
Single-Cell RNA Sequencing of Cerebrospinal Fluid as an Advanced Form of Liquid Biopsy for Neurological Disorders

 , ,
, ,
Abstract
:1. Introduction
2. CSF as a Repertoire of Biomarkers in Diseases of the CNS
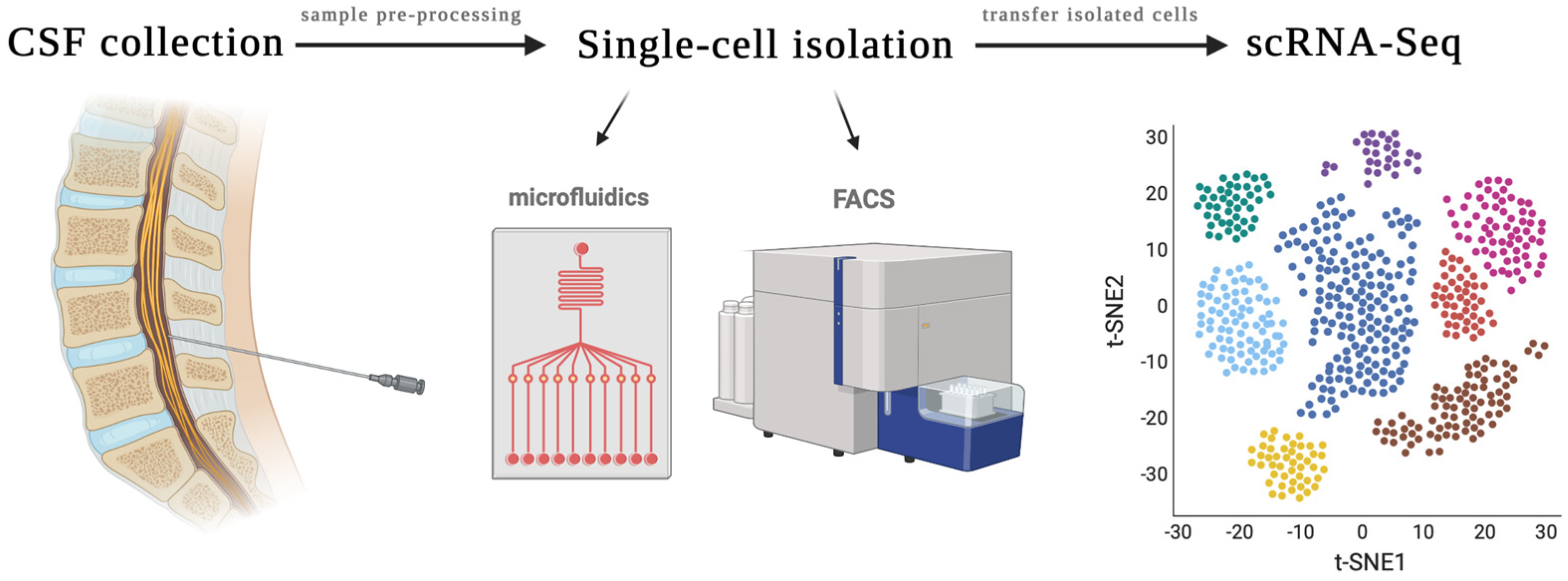
3. Single-Cell Sequencing of CSF
3.1. Sample Pre-Processing
3.2. Single-Cell Isolation Techniques
3.3. Library Preparation, Sequencing and Computational Analysis
4. Single-Cell RNA Sequencing of the CSF in Neuro-Oncology
4.1. CTC scRNA-Seq to Understand Tumor Heterogeneity, Disease Progression and Metastasis
4.2. CTC scRNA-Seq to Diagnose the Origin of Carcinoma of Unknown Primary
4.3. scRNA-Seq to Study the Immune Microenvironment and Metabolic Adaptations of Tumor Cells
4.4. Predicting Responses to Targeted Therapies
4.5. Combined Analysis of CTCs and Other Liquid Biopsy Components
5. Single-Cell RNA Sequencing in CNS Disease of Non-Oncological Etiology
5.1. Alzheimer’s Disease
5.2. Neurological Sequelae of COVID-19
5.3. Multiple Sclerosis
5.4. HIV-Associated Neuronal Injury
5.5. Meningitis
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shankar, G.M.; Balaj, L.; Stott, S.L.; Nahed, B.; Carter, B.S. Liquid biopsy for brain tumors. Expert Rev. Mol. Diagn. 2017, 17, 943–947. [Google Scholar] [CrossRef] [PubMed]
- Spector, R.; Robert Snodgrass, S.; Johanson, C.E. A balanced view of the cerebrospinal fluid composition and functions: Focus on adult humans. Exp. Neurol. 2015, 273, 57–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wick, M.; Gross, C.C.; Isenmann, S.; Strik, H. Cytology of cerebrospinal fluid: Standards, importance and modern methods. Nervenarzt 2016, 87, 1276–1281. [Google Scholar] [CrossRef] [PubMed]
- de Graaf, M.T.; Smitt, P.A.S.; Luitwieler, R.L.; van Velzen, C.; van den Broek, P.D.; Kraan, J.; Gratama, J.W. Central memory CD4+ T cells dominate the normal cerebrospinal fluid. Cytom. B Clin. Cytom. 2011, 80, 43–50. [Google Scholar] [CrossRef]
- Ransohoff, R.M.; Engelhardt, B. The anatomical and cellular basis of immune surveillance in the central nervous system. Nat. Rev. Immunol. 2012, 12, 623–635. [Google Scholar] [CrossRef]
- Papadopoulos, Z.; Herz, J.; Kipnis, J. Meningeal Lymphatics: From Anatomy to Central Nervous System Immune Surveillance. J. Immunol. 2020, 204, 286–293. [Google Scholar] [CrossRef]
- Gorchynski, J.; Oman, J.; Newton, T. Interpretation of traumatic lumbar punctures in the setting of possible subarachnoid hemorrhage: Who can be safely discharged? Cal. J. Emerg. Med. 2007, 8, 3–7. [Google Scholar]
- Hrishi, A.P.; Sethuraman, M. Cerebrospinal Fluid (CSF) Analysis and Interpretation in Neurocritical Care for Acute Neurological Conditions. Indian J. Crit. Care Med. 2019, 23, 115–119. [Google Scholar] [CrossRef]
- Edwards, C.; Leira, E.C.; Gonzalez-Alegre, P. Residency training: A failed lumbar puncture is more about obesity than lack of ability. Neurology 2015, 84, e69–e72. [Google Scholar] [CrossRef] [Green Version]
- Otto, F.; Harrer, C.; Pilz, G.; Wipfler, P.; Harrer, A. Role and Relevance of Cerebrospinal Fluid Cells in Diagnostics and Research: State-of-the-Art and Underutilized Opportunities. Diagnostics 2021, 12, 79. [Google Scholar] [CrossRef]
- Ruan, H.; Zhou, Y.; Shen, J.; Zhai, Y.; Xu, Y.; Pi, L.; Huang, R.; Chen, K.; Li, X.; Ma, W.; et al. Circulating tumor cell characterization of lung cancer brain metastases in the cerebrospinal fluid through single-cell transcriptome analysis. Clin. Transl. Med. 2020, 10, e246. [Google Scholar] [CrossRef] [PubMed]
- Soffietti, R.; Bettegowda, C.; Mellinghoff, I.K.; Warren, K.E.; Ahluwalia, M.S.; De Groot, J.F.; Galanis, E.; Gilbert, M.R.; Jaeckle, K.A.; Le Rhun, E.; et al. Liquid biopsy in gliomas: A RANO review and proposals for clinical applications. Neuro-Oncology 2022, 24, 855–871. [Google Scholar] [CrossRef] [PubMed]
- Mattox, A.K.; Yang, B.; Douville, C.; Lo, S.-F.; Sciubba, D.; Wolinsky, J.P.; Gokaslan, Z.L.; Robison, J.; Blair, C.; Jiao, Y.; et al. The mutational landscape of spinal chordomas and their sensitive detection using circulating tumor DNA. Neurooncol. Adv. 2020, 3, vdaa173. [Google Scholar] [CrossRef] [PubMed]
- Muralidharan, K.; Yekula, A.; Small, J.L.; Rosh, Z.S.; Kang, K.M.; Wang, L.; Lau, S.; Zhang, H.; Lee, H.; Bettegowda, C.; et al. TERT promoter mutation analysis for blood-based diagnosis and monitoring of gliomas. Clin. Cancer Res. 2021, 27, 169–178. [Google Scholar] [CrossRef]
- Azad, T.D.; Jin, M.C.; Bernhardt, L.J.; Bettegowda, C. Liquid biopsy for pediatric diffuse midline glioma: A review of circulating tumor DNA and cerebrospinal fluid tumor DNA. Neurosurg. Focus 2020, 48, E9. [Google Scholar] [CrossRef] [Green Version]
- Mattox, A.K.; Yan, H.; Bettegowda, C. The potential of cerebrospinal fluid-based liquid biopsy approaches in CNS tumors. Neuro-Oncology 2019, 21, 1509–1518. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J.D.; Li, L.; Wang, Y.; Thoburn, C.; Afsari, B.; Danilova, L.; Douville, C.; Javed, A.A.; Wong, F.; Mattox, A.; et al. Detection and localization of surgically resectable cancers with a multi-analyte blood test. Science 2018, 359, 926–930. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Bettegowda, C. Applications of DNA-Based Liquid Biopsy for Central Nervous System Neoplasms. J. Mol. Diagn. 2016, 19, 24–34. [Google Scholar] [CrossRef] [Green Version]
- Bettegowda, C.; Sausen, M.; Leary, R.; Kinde, I.; Agrawal, N.; Bartlett, B.; Wang, H.; Luber, B.; Kinzler, K.; Vogelstein, B.; et al. Detection of Circulating Tumor DNA in Early and Late Stage Human Malignancies. Neuro-Oncology 2014, 16, iii7. [Google Scholar] [CrossRef]
- Shalek, A.K.; Satija, R.; Shuga, J.; Trombetta, J.J.; Gennert, D.; Lu, D.; Chen, P.; Gertner, R.S.; Gaublomme, J.T.; Yosef, N.; et al. Single-cell RNA-seq reveals dynamic paracrine control of cellular variation. Nature 2014, 510, 363–369. [Google Scholar] [CrossRef] [Green Version]
- Eberwine, J.; Yeh, H.; Miyashiro, K.; Cao, Y.; Nair, S.; Zettel, M.; Finnell, R.; Coleman, P. Analysis of gene expression in single live neurons. Proc. Natl. Acad. Sci. USA 1992, 89, 3010–3014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, B.; Lee, J.H.; Bang, D. Author Correction: Single-cell RNA sequencing technologies and bioinformatics pipelines. Exp. Mol. Med. 2021, 53, 1005. [Google Scholar] [CrossRef] [PubMed]
- Yekula, A.; Muralidharan, K.; Rosh, Z.S.; Youngkin, A.E.; Kang, K.M.; Balaj, L.; Carter, B.S. Liquid Biopsy Strategies to Distinguish Progression from Pseudoprogression and Radiation Necrosis in Glioblastomas. Adv. Biosyst. 2020, 4, e2000029. [Google Scholar] [CrossRef] [PubMed]
- Yekula, A.; Muralidharan, K.; Kang, K.M.; Wang, L.; Balaj, L.; Carter, B.S. From laboratory to clinic: Translation of extracellular vesicle based cancer biomarkers. Methods 2020, 177, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Teunissen, C.E.; Petzold, A.; Bennett, J.L.; Berven, F.S.; Brundin, L.; Comabella, M.; Franciotta, D.; Frederiksen, J.L.; Fleming, J.O.; Furlan, R.; et al. A consensus protocol for the standardization of cerebrospinal fluid collection and biobanking. Neurology 2009, 73, 1914–1922. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tung, P.-Y.; Blischak, J.D.; Hsiao, C.J.; Knowles, D.A.; Burnett, J.E.; Pritchard, J.K.; Gilad, Y. Batch effects and the effective design of single-cell gene expression studies. Sci. Rep. 2017, 7, 39921. [Google Scholar] [CrossRef] [Green Version]
- Guo, F.; Li, L.; Li, J.; Wu, X.; Hu, B.; Zhu, P.; Wen, L.; Tang, F. Single-cell multi-omics sequencing of mouse early embryos and embryonic stem cells. Cell Res. 2017, 27, 967–988. [Google Scholar] [CrossRef]
- Habli, Z.; AlChamaa, W.; Saab, R.; Kadara, H.; Khraiche, M.L. Circulating Tumor Cell Detection Technologies and Clinical Utility: Challenges and Opportunities. Cancers 2020, 12, 1930. [Google Scholar] [CrossRef]
- Julius, M.H.; Masuda, T.; Herzenberg, L.A. Demonstration that antigen-binding cells are precursors of antibody-producing cells after purification with a fluorescence-activated cell sorter. Proc. Natl. Acad. Sci. USA 1972, 69, 1934–1938. [Google Scholar] [CrossRef] [Green Version]
- Whitesides, G.M. The origins and the future of microfluidics. Nature 2006, 442, 368–373. [Google Scholar] [CrossRef]
- Swennenhuis, J.F.; van Dalum, G.; Zeune, L.L.; Terstappen, L.W.M.M. Improving the CellSearch® system. Expert Rev. Mol. Diagn. 2016, 16, 1291–1305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milojkovic Kerklaan, B.; Pluim, D.; Bol, M.; Hofland, I.; Westerga, J.; van Tinteren, H.; Beijnen, J.H.; Boogerd, W.; Schellens, J.H.M.; Brandsma, D. EpCAM-based flow cytometry in cerebrospinal fluid greatly improves diagnostic accuracy of leptomeningeal metastases from epithelial tumors. Neuro-Oncology 2016, 18, 855–862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Bussel, M.T.; Pluim, D.; Kerklaan, B.M.; Bol, M.; Sikorska, K.; Linders, D.T.; van den Broek, D.; Beijnen, J.H.; Jan, H.M.; Schellens, J.H.M.; et al. Circulating epithelial tumor cell analysis in CSF in patients with leptomeningeal metastases. Neurology 2020, 94, e521–e528. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Fleisher, M.; Rosenblum, M.; Lin, O.; Boire, A.; Briggs, S.; Bensman, Y.; Hurtado, B.; Shagabayeva, L.; De Angelis, L.M.; et al. Cerebrospinal fluid circulating tumor cells: A novel tool to diagnose leptomeningeal metastases from epithelial tumors. Neuro-Oncology 2017, 19, 1248–1254. [Google Scholar] [CrossRef]
- Su, S.; Li, X. Dive into Single, Seek Out Multiple: Probing Cancer Metastases via Single-Cell Sequencing and Imaging Techniques. Cancers 2021, 13, 1067. [Google Scholar] [CrossRef]
- Sullivan, J.P.; Nahed, B.V.; Madden, M.W.; Oliveira, S.M.; Springer, S.; Bhere, D.; Chi, A.S.; Wakimoto, H.; Rothenberg, S.M.; Sequist, L.V.; et al. Brain tumor cells in circulation are enriched for mesenchymal gene expression. Cancer Discov. 2014, 4, 1299–1309. [Google Scholar] [CrossRef] [Green Version]
- Müller, C.; Holtschmidt, J.; Auer, M.; Heitzer, E.; Lamszus, K.; Schulte, A.; Matschke, J.; Langer-Freitag, S.; Gasch, C.; Stoupiec, M.; et al. Hematogenous dissemination of glioblastoma multiforme. Sci. Transl. Med. 2014, 6, 247ra101. [Google Scholar] [CrossRef]
- Krol, I.; Castro-Giner, F.; Maurer, M.; Gkountela, S.; Szczerba, B.M.; Scherrer, R.; Coleman, N.; Carreira, S.; Bachmann, F.; Anderson, S.; et al. Detection of circulating tumour cell clusters in human glioblastoma. Br. J. Cancer 2018, 119, 487–491. [Google Scholar] [CrossRef] [Green Version]
- MacArthur, K.M.; Kao, G.D.; Chandrasekaran, S.; Alonso-Basanta, M.; Chapman, C.; Lustig, R.A.; Wileyto, E.P.; Hahn, S.M.; Dorsey, J.F. Detection of brain tumor cells in the peripheral blood by a telomerase promoter-based assay. Cancer Res. 2014, 74, 2152–2159. [Google Scholar] [CrossRef] [Green Version]
- Seo, Y.J.; Cho, W.H.; Kang, D.W.; Cha, S.H. Extraneural metastasis of glioblastoma multiforme presenting as an unusual neck mass. J. Korean Neurosurg. Soc. 2012, 51, 147–150. [Google Scholar] [CrossRef]
- Smalley, I.; Chen, Z.; Phadke, M.S.; Li, J.; Yu, X.; Wyatt, C.; Evernden, B.; Messina, J.L.; Sarnaik, A.; Sondak, V.K.; et al. Single-Cell Characterization of the Immune Microenvironment of Melanoma Brain and Leptomeningeal Metastases. Clin. Cancer Res. 2021, 27, 4109–4125. [Google Scholar] [CrossRef] [PubMed]
- Chi, Y.; Remsik, J.; Kiseliovas, V.; Derderian, C.; Sener, U.; Alghader, M.; Saadeh, F.; Nikishina, K.; Bale, T.; Iacobuzio-Donahue, C.; et al. Cancer cells deploy lipocalin-2 to collect limiting iron in leptomeningeal metastasis. Science 2020, 369, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Ruan, H.; Wang, Z.; Zhai, Y.; Xu, Y.; Pi, L.; Zheng, J.; Zhou, Y.; Zhang, C.; Huang, R.; Chen, K.; et al. Single-cell transcriptome analysis of diffuse large B cells in cerebrospinal fluid of central nervous system lymphoma. iScience 2021, 24, 102972. [Google Scholar] [CrossRef]
- Mochizuki, A.; Ramakrishna, S.; Good, Z.; Patel, S.; Chinnasamy, H.; Yeom, K.; Schultz, L.; Richards, R.; Campen, C.; Reschke, A.; et al. Omic-11. Single cell RNA sequencing from the csf of subjects with h3k27m+ dipg/dmg treated with gd2 car t-cellular therapy. Neuro-Oncology 2021, 23, i39. [Google Scholar] [CrossRef]
- Prakadan, S.M.; Alvarez-Breckenridge, C.A.; Markson, S.C.; Kim, A.E.; Klein, R.H.; Nayyar, N.; Navia, A.W.; Kuter, B.M.; Kolb, K.E.; Bihun, I.; et al. Genomic and transcriptomic correlates of immunotherapy response within the tumor microenvironment of leptomeningeal metastases. Nat. Commun. 2021, 12, 5955. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Perez, C.; Planas-Rigol, E.; Trincado, J.L.; Bonfill-Teixidor, E.; Arias, A.; Marchese, D.; Moutinho, C.; Serna, G.; Pedrosa, L.; Iurlaro, R.; et al. Immune cell profiling of the cerebrospinal fluid enables the characterization of the brain metastasis microenvironment. Nat. Commun. 2021, 12, 1–10. [Google Scholar] [CrossRef]
- Yekula, A.; Yekula, A.; Muralidharan, K.; Kang, K.; Carter, B.S.; Balaj, L. Extracellular Vesicles in Glioblastoma Tumor Microenvironment. Front. Immunol. 2020, 10, 3137. [Google Scholar] [CrossRef]
- Li, Y.; Polyak, D.; Lamsam, L.; Connolly, I.D.; Johnson, E.; Khoeur, L.K.; Andersen, S.; Granucci, M.; Stanley, G.; Liu, B.; et al. Comprehensive RNA analysis of CSF reveals a role for CEACAM6 in lung cancer leptomeningeal metastases. NPJ Precis. Oncol. 2021, 5, 90. [Google Scholar] [CrossRef]
- Gate, D.; Saligrama, N.; Leventhal, O.; Yang, A.C.; Unger, M.S.; Middeldorp, J.; Chen, K.; Lehallier, B.; Channappa, D.; De Los Santos, M.B.; et al. Clonally expanded CD8 T cells patrol the cerebrospinal fluid in Alzheimer’s disease. Nature 2020, 577, 399–404. [Google Scholar] [CrossRef]
- Blennow, K.; Zetterberg, H. Biomarkers for Alzheimer’s disease: Current status and prospects for the future. J. Intern. Med. 2018, 284, 643–663. [Google Scholar] [CrossRef] [Green Version]
- Song, E.; Bartley, C.M.; Chow, R.D.; Ngo, T.T.; Jiang, R.; Zamecnik, C.R.; Dandekar, R.; Loudermilk, R.P.; Dai, Y.; Liu, F.; et al. Divergent and self-reactive immune responses in the CNS of COVID-19 patients with neurological symptoms. Cell Rep. Med. 2021, 2, 100288. [Google Scholar] [CrossRef] [PubMed]
- Ramesh, A.; Schubert, R.D.; Greenfield, A.L.; Dandekar, R.; Loudermilk, R.; Sabatino, J.J., Jr.; Koelzer, M.T.; Tran, E.B.; Koshal, K.; Kim, K.; et al. A pathogenic and clonally expanded B cell transcriptome in active multiple sclerosis. Proc. Natl. Acad. Sci. USA 2020, 117, 22932–22943. [Google Scholar] [CrossRef] [PubMed]
- Esaulova, E.; Cantoni, C.; Shchukina, I.; Zaitsev, K.; Bucelli, R.C.; Wu, G.F.; Artyomov, M.N.; Cross, A.H.; Edelson, B.T. Single-cell RNA-seq analysis of human CSF microglia and myeloid cells in neuroinflammation. Neurol. Neuroimmunol. Neuroinflamm. 2020, 7, e732. [Google Scholar] [CrossRef] [PubMed]
- Beltrán, E.; Gerdes, L.A.; Hansen, J.; Flierl-Hecht, A.; Krebs, S.; Blum, H.; Ertl-Wagner, B.; Barkhof, F.; Kümpfel, T.; Hohlfeld, R.; et al. Early adaptive immune activation detected in monozygotic twins with prodromal multiple sclerosis. J. Clin. Investig. 2019, 129, 4758–4768. [Google Scholar] [CrossRef]
- Farhadian, S.F.; Mehta, S.; Zografou, C.; Robertson, K.; Price, R.W.; Pappalardo, J.; Chiarella, J.; Hafler, D.A.; Spudich, S.S. Single-cell RNA sequencing reveals microglia-like cells in cerebrospinal fluid during virologically suppressed HIV. JCI Insight 2018, 3, e121718. [Google Scholar] [CrossRef] [Green Version]
- Chen, M.; Hong, N.; Hu, S.; Wang, P.; Guan, H.; Xiao, M.; Zhu, X.; Al-Hatmi, A.M.; Zhou, Z.; Gao, L.; et al. Molecular identification of Cryptococcus gattii from cerebrospinal fluid using single-cell sequencing: A case study. J. Infect. 2020, 81, 634–638. [Google Scholar] [CrossRef]


{kind=link}
| Disease | Study | Experimental Group | No. Patients | Control Group | No. Patients | Cell Isolation Method | Sequencing Method | Conclusion |
|---|---|---|---|---|---|---|---|---|
| LMM | Ruan et al. (2020) | Patients with LMM secondary to LUAD or CUP | 5 | Healthy controls | 3 | FACS | Smart-seq2/Illumina HiSeqX | Identified candidate genes for RNA-based detection of CSF-CTCs in patients with LMM of LUAD and CUP. |
| LMM | Chi et al. (2020) | Patients with LMM secondary to breast cancer (N = 3) or NSCLC (N = 2) | 5 | Patients with cancer having no LMM | 18 | Flow cytometry | 10X Genomics/Illumina NovaSeq 6000 | Cancer cells, but not macrophages, within the CSF of patients with LMM express the iron-binding protein LCN2 and its receptor SCL22A17, with cancer cells appearing to survive in the CSF by outcompeting macrophages for iron. |
| LMM | Li et al. (2021) | Patients with LMM secondary to NSCLC | 4 | Nontumorgenic cells (e.g., immune cells) in the CSF | 1 | Microfluidic chip | Nextera XT DNA Library Preparation Kit (Illumina)/NextSeq mid-output Kit (Illumina) | Cell migration in NSCLC cell lines was directly proportional to CEACAM6 expression, suggesting a role in disease progression. |
| LMM | Prakadan et al. (2021) | Patients enrolled in clinical trials investigating the use of ICI in LMD | 19 | Nontumorgenic cells (e.g., immune cells) in the CSF | 19 | Pico-wells | Seq-Well/Illumina 75 Cycle NextSeq500 Kit or Illumina 100 Cycle NovaSeq6000S Kit | CD8+ T cells in the CSF are more abundant and proliferative in samples treated with ICI and exhibited higher levels of genes associated with effector function and IFN-γ signaling relative to untreated samples. |
| Brain metastasis and LMM | Rubio-Perez et al. (2021) | Patients with brain metastasis or LMM of LUAD, LUSC, SCLC, SKCM, BRCA, ESCA, HNSC and URO | 6 | Tumor-infiltrating cells as opposed to CSF cells | 6 | Flow cytometry | 10X Genomics/Illumina NovaSeq 6000 | Brain metastasis immune cell infiltrates are recapitulated in the CSF compartment. There was a significantly higher CD8+/CD4+ T cell ratio in the tumor compared to the CSF. |
| Brain metastasis and LMM | Smalley et al. (2021) | Patients with brain metastasis or LMM of melanoma | 24 | Patients with skin metastasis only | 2 | NR | 10X Genomics/Illumina NextSeq 500 | The LMM microenvironment was characterized by an immune-suppressed T-cell landscape distinct from that of brain and skin metastases. A rare population of dendritic cells (DC3) was associated with increased overall survival and positively regulated the immune environment through modulation of activated T cells and MHC expression. |
| CNSL-DLBCL | Ruan et al. (2021) | Patients with LMM secondary to CNSL-DLBCL | 6 | Healthy controls | 3 | FACS | Smart-seq2/Illumina HiSeqX | Identified inherent heterogeneity of CSF-DLBCs in cell cycle state, cancer-testis antigen expression, and classification based on single-cell germinal center B-cell signature. Identified 16 upregulated genes in CSF-DLBCs compared to normal B cells, which showed possible ‘homing effect’ of the CNS-DLBCL for the leptomeninges. |
| Alzheimer’s Disease | Gate et al. (2020) | Patients with AD or prodromal MCI | 9 AD, 9 MCI | Age-matched healthy controls | 9 | Flow cytometry | 10X Genomics/NextSeq550 Sequencer (Illumina) | TCR signaling was enhanced in CD8+ TEMRA cells circulating in the CSF of patients with AD and was negatively associated with patient cognition. |
| Neurological sequelae of COVID-19 | Song et al. (2021) | Patients with neurological sequelae of COVID-19 infection | 6 | Uninfected controls | 3 | Flow cytometry | 10X Genomics/Illumina Novaseq | Immune cell scRNA-Seq showed divergent T cell activation in the CNS during COVID-19 infection. |
| Multiple Sclerosis | Beltrán et al. (2019) | Twins with multiple sclerosis or subclinical neuroinflammation | 16 | Non-MS twins and control patients with idiopathic intracranial hypertension | 6 | FACS | Smart-Seq2/Illumina NGS HiSeq | Provided evidence for early concomitant activation of 3 components of the adaptive immune system in MS, with a notable contribution of clonally expanded TRM-like CD8+cells. |
| Multiple Sclerosis | Ramesh et al. (2020) | Patients with RRMS (n = 12) or other neurologic disease (n = 1) | 13 | Healthy controls | 3 | Flow cytometry | 10X Genomics/Illumina HiSeq4000 | Provided evidence that in MS, CSF B cells are driven to an inflammatory and clonally expanded memory and plasmablast/plasma cell phenotype. |
| Multiple Sclerosis, Anti-MOG disorder, HIV | Esaulova et al. (2020) | Patients with inflammatory demyelinating disease (either RRMS and or anti-MOG disorder), available sequencing data on 2 patients with HIV | 13 | A subject with IIH, a subject with ALS, and a healthy control | 3 | Flow cytometry | 10X Genomics/Illumina HiSeq4000 or Novaseq Sequencer | Identified distinct myeloid cell types present within the CSF of subjects with neuroinflammation. |
| Multiple Sclerosis | Hrastelj et al. (2021) | Patients with newly diagnosed, treatment-naïve MS | 21 | Patients with non-inflammatory disorders (e.g., IIH) | 20 | FACS | Tecan Ovation SoLo RNA-seq System/Illumina HiSeq4000 | CSF CD4+ T cells displayed a distinct gene expression profile when compared to blood CD4+ T cells, which was similar in non-inflammatory controls and MS and was predominated by migration molecules. |
| HIV | Farhadian et al. (2018) | HIV+ participants | 3 | Non-HIV+ controls | 2 | SeqWell array | SeqWell/Illumina HiSeq4000 platform | Identified a rare (<5% of cells) subset of myeloid cells found only in the CSF that present a gene expression signature that overlaps significantly with neurodegenerative disease–associated microglia and may perpetuate neuronal injury during HIV infection. |
| Meningitis | Chen et al. (2020) | Patient with cryptococcal meningitis (case report) | 1 | N/A | N/A | Laser microdissection | REPLI-g Single Cell Kit/NEBNext® UltraDNA Library Prep Kit | scRNA sequencing was used for the diagnosis of CNS-related mycosis caused by pathogenic fungi that could not be cultured. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yekula, A.; Tracz, J.; Rincon-Torroella, J.; Azad, T.; Bettegowda, C. Single-Cell RNA Sequencing of Cerebrospinal Fluid as an Advanced Form of Liquid Biopsy for Neurological Disorders. Brain Sci. 2022, 12, 812. https://doi.org/10.3390/brainsci12070812
Yekula A, Tracz J, Rincon-Torroella J, Azad T, Bettegowda C. Single-Cell RNA Sequencing of Cerebrospinal Fluid as an Advanced Form of Liquid Biopsy for Neurological Disorders. Brain Sciences. 2022; 12(7):812. https://doi.org/10.3390/brainsci12070812
Chicago/Turabian StyleYekula, Anudeep, Jovanna Tracz, Jordina Rincon-Torroella, Tej Azad, and Chetan Bettegowda. 2022. "Single-Cell RNA Sequencing of Cerebrospinal Fluid as an Advanced Form of Liquid Biopsy for Neurological Disorders" Brain Sciences 12, no. 7: 812. https://doi.org/10.3390/brainsci12070812