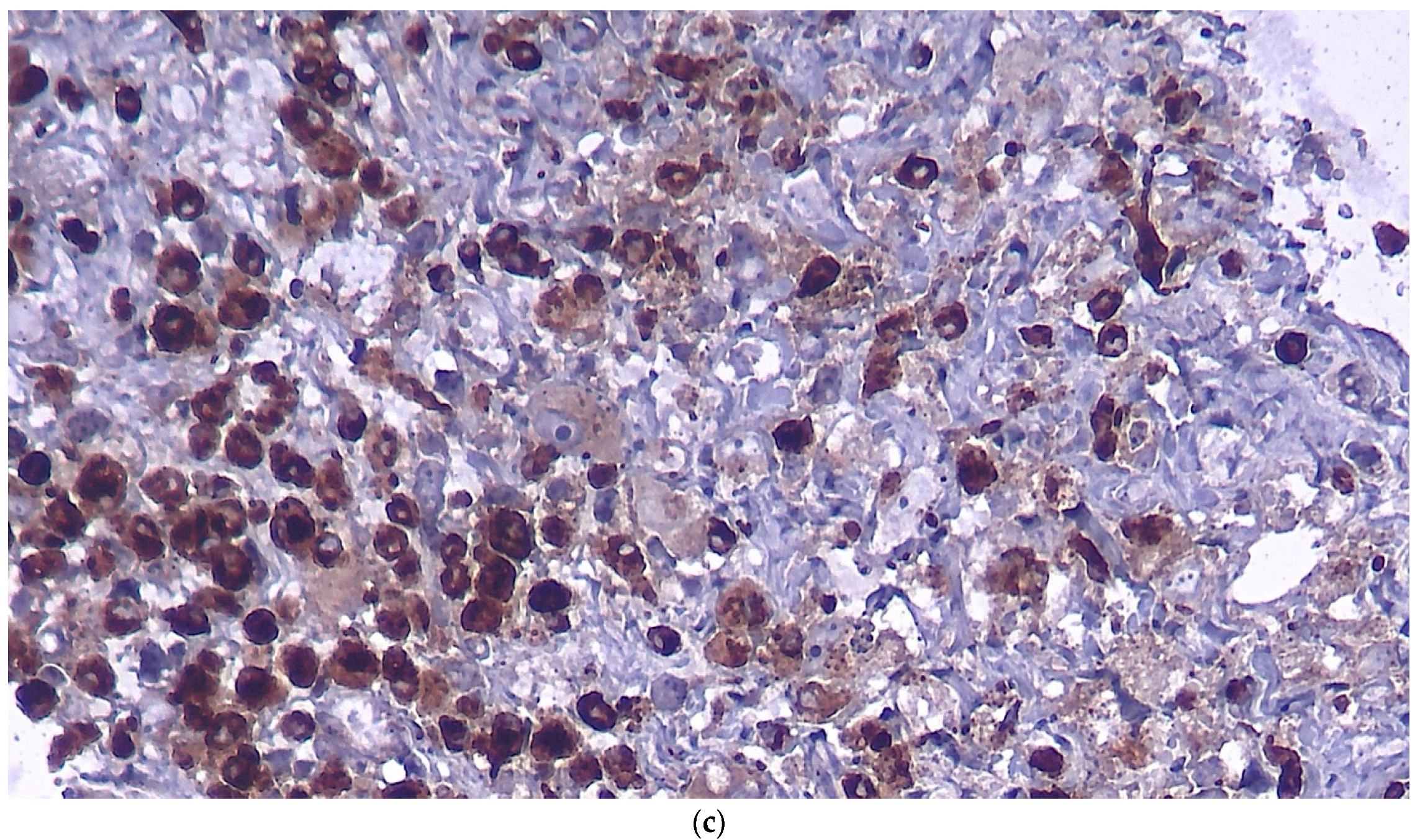
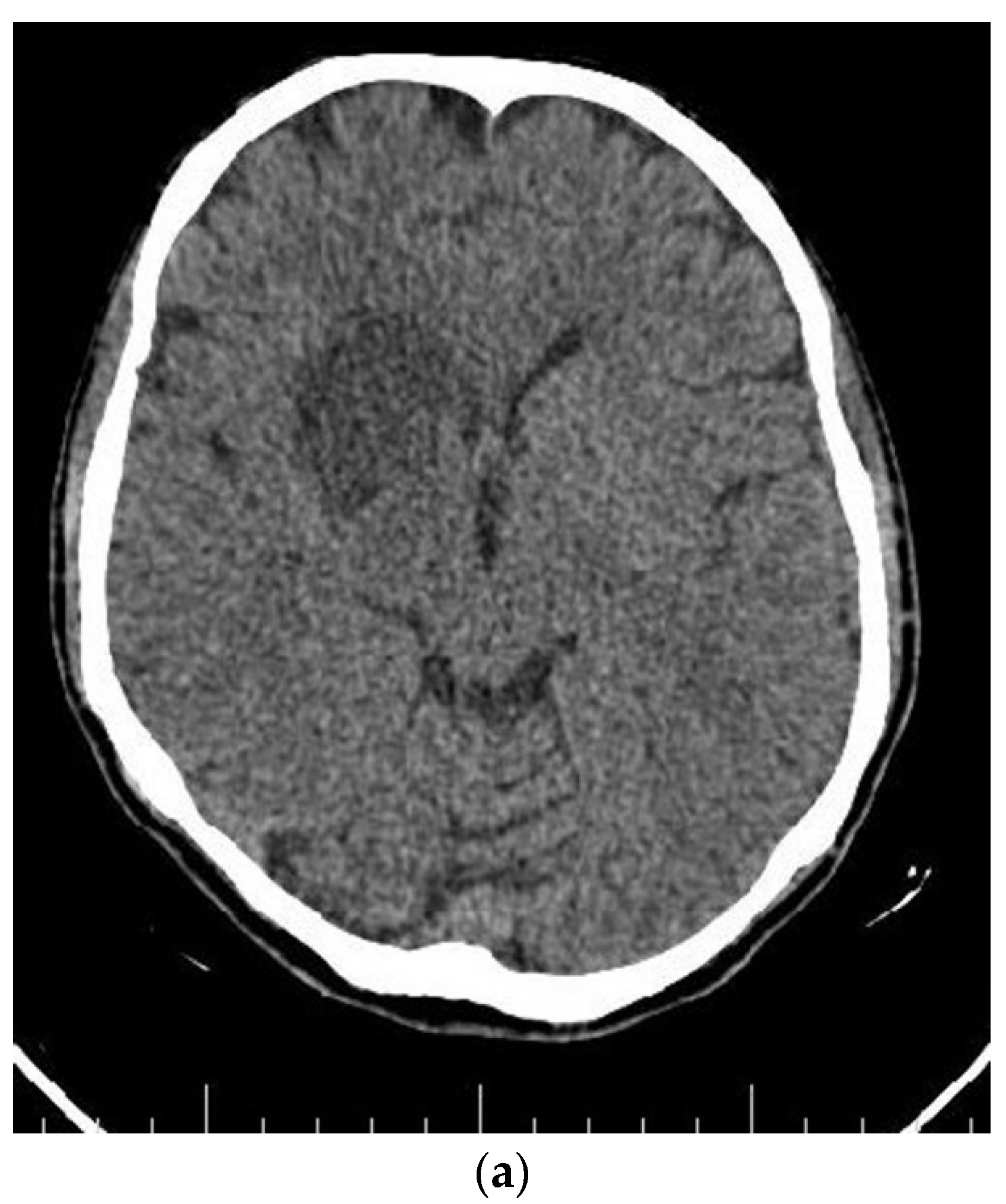
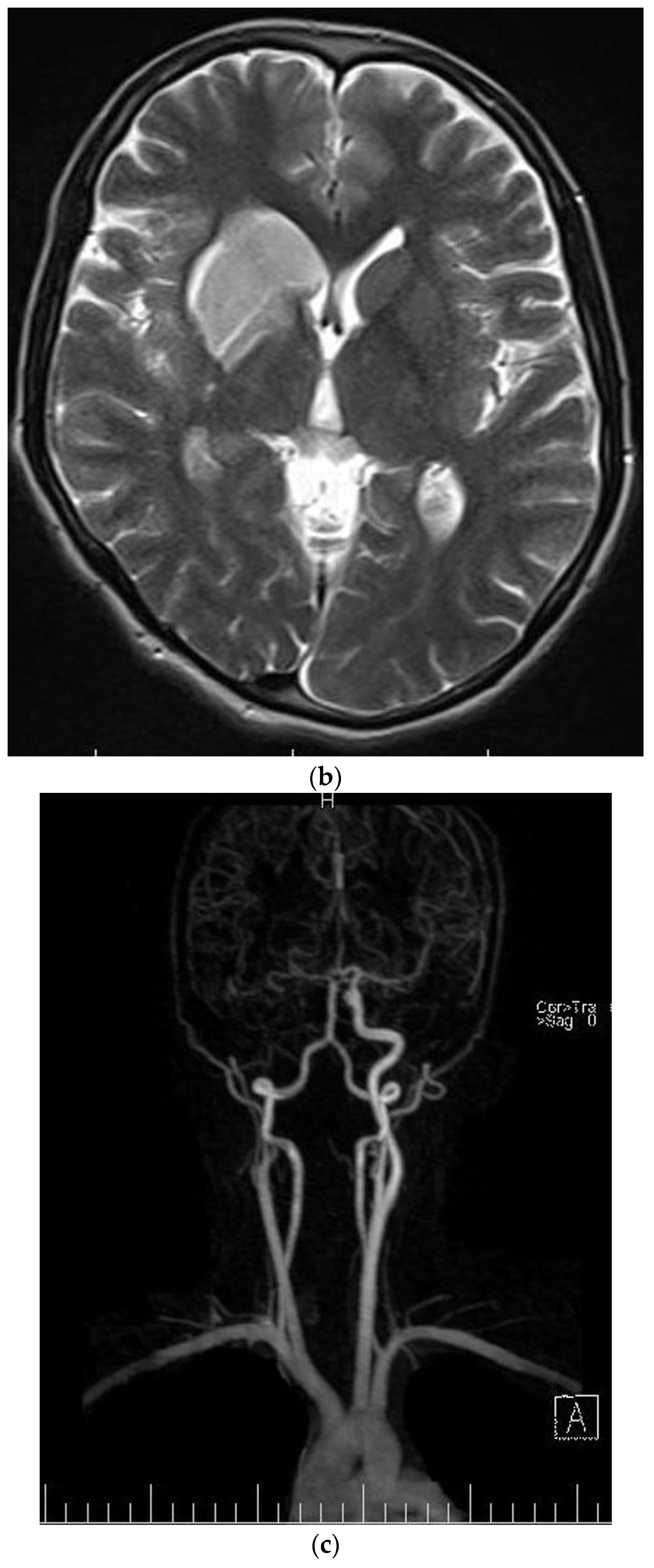
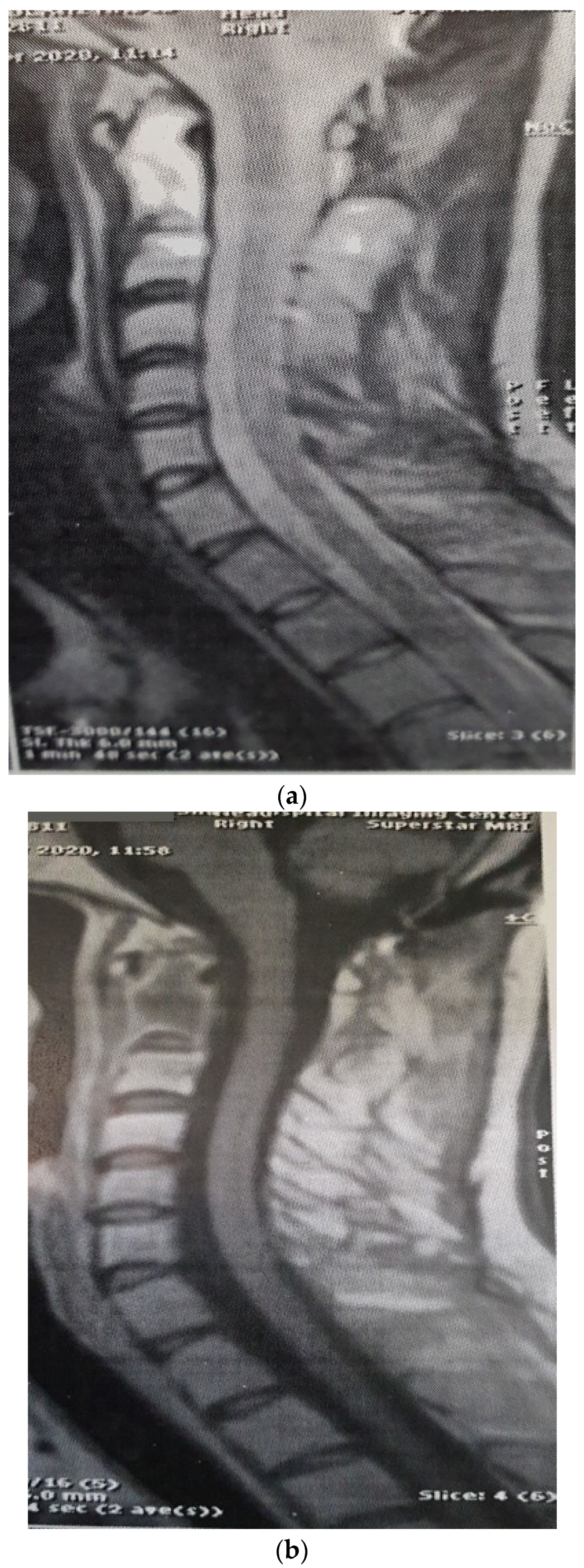
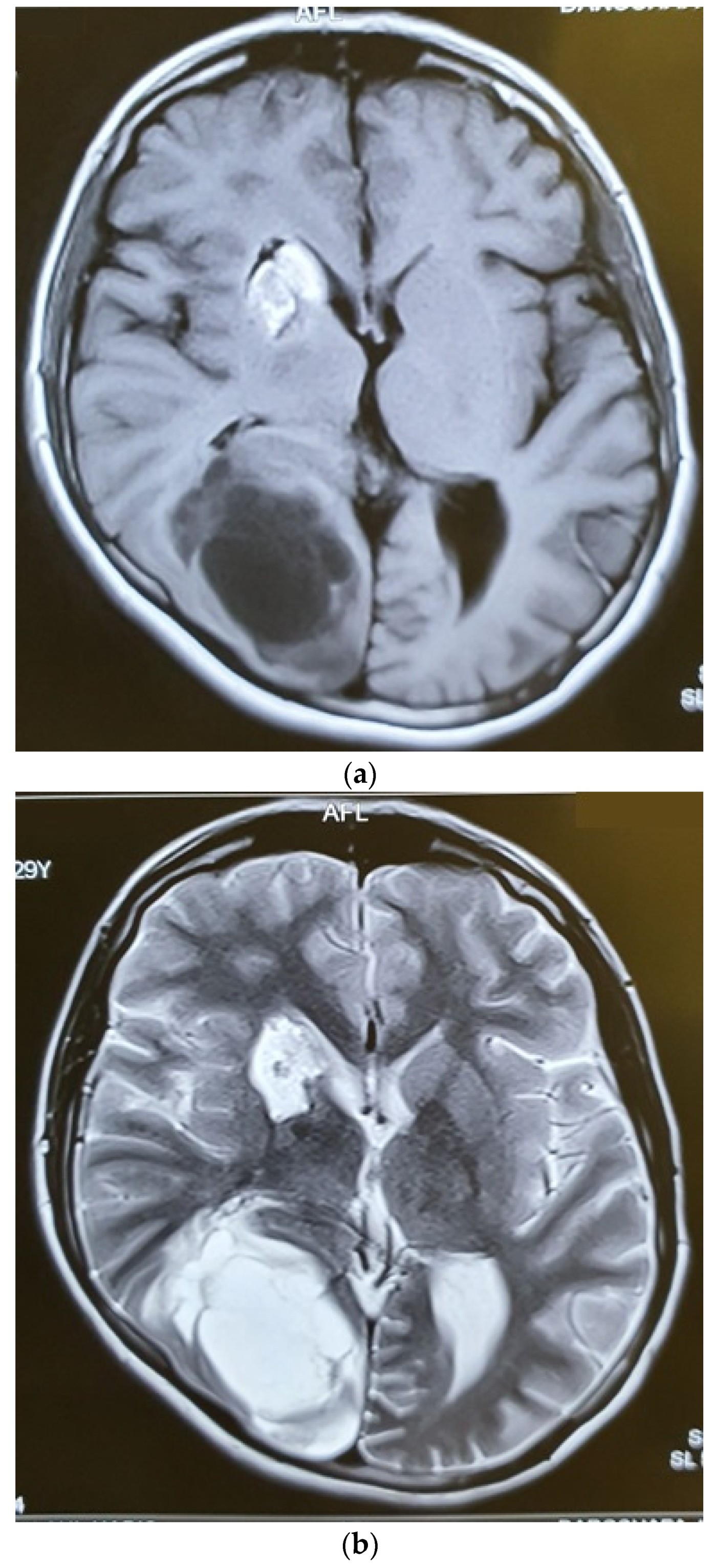
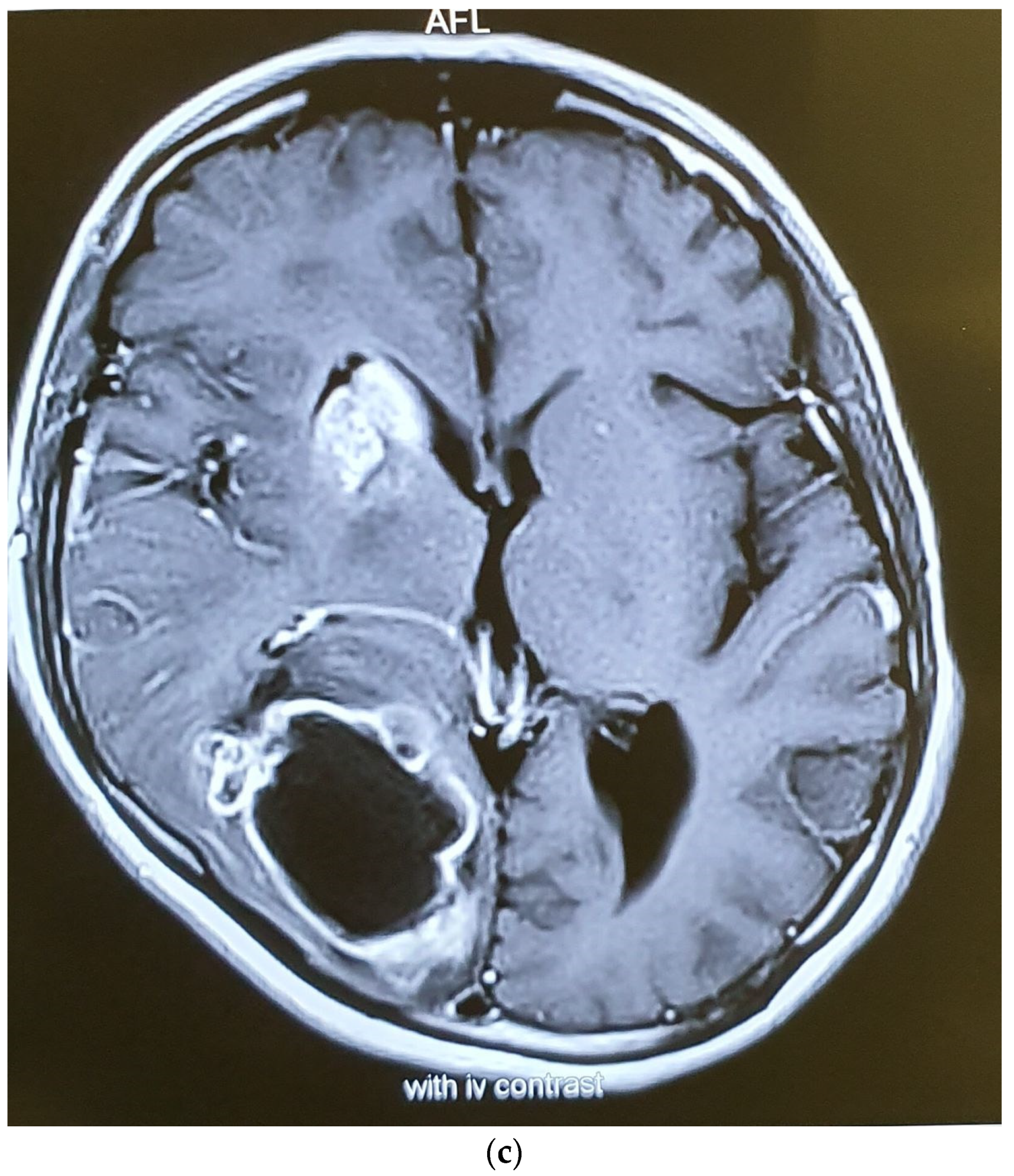
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CNS | Central nervous system |
| CT | Computed tomography |
| MR | Magnetic resonance |
| HS | Histiocytic sarcoma |
| DLBCL | Diffuse large B-cell lymphoma |
| ALCL | Anaplastic large cell lymphoma |
| IHC | Immunohistochemical |
| PET | Positron emission tomography |
References
- Hornick, J.L.; Jaffe, E.S.; Fletcher, C.D. Extranodal histiocytic sarcoma: Clinicopathologic analysis of 14 cases of a rare epithelioid malignancy. Am. J. Surg. Pathol. 2004, 28, 1133–1144. [Google Scholar] [CrossRef] [PubMed]
- Patnaik, A.; Mishra, S.S.; Senapati, S.B. A rare case of primary extranodal, extradural histiocytic sarcoma of the thoracic spine and review of literature. Surg. Neurol. Int. 2012, 3, 96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, E.; Hutchinson, C.B.; Huang, Q.; Sebastian, S.; Rehder, C.; Kanaly, A.; Moore, J.; Datto, M. Histiocytic sarcoma arising in indolent small B-cell lymphoma: Report of two cases with molecular/genetic evidence suggestive of a ‘transdifferentiation’ during the clonal evolution. Leuk. Lymphoma 2010, 51, 802–812. [Google Scholar] [CrossRef] [PubMed]
- Shinoda, H.; Yoshida, A.; Teruya-Feldstein, J. Malignant histiocytoses/disseminated histiocytic sarcoma with hemophagocytic syndrome in a patient with mediastinal germ cell tumor. Appl. Immunohistochem. Mol. Morphol. 2009, 17, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Buonocore, S.; Valente, A.L.; Nightingale, D.; Bogart, J.; Souid, A.K. Histiocytic sarcoma in a 3-year-old male: A case report. Pediatrics 2005, 116, e322–e325. [Google Scholar] [CrossRef] [PubMed]
- Kaushal, R.; Jambhekar, N.A.; Rao, S.; Raju, S.; Suryawanshi, P.; Shet, T.; Puri, A. Primary extranodal histiocytic sarcoma of lumbar spine. Skelet. Radiol. 2012, 41, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Lin, B.; Chen, Z.W.; Wang, N.; Guo, Z.M.; Liu, H.; Zeng, M. Total en bloc spondylectomy of L3 vertebra for histiocytic sarcoma. Orthopedics 2012, 35, e610–e614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pileri, S.A.; Grogan, T.M.; Harris, N.L.; Banks, P.; Campo, E.; Chan, J.K.; Favera, R.D.; Delsol, G.; De Wolf-Peeters, C.; Falini, B.; et al. Tumours of histiocytes and accessory dendritic cells: An immunohistochemical approach to classification from the International Lymphoma Study Group based on 61 cases. Histopathology 2002, 41, 1–29. [Google Scholar] [CrossRef] [PubMed]
- Sohn, B.S.; Kim, T.; Kim, J.E.; Bae, E.; Park, C.J.; Huh, J.; Lee, S.O. A case of histiocytic sarcoma presenting with primary bone marrow involvement. J. Korean Med. Sci. 2010, 25, 313–316. [Google Scholar] [CrossRef] [PubMed]
- Skala, S.L.; Lucas, D.R.; Dewar, R. Histiocytic Sarcoma: Review, Discussion of Transformation From B-Cell Lymphoma, and Differential Diagnosis. Arch. Pathol. Lab. Med. 2018, 142, 1322–1329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, S.; Schild, M.; Tran, D.; Zhang, X.; Zhang, W.L.; Shen, S.; Xu, H.T.; Yang, L.H.; Wang, E. Primary central nervous system histiocytic sarcoma: A case report and review of literature. Medicine 2018, 97, e11271. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Nordberg, M.L.; Fowler, M.R. Histiocytic sarcoma involving the central nervous system: Clinical, immunohistochemical, and molecular genetic studies of a case with review of the literature. Am. J. Surg. Pathol. 2003, 27, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Go, H.; Jeon, Y.K.; Huh, J.; Choi, S.J.; Choi, Y.D.; Cha, H.J.; Kim, H.J.; Park, G.; Min, S.; Kim, J.E. Frequent detection of BRAF(V600E) mutations in histiocytic and dendritic cell neoplasms. Histopathology 2014, 65, 261–272. [Google Scholar] [CrossRef] [PubMed]
- Facchetti, F.; Pileri, S.A.; Lorenzi, L.; Tabanelli, V.; Rimsza, L.; Pittaluga, S.; Dirnhofer, S.; Copie-Bergman, C.; de Leval, L.; Rosenwald, A.; et al. Histiocytic and dendritic cell neoplasms: What have we learnt by studying 67 cases. Virchows Arch. 2017, 471, 467–489. [Google Scholar] [CrossRef] [PubMed]
- Pericart, S.; Waysse, C.; Siegfried, A.; Struski, S.; Delabesse, E.; Laurent, C.; Evrard, S. Subsequent development of histiocytic sarcoma and follicular lymphoma: Cytogenetics and next-generation sequencing analyses provide evidence for transdifferentiation of early common lymphoid precursor-a case report and review of literature. Virchows Arch. 2020, 476, 609–614. [Google Scholar] [CrossRef] [PubMed]
- Kommalapati, A.; Tella, S.H.; Go, R.S.; Goyal, G. Predictors of survival, treatment patterns, and outcomes in histiocytic sarcoma. Leuk. Lymphoma 2019, 60, 553–555. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Patel, J.L.; Tao, R.; Cannon, R.B.; Monroe, M.; Goyal, G. Near Complete Response to Trametinib Treatment in Histiocytic Sarcoma Harboring a Somatic KRAS Mutation. J. Natl. Compr. Canc. Netw. 2022, 20, 618–621. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author/Year | Age/Sex | Location | IHC | Treatment | Follow-Up |
|---|---|---|---|---|---|
| Pileri et al. (2002) [8] | 26, male | T4, T5 | CD 68, lysozyme, S100, CD45 | Radiotherapy and autologous bone marrow transplantation at the time of relapse | After 3 years, alive in complete remisssion |
| Kaushal et al. (2012) [6] | 17, male | L3 | LCA, vimentin, CD68, CD163, Ki67 20% | Surgery + radiotherapy | Disease-free 3.5 years after surgery |
| Lin et al. (2012) [7] | 27, female | L3 | Cd68, vimentin, S100 | Surgery (spondylectomy) without adjuvant treatment | No recurrence after 2 years |
| Patnaik et al. (2012) [2] | 22, male | T8, T9 | S100, CD38, Lysosyme | Partial excision without adjuvant treatment | Alive after 5 months |
| Buonocore et al. (2005) [5] | 3, male | L4, T6 | CD68, focal S100, CD15 | Surgery and radiotherapy just to L4 and chemotherapy, and thereafter, chemoradiotherapy to pulmonary metastases | Two pulmonary nodules developed no change in the T6 lesion |
| Sohn et al. (2010) [9] | 63, male | Multiple thoraco lumbar vertebra | CD68, S100 protein, CD31, CD99, vimentin weakly positive for: CD21, CD4, lysozyme | The patient refused all treatments | Died after 2 months |
| The current case | 29, female | C2 | CD45, CD43, CD68, S100 | Surgery and radiotherapy | Brain metastasis after 9 months |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bahrami, E.; Najafi, M.; Jahanbakhshi, A.; Hatam, J.; Molanaei, S.; Ciammella, P.; Cozzi, S. Histiocytic Sarcoma Involving Cervical Vertebra: A Case Report and Review of the Literature. Brain Sci. 2022, 12, 958. https://doi.org/10.3390/brainsci12070958
Bahrami E, Najafi M, Jahanbakhshi A, Hatam J, Molanaei S, Ciammella P, Cozzi S. Histiocytic Sarcoma Involving Cervical Vertebra: A Case Report and Review of the Literature. Brain Sciences. 2022; 12(7):958. https://doi.org/10.3390/brainsci12070958
Chicago/Turabian StyleBahrami, Eshagh, Masoumeh Najafi, Amin Jahanbakhshi, Jaber Hatam, Saadat Molanaei, Patrizia Ciammella, and Salvatore Cozzi. 2022. "Histiocytic Sarcoma Involving Cervical Vertebra: A Case Report and Review of the Literature" Brain Sciences 12, no. 7: 958. https://doi.org/10.3390/brainsci12070958