
Can Early Neuromuscular Rehabilitation Protocol Improve Disability after a Hemiparetic Stroke? A Pilot Study


 and
and
Abstract
:1. Introduction
2. Materials and Methods
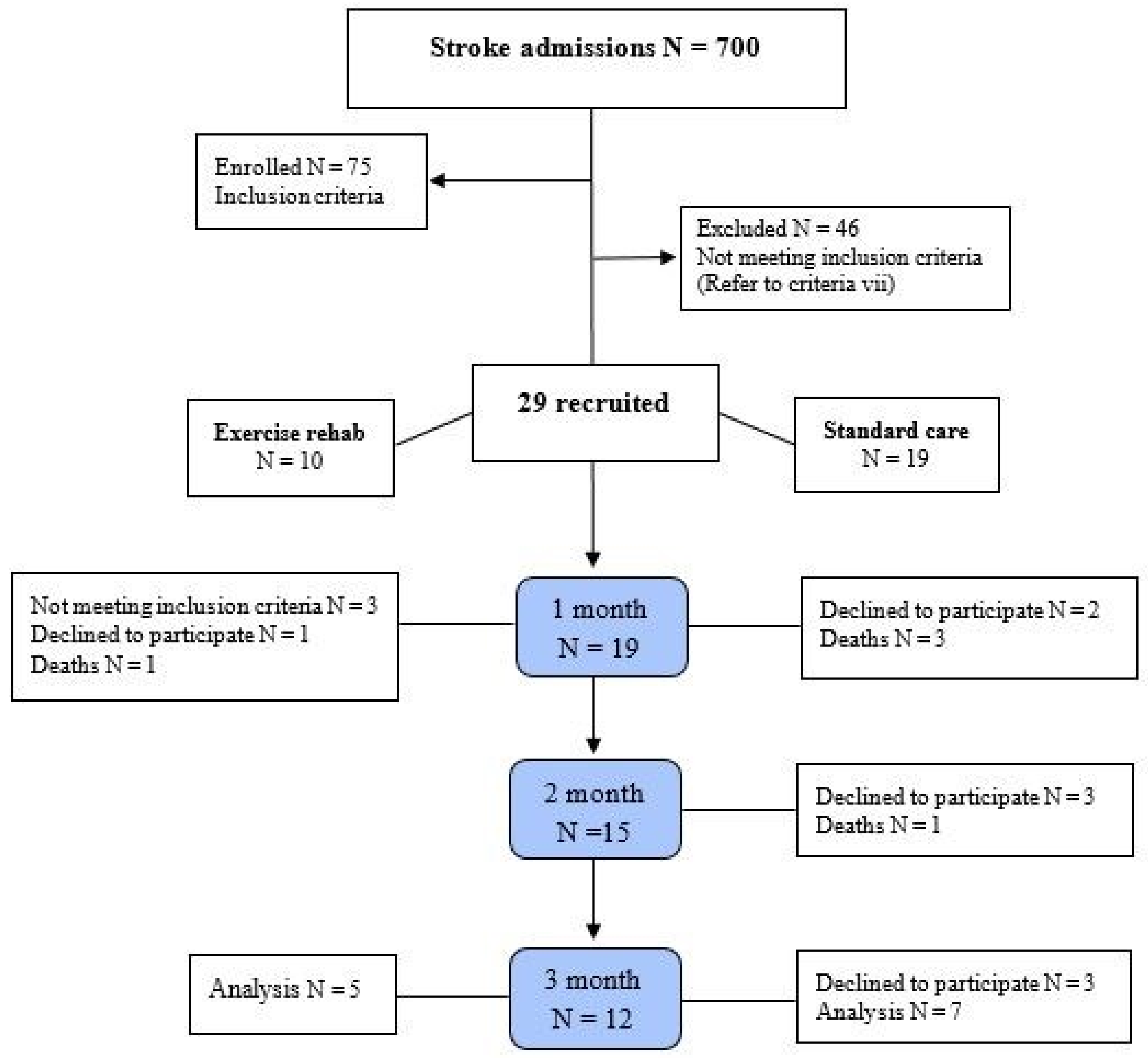
2.1. Participants
2.2. Sample Size
2.3. Patient Demographics
2.4. The Experimental Approach to the Problem
2.5. Neuromuscular Rehabilitation Protocol
2.6. Outcome Measures
2.7. Statistical Analysis
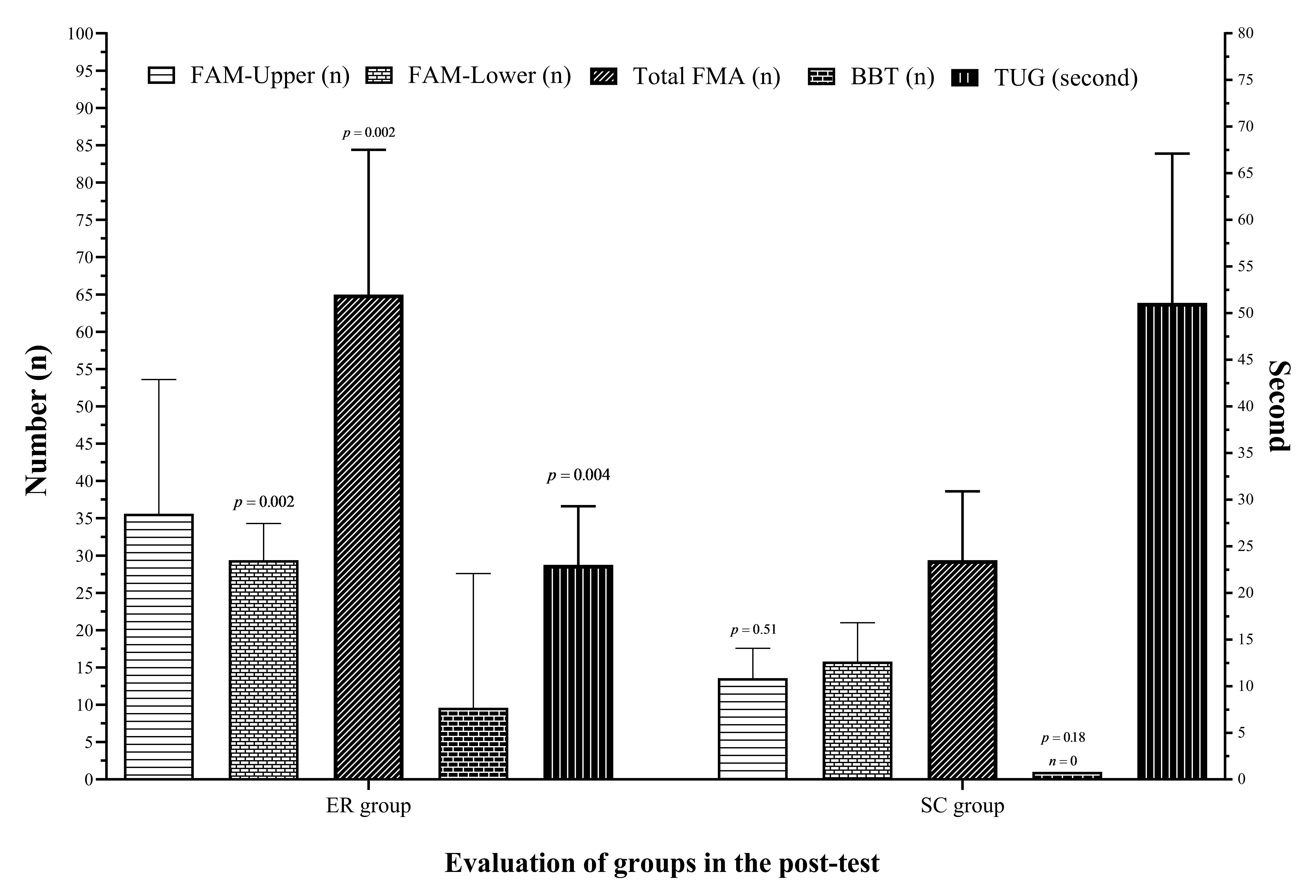
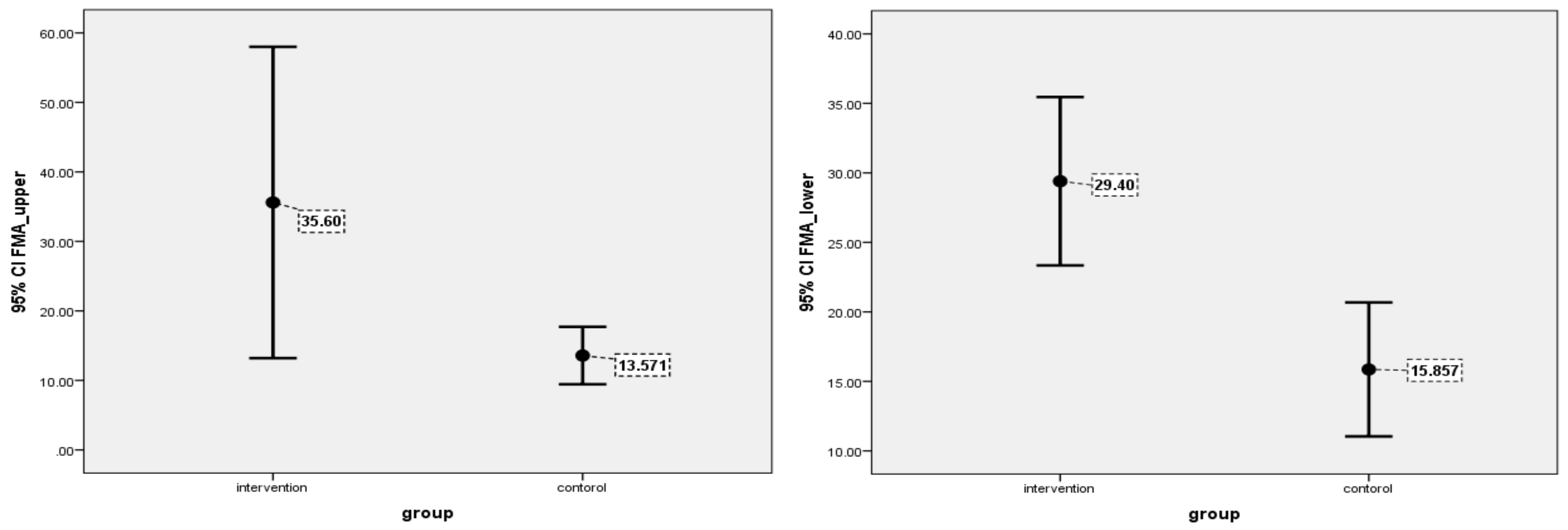
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Feigin, V.L.; Lawes, C.M.M.; Bennett, D.A.; Anderson, C.S. Stroke Epidemiology: A Review of Population-Based Studies of Incidence, Prevalence, and Case-Fatality in the Late 20th Century. Lancet Neurol. 2003, 2, 43–53. [Google Scholar] [CrossRef]
- Roger, V.L.; Go, A.S.; Lloyd-Jones, D.M.; Adams, R.J.; Berry, J.D.; Brown, T.M.; Carnethon, M.R.; Dai, S.; De Simone, G.; Ford, E.S. Heart Disease and Stroke Statistics—2011 Update: A Report from the American Heart Association. Circulation 2011, 123, e18–e209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, G.; Durstine, J.L.; Painter, P.; Medicine, A.C. Acsm’s Exercise Management for Persons with Chronic Diseases and Disabilities, 4th ed; Human Kinetics: Champaign, IL, USA, 2016; ISBN 1450434142. [Google Scholar]
- Bamford, J.; Dennis, M.; Sandercock, P.; Burn, J.; Warlow, C. The Frequency, Causes and Timing of Death within 30 Days of a First Stroke: The Oxfordshire Community Stroke Project. J. Neurol. Neurosurg. Psychiatry 1990, 53, 824–829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernhardt, J.; Dewey, H.; Thrift, A.; Collier, J.; Donnan, G. A Very Early Rehabilitation Trial for Stroke (AVERT) Phase II Safety and Feasibility. Stroke 2008, 39, 390–396. [Google Scholar] [CrossRef] [PubMed]
- Cumming, T.B.; Thrift, A.G.; Collier, J.M.; Churilov, L.; Dewey, H.M.; Donnan, G.A.; Bernhardt, J. Very Early Mobilization after Stroke Fast-Tracks Return to Walking: Further Results from the Phase II AVERT Randomized Controlled Trial. Stroke 2011, 42, 153–158. [Google Scholar] [CrossRef] [Green Version]
- Tay-Teo, K.; Moodie, M.; Bernhardt, J.; Thrift, A.G.; Collier, J.; Donnan, G.; Dewey, H. Economic Evaluation alongside a Phase II, Multi-Centre, Randomised Controlled Trial of Very Early Rehabilitation after Stroke (AVERT). Cerebrovasc. Dis. 2008, 26, 475–481. [Google Scholar] [CrossRef]
- Langhorne, P.; Ramachandra, S.; Collaboration, S.U.T. Organised Inpatient (Stroke Unit) Care for Stroke: Network Meta-analysis. Cochrane Database Syst. Rev. 2020. [Google Scholar] [CrossRef]
- Diserens, K.; Michel, P.; Bogousslavsky, J. Early Mobilisation after Stroke: Review of the Literature. Cerebrovasc. Dis. 2006, 22, 183–190. [Google Scholar] [CrossRef]
- Bayley, M.T.; Bowen, A.; English, C.; Teasell, R.; Eng, J.J. Where to Now? AVERT Answered an Important Question, but Raised Many More. Int. J. Stroke 2017, 12, 683–686. [Google Scholar] [CrossRef] [Green Version]
- Li, F.; Pendy Jr, J.T.; Ding, J.N.; Peng, C.; Li, X.; Shen, J.; Wang, S.; Geng, X. Exercise Rehabilitation Immediately Following Ischemic Stroke Exacerbates Inflammatory Injury. Neurol. Res. 2017, 39, 530–537. [Google Scholar] [CrossRef]
- Billinger, S.A.; Arena, R.; Bernhardt, J.; Eng, J.J.; Franklin, B.A.; Johnson, C.M.; MacKay-Lyons, M.; Macko, R.F.; Mead, G.E.; Roth, E.J. Physical Activity and Exercise Recommendations for Stroke Survivors: A Statement for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2014, 45, 2532–2553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rethnam, V.; Langhorne, P.; Churilov, L.; Hayward, K.S.; Herisson, F.; Poletto, S.R.; Tong, Y.; Bernhardt, J. Early Mobilisation Post-Stroke: A Systematic Review and Meta-Analysis of Individual Participant Data. Disabil. Rehabil. 2022, 44, 1156–1163. [Google Scholar] [CrossRef]
- Kramer, S.F.; Hung, S.H.; Brodtmann, A. The Impact of Physical Activity before and after Stroke on Stroke Risk and Recovery: A Narrative Review. Curr. Neurol. Neurosci. Rep. 2019, 19, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Stinear, C.M.; Lang, C.E.; Zeiler, S.; Byblow, W.D. Advances and Challenges in Stroke Rehabilitation. Lancet Neurol. 2020, 19, 348–360. [Google Scholar] [CrossRef]
- Dorsch, S.; Elkins, M.R. Repetitions and Dose in Stroke Rehabilitation. J. Physiother. 2020, 66, 211–212. [Google Scholar] [CrossRef] [PubMed]
- Yelnik, A.P.; Quintaine, V.; Andriantsifanetra, C.; Wannepain, M.; Reiner, P.; Marnef, H.; Evrard, M.; Meseguer, E.; Devailly, J.P.; Lozano, M. AMOBES (Active Mobility Very Early after Stroke) a Randomized Controlled Trial. Stroke 2017, 48, 400–405. [Google Scholar] [CrossRef]
- Regan, E.W.; Handlery, R.; Liuzzo, D.M.; Stewart, J.C.; Burke, A.R.; Hainline, G.M.; Horn, C.; Keown, J.T.; McManus, A.E.; Lawless, B.S. The Neurological Exercise Training (NExT) Program: A Pilot Study of a Community Exercise Program for Survivors of Stroke. Disabil. Health J. 2019, 12, 528–532. [Google Scholar] [CrossRef]
- Mathiowetz, V.; Volland, G.; Kashman, N.; Weber, K. Adult Norms for the Box and Block Test of Manual Dexterity. Am. J. Occup. Ther. 1985, 39, 386–391. [Google Scholar] [CrossRef] [Green Version]
- Sanford, J.; Moreland, J.; Swanson, L.R.; Stratford, P.W.; Gowland, C. Reliability of the Fugl-Meyer Assessment for Testing Motor Performance in Patients Following Stroke. Phys. Ther. 1993, 73, 447–454. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The Timed “Up & Go”: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Nobari, H.; Rezaei, S.; Sheikh, M.; Fuentes-García, J.P.; Pérez-Gómez, J. Effect of Virtual Reality Exercises on the Cognitive Status and Dual Motor Task Performance of the Aging Population. Int. J. Environ. Res. Public Health 2021, 18, 8005. [Google Scholar] [CrossRef] [PubMed]
- Hubbard, I.J.; Carey, L.M.; Budd, T.W.; Levi, C.; McElduff, P.; Hudson, S.; Bateman, G.; Parsons, M.W. A Randomized Controlled Trial of the Effect of Early Upper-Limb Training on Stroke Recovery and Brain Activation. Neurorehabil. Neural Repair 2015, 29, 703–713. [Google Scholar] [CrossRef] [PubMed]
- Masiero, S.; Armani, M.; Rosati, G. Upper-Limb Robot-Assisted Therapy in Rehabilitation of Acute Stroke Patients: Focused Review and Results of New Randomized Controlled Trial. J. Rehabil. Res. Dev. 2011, 48, 355–366. [Google Scholar] [CrossRef] [PubMed]
- Saposnik, G.; Cohen, L.G.; Mamdani, M.; Pooyania, S.; Ploughman, M.; Cheung, D.; Shaw, J.; Hall, J.; Nord, P.; Dukelow, S. Efficacy and Safety of Non-Immersive Virtual Reality Exercising in Stroke Rehabilitation (EVREST): A Randomised, Multicentre, Single-Blind, Controlled Trial. Lancet Neurol. 2016, 15, 1019–1027. [Google Scholar] [CrossRef] [Green Version]
- Bernhardt, J.; Langhorne, P.; Lindley, R.I.; Thrift, A.G.; Ellery, F.; Collier, J.; Churilov, L.; Moodie, M.; Dewey, H.; Donnan, G. Efficacy and Safety of Very Early Mobilisation within 24 h of Stroke Onset (AVERT): A Randomised Controlled Trial. Lancet 2015, 386, 46–55. [Google Scholar]
- Strømmen, A.M.; Christensen, T.; Jensen, K. Intensive Treadmill Training in the Acute Phase after Ischemic Stroke. Int. J. Rehabil. Res. 2016, 39, 145–152. [Google Scholar] [CrossRef]
- Sandberg, K.; Kleist, M.; Falk, L.; Enthoven, P. Effects of Twice-Weekly Intense Aerobic Exercise in Early Subacute Stroke: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2016, 97, 1244–1253. [Google Scholar] [CrossRef] [Green Version]
- Langhorne, P.; Wu, O.; Rodgers, H.; Ashburn, A.; Bernhardt, J. A Very Early Rehabilitation Trial after Stroke (AVERT): A Phase III, Multicentre, Randomised Controlled Trial. Health Technol. Assess. (Rockv). 2017. [Google Scholar] [CrossRef]
- Lee, S.-U.; Kim, D.-Y.; Park, S.-H.; Choi, D.-H.; Park, H.-W.; Han, T.R. Mild to Moderate Early Exercise Promotes Recovery from Cerebral Ischemia in Rats. Can. J. Neurol. Sci. 2009, 36, 443–449. [Google Scholar] [CrossRef] [Green Version]
- Biernaskie, J.; Chernenko, G.; Corbett, D. Efficacy of Rehabilitative Experience Declines with Time after Focal Ischemic Brain Injury. J. Neurosci. 2004, 24, 1245–1254. [Google Scholar] [CrossRef]
- Yang, L.; Zhang, J.; Deng, Y.; Zhang, P. The Effects of Early Exercise on Motor, Sense, and Memory Recovery in Rats with Stroke. Am. J. Phys. Med. Rehabil. 2017, 96, e36–e43. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Wang, P.P.; Meng, P.P.; Han, C.; Yue, S.W. Intensive Training Accelerates the Recovery of Motor Functions Following Cerebral Ischemia-Reperfusion in MCAO Rats. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 3839–3852. [Google Scholar] [PubMed]
- Li, Z.; Zhang, X.; Wang, K.; Wen, J. Effects of Early Mobilization after Acute Stroke: A Meta-Analysis of Randomized Control Trials. J. Stroke Cerebrovasc. Dis. 2018, 27, 1326–1337. [Google Scholar] [CrossRef] [PubMed]
- Imura, T.; Nagasawa, Y.; Fukuyama, H.; Imada, N.; Oki, S.; Araki, O. Effect of Early and Intensive Rehabilitation in Acute Stroke Patients: Retrospective Pre-/Post-Comparison in Japanese Hospital. Disabil. Rehabil. 2018, 40, 1452–1455. [Google Scholar] [CrossRef]
- Moore, J.L.; Nordvik, J.E.; Erichsen, A.; Rosseland, I.; Bø, E.; Hornby, T.G.; Team, F.-O. Implementation of High-Intensity Stepping Training during Inpatient Stroke Rehabilitation Improves Functional Outcomes. Stroke 2020, 51, 563–570. [Google Scholar] [CrossRef]
- Di Lauro, A.; Pellegrino, L.; Savastano, G.; Ferraro, C.; Fusco, M.; Balzarano, F.; Franco, M.M.; Biancardi, L.G.; Grasso, A. A Randomized Trial on the Efficacy of Intensive Rehabilitation in the Acute Phase of Ischemic Stroke. J. Neurol. 2003, 250, 1206–1208. [Google Scholar] [CrossRef]
- Dromerick, A.W.; Lang, C.E.; Birkenmeier, R.L.; Wagner, J.M.; Miller, J.P.; Videen, T.O.; Powers, W.J.; Wolf, S.L.; Edwards, D.F. Very Early Constraint-Induced Movement during Stroke Rehabilitation (VECTORS): A Single-Center RCT. Neurology 2009, 73, 195–201. [Google Scholar] [CrossRef] [Green Version]
- Bernhardt, J.; Churilov, L.; Ellery, F.; Collier, J.; Chamberlain, J.; Langhorne, P.; Lindley, R.I.; Moodie, M.; Dewey, H.; Thrift, A.G. Prespecified Dose-Response Analysis for a Very Early Rehabilitation Trial (AVERT). Neurology 2016, 86, 2138–2145. [Google Scholar] [CrossRef] [Green Version]
- Egan, K.J.; Janssen, H.; Sena, E.S.; Longley, L.; Speare, S.; Howells, D.W.; Spratt, N.J.; Macleod, M.R.; Mead, G.E.; Bernhardt, J. Exercise Reduces Infarct Volume and Facilitates Neurobehavioral Recovery: Results from a Systematic Review and Meta-Analysis of Exercise in Experimental Models of Focal Ischemia. Neurorehabil. Neural Repair 2014, 28, 800–812. [Google Scholar] [CrossRef]
- Deplanque, D.; Masse, I.; Libersa, C.; Leys, D.; Bordet, R. Previous Leisure-Time Physical Activity Dose Dependently Decreases Ischemic Stroke Severity. Stroke Res. Treat. 2012, 2012. [Google Scholar] [CrossRef] [Green Version]
- Willey, J.Z.; Moon, Y.P.; Paik, M.C.; Boden-Albala, B.; Sacco, R.L.; Elkind, M.S. V Physical Activity and Risk of Ischemic Stroke in the Northern Manhattan Study. Neurology 2009, 73, 1774–1779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, E.J.; Lannin, N.A.; Ada, L.; Schmidt, J. Increasing the Amount of Usual Rehabilitation Improves Activity after Stroke: A Systematic Review. J. Physiother. 2016, 62, 182–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- James, J.; McGlinchey, M.P. How Active Are Stroke Patients in Physiotherapy Sessions and Is This Associated with Stroke Severity? Disabil. Rehabil. 2021, 1, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Aguilera-Rubio, Á.; Cuesta-Gómez, A.; Mallo-López, A.; Jardón-Huete, A.; Oña-Simbaña, E.D.; Alguacil-Diego, I.M. Feasibility and Efficacy of a Virtual Reality Game-Based Upper Extremity Motor Function Rehabilitation Therapy in Patients with Chronic Stroke: A Pilot Study. Int. J. Environ. Res. Public Health 2022, 19, 3381. [Google Scholar] [CrossRef]
- Kluding, P.M.; Tseng, B.Y.; Billinger, S.A. Exercise and Executive Function in Individuals with Chronic Stroke: A Pilot Study. J. Neurol. Phys. Ther. JNPT 2011, 35, 11. [Google Scholar] [CrossRef]
- Xing, Y.; Yang, S.-D.; Dong, F.; Wang, M.-M.; Feng, Y.-S.; Zhang, F. The Beneficial Role of Early Exercise Training Following Stroke and Possible Mechanisms. Life Sci. 2018, 198, 32–37. [Google Scholar] [CrossRef]
- Tanaka, H.; Kitamura, G.; Nankaku, M.; Taniguchi, M.; Shide, K.; Fujita, M.; Ida, M.; Oshima, S.; Kikuchi, T.; Maki, T. Association of Physical Activity and Nutritional Intake with Muscle Quantity and Quality Changes in Acute Stroke Patients. J. Stroke Cerebrovasc. Dis. 2022, 31, 106442. [Google Scholar] [CrossRef]
- Dromerick, A.W.; Geed, S.; Barth, J.; Brady, K.; Giannetti, M.L.; Mitchell, A.; Edwardson, M.A.; Tan, M.T.; Zhou, Y.; Newport, E.L. Critical Period After Stroke Study (CPASS): A Phase II Clinical Trial Testing an Optimal Time for Motor Recovery after Stroke in Humans. Proc. Natl. Acad. Sci. USA 2021, 118, e2026676118. [Google Scholar] [CrossRef]
- Bernhardt, J.; Hayward, K.S.; Kwakkel, G.; Ward, N.S.; Wolf, S.L.; Borschmann, K.; Krakauer, J.W.; Boyd, L.A.; Carmichael, S.T.; Corbett, D. Agreed Definitions and a Shared Vision for New Standards in Stroke Recovery Research: The Stroke Recovery and Rehabilitation Roundtable Taskforce. Int. J. Stroke 2017, 12, 444–450. [Google Scholar] [CrossRef]
- Amorós-Aguilar, L.; Rodríguez-Quiroga, E.; Sánchez-Santolaya, S.; Coll-Andreu, M. Effects of Combined Interventions with Aerobic Physical Exercise and Cognitive Training on Cognitive Function in Stroke Patients: A Systematic Review. Brain Sci. 2021, 11, 473. [Google Scholar] [CrossRef]
- Suzuki, K.; Tominaga, T.; Ruhee, R.T.; Ma, S. Characterization and Modulation of Systemic Inflammatory Response to Exhaustive Exercise in Relation to Oxidative Stress. Antioxidants 2020, 9, 401. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Role | Group | Sex | ge | Lesion Location | NIHSS | MRS | LS | TTS |
|---|---|---|---|---|---|---|---|---|
| 1 | ER | Female | 36 | Frontoparietal + basal ganglia | 12 | 4 | left | 72 |
| 2 | ER | Male | 81 | Pons + medulla | 10 | 4 | Right | 48 |
| 3 | ER | Male | 83 | basal ganglia | 9 | 4 | Right | 24 |
| 4 | ER | Male | 67 | Frontoparietal + basal ganglia | 16 | 5 | left | 48 |
| 5 | ER | Male | 53 | Basal ganglia + temporal cortex | 11 | 5 | left | 24 |
| 6 | SC | Male | 42 | Tempofrontal+ basal ganglia | 16 | 5 | left | 24 |
| 7 | SC | Male | 53 | Basal ganglia | 13 | 4 | Right | 48 |
| 8 | SC | Female | 51 | Frontoparietal + basal ganglia | 13 | 5 | left | 72 |
| 9 | SC | Female | 40 | Frontopariental + basal ganglia | 17 | 5 | Right | 24 |
| 10 | SC | Male | 57 | Basal ganglia | 17 | 5 | left | 72 |
| 11 | SC | Male | 48 | basal ganglia | 16 | 5 | left | 24 |
| 12 | SC | Male | 41 | Basal ganglia | 9 | 4 | left | 48 |
| Mode of Exercise | Major Goals | Intensity/Frequency/Duration |
|---|---|---|
| Flexibility Stretching (ROM upper & lower limb) | • Increase ROM of involved extremities • Prevent contractures | • 6 d/wk • ROM stretch for 10 minutes |
| Strength • Circuit training • Weight machines • Free weights • TheraBand • Isometric exercise Aerobic exercise (15–30 min) | Increase independence in ADLs | • 2 sets of 15–30 repetitions of 8–14 exercises • RPE: 11–20 (6–20 scale) involving the major muscle groups • heart rate: under maximum, 220-age • 6 d/wk |
| Neuromuscular Coordination and balance activities • Use everything they can take and practice with | • Improve level of safety during ADLs | 6 d/wk |
| Role | Groups | FAM Upper (n) | FAM Lower (n) | TUG (s) | BBT (n) | ||||
|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | ||
| 1 | ER | 3 | 18 | 5 | 34 | 0 | 14.35 | 0 | 0 |
| 2 | ER | 4 | 31 | 6 | 26 | 0 | 29.57 | 0 | 0 |
| 3 | ER | 29 | 64 | 5 | 30 | 0 | 25.76 | 0 | 42 |
| 4 | ER | 0 | 24 | 4 | 23 | 0 | 26.77 | 0 | 0 |
| 5 | ER | 2 | 41 | 10 | 34 | 0 | 18.61 | 0 | 6 |
| 6 | SC | 0 | 8 | 2 | 10 | 0 | 60 * | 0 | 0 |
| 7 | SC | 2 | 14 | 4 | 15 | 0 | 60 * | 0 | 0 |
| 8 | SC | 2 | 11 | 2 | 16 | 0 | 60 * | 0 | 0 |
| 9 | SC | 2 | 16 | 3 | 18 | 0 | 37.46 | 0 | 0 |
| 10 | SC | 0 | 12 | 2 | 9 | 0 | 60 * | 0 | 0 |
| 11 | SC | 0 | 12 | 0 | 19 | 0 | 60 * | 0 | 0 |
| 12 | SC | 0 | 22 | 0 | 24 | 0 | 20.24 | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yazdani, M.; Chitsaz, A.; Zolaktaf, V.; Saadatnia, M.; Ghasemi, M.; Nazari, F.; Chitsaz, A.; Suzuki, K.; Nobari, H. Can Early Neuromuscular Rehabilitation Protocol Improve Disability after a Hemiparetic Stroke? A Pilot Study. Brain Sci. 2022, 12, 816. https://doi.org/10.3390/brainsci12070816
Yazdani M, Chitsaz A, Zolaktaf V, Saadatnia M, Ghasemi M, Nazari F, Chitsaz A, Suzuki K, Nobari H. Can Early Neuromuscular Rehabilitation Protocol Improve Disability after a Hemiparetic Stroke? A Pilot Study. Brain Sciences. 2022; 12(7):816. https://doi.org/10.3390/brainsci12070816
Chicago/Turabian StyleYazdani, Mahdi, Ahmad Chitsaz, Vahid Zolaktaf, Mohammad Saadatnia, Majid Ghasemi, Fatemeh Nazari, Abbas Chitsaz, Katsuhiko Suzuki, and Hadi Nobari. 2022. "Can Early Neuromuscular Rehabilitation Protocol Improve Disability after a Hemiparetic Stroke? A Pilot Study" Brain Sciences 12, no. 7: 816. https://doi.org/10.3390/brainsci12070816