
Effects of Electromyography Bridge on Upper Limb Motor Functions in Stroke Participants: An Exploratory Randomized Controlled Trial

Abstract
:1. Introduction
2. Materials and Methods
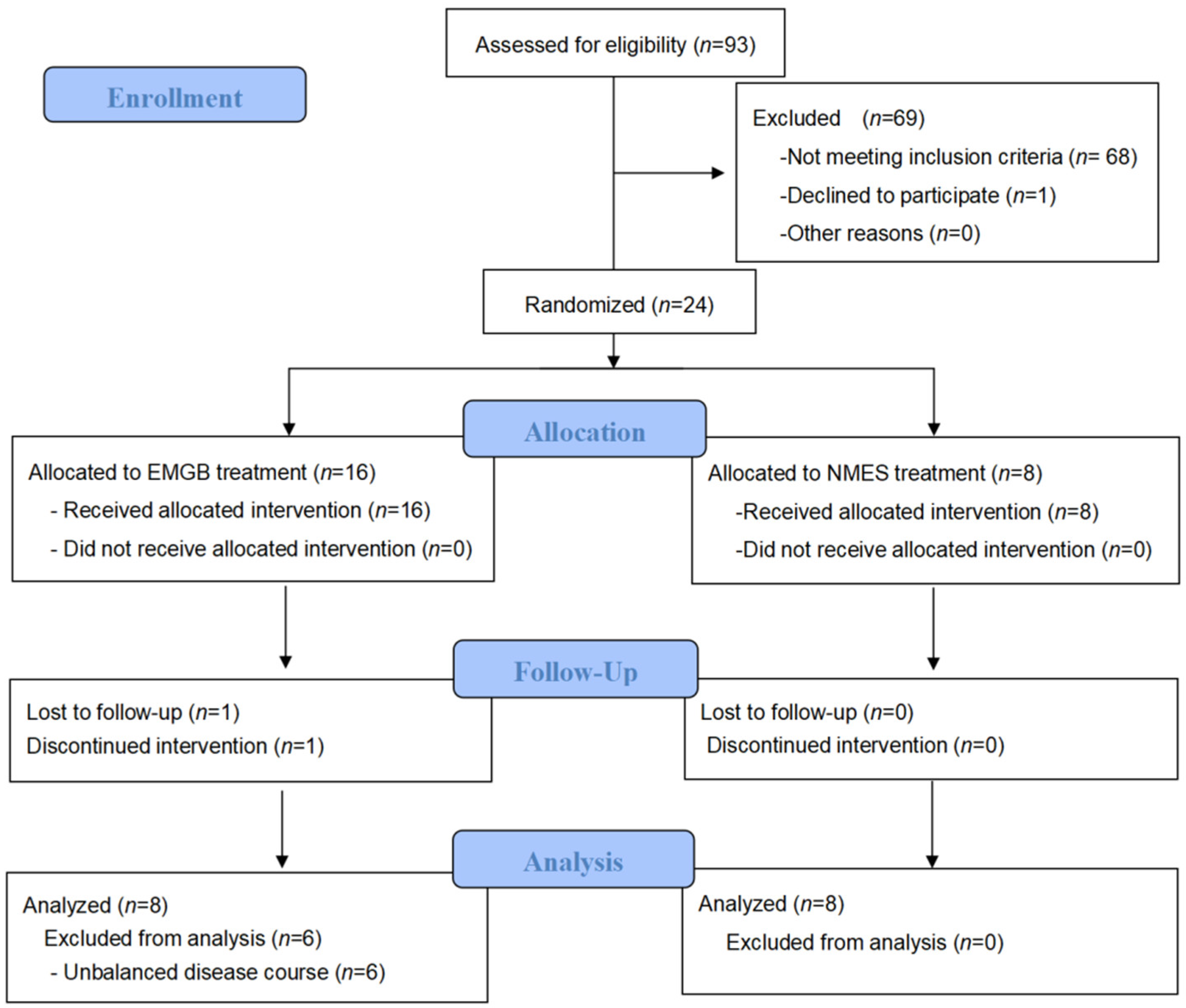
2.1. Study Design
2.2. Participants and Setting
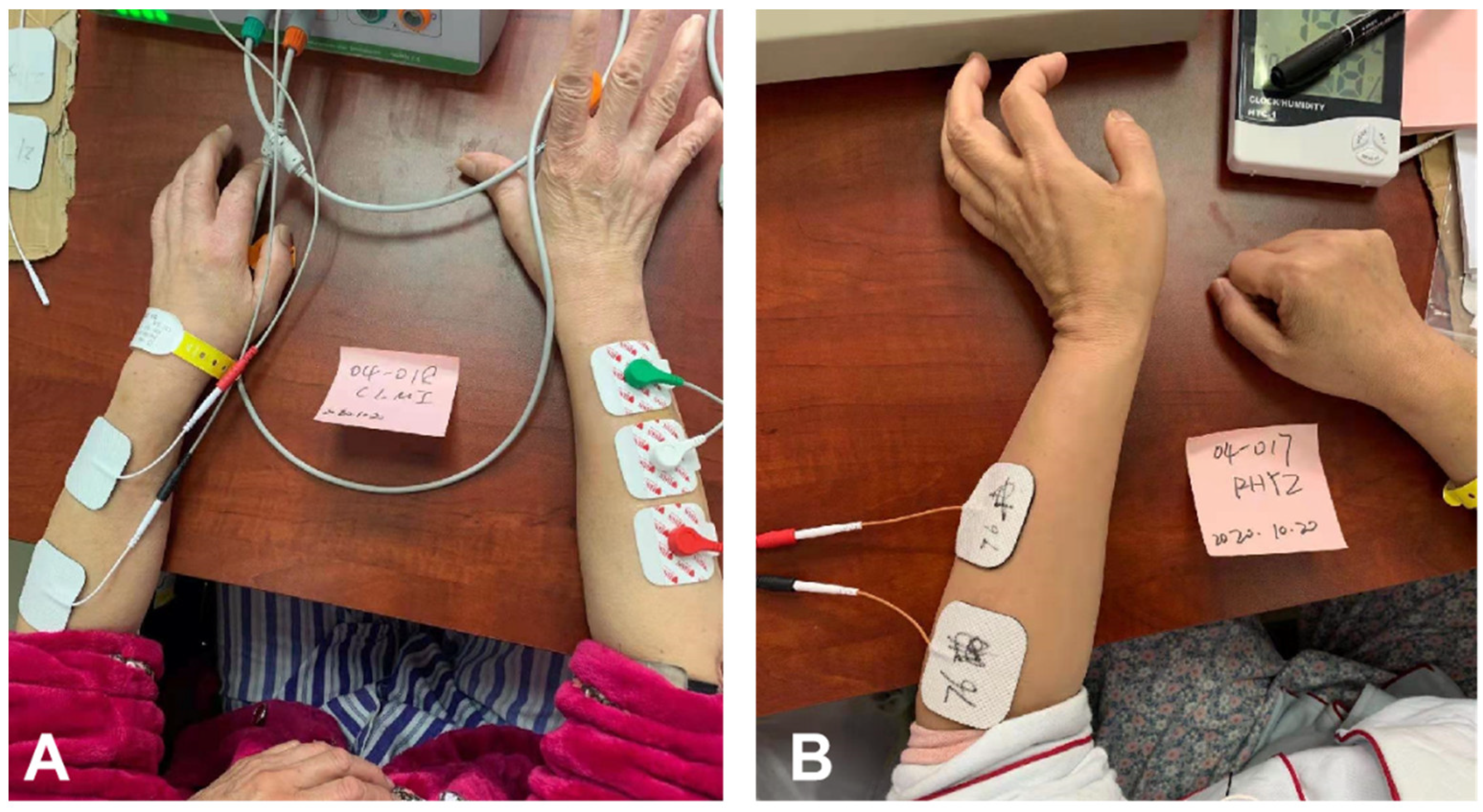
2.3. Procedure
2.3.1. EMGB Group
2.3.2. NMES Group
2.4. Outcome Measurement
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
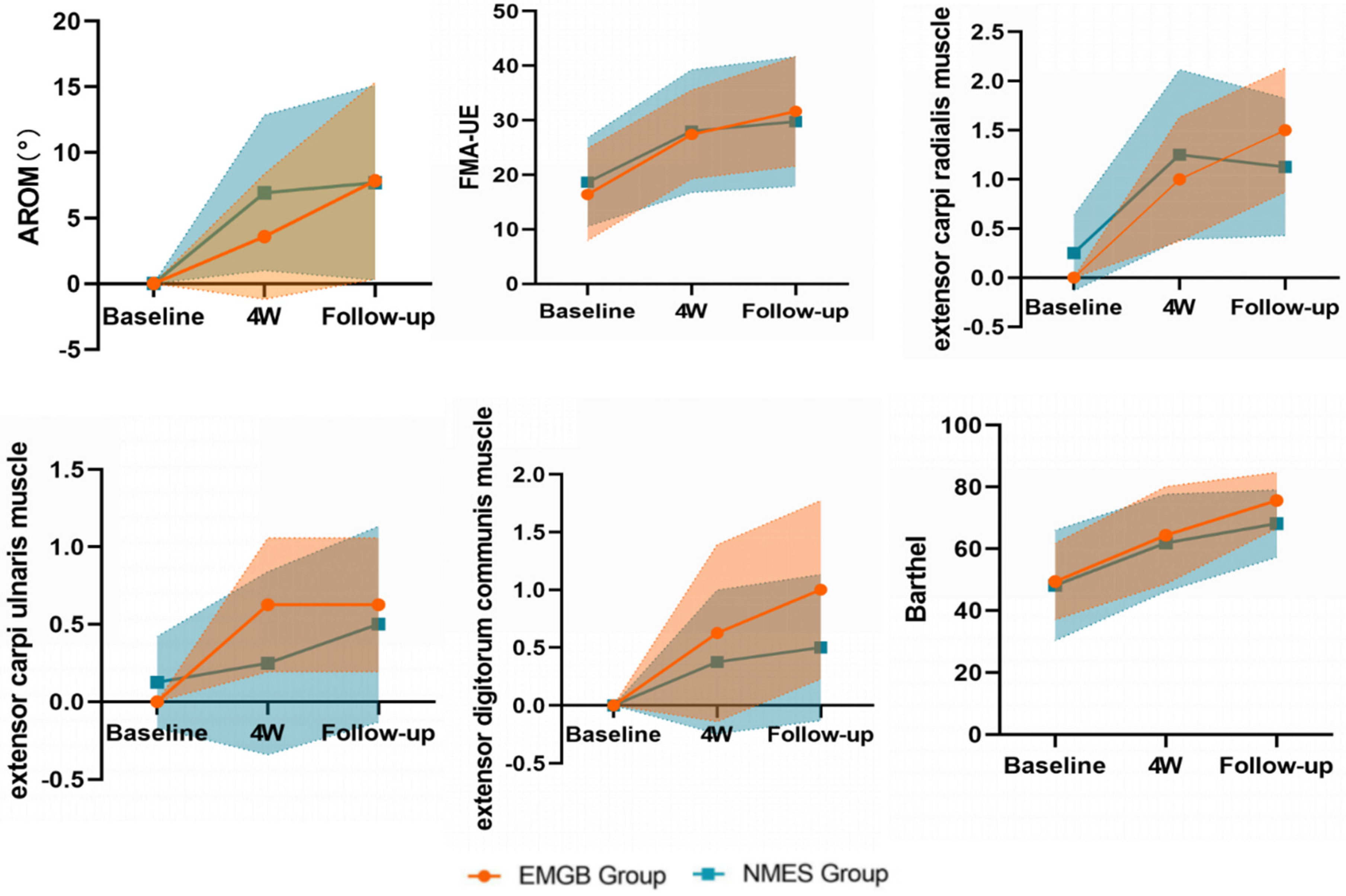
3.2. Primary Outcomes
3.3. Secondary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mozaffffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; de Ferranti, S.; Després, J.; Fullerton, H.J.; Howard, V.J.; et al. Heart disease and stroke statistics–2015 update: A report from the American Heart Association. Circulation 2015, 131, e29–e322. [Google Scholar]
- Feigin, V.L.; Lawes, C.M.M.; Bennett, D.A.; Anderson, C.S. Stroke epidemiology: A review of population-based studies of incidence, prevalence, and case-fatality in the late 20th century. Lancet Neurol. 2003, 2, 43–53. [Google Scholar] [CrossRef]
- Park, K.; Chang, P.H.; Kang, S.H. In Vivo Estimation of Human Forearm and Wrist Dynamic Properties. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 436–446. [Google Scholar] [CrossRef] [PubMed]
- Dawson, J.; Pierce, D.; Dixit, A.; Kimberley, T.J.; Robertson, M.; Tarver, B.; Hilmi, O.; McLean, J.; Forbes, K.; Kilgard, M.P.; et al. Safety, Feasibility, and Efficacy of Vagus Nerve Stimulation Paired with Upper-Limb Rehabilitation after Ischemic Stroke. Stroke 2016, 47, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.Y.; Chair, S.Y.; Chau, J.P.C. Effectiveness of a strength-oriented psychoeducation on caregiving competence, problem-solving abilities, psychosocial outcomes and physical health among family caregiver of stroke survivors: A randomised controlled trial. Int. J. Nurs. Stud. 2018, 87, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Wang, D.; Wong, K.S.; Wang, Y. Stroke and stroke care in China: Huge burden, significant workload, and a national priority. Stroke 2011, 42, 3651–3654. [Google Scholar] [CrossRef] [PubMed]
- Carson, R.G.; Buick, A.R. Neuromuscular electrical stimulation-promoted plasticity of the human brain. J. Physiol. 2021, 599, 2375–2399. [Google Scholar] [CrossRef]
- Insausti-Delgado, A.; López-Larraz, E.; Omedes, J.; Ramos-Murguialday, A. Intensity and Dose of Neuromuscular Electrical Stimulation Influence Sensorimotor Cortical Excitability. Front. Neurosci. 2021, 15, 593360. [Google Scholar] [CrossRef]
- Yang, J.D.; Liao, C.H.; Huang, S.H.; Tam, K.A.; Liou, T.S.; Lee, Y.U.; Lin, C.H.; Chen, H.U. Effectiveness of electrical stimulation therapy in improving arm function after stroke: A systematic review and a meta-analysis of randomised controlled trials. Clin. Rehabi. 2019, 33, 1286–1297. [Google Scholar] [CrossRef]
- Sentandreu-Mañó, T.; Tomás, J.M.; Ricardo Salom Terrádez, J. A randomised clinical trial comparing 35 Hz versus 50 Hz frequency stimulation effects on hand motor recovery in older adults after stroke. Sci. Rep. 2021, 11, 9131. [Google Scholar] [CrossRef]
- Knutson, J.S.; Harley, M.Y.; Hisel, T.Z.; Makowski, N.S.; Fu, M.J.; Chae, J. Contralaterally controlled functional electrical stimulation for stroke rehabilitation. Annu. Int. Conf. IEEE. Eng. Med. Biol. Soc. 2012, 2012, 314–317. [Google Scholar] [PubMed] [Green Version]
- Knutson, J.S.; Gunzler, D.D.; Wilson, R.D.; Chae, J. Contralaterally Controlled Functional Electrical Stimulation Improves Hand Dexterity in Chronic Hemiparesis: A Randomized Trial. Stroke 2016, 47, 2596–2602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.X.; Wang, H.A.; Bao, X.U.; Lü, X.I.; Wang, Z.H. A frequency and pulse-width co-modulation strategy for transcutaneous neuromuscular electrical stimulation based on sEMG timedomain features. J. Neural. Eng. 2016, 13, 016004. [Google Scholar] [CrossRef]
- Huang, Z.H.; Wang, Z.; Lv, X.; Zhou, Y.; Wang, H.; Zong, S. A novel functional electrical stimulation-control system for restoring motor function of post-stroke hemiplegic patients. Neural. Regen. Res. 2014, 9, 2102–2110. [Google Scholar]
- Monte-Silva, K.; Piscitelli, D.; Norouzi-Gheidari, N.; Batalla, M.A.P.; Archambault, P.; Levin, M.F. Electromyogram-Related Neuromuscular Electrical Stimulation for Restoring Wrist and Hand Movement in Poststroke Hemiplegia: A Systematic Review and Meta-Analysis. Neurorehabilit. Neural Repair 2019, 33, 96–111. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.X.; Xia, Y.; Huang, J.; Wang, H.P.; Bao, X.L.; Bi, Z.Y.; Chen, X.B.; Gao, Y.J.; Lü, X.Y.; Wang, Z.G. Electromyographic bridge for promoting the recovery of hand movements in subacute stroke patients: A randomized controlled trial. J. Rehabil. Med. 2017, 49, 629–636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meilink, A.; Hemmen, B.; Seelen, H.A.; Kwakkel, G. Impact of EMG-triggered neuromuscular stimulation of the wrist and finger extensors of the paretic hand after stroke: A systematic review of the literature. Clin. Rehabil. 2008, 22, 291–305. [Google Scholar] [CrossRef]
- Boyaci, A.; Topuz, O.; Alkan, H.; Ozgen, M.; Sarsan, A.; Yildiz, N.; Ardic, F. Comparison of the effectiveness of active and passive neuromuscular electrical stimulation of hemiplegic upper extremities: A randomized, controlled trial. Int. J. Rehabil. Res. 2013, 36, 315–322. [Google Scholar] [CrossRef]
- Bernhardt, J.; Hayward, K.S.; Kwakkel, G.; Ward, N.S.; Wolf, S.L.; Borschmann, K.; Krakauer, J.W.; Boyd, L.A.; Carmichael, S.T.; Corbett, D.; et al. Agreed definitions and a shared vision for new standards in stroke recovery research: The Stroke Recovery and Rehabilitation Roundtable taskforce. Int. J. Stroke 2017, 12, 444–450. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Snaith, R.P. Hamilton rating scale for depression. Br. J. Psychiatry 1977, 131, 431–432. [Google Scholar] [CrossRef] [PubMed]
- Stinear, C.M.; Lang, C.E.; Zeiler, S.; Byblow, W.D. Advances and challenges in stroke rehabilitation. Lancet Neurol. 2020, 19, 348–360. [Google Scholar] [CrossRef]
- Zhou, Y.X.; Wang, H.P.; Cao, X.P.; Bi, Z.Y.; Gao, Y.J.; Chen, X.B.; Lu, X.-Y.; Wang, Z.-G. Electromyographic Bridge-a multi-movement volitional control method for functional electrical stimulation: Prototype system design and experimental validation. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2017, 2017, 205–208. [Google Scholar]
- Wang, Z.G.; Lü, X.Y.; Wang, H.P.; Bao, X.L.; Bi, Z.Y. Electromyographic bridge for motor function rehabilitation of paralyzed limbs. In Proceedings of the 12th National Conference of Chinese Society for Neuroscience, Tianjin, China, 12 October 2017. [Google Scholar]
- Stinear, C.M.; Barber, P.A.; Coxon, J.P.; Fleming, M.K.; Byblow, W.D. Priming the motor system enhances the effects of upper limb therapy in chronic stroke. Brain 2008, 131, 1381–1390. [Google Scholar] [CrossRef] [Green Version]
- Stewart, K.C.; Cauraugh, J.H.; Summers, J.J. Bilateral movement training and stroke rehabilitation: A systematic review and meta-analysi. J. Neurol. Sci. 2008, 244, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Khaslavskaia, S.; Sinkjaer, T. Motor cortex excitability following repetitive electrical stimulation of the common peroneal nerve depends on the voluntary drive. Exp. Brain Res. 2005, 162, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Buetefisch, C.; Heger, R.; Schicks, W.; Seitz, R.; Netz, J. Hebbiantype stimulation during robot-assisted training in patients with stroke. Neurorehabil. Neural. Repair 2016, 25, 645–655. [Google Scholar] [CrossRef]
- Ring, H.; Rosenthal, N. Controlled study of neuroprosthetic functional electrical stimulation in sub-acute post-stroke rehabilitation. J. Rehabil. Med. 2005, 37, 32–36. [Google Scholar] [CrossRef] [Green Version]
- Lin, Z.; Yan, T. Long-term effectiveness of neuromuscular electrical stimulation for promoting motor recovery of the upper extremity after stroke. J. Rehabil. Med. 2011, 43, 506–510. [Google Scholar]
- Bolton, D.A.; Cauraugh, J.H.; Hausenblas, H.A. Electromyogram-triggered neuromuscular stimulation and stroke motor recovery of arm/hand functions: A meta-analysis. J. Neurol. Sci. 2004, 223, 121–127. [Google Scholar] [CrossRef]
- Shin, H.K.; Cho, S.H.; Jeon, H.S.; Lee, Y.H.; Song, J.C.; Jang, S.H.; Lee, C.H.; Kwon, Y.H. Cortical effect and functional recovery by the electromyography-triggered neuromuscular stimulation in chronic stroke patients. Neurosci. Lett. 2008, 442, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Hemmen, B.; Seelen, H.A. Effects of movement imagery and electromyography-triggered feedback on arm hand function in stroke patients in the subacute phase. Clin. Rehabil. 2007, 21, 587–594. [Google Scholar] [CrossRef] [PubMed]
- Andrews, A.W.; Bohmmon, R.W. Distribution of muscle strength impairments following stroke. Clin. Rehabil. 2000, 14, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Dewald, J.P.A.; Sheshadri, V.; Dawson, M.L.; Beer, R.F. Upperlimb discoordination in hemiparetic stroke: Implications for neurorehabilitation. Top. Stroke Rehabil. 2001, 8, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, N.; Izumi, S.I. Maladaptive plasticity for motor recovery after stroke: Mechanisms and approaches. Neural. Plast. 2012, 2012, 359728. [Google Scholar] [CrossRef]
- Gates, D.H.; Walters, L.S.; Cowley, J.; Wilken, J.M.; Resnik, L. Range of Motion Requirements for Upper-Limb Activities of Daily Living. Am. J. Occup. Ther. 2016, 70, 7001350010p1–7001350010p10. [Google Scholar] [CrossRef] [Green Version]
- Brumfield, R.H.; Champoux, J.A. A biomechanical study of normal functional wrist motion. Clin. Orthop. 1984, 187, 23–25. [Google Scholar] [CrossRef]
- Piscitelli, D.; Pellicciari, L. Responsiveness: Is it time to move beyond ordinal scores and approach interval measurements? Clin. Rehabil. 2018, 32, 1426–1427. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| EMGB Group (n = 8) | NMES Group (n = 8) | p Value | |
|---|---|---|---|
| Age, y | 52.75 ± 17.16 | 53.88 ± 10.70 | 0.877 |
| Sex, n (%) | |||
| Male | 5 (62.5) | 5 (62.5) | 1 |
| Female | 3 (37.5) | 3 (37.5) | |
| Stroke type, n (%) | |||
| Infarction | 4 (50.0) | 2 (0.25) | 0.608 |
| Hemorrhage | 4 (50.0) | 6 (0.75) | |
| Hemiplegia side | |||
| Left | 6 (0.75) | 5 (62.5) | 1 |
| Right | 2 (0.25) | 3 (37.5) | |
| Muscle tone | 0.38 ± 0.52 | 0.50 ± 0.53 | 0.642 |
| HAMD | 4.75 ± 6.82 | 5.50 ± 6.72 | 0.838 |
| Stroke onset, month | 1.38 ± 1.06 | 1.63 ± 1.06 | 0.645 |
| Baseline | Mean Difference between Groups (95%), p Value | 4w | Mean Difference between Groups (95%), p Value | Follow-up | Mean Difference between Groups (95%), p Value | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| EMGB | NMES | EMGB | NMES | EMGB | NMES | ||||||||
| N | 8 | 8 | 8 | 8 | 8 | 8 | |||||||
| Primary Outcome | AROM | 0.00 ± 0.00 | 0.00 ± 0.00 | 0.00 (0.00, 0.00) | 3.60 ± 5.70 | 6.92 ± 7.09 | −3.32 (−10.22, 3.58), 0.319 | 7.85 ± 8.98 | 7.70 ± 8.88 | 0.15 (−9.42, 9.73), 0.97 | |||
| mean change (95% CI) from baseline, p value | 3.60 (−1.28, 8.47), 0.136 | 6.92 (2.04, 11.80), 0.009 | 7.85 (1.08, 14.63), 0.026 | 7.70 (0.93, 14.47), 0.029 | |||||||||
| Secondary Outcomes | FMA-UE | 16.38 ± 10.14 | 18.63 ± 9.74 | −2.25 (−12.1, 8.41), 0.66 | 27.38 ± 9.77 | 28.00 ± 13.46 | −0.63 (−13.24, 11.99), 0.92 | 31.63 ± 12.03 | 29.75 ± 14.22 | 1.875 (−12.25, 16.00), 0.78 | |||
| mean change (95% CI) from baseline, p value | 11.00 (5.10, 16.0), 0.001 | 9.38 (3.47, 15.28), 0.004 | 15.25 (7.64, 22.86), 0.001 | 11.13 (3.51, 18.74), 0.007 | |||||||||
| extensor carpi radialis muscle | 0.00 ± 0.00 | 0.25 ± 0.46 | −0.25 (−0.60, 0.10), 0.149 | 1.00 ± 0.76 | 1.25 ± 1.04 | −0.25 (−1.22, 0.72), 0.590 | 1.50 ± 0.76 | 1.13 ± 0.83 | 0.38 (−0.48, 1.23), 0.362 | ||||
| mean change (95% CI) from baseline, p value | 1.00 (0.30, 1.70), 0.009 | 1.00 (0.30, 1.70), 0.009 | 1.50 (0.90, 2.10), 0.000 | 0.88 (0.27, 1.48), 0.008 | |||||||||
| extensor carpi ulnaris muscle | 0.00 ± 0.00 | 0.13 ± 0.35 | −0.13 (−0.39, 0.14), 0.334 | 0.63 ± 0.52 | 0.25 ± 0.71 | 0.38 (−0.29, 1.04), 0.246 | 0.63 ± 0.52 | 0.50 ± 0.76 | 0.13 (−0.57, 0.82), 0.705 | ||||
| mean change (95% CI) from baseline, p value | 0.63 (0.10–1.15), 0.023 | 0.13 (−0.40, 0.65), 0.619 | 0.63 (0.14, 1.11), 0.015 | 0.38 (−0.11, 0.86), 0.12 | |||||||||
| extensor digitorum communis muscle | 0.00 ± 0.00 | 0.00 ± 0.00 | 0.00 (0.00, 0.00) | 0.63 ± 0.92 | 0.38 ± 0.74 | 0.25 (−0.65, 1.15), 0.559 | 1.00 ± 0.93 | 0.50 ± 0.76 | 0.50 (−0.41, 1.41), 0.256 | ||||
| mean change (95% CI) from baseline, p value | 0.63 (−0.01, 1.26), 0.053 | 0.38 (−0.26, 1.01), 0.224 | 1.00 (0.36, 1.64), 0.005 | 0.50 (−0.14, 1.14), 0.116 | |||||||||
| BI | 49.38 ± 14.74 | 48.13 ± 21.37 | 1.25 (−18.44, 20.94), 0.894 | 64.38 ± 18.79 | 61.88 ± 18.89 | 2.50 (−17.70, 22.70), 0.795 | 75.63 ± 10.84 | 68.13 ± 13.08 | 7.50 (−5.38, 20.38), 0.232 | ||||
| mean change (95% CI) from baseline, p value | 15.00 (5.10, 24.90), 0.006 | 13.75 (3.85, 23.65), 0.01 | 26.25 (17.80, 34.70), 0.000 | 20.00 (11.55, 28.45), 0.000 | |||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, Q.; Jia, G.; Jia, L.; Wang, Y.; Jiang, W.; Feng, Y.; Jiang, H.; Yu, L.; Yu, J.; Tan, B. Effects of Electromyography Bridge on Upper Limb Motor Functions in Stroke Participants: An Exploratory Randomized Controlled Trial. Brain Sci. 2022, 12, 870. https://doi.org/10.3390/brainsci12070870
Zhao Q, Jia G, Jia L, Wang Y, Jiang W, Feng Y, Jiang H, Yu L, Yu J, Tan B. Effects of Electromyography Bridge on Upper Limb Motor Functions in Stroke Participants: An Exploratory Randomized Controlled Trial. Brain Sciences. 2022; 12(7):870. https://doi.org/10.3390/brainsci12070870
Chicago/Turabian StyleZhao, Qin, Gongwei Jia, Lang Jia, Yule Wang, Wei Jiang, Yali Feng, Hang Jiang, Lehua Yu, Jing Yu, and Botao Tan. 2022. "Effects of Electromyography Bridge on Upper Limb Motor Functions in Stroke Participants: An Exploratory Randomized Controlled Trial" Brain Sciences 12, no. 7: 870. https://doi.org/10.3390/brainsci12070870