
Assessment of Vestibular-Evoked Myogenic Potentials in Parkinson’s Disease: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Article Selection
2.3. Diagnosis of PD and Measurement of VEMPs
2.4. Data Extraction
2.5. Quality Assessment

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Total n | Design | % F | Age | Type | Acoustic Stimuli |
|---|---|---|---|---|---|---|
| Pollak et al., 2009 [22] | PD n = 54 Control n = 53 | CC | 48.9 62.7 | 66 ± 10.1 46 ± 15 | cVEMP | ACS |
| de Natale et al., 2015 (a) [8] | PD n = 33 Control n = 27 | CS | 48.5 44.4 | 65.65 ± 6.78 61.8 ± 9.54 | cVEMP oVEMP mVEMP | ACS |
| de Natale et al., 2015 (b) [11] | PD n = 24 Control n = 24 | CS | 41.6 37.5 | 66.2 ± 6.8 61.9 ± 9.54 | cVEMP oVEMP mVEMP | ACS |
| Venhovens et al., 2016 [13] | PD n = 30 Control n = 25 | CC | 13.3 40 | 70 ± 7 67 ± 10 | cVEMP oVEMP | ACS |
| Hassan et al., 2017 [23] | PD n = 15 Control n = 15 | CS | 20 33.3 | 59.2 ± 10.08 59 ± 9 | cVEMP | ACS |
| Lazzaro et al., 2018 [6] | PD n = 15 Control n = 30 | CS | 46.7 50 | 69.6 ± 7.11 69.36 ± 6.67 | cVEMP | ACS |
| Cicekli et al., 2019 [17] | PD n = 30 Control n = 28 | CS | 46.7 28.6 | 60.6 ±13.1 59.1 ± 6.4 | cVEMP | ACS |
| Hussein et al., 2019 [16] | PD n = 18 Control n = 15 | CC | 20 46.67 | 64.8 ± 7.488 64.27 ± 5.257 | cVEMP | ACS |
| Mohammed et al., 2019 [24] | PD n = 6 Control n = 14 | CS | 46.2 57.1 | 68.67 ± 6.5 64.79 ± 6.1 | cVEMP | ACS |
| Scarpa et al., 2020 [25] | PD n = 15 Control n = 20 | CC | 26.7 45 | 64.3 ± 7.1 64.5 ± 6.9 | cVEMP | ACS |
| Hawkins et al., 2020 [26] | PD n = 40 Control n = 40 | CC | 32 37 | 69.58 ± 6.27 69.88 ± 5.41 | cVEMP oVEMP | ACS BCV |
| Ampar et al., 2021 [27] | PD n = 25 Control n = 25 | CC | 24 40 | 68.3 ± 8.9 65.0 ± 7.9 | cVEMP | ACS |
| Klunk et al., 2021 [14] | PD n = 30 Control n = 30 | CS | 40 40 | 65.1 ±10.8 63.4 ± 11.8 | cVEMP oVEMP | ACS |
| Berkiten et al., 2022 [7] | PD n = 40 Control n = 40 | CS | 40 55 | 63.2 ± 7.94 60.36 ±7.68 | cVEMP oVEMP | ACS |
| Xie et al., 2022 [15] | PD n = 82 Control n = 41 | CS | 43.9 48.8 | 62.9 ± 7.89 61.49 ± 8.39 | cVEMP oVEMP mVEMP | ACS |
2.6. Statistical Analysis
3. Results
3.1. Description of Studies
3.2. Abnormal Findings of VEMPs
3.2.1. Absence Rates of VEMPs
3.2.2. Changes in VEMP Latencies
3.2.3. Peak-to-Peak Amplitudes
3.2.4. Amplitude Asymmetry Ratio (AAR)
3.2.5. Interside Peak Difference
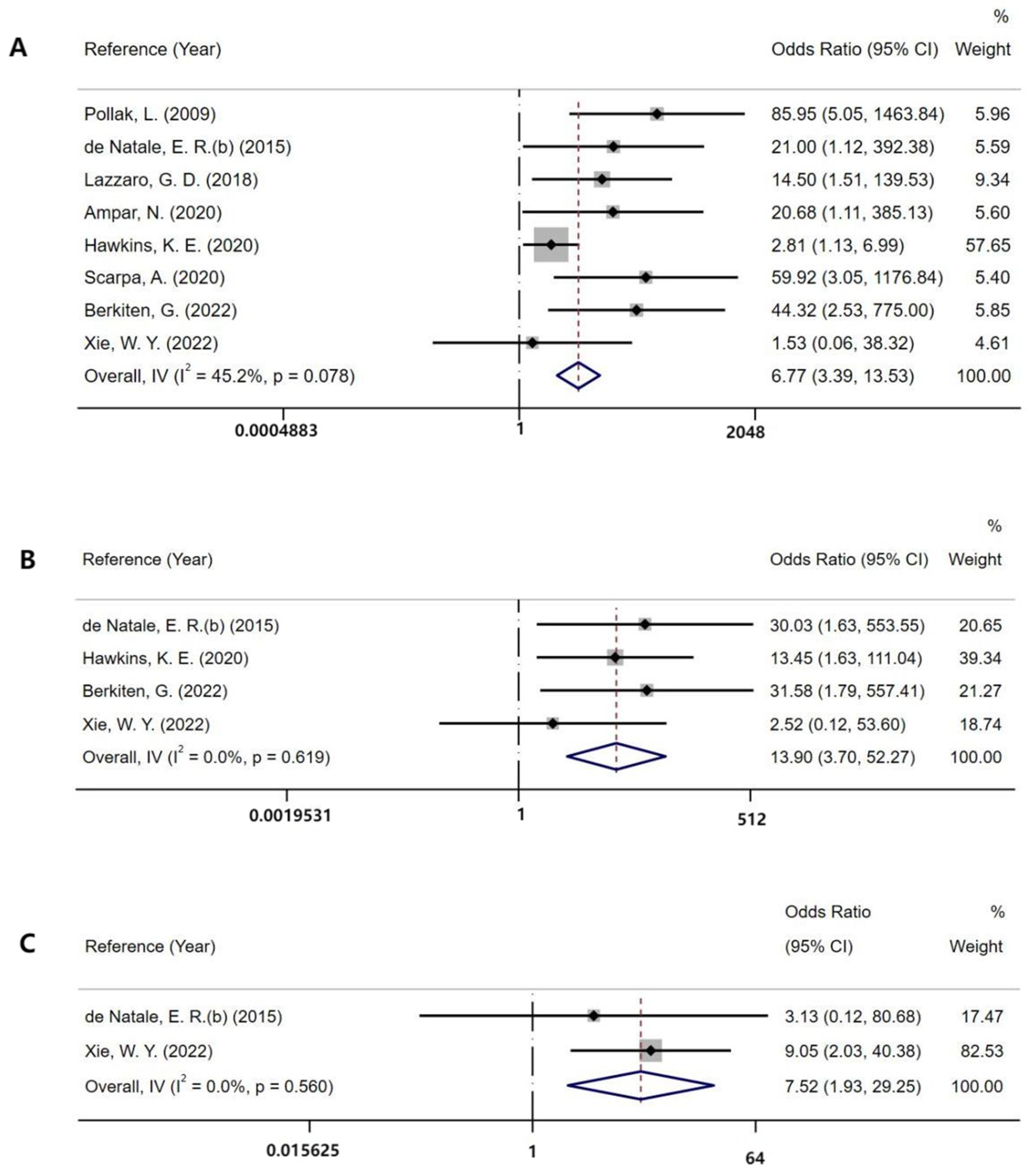
3.3. Fall
3.4. Subgroup Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Database | Search Terms |
|---|---|
| PubMed | ((Parkinson’s disease) OR (Primary Parkinsonism) OR (Paralysis Agitans))AND((vestibular evoked myogenic potential) OR VEMP OR oVEMP OR cVEMP OR (vestibulospinal Dysfunction) OR (vestibular dysfunction) OR (Vestibulospinal Reflex)) |
| Embase | 1.‘Parkinson disease’/exp 2.‘Parkinson disease’:ab,ti OR ‘Primary Parkinsonism’:ab,ti OR ‘Paralysis Agitans’:ab,ti 3.#1 OR #2 4.‘vestibular evoked myogenic potential ‘:ab,ti OR ‘VEMP’:ab,ti OR ‘vestibulospinal Dysfunction’:ab,ti OR ‘vestibular dysfunction’:ab,ti OR ‘Vestibulospinal Reflx’:ab,ti OR ‘oVEMP’:ab,ti OR ‘mVEMP’:ab,ti 5.#3 AND #4 6.[conference review]/lim OR [conference Abstract]/lim OR [conference Paper]/lim OR [editorial]/lim OR [erratum]/lim OR [letter]/lim 7.#5 NOT#6 |
| Web of Science | (TS= (vestibular evoked myogenic potential OR VEMP OR oVEMP OR cVEMP OR vestibulospinal Dysfunction OR vestibular dysfunction OR Vestibulospinal Reflex)) AND (TS = (Parkinson’s disease OR Primary Parkinsonism Paralysis Agitans)) |
Appendix B
| Study | S1 | S2 | S3 | S4 | C1 | E1 | E2 | E3 | Total |
|---|---|---|---|---|---|---|---|---|---|
| Pollak et al., 2009 [22] | - | - | - | ★ | - | ★ | ★ | ★ | 4 |
| de Natale et al., 2015 (a) [8] | ★ | - | - | ★ | ★★ | ★ | ★ | ★ | 7 |
| de Natale et al. 2015 (b) [11] | - | - | - | ★ | ★★ | ★ | ★ | ★ | 6 |
| Venhovens et al., 2016 [13] | ★ | - | - | ★ | ★★ | ★ | ★ | ★ | 7 |
| Hassan et al. 2017 [23] | ★ | - | - | ★ | ★ | ★ | ★ | ★ | 6 |
| Lazzaro et al., 2018 [6] | ★ | ★ | - | ★ | ★★ | ★ | ★ | ★ | 8 |
| Cicekli et al., 2019 [17] | - | ★ | - | ★ | ★ | ★ | ★ | ★ | 6 |
| Hussein et al. 2019 [16] | ★ | ★ | - | ★ | ★★ | ★ | ★ | ★ | 8 |
| Mohammed et al., 2019 [24] | - | ★ | - | ★ | ★ | ★ | ★ | ★ | 6 |
| Scarpa et al., 2020 [25] | ★ | - | - | ★ | ★★ | ★ | ★ | ★ | 7 |
| Hawkins et al., 2020 [26] | - | ★ | ★ | ★ | ★★ | ★ | ★ | ★ | 8 |
| Ampar et al., 2021 [27] | ★ | ★ | - | ★ | ★ | ★ | ★ | ★ | 7 |
| Klunk et al., 2021 [14] | ★ | - | - | ★ | ★★ | ★ | ★ | ★ | 7 |
| Berkiten et al., 2022 [7] | ★ | - | - | ★ | ★★ | ★ | ★ | ★ | 7 |
| Xie et al., 2022 [15] | ★ | ★ | - | ★ | ★★ | ★ | ★ | ★ | 8 |
References
- Ascherio, A.; Schwarzschild, M.A. The epidemiology of Parkinson’s disease: Risk factors and prevention. Lancet Neurol. 2016, 15, 1257–1272. [Google Scholar] [PubMed]
- Simon, D.K.; Tanner, C.M.; Brundin, P. Parkinson Disease Epidemiology, Pathology, Genetics, and Pathophysiology. Clin. Geriatr. Med. 2020, 36, 1–12. [Google Scholar] [PubMed]
- Tolosa, E.; Garrido, A.; Scholz, S.W.; Poewe, W. Challenges in the diagnosis of Parkinson’s disease. Lancet Neurol. 2021, 20, 385–397. [Google Scholar] [PubMed]
- Figura, M.; Friedman, A. In search of Parkinson’s disease biomarkers-is the answer in our mouths? A systematic review of the literature on salivary biomarkers of Parkinson’s disease. Neurol. Neurochir. Pol. 2020, 54, 14–20. [Google Scholar]
- Miller, D.B.; O’Callaghan, J.P. Biomarkers of Parkinson’s disease: Present and future. Metabolism 2015, 64, S40–S46. [Google Scholar]
- Lazzaro, G.D.; Schirinzi, T.; Giambrone, M.P.; Mauro, R.D.; Palmieri, M.G.; Rocchi, C.; Tinazzi, M.; Mercuri, N.B.; Girolamo, S.D.; Pisani, A. Pisa syndrome in Parkinson’s disease: Evidence for bilateral vestibulospinal dysfunction. Parkinson’s Dis. 2018, 2018, 8673486. [Google Scholar]
- Berkiten, G.; Tutar, B.; Atar, S.; Kumral, T.L.; Saltürk, Z.; Akan, O.; Sari, H.; Onaran, Ö.; Biltekin Tuna, Ö.; Uyar, Y. Assessment of the Clinical Use of Vestibular Evoked Myogenic Potentials and the Video Head Impulse Test in the Diagnosis of Early-Stage Parkinson’s Disease. Ann. Otol. Rhinol. Laryngol. 2022, Epub ahead of print. 34894211067838. [Google Scholar]
- De Natale, E.R.; Ginatempo, F.; Paulus, K.S.; Manca, A.; Mercante, B.; Pes, G.M.; Agnetti, V.; Tolu, E.; Deriu, F. Paired neurophysiological and clinical study of the brainstem at different stages of Parkinson’s Disease. Clin. Neurophysiol. 2015, 126, 1871–1878. [Google Scholar]
- Taylor, R.L.; Welgampola, M.S.; Nham, B.; Rosengren, S.M. Vestibular-Evoked Myogenic Potential Testing in Vestibular Localization and Diagnosis. Semin. Neurol. 2020, 40, 18–32. [Google Scholar]
- Colebatch, J.G.; Rosengren, S.M.; Welgampola, M.S. Vestibular-evoked myogenic potentials. Handb. Clin. Neurol. 2016, 137, 133–155. [Google Scholar]
- De Natale, E.R.; Ginatempo, F.; Paulus, K.S.; Pes, G.M.; Manca, A.; Tolu, E.; Agnetti, V.; Deriu, F. Abnormalities of vestibular-evoked myogenic potentials in idiopathic Parkinson’s disease are associated with clinical evidence of brainstem involvement. Neurol. Sci. 2015, 36, 995–1001. [Google Scholar] [PubMed]
- Shalash, A.S.; Hassan, D.M.; Elrassas, H.H.; Salama, M.M.; Mendez-Hernandez, E.; Salas-Pacheco, J.M.; Arias-Carrion, O. Auditory- and Vestibular-Evoked Potentials Correlate with Motor and Non-Motor Features of Parkinson’s Disease. Front. Neurol. 2017, 8, 55. [Google Scholar] [PubMed]
- Venhovens, J.; Meulstee, J.; Bloem, B.R.; Verhagen, W.I. Neurovestibular analysis and falls in Parkinson’s disease and atypical parkinsonism. Eur. J. Neurosci. 2016, 43, 1636–1646. [Google Scholar] [PubMed] [Green Version]
- Klunk, D.; Woost, T.B.; Fricke, C.; Classen, J.; Weise, D. Differentiating neurodegenerative parkinsonian syndromes using vestibular evoked myogenic potentials and balance assessment. Clin. Neurophysiol. 2021, 132, 2808–2819. [Google Scholar] [PubMed]
- Xie, W.Y.; Shen, Y.; Chen, Y.; Zhuang, S.; Wang, Y.L.; Jin, H.; Li, H.X.; Yan, J.H.; Li, Y.; Mao, C.J.; et al. REM sleep without atonia and vestibular-evoked myogenic potentials: Clinical brainstem dysfunction in early-stage Parkinson’s disease and isolated REM sleep behavior disorder. Sleep Med. 2022, 89, 122–129. [Google Scholar] [PubMed]
- Hussein, M.; Koura, R. Auditory and vestibular dysfunction in patients with Parkinson’s disease. Egypt. J. Otolaryngol. 2019, 35, 313–321. [Google Scholar]
- Cicekli, E.; Titiz, A.P.; Titiz, A.; Oztekin, N.; Mujdeci, B. Vestibular Evoked Myogenic Potential Responses in Parkinson’s Disease. Ideggyogy. Szle Clin. Neurosci. 2019, 72, 419–425. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar]
- Hughes, A.J.; Daniel, S.E.; Kilford, L.; Lees, A.J. Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: A clinico-pathological study of 100 cases. J. Neurol. Neurosurg. Psychiatry 1992, 55, 181–184. [Google Scholar]
- Rosengren, S.M.; Colebatch, J.G.; Young, A.S.; Govender, S.; Welgampola, M.S. Vestibular evoked myogenic potentials in practice: Methods, pitfalls and clinical applications. Clin. Neurophysiol. Pract. 2019, 4, 47–68. [Google Scholar]
- Lo, C.K.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar]
- Pollak, L.; Prohorov, T.; Kushnir, M.; Rabey, M. Vestibulocervical reflexes in idiopathic Parkinson disease. Neurophysiol. Clin. 2009, 39, 235–240. [Google Scholar] [PubMed]
- Hassan, D.M.; Shalash, A. Auditory brainstem evoked responses and vestibular evoked myogenic potentials: Potential biomarkers in Parkinson’s disease. Egypt. J. Otolaryngol. 2017, 33, 508–517. [Google Scholar]
- Mohammed Ali, F.; Westling, M.; Zhao, L.H.L.; Corneil, B.D.; Camp, A.J. Splenius capitis: Sensitive target for the cVEMP in older and neurodegenerative patients. Eur. Arch. Oto-Rhino-Laryngol. 2019, 276, 2991–3003. [Google Scholar] [PubMed]
- Scarpa, A.; Cassandro, C.; Vitale, C.; Ralli, M.; Policastro, A.; Barone, P.; Cassandro, E.; Pellecchia, M.T. A comparison of auditory and vestibular dysfunction in Parkinson’s disease and Multiple System Atrophy. Parkinsonism Relat. Disord. 2020, 71, 51–57. [Google Scholar] [PubMed]
- Hawkins, K.E.; Chiarovano, E.; Paul, S.S.; MacDougall, H.G.; Curthoys, I.S. Static and dynamic otolith reflex function in people with Parkinson’s disease. Eur. Arch. Oto-Rhino-Laryngol. 2021, 278, 2057–2065. [Google Scholar]
- Ampar, N.; Mehta, A.; Mahale, R.R.; Javali, M.; Pradeep, R.; Acharya, P.; Srinivasa, R. Electrophysiological Evaluation of Audiovestibular Pathway Dysfunction in Parkinson’s Disease and Its Correlates: A Case Control Study. Ann. Indian Acad. Neurol. 2021, 24, 531–535. [Google Scholar]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [PubMed]
- Hawkins, K.E.; Paul, S.S.; Chiarovano, E.; Curthoys, I.S. Using virtual reality to assess vestibulo-visual interaction in people with Parkinson’s disease compared to healthy controls. Exp. Brain Res. 2021, 239, 3553–3564. [Google Scholar] [PubMed]







| Outcomes | Findings | Subgroup | Studies, n | SMD (95%CI) | I2 (%) | p |
|---|---|---|---|---|---|---|
| cVEMP | P13 latency | Total | 15 | 0.55 (0.09, 1.02) | 90.5 | <0.001 |
| Age | 15 | 0.55 (0.09, 1.02) | 90.5 | <0.001 | ||
| <65 years old | 6 | 0.97 (−0.19, 2.14) | 95.6 | <0.001 | ||
| ≥65 years old | 9 | 0.30 (−0.04, 0.63) | 70.4 | 0.001 | ||
| Hoehn and Yahr stage | 10 | 0.51 (−0.07, 1.08) | 92.2 | <0.001 | ||
| <2.5 | 7 | 0.33 (−0.40, 1.06) | 93.4 | <0.001 | ||
| ≥2.5 | 3 | 0.94 (−0.22, 2.11) | 91.4 | <0.001 | ||
| Peak-to-peak amplitude | Total | 10 | −0.54 (−0.95, −0.14) | 79.9 | <0.001 | |
| Age | 10 | −0.54 (−0.95, −0.14) | 79.9 | <0.001 | ||
| <65 years old | 4 | −1.05 (−2.16, 0.05) | 92.4 | <0.001 | ||
| ≥65 years old | 6 | −0.27 (−0.50, −0.05) | 1.9 | 0.404 | ||
| Hoehn and Yahr stage | 7 | −0.48 (−0.99, 0.03) | 84.4 | <0.001 | ||
| <2.5 | 5 | −0.03 (−0.24, 0.18) | 0 | 0.627 | ||
| ≥2.5 | 2 | −1.99 (−1.20, 0.05) | 93.4 | <0.001 | ||
| AAR | Total | 4 | 0.99 (0.54, 1.44) | 57.7 | 0.069 | |
| Age | 4 | 0.99 (0.54, 1.44) | 57.7 | 0.069 | ||
| <65 years old | 2 | 1.37 (0.19, 2.55) | 82.2 | 0.018 | ||
| ≥65 years old | 2 | 0.77 (0.38, 1.16) | 0 | 0.578 | ||
| Hoehn and Yahr stage | 4 | 0.99 (0.54, 1.44) | 57.7 | 0.069 | ||
| <2.5 | 3 | 0.79 (0.5, 1.09) | 0 | 0.841 | ||
| ≥2.5 | 1 | 2.04 (1.15, 2.93) | 0 | - | ||
| oVEMP | P15 latency | Total | 8 | 0.53 (0.10, 0.95) | 82.0 | <0.001 |
| Age | 8 | 0.53 (0.10, 0.95) | 82.0 | <0.001 | ||
| <65 years old | 3 | 0.43 (−0.73, 1.59) | 93.7 | <0.001 | ||
| ≥65 years old | 5 | 0.58 (0.28, 0.88) | 39.9 | 0.155 | ||
| Hoehn and Yahr stage | 8 | 0.53 (0.10, 0.95) | 82.0 | <0.001 | ||
| <2.5 | 7 | 0.51 (0.05, 0.98) | 84.5 | <0.001 | ||
| ≥2.5 | 1 | 0.64 (−0.09, 1.38) | 0 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cui, W.; Duan, Z.; Feng, J. Assessment of Vestibular-Evoked Myogenic Potentials in Parkinson’s Disease: A Systematic Review and Meta-Analysis. Brain Sci. 2022, 12, 956. https://doi.org/10.3390/brainsci12070956
Cui W, Duan Z, Feng J. Assessment of Vestibular-Evoked Myogenic Potentials in Parkinson’s Disease: A Systematic Review and Meta-Analysis. Brain Sciences. 2022; 12(7):956. https://doi.org/10.3390/brainsci12070956
Chicago/Turabian StyleCui, Wenqi, Zhenghao Duan, and Juan Feng. 2022. "Assessment of Vestibular-Evoked Myogenic Potentials in Parkinson’s Disease: A Systematic Review and Meta-Analysis" Brain Sciences 12, no. 7: 956. https://doi.org/10.3390/brainsci12070956