
Supramarginal Resection for Glioblastoma: It Is Time to Set Boundaries! A Critical Review on a Hot Topic


1
Unit of Neurosurgery, Department of Surgical Sciences, Hospital Santa Maria Goretti, 04100 Latina, Italy
2
Head and Neck Department, Neurosurgery, Istituto Ospedaliero Fondazione Poliambulanza, 25124 Brescia, Italy
3
Technology for Health PhD Program, University of Brescia, 25124 Brescia, Italy
4
IRCCS Fondazione Policlinico San Matteo, 27100 Pavia, Italy
*
Author to whom correspondence should be addressed.
Brain Sci. 2022, 12(5), 652; https://doi.org/10.3390/brainsci12050652
Submission received: 15 April 2022
/
Revised: 13 May 2022
/
Accepted: 14 May 2022
/
Published: 16 May 2022
(This article belongs to the Special Issue Frontiers in Neurooncology and Neurosurgery)
Abstract
:Glioblastoma are the most common primary malignant brain tumors with a highly infiltrative behavior. The extent of resection of the enhancing component has been shown to be correlated to survival. Recently, it has been proposed to move the resection beyond the contrast-enhanced portion into the MR hyper intense tissue which typically surrounds the tumor, the so-called supra marginal resection (SMR). Though it should be associated with better overall survival (OS), a potential harmful resection must be avoided in order not to create new neurological deficits. Through this work, we aimed to perform a critical review of SMR in patients with Glioblastoma. A Medline database search and a pooled meta-analysis of HRs were conducted; 19 articles were included. Meta-analysis revealed a pooled OS HR of 0.64 (p = 0.052). SMR is generally considered as the resection of any T1w gadolinium-enhanced tumor exceeding FLAIR volume, but no consensus exists about the amount of volume that must be resected to have an OS gain. Equally, the role and the weight of several pre-operative features (tumor volume, location, eloquence, etc.), the intraoperative methods to extend resection, and the post-operative deficits, need to be considered more deeply in future studies.
1. Introduction
Glioblastoma represents the most common primary malignant brain tumor in adults with a less than 7% 5-year survival rate despite complete resection and adjuvant therapies. By definition, it is an incurable disease due to its infiltrative nature which invariably and typically brings relapse around the surgical cavity or, less frequently, into new remote tumoral foci [1]. This peculiarity was already noted by Dandy who tried to eliminate most of the tumor by performing a hemispherectomy, with frustrating results in terms of neurological deficit and, ultimately, survival. That attempt represented the first experience with supramarginal resection (SMR) [2].
Usually, Glioblastoma is depicted on MRI as a contrast-enhanced nodule surrounded by a T2 hyperintense signal of variable shape and extension; this hyper signal is generally thought to represent infiltrated brain. Surgery has classically aimed toward the complete resection of the MRI T1w sequence enhancing tumor and accumulated data show the benefit of complete resection over partial resection or biopsy [3,4]. Understandably, several authors investigated if resecting brain matter beyond the contrast-enhanced area could add further improvements in overall survival (OS). Despite the wide range of variability in patients’ cohorts, selection criteria, surgical techniques, and evaluation of results, the majority of researchers agreed with the fact that SMR could improve OS.
Although it could seem logical that, for an infiltrating disease, the more tumor is eliminated the more positive effects can be expected, in Glioblastoma, the matter of maintaining a balance between aggressive resection and neurological functioning is of particular interest due to the short survival and the eventual lack of time for recovery. Still, looking at the available evidence, many issues are unresolved, starting from the definition of SMR itself. Similarly, the extent of resection after which an SMR is obtained and how to assess it is not clear. Are there intraoperative adjuncts that guide the surgeon to push resection beyond the contrast-enhanced edges? More generally, can an SMR be proposed for all Glioblastoma patients? Are there pre-operative selection criteria for SMR? How can SMR be balanced with the functional outcome? What is the relationship between SMR and standard prognostic factors (i.e., age, volume, site, genetic features, involvement of periventricular zone, etc.)?
In this work, we performed a critical literature review on SMR on patients affected by Glioblastoma, trying to shed light on many debated points that need to be elucidated before it can be considered a clearly advantageous treatment.
2. Materials and Methods
A search was conducted on Medline Database using the following keywords: “Supramarginal resection”, “Supratotal resection”, “FLAIR resection”, “FLAIRectomy”, and “Lobectomy” associated with “Glioblastoma” OR “Glioma” OR “High grade Glioma”. Relevant papers were also obtained by references sections. A clinical series and literature review were included in this analysis. Articles were excluded if they concerned low-grade gliomas. Case reports, surveys, and consensus statements were excluded from the review, but they were considered for the discussion. Moreover, whenever it was possible, overall survival Hazard Ratios were collected and analyzed in a pooled meta-analysis. Specifically, it was performed using R software (R Core Team, Wien, Austria) and the package “metafor” [5]. Multilevel linear mixed effects models with an unstructured covariance matrix were used for the meta-analysis in order to account for the clustering of data deriving from the same studies. p values < 0.05 were considered statistically significant.
3. Results
A total of 19 articles were included, with 2 literature reviews [6,7] and 17 clinical series. The majority of them defined SMR as the resection of any FLAIR volume beyond T1 contrast-enhanced tumor edges. Meanwhile, papers by Roh et al., Schneider et al., and Figueroa et al. equated SMR to the concept of lobectomy; particularly, the two last papers showed the results of a standard or a minimally invasive anterior temporal lobectomy [8,9]. Finally, IONM represented the most commonly used intraoperative method.
A paper by Karshnia et al. was excluded because it was a consensus of recommendations [10], while another by Rakovec et al. was not included as it was a survey [11]. The work by Borger et al. was excluded considering that the authors analyzed the seizure outcome of the same patients as Schneider et al., already included in this review [12]. Table 1 shows all the available data extracted from the analyzed papers. Considering that the single-center retrospective observational cohort studies represented the greatest part of the included papers, the level of evidence could be summarized as class C-EO [13].
As far as meta-analysis was concerned, some papers were excluded. A study by Roh et al. was discharged because HR was reported as the ratio between SupTR and GTR [14]; works by Pessina et al. and Shah et al. did not show HR [15,16]; a paper by Certo et al. described a correlation index and was not included [17]; only representation of Kaplan-Meier curves by Altieri et al. and Aldave et al. led to the exclusion of these studies [18,19]; and a paper by Mampre et al. was excluded due to the hazard-ratio being calculated for post-operative volumes and not according to extent of resection [20]. The work of Eyopoglu et al. was excluded as it was not a controlled study [21]. As for a paper by Tripathi et al., HR was considered for every t ype of glioma but, belonging to the same study, they were interpreted as correlated [22]. Finally, since Li et al. described SMR HR for a FLAIR resection of at least 53.21%, only this result was included in this work [23].
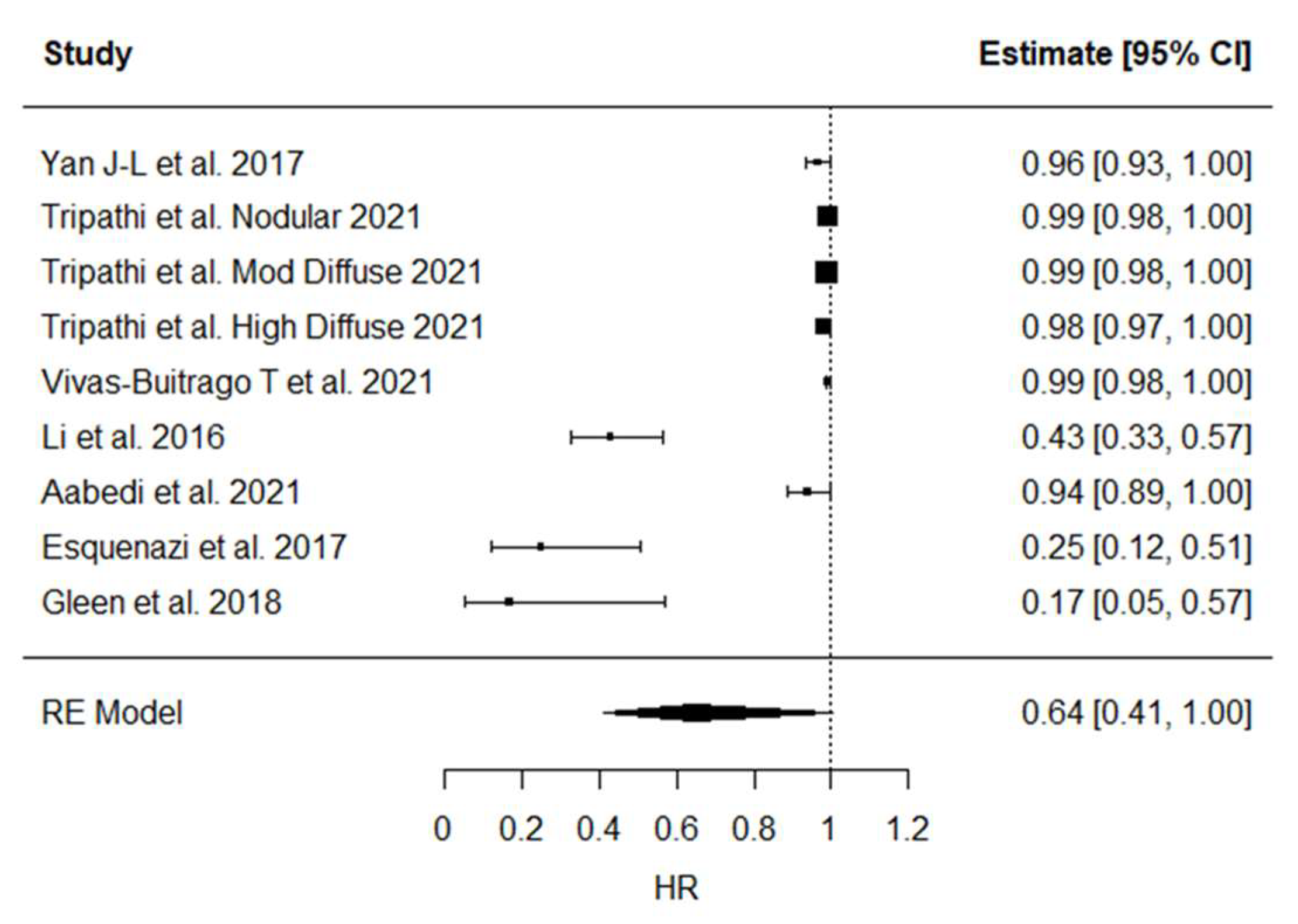
Statistical analysis revealed a high and significant heterogeneity between studies (p < 0.001). The calculated pooled HR was 0.64 (0.41–1.00, p = 0.052) (Figure 1).
4. Discussion
Glioblastoma continues to represent a hard therapeutic challenge considering its high malignancy due to its infiltrative nature. A recent 2021 WHO Classification abutted the term “glioblastoma” to only wild-type IDH gliomas with certain pathological and molecular features; on the contrary, we are allowed to include a “grade 4 astrocytoma” if the IDH gene is mutated. The difference is substantial, considering the clinical course, therapeutic response, and patient prognosis [24,25]. Whatever the definition, one of the mainstays for surgery of gliomas pivots around the so-called “maximal safe resection” which implies balancing oncological useful resection with maintaining optimal neurological functioning. In fact, both of these goals (total removal and neurological integrity) equally influence the prognosis [26].
4.1. Definition of SMR, Its Impact on OS, and the Role of FLAIR
There is a discrete consensus about the definition of SMR since the majority of the studies state that SMR is the resection of any part of a T1w gadolinium-enhanced tumor exceeding FLAIR volume.
However, far less agreement can be found concerning the role of SMR and its impact on OS. In fact, in contrast to the well-established role of the EOR of the contrast-enhanced component, when considering the so-called “FLAIR-ectomy” there is much less agreement. Li et al. found that a resection larger than 53.2% of FLAIR volume confers an advantage on OS in previously untreated IDH mutated patients [23]. A quite similar value was found by Pessina et al. and Tripathi et al. who conducted a different analysis according to the radiological appearance of the tumor; while SMR seems to bring an OS advantage in patients with moderately and highly diffuse wtIDH glioblastomas; in case of nodular ones, a maximum of 29% of FLAIR volume would be advantageous [24]. Additionally, Yan et al. found the DTI sequence’s anisotropic component to bepositively associated with OS and PFS [27]. The review by Karschnia et al. tried to clarify the topic concluding that SMR is defined as any resection beyond contrast enhancement into T2w/FLAIR hyperintensity [10].
It is evident that many of the uncertainties come from the real significance of the hyperintense T2 signal. It is generally found that the GBM relapses just beyond the resected contrast-enhanced edges, as some works claimed it is plausible to think that stem-like cells can be found in this area [28]. Studies comparing MR and 18FET-PET demonstrated that the T2 hyper signal is likely to host tumor cells [29]. However, PET imaging is an advanced modality that is not available in every center, so the majority of the studies are based on standard MR imaging. From this perspective, the FLAIR hyper signal has been retained as a marker of tumoral infiltration, although it cannot actually distinguish infiltration from brain edema. To resolve that issue, a FLAIR hyper signal can be found around brain metastasis too, reflecting a vasogenic edema [30]. Some studies tried to develop methods to differentiate tumor infiltration areas from edema. Certo et al. described a manual segmentation method that distinguished Region of Interests (ROIs) with different hyperintensity values on FLAIR sequences; ROIs with higher values represented edema [17]. Other studies revealed that Apparent Diffusion Coefficient (ADC) mapping can have a prognostic value in patients with a Glioblastoma, as it reflects water sequestration and, as a consequence, hypercellularity. Elson et al. found that a <0.3 minimum ADC value was associated with a shorter OS and PFS [31]. Finally, a peritumoral FLAIR hyper signal could have a different significance, and hence, the benefit of removing apparently healthy tissue beyond the contrast-enhancing “meaty” tissue has conflicting evidence.
4.2. SMR, Tumor Volume, and Location
When talking about the resection of an infiltrating brain tumor, the first questions that arise in the surgeon’s mind are about the location (eloquent/critical area versus less “dangerous” areas) and volume, which are intimately bound. A large part of the studies included in this review showed a wide range of pre-operative tumor volumes and only a few differentiated between eloquent and non-eloquent locations. For example, Vivaz-Butraigo et al. reported a range between 1 and 124 cm3 for contrast-enhanced volumes that reached 182.74 cm3 in FLAIR sequences. They reported a positive influence in cases of 20% to 50% SMR, without a clear advantage for greater resection [32].
Although in a standardized predictive model for Glioblastoma pre-operative tumors volume is not usually considered, it is intuitive that larger tumors can hamper SMR, especially when coupled to an eloquent or near-eloquent location. Such a consideration found important feedback in the work by Roh et al. which showed that a frontal or temporal lobectomy for glioblastoma located in the non-dominant hemisphere was associated with longer OS and PFS [14]. Schneider et al. showed an anterior temporal lobectomy was able to prolong both OS and PFS, both on the dominant and non-dominant sides. On the contrary, Figueroa et al. did not find a survival advantage in using this technique. Regardless, according to the survey by Rakovec et al., the neurosurgical oncology community seems to agree with limiting the SMR to right anterior temporal and right frontal lobe GBM [11].
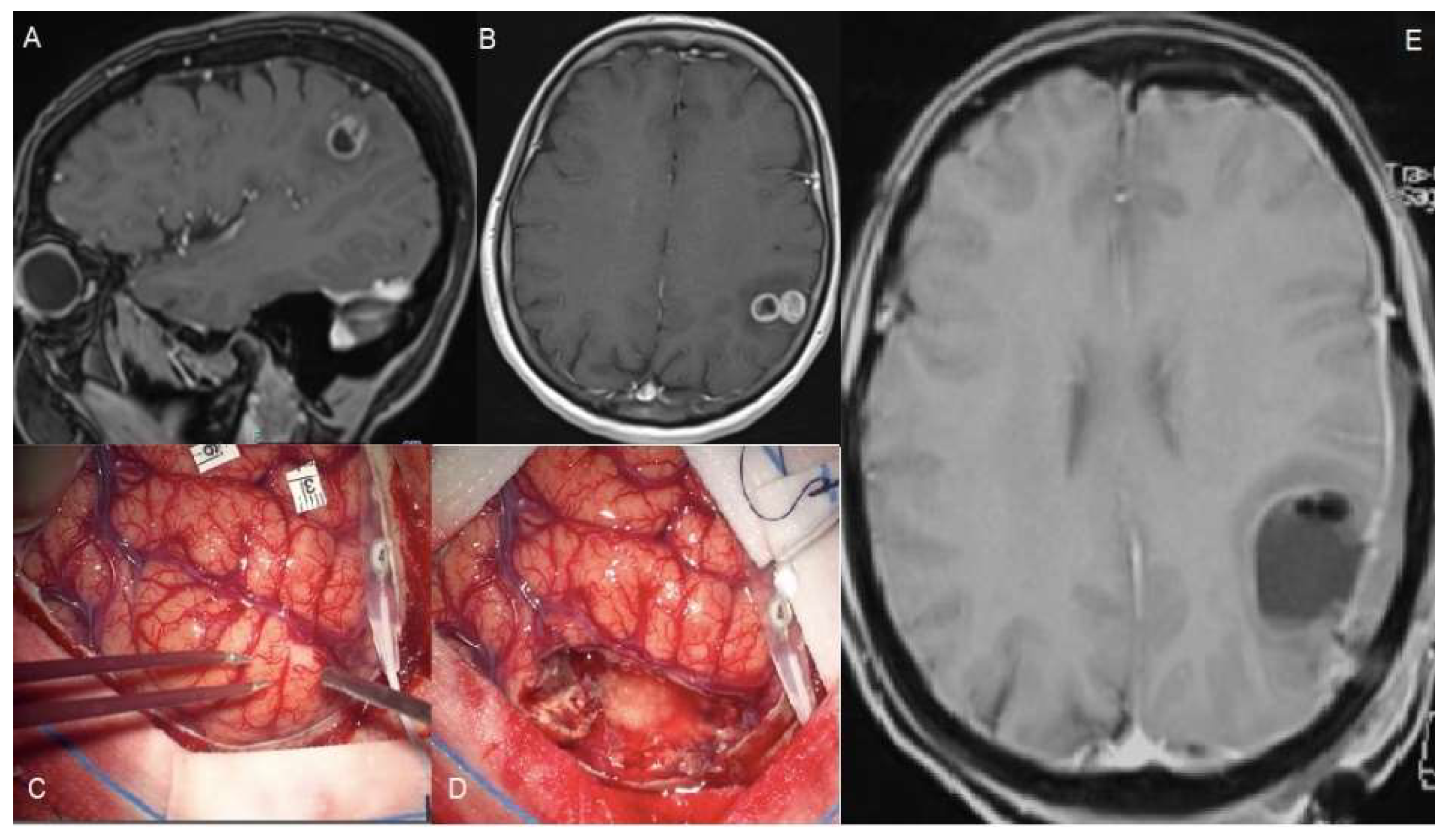
In some cases, such as a small GBM located in the eloquent area, SMR can be advocated (see Figure 2); however, this only concerns single cases and a very attentive selection. Other than these very specific cases, it seems hard to conceive that patients with larger lesions near or inside eloquent areas could benefit from SMR without putting them at higher risk of neurological outcomes. As discussed below, accumulated evidence demonstrated that a worsened post-operative neurological performance abrogates survival benefits from complete tumor resection or unilobed tumor location [33,34,35]. An analog consideration could be done for tumors infiltrating deep neural and vascular structures (i.e., insular glioblastoma) which typically represent the boundaries of the resection cavity. It appears that a deeper analysis is needed in order to clarify the role of tumor volume and location on SMR, with special attention regarding the eloquent area location.
4.3. SMR and Tumors Infiltrating Periventricular White Matter
Tumor-initiating brain cells are thought to be placed into the so-called Subventricular Zone (SVZ) and evidence supporting this assumption is still accumulating. The contact between cancerous cells and SVZ seems to confer higher resistance to traditional radio- and chemotherapy [36]. Additionally, a lateral ventricle wall involvement is considered the source of leptomeningeal dissemination and, finally, for obstructive hydrocephalus [37]. Hallaert et al. analyzed 214 patients and found that contact with SVZ was associated with unmethylated MGMT and a shorter OS [38]. Vivaz-Buitrago et al. and Tripathi et al. examined the involvement of the lateral ventricle, confirming its role as a poor prognostic factor in case the contrast-enhancement reaches the ependyma [32]. However, the role of the infiltration of the ependyma by the FLAIR hyper signal received less attention. Mistry et al. demonstrated that the distance between glioblastoma and SVZ did not influence OS, which, on the contrary, suffers from the contact between SVZ and contrast-enhancement edges [22]. This data seems conflicting since as long as the tumor grows toward the SVZ, it is difficult to explain why it appears true for the CE portion only. In other words, if FLAIR volume contains tumoral cells, it should have the same role in the SVZ involvement. As a consequence, does the resection of this volume confer increased OS? Undoubtedly, more studies are necessary and this factor should be well analyzed if the neurosurgical community wants to establish criteria for SMR in the case of high-grade gliomas.
4.4. SMR and Intraoperative Techniques
There are several technological tools used intraoperatively to guide tumor resection which help in better visualizing tumor tissue such as intraoperative MRI, ultrasound, fluorescent agents, and 5-ALA. These latter two are specifically addressed to detect tissue that corresponds to the contrast-enhancing MR images.
There is no clarity on how intraoperative technologies make SMR feasible in glioma surgery. Certainly, the use of iMR (intraoperative magnetic resonance) and fluorophores helps in the best extension of tumor resection [39,40].
When coming to the eloquent location of tumors, intraoperative mapping is useful to guide resection according to functional boundaries rather than only anatomical. This strategy has shown robust results both for LGG and HGG. However, despite the use of functional monitoring and mapping, the idea to pursue aggressive resection in GBM has to take into account the fact that rapidly growing tumors bring a more destructive behavior compared to their slow-growing counterparts. This biological difference implies that brain plasticity has much less time to intervene, not allowing the brain to reshape and potentially increasing the risk for post-operative definitive impairments [41].
Pessina et al. performed a resection guided by neuronavigation and ultrasounds, extending until cortical and subcortical stimulation enhanced the risk of neurological deficits [15].
Some authors assert that sodium fluorescein, which accumulates in the extracellular space when the barrier is damaged, may be the intraoperative equivalent of the radiological signal given by gadolinium. The same authors state that this marker extends beyond tumor regions with contrast pinch and therefore can predict the pathological tissue facilitating resection [42]. Other authors recommend associating fluorescein with Raman spectroscopy which has been shown to be able to identify tumor versus healthy tissue at the margins of resection [43]. Furthermore, laser endomicroscopy, associated with fluorescein, can also have the same effect [44,45,46]. However, the use of 5-ALA appears questionable. In fact, despite Eyopoglu et al. finding an OS advantage in the DiVA group, Roh et al. did not obtain a better survival in their subgroup of patients in which 5-ALA was employed [21,32]. Nevertheless, experiences are limited and they cannot be elevated as a standard methodology.
4.5. SMR and Functional Outcome
It has been established that the total or near-total resection of the contrast-enhancing component is a strong predictor of prolonged OS [47,48,49,50,51]. In more recent years, it has also been demonstrated how radical resection must be balanced with the preservation of adequate functional outcomes, since this latter can negatively affect the deployment of adjuvant treatments and the OS. A first retrospective study published by McGirt et al. on Glioblastoma patients who received tumor resection introduced the prominent role of surgically acquired language and motor deficit on survival impairment (9.0-months and 9.6-months median survival, respectively, compared to 12.8 months without a new deficit, p < 0.05) [33]. Furthermore, in 2015, Verlut et al. showed that post-operative motor deterioration was associated with poor outcomes in patients receiving surgery followed chemo-radiotherapy [46]. Specifically, it has more recently been demonstrated how severe post-operative neurological deficits significantly reduce survival rates and become a predominant negative prognosticator over EOR, tumor location, KPS, age at the date of surgery, MGMT promoter methylation status, and adjuvant treatment regimen. Rahman and colleagues published a comprehensive work demonstrating that post-surgical acquired neurological deficits abrogate the survival benefit gained by EOR of 95% and more [34].
So, if these considerations hold true for radical resection, it is still more of a concern when dealing with SMR, especially when tumors are located near or inside eloquent locations. Aabaedi et al. claimed that as far as the subgroup of wild-type IDH Glioblastoma is concerned, no difference between CE and non-CE resection emerged in terms of OS; on the contrary, they reinforced the concept that a neurological impairment represents the real key factor for survival of these patients [52].
The greatest part of the papers included in our review compared pre- and post-operative KPS and they did not find any difference, concluding that SMR was not associated with a worse clinical outcome. Nevertheless, even if KPS has a great value in the oncological field, it is necessary to remember that it does not explore every clinical aspect. In fact, less attention has been paid to post-operative cognitive status evaluation; only a few studies in this review conducted a deep analysis of specific symptoms, above all neurocognitive ones. As emerged from the review by Gately et al., a longer OS should be balanced with a certain quality of life that permits them to maintain real functional independence [53]. Therefore, as Roh et al. stated, a study that analyzes the effects of SMR on neuropsychological functions is desirable [14].
4.6. Pooled HR Meta-Analysis
We conducted a pooled meta-analysis to summarize overall survival HR resulting from every study included as described earlier. The first element that emerges is the high heterogeneity between studies which makes it difficult to make a generalization. Moreover, confidence intervals did not include the indifference in only three cases. Furthermore, Li et al. did not report the overall FLAIR resection HR, a result that could have an important value in the final analysis. Nevertheless, despite all these elements, we obtained a slightly significant advantage on OS by performing an SMR, but it only reinforces our aforementioned considerations. In other words, the evidence to support the superiority of SMR over GTR on PFS and OS is weak.
In conclusion, except for a few studies, clear criteria for a pre-operative allocation to a more aggressive surgery do not exist. Moreover, as the patient’s post-operative neurological outcome is universally recognized as the most important factor influencing OS, it appears necessary to conduct a more detailed prospective study evaluating the anatomical, radiological, and surgical factors favoring SMR.
5. Conclusions
We performed a critical review of published articles concerning SMR in patients affected by glioblastoma. The definition of SMR is still debatable and no consensus exists on which radiological and clinical criteria would indicate it as a useful treatment. Similarly, which intraoperative method is the most successful in performing a safe and effective SMR has yet to be determined. Finally, the detailed analysis of post-operative neurological outcomes is limited to KPS and does not consider neurocognitive functions.
Funding
This research received no external funding.
Acknowledgments
We thank Marco Viganò for their support in pooled meta-analysis.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Guerrini, F.; Mazzeo, L.A.; Rossi, G.; Verlotta, M.; Del Maestro, M.; Rampini, A.D.; Pesce, A.; Vigano, M.; Luzzi, S.; Galzio, R.J.; et al. Is It Worth Considering Multicentric High-Grade Glioma a Surgical Disease? Analysis of Our Clinical Experience and Literature Review. Tomography 2021, 7, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Bell, E., Jr.; Karnosh, L.J. Cerebral hemispherectomy; report of a case 10 years after operation. J. Neurosurg. 1949, 6, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Stummer, W.; Reulen, H.J.; Meinel, T.; Pichlmeier, U.; Schumacher, W.; Tonn, J.C.; Rohde, V.; Oppel, F.; Turowski, B.; Woiciechowsky, C.; et al. Extent of resection and survival in glioblastoma multiforme: Identification of and adjustment for bias. Neurosurgery 2008, 62, 564–576; discussion 564–576. [Google Scholar] [CrossRef] [PubMed]
- Chaichana, K.L.; Jusue-Torres, I.; Navarro-Ramirez, R.; Raza, S.M.; Pascual-Gallego, M.; Ibrahim, A.; Hernandez-Hermann, M.; Gomez, L.; Ye, X.; Weingart, J.D.; et al. Establishing percent resection and residual volume thresholds affecting survival and recurrence for patients with newly diagnosed intracranial glioblastoma. Neuro-Oncology 2014, 16, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Viechtbauer, W. Conducting Meta-Analyses in R with the metafor Package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef] [Green Version]
- Dimou, J.; Beland, B.; Kelly, J. Supramaximal resection: A systematic review of its safety, efficacy and feasibility in glioblastoma. J. Clin. Neurosci. 2020, 72, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Certo, F.; Stummer, W.; Farah, J.O.; Freyschlag, C.; Visocchi, M.; Morrone, A.; Altieri, R.; Toccaceli, G.; Peschillo, S.; Thome, C.; et al. Supramarginal resection of glioblastoma: 5-ALA fluorescence, combined intraoperative strategies and correlation with survival. J. Neurosurg. Sci. 2019, 63, 625–632. [Google Scholar] [CrossRef]
- Schneider, M.; Potthoff, A.L.; Keil, V.C.; Guresir, A.; Weller, J.; Borger, V.; Hamed, M.; Waha, A.; Vatter, H.; Guresir, E.; et al. Surgery for temporal glioblastoma: Lobectomy outranks oncosurgical-based gross-total resection. J. Neuro-Oncol. 2019, 145, 143–150. [Google Scholar] [CrossRef]
- Figueroa, J.; Morell, A.; Bowory, V.; Shah, A.H.; Eichberg, D.; Buttrick, S.S.; Richardson, A.; Sarkiss, C.; Ivan, M.E.; Komotar, R.J. Minimally invasive keyhole temporal lobectomy approach for supramaximal glioma resection: A safety and feasibility study. J. Clin. Neurosci. 2020, 72, 57–62. [Google Scholar] [CrossRef]
- Karschnia, P.; Vogelbaum, M.A.; van den Bent, M.; Cahill, D.P.; Bello, L.; Narita, Y.; Berger, M.S.; Weller, M.; Tonn, J.C. Evidence-based recommendations on categories for extent of resection in diffuse glioma. Eur. J. Cancer 2021, 149, 23–33. [Google Scholar] [CrossRef]
- Rakovec, M.; Khalafallah, A.M.; Wei, O.; Day, D.; Sheehan, J.P.; Sherman, J.H.; Mukherjee, D. A Consensus Definition of Supratotal Resection for Anatomically Distinct Primary Glioblastoma: An AANS/CNS Section on Tumors Survey of Neurosurgical Oncologists. J. Neuro-Oncol. 2022. [Google Scholar] [CrossRef]
- Borger, V.; Hamed, M.; Ilic, I.; Potthoff, A.L.; Racz, A.; Schafer, N.; Guresir, E.; Surges, R.; Herrlinger, U.; Vatter, H.; et al. Seizure outcome in temporal glioblastoma surgery: Lobectomy as a supratotal resection regime outclasses conventional gross-total resection. J. Neuro-Oncol. 2021, 152, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Halperin, J.L.; Levine, G.N.; Al-Khatib, S.M.; Birtcher, K.K.; Bozkurt, B.; Brindis, R.G.; Cigarroa, J.E.; Curtis, L.H.; Fleisher, L.A.; Gentile, F.; et al. Further Evolution of the ACC/AHA Clinical Practice Guideline Recommendation Classification System: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2016, 133, 1426–1428. [Google Scholar] [CrossRef] [PubMed]
- Roh, T.H.; Kang, S.G.; Moon, J.H.; Sung, K.S.; Park, H.H.; Kim, S.H.; Kim, E.H.; Hong, C.K.; Suh, C.O.; Chang, J.H. Survival benefit of lobectomy over gross-total resection without lobectomy in cases of glioblastoma in the noneloquent area: A retrospective study. J. Neurosurg. 2019, 132, 895–901. [Google Scholar] [CrossRef] [PubMed]
- Pessina, F.; Navarria, P.; Cozzi, L.; Ascolese, A.M.; Simonelli, M.; Santoro, A.; Clerici, E.; Rossi, M.; Scorsetti, M.; Bello, L. Maximize surgical resection beyond contrast-enhancing boundaries in newly diagnosed glioblastoma multiforme: Is it useful and safe? A single institution retrospective experience. J. Neuro-Oncol. 2017, 135, 129–139. [Google Scholar] [CrossRef]
- Shah, A.H.; Mahavadi, A.; Di, L.; Sanjurjo, A.; Eichberg, D.G.; Borowy, V.; Figueroa, J.; Luther, E.; de la Fuente, M.I.; Semonche, A.; et al. Survival benefit of lobectomy for glioblastoma: Moving towards radical supramaximal resection. J. Neuro-Oncol. 2020, 148, 501–508. [Google Scholar] [CrossRef]
- Certo, F.; Altieri, R.; Maione, M.; Schonauer, C.; Sortino, G.; Fiumano, G.; Tirro, E.; Massimino, M.; Broggi, G.; Vigneri, P.; et al. FLAIRectomy in Supramarginal Resection of Glioblastoma Correlates with Clinical Outcome and Survival Analysis: A Prospective, Single Institution, Case Series. Oper. Neurosurg. 2021, 20, 151–163. [Google Scholar] [CrossRef]
- Altieri, R.; Melcarne, A.; Soffietti, R.; Ruda, R.; Franchino, F.; Pellerino, A.; La Rocca, G.; Sabatino, G.; Olivi, A.; Ducati, A.; et al. Supratotal Resection of Glioblastoma: Is Less More? Surg. Technol. Int. 2019, 35, 432–440. [Google Scholar]
- Aldave, G.; Tejada, S.; Pay, E.; Marigil, M.; Bejarano, B.; Idoate, M.A.; Diez-Valle, R. Prognostic value of residual fluorescent tissue in glioblastoma patients after gross total resection in 5-aminolevulinic Acid-guided surgery. Neurosurgery 2013, 72, 915–920; discussion 920–921. [Google Scholar] [CrossRef]
- Mampre, D.; Ehresman, J.; Pinilla-Monsalve, G.; Osorio, M.A.G.; Olivi, A.; Quinones-Hinojosa, A.; Chaichana, K.L. Extending the resection beyond the contrast-enhancement for glioblastoma: Feasibility, efficacy, and outcomes. Br. J. Neurosurg. 2018, 32, 528–535. [Google Scholar] [CrossRef]
- Eyupoglu, I.Y.; Hore, N.; Merkel, A.; Buslei, R.; Buchfelder, M.; Savaskan, N. Supra-complete surgery via dual intraoperative visualization approach (DiVA) prolongs patient survival in glioblastoma. Oncotarget 2016, 7, 25755–25768. [Google Scholar] [CrossRef] [PubMed]
- Tripathi, S.; Vivas-Buitrago, T.; Domingo, R.A.; Biase, G.; Brown, D.; Akinduro, O.O.; Ramos-Fresnedo, A.; Sherman, W.; Gupta, V.; Middlebrooks, E.H.; et al. IDH-wild-type glioblastoma cell density and infiltration distribution influence on supramarginal resection and its impact on overall survival: A mathematical model. J. Neurosurg. 2021, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.M.; Suki, D.; Hess, K.; Sawaya, R. The influence of maximum safe resection of glioblastoma on survival in 1229 patients: Can we do better than gross-total resection? J. Neurosurg. 2016, 124, 977–988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro-Oncology 2021, 23, 1231–1251. [Google Scholar] [CrossRef] [PubMed]
- Wen, P.Y.; Packer, R.J. The 2021 WHO Classification of Tumors of the Central Nervous System: Clinical implications. Neuro-Oncology 2021, 23, 1215–1217. [Google Scholar] [CrossRef]
- Sanai, N.; Polley, M.Y.; McDermott, M.W.; Parsa, A.T.; Berger, M.S. An extent of resection threshold for newly diagnosed glioblastomas. J. Neurosurg. 2011, 115, 3–8. [Google Scholar] [CrossRef] [Green Version]
- Yan, J.L.; van der Hoorn, A.; Larkin, T.J.; Boonzaier, N.R.; Matys, T.; Price, S.J. Extent of resection of peritumoral diffusion tensor imaging-detected abnormality as a predictor of survival in adult glioblastoma patients. J. Neurosurg. 2017, 126, 234–241. [Google Scholar] [CrossRef]
- Torres, D.; Canoll, P. Alterations in the Brain Microenvironment in Diffusely Infiltrating Low-Grade Glioma. Neurosurg. Clin. N. Am. 2019, 30, 27–34. [Google Scholar] [CrossRef]
- Suchorska, B.; Jansen, N.L.; Linn, J.; Kretzschmar, H.; Janssen, H.; Eigenbrod, S.; Simon, M.; Popperl, G.; Kreth, F.W.; la Fougere, C.; et al. Biological tumor volume in 18FET-PET before radiochemotherapy correlates with survival in GBM. Neurology 2015, 84, 710–719. [Google Scholar] [CrossRef] [Green Version]
- Muccio, C.F.; Tarantino, A.; Esposito, G.; Cerase, A. Differential diagnosis by unenhanced FLAIR T2-weighted magnetic resonance images between solitary high grade gliomas and cerebral metastases appearing as contrast-enhancing cortico-subcortical lesions. J. Neuro-Oncol. 2011, 103, 713–717. [Google Scholar] [CrossRef]
- Elson, A.; Bovi, J.; Siker, M.; Schultz, C.; Paulson, E. Evaluation of absolute and normalized apparent diffusion coefficient (ADC) values within the post-operative T2/FLAIR volume as adverse prognostic indicators in glioblastoma. J. Neuro-Oncol. 2015, 122, 549–558. [Google Scholar] [CrossRef] [PubMed]
- Vivas-Buitrago, T.; Domingo, R.A.; Tripathi, S.; De Biase, G.; Brown, D.; Akinduro, O.O.; Ramos-Fresnedo, A.; Sabsevitz, D.S.; Bendok, B.R.; Sherman, W.; et al. Influence of supramarginal resection on survival outcomes after gross-total resection of IDH-wild-type glioblastoma. J. Neurosurg. 2022, 136, 1–8. [Google Scholar] [CrossRef] [PubMed]
- McGirt, M.J.; Mukherjee, D.; Chaichana, K.L.; Than, K.D.; Weingart, J.D.; Quinones-Hinojosa, A. Association of surgically acquired motor and language deficits on overall survival after resection of glioblastoma multiforme. Neurosurgery 2009, 65, 463–469; discussion 469–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verlut, C.; Mouillet, G.; Magnin, E.; Buffet-Miny, J.; Viennet, G.; Cattin, F.; Billon-Grand, N.C.; Bonnet, E.; Servagi-Vernat, S.; Godard, J.; et al. Age, Neurological Status MRC Scale, and Postoperative Morbidity are Prognostic Factors in Patients with Glioblastoma Treated by Chemoradiotherapy. Clinical Medicine Insights. Oncology 2016, 10, 77–82. [Google Scholar] [CrossRef] [Green Version]
- Rahman, M.; Abbatematteo, J.; De Leo, E.K.; Kubilis, P.S.; Vaziri, S.; Bova, F.; Sayour, E.; Mitchell, D.; Quinones-Hinojosa, A. The effects of new or worsened postoperative neurological deficits on survival of patients with glioblastoma. J. Neurosurg. 2017, 127, 123–131. [Google Scholar] [CrossRef]
- Piccirillo, S.G.; Spiteri, I.; Sottoriva, A.; Touloumis, A.; Ber, S.; Price, S.J.; Heywood, R.; Francis, N.J.; Howarth, K.D.; Collins, V.P.; et al. Contributions to drug resistance in glioblastoma derived from malignant cells in the sub-ependymal zone. Cancer Res. 2015, 75, 194–202. [Google Scholar] [CrossRef] [Green Version]
- Mistry, A.M.; Kelly, P.D.; Gallant, J.N.; Mummareddy, N.; Mobley, B.C.; Thompson, R.C.; Chambless, L.B. Comparative Analysis of Subventricular Zone Glioblastoma Contact and Ventricular Entry During Resection in Predicting Dissemination, Hydrocephalus, and Survival. Neurosurgery 2019, 85, E924–E932. [Google Scholar] [CrossRef]
- Hallaert, G.; Pinson, H.; Van den Broecke, C.; Vanhauwaert, D.; Van Roost, D.; Boterberg, T.; Kalala, J.P. Subventricular zone contacting glioblastoma: Tumor size, molecular biological factors and patient survival. Acta Oncol. 2020, 59, 1474–1479. [Google Scholar] [CrossRef]
- Stummer, W.; Pichlmeier, U.; Meinel, T.; Wiestler, O.D.; Zanella, F.; Reulen, H.J. Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: A randomised controlled multicentre phase III trial. Lancet Oncol. 2006, 7, 392–401. [Google Scholar] [CrossRef]
- Senft, C.; Bink, A.; Franz, K.; Vatter, H.; Gasser, T.; Seifert, V. Intraoperative MRI guidance and extent of resection in glioma surgery: A randomised, controlled trial. Lancet Oncol. 2011, 12, 997–1003. [Google Scholar] [CrossRef]
- Duffau, H. The huge plastic potential of adult brain and the role of connectomics: New insights provided by serial mappings in glioma surgery. Cortex J. Devoted Study Nerv. Syst. Behav. 2014, 58, 325–337. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.M.; Banu, M.A.; Canoll, P.; Bruce, J.N. Rationale and Clinical Implications of Fluorescein-Guided Supramarginal Resection in Newly Diagnosed High-Grade Glioma. Front. Oncol. 2021, 11, 666734. [Google Scholar] [CrossRef] [PubMed]
- Hollon, T.; Lewis, S.; Freudiger, C.W.; Sunney Xie, X.; Orringer, D.A. Improving the accuracy of brain tumor surgery via Raman-based technology. Neurosurg. Focus 2016, 40, E9. [Google Scholar] [CrossRef] [PubMed]
- Martirosyan, N.L.; Eschbacher, J.M.; Kalani, M.Y.; Turner, J.D.; Belykh, E.; Spetzler, R.F.; Nakaji, P.; Preul, M.C. Prospective evaluation of the utility of intraoperative confocal laser endomicroscopy in patients with brain neoplasms using fluorescein sodium: Experience with 74 cases. Neurosurg. Focus 2016, 40, E11. [Google Scholar] [CrossRef] [Green Version]
- Acerbi, F.; Pollo, B.; De Laurentis, C.; Restelli, F.; Falco, J.; Vetrano, I.G.; Broggi, M.; Schiariti, M.; Tramacere, I.; Ferroli, P.; et al. Ex Vivo Fluorescein-Assisted Confocal Laser Endomicroscopy (CONVIVO(R) System) in Patients with Glioblastoma: Results from a Prospective Study. Front. Oncol. 2020, 10, 606574. [Google Scholar] [CrossRef] [PubMed]
- Belykh, E.; Onaka, N.R.; Zhao, X.; Abramov, I.; Eschbacher, J.M.; Nakaji, P.; Preul, M.C. High-Dose Fluorescein Reveals Unusual Confocal Endomicroscope Imaging of Low-Grade Glioma. Front. Oncol. 2021, 12, 668656. [Google Scholar] [CrossRef]
- Lacroix, M.; Abi-Said, D.; Fourney, D.R.; Gokaslan, Z.L.; Shi, W.; DeMonte, F.; Lang, F.F.; McCutcheon, I.E.; Hassenbusch, S.J.; Holland, E.; et al. A multivariate analysis of 416 patients with glioblastoma multiforme: Prognosis, extent of resection, and survival. J. Neurosurg. 2001, 95, 190–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, J.S.; Chang, E.F.; Lamborn, K.R.; Chang, S.M.; Prados, M.D.; Cha, S.; Tihan, T.; Vandenberg, S.; McDermott, M.W.; Berger, M.S. Role of extent of resection in the long-term outcome of low-grade hemispheric gliomas. J. Clin. Oncol. 2008, 26, 1338–1345. [Google Scholar] [CrossRef]
- Sanai, N.; Berger, M.S. Glioma extent of resection and its impact on patient outcome. Neurosurgery 2008, 62, 753–764; discussion 264–266. [Google Scholar] [CrossRef] [Green Version]
- Grabowski, M.M.; Recinos, P.F.; Nowacki, A.S.; Schroeder, J.L.; Angelov, L.; Barnett, G.H.; Vogelbaum, M.A. Residual tumor volume versus extent of resection: Predictors of survival after surgery for glioblastoma. J. Neurosurg. 2014, 121, 1115–1123. [Google Scholar] [CrossRef]
- Petrecca, K.; Guiot, M.C.; Panet-Raymond, V.; Souhami, L. Failure pattern following complete resection plus radiotherapy and temozolomide is at the resection margin in patients with glioblastoma. J. Neuro-Oncol. 2013, 111, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Aabedi, A.A.; Young, J.S.; Zhang, Y.; Ammanuel, S.; Morshed, R.A.; Dalle Ore, C.; Brown, D.; Phillips, J.J.; Oberheim Bush, N.A.; Taylor, J.W.; et al. Association of Neurological Impairment on the Relative Benefit of Maximal Extent of Resection in Chemoradiation-Treated Newly Diagnosed Isocitrate Dehydrogenase Wild-Type Glioblastoma. Neurosurgery 2022, 90, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Gately, L.; McLachlan, S.A.; Dowling, A.; Philip, J. Life beyond a diagnosis of glioblastoma: A systematic review of the literature. J. Cancer Surviv. Res. Pract. 2017, 11, 447–452. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
OS HRs Pooled Meta-Analysis.

Figure 2.
A 56-year-old female suffered a single seizure (speech articulation impairment lasting 10 min). The upper figures (A,B) show pre-operative T1 gadolinium-enhanced MRIs of a Glioblastoma infiltrating the left supramarginal gyrus. The patient was operated on through an awake craniotomy and direct language mapping (C,D). Since the mapping did not show activation areas on the supramarginal gyrus, a complete gyrus resection was performed. (E) The post-operative MRI confirmed the complete resection not only of the tumor but also of the gyrus. Post-operatively, the patient did not experience any speech disturbances.
Figure 2.
A 56-year-old female suffered a single seizure (speech articulation impairment lasting 10 min). The upper figures (A,B) show pre-operative T1 gadolinium-enhanced MRIs of a Glioblastoma infiltrating the left supramarginal gyrus. The patient was operated on through an awake craniotomy and direct language mapping (C,D). Since the mapping did not show activation areas on the supramarginal gyrus, a complete gyrus resection was performed. (E) The post-operative MRI confirmed the complete resection not only of the tumor but also of the gyrus. Post-operatively, the patient did not experience any speech disturbances.


{kind=link}
{kind=link}
Table 1.
Data of clinical studies. The table shows data collected from clinical studies. Pre T1c vol (cc): pre-operative T1w plus gadolinium tumor volume; Ependyma: involvement of ventricular of periventricular white matter; Intraop Methods: intraoperative methods; NA: not available; iMRI: intraoperative MRI; IONM: intraoperative neurophysiological monitoring; GTR: gross total resection; SMR: supramarginal resection; i-CT: intraoperative CT scan; i-US: intraoperative ultrasound.
Table 1.
Data of clinical studies. The table shows data collected from clinical studies. Pre T1c vol (cc): pre-operative T1w plus gadolinium tumor volume; Ependyma: involvement of ventricular of periventricular white matter; Intraop Methods: intraoperative methods; NA: not available; iMRI: intraoperative MRI; IONM: intraoperative neurophysiological monitoring; GTR: gross total resection; SMR: supramarginal resection; i-CT: intraoperative CT scan; i-US: intraoperative ultrasound.
| Authors | Definition of Useful SMR | Impact on OS | Pre T1c Vol (cc) | Location | Ependyma | Intraop Methods | Functional Outcomes | Conclusions |
|---|---|---|---|---|---|---|---|---|
| Yan J-L et al., 2017 | Resection of DTI anisotropic component (q) > 89% | ≈100 days more | 46 ± 30 | 10 in Eloquent Areas, 12 Near-Eloquent, and 9 Non-Eloquent | NA | NA | NA | DTI anisotropic q component resection is related to better PFS |
| Tripathi S et al., 2021 | Resection of FLAIR volume beyond T1c: Highly diffuse: 30–99%; Moderately diffuse: 10–60%; and Nodular: 10–29% | Nearly double survival | 36.2 | NA | Worse Survival | NA | NA | Moderately- and highly-diffuse wtIDH gliomas benefited from SMR |
| Vivas-Buitrago T et al., 2021 | 20 to 50% FLAIR volume resection beyond T1c | Increased without time definition | 36.2 | No effect on OS | Worse Survival | NA | NA | A FLAIR resection of at least 20% but less than 60% is associated with improved OS |
| Roh et al., 2020 | Frontal/temporal lobectomy on non-dominant hemisphere | ≈36 months more | 61.1 Frontal location and 41.9 Temporal Location | NA | NA | Tractography, neuronavigation, and 5-ALA | No difference in post-KPS | Non-dominant side GTR plus lobectomy is associated with a better OS and PFS without decreasing performance |
| Li et al., 2016 | Resection of 53.21% of FLAIR beyond T1c | ≈5 months more | 31.0 (0.3–186.3) | NA | NA | IONM and awake surgery | More motor deficits if FLAIR EOR < 53.21% | Resection of a minimum of 53.21% of FLAIR beyond T1c is associated with improved OS |
| Aabedi et al., 2021 | No advantage was found in the NCE group | None | 28.8 (0.5–172.1) | 37.7% Frontal, 32.0% Temporal, 20.1% Parietal, 19% Occipital, and 0.4% Insula | NA | NA | Post-operative impairment was the only factor affecting OS | Post-operative neurological impairment was the only factor affecting OS |
| Certo et al., 2020 | Resection of tumoral FLAIR volume beyond T1c | NA | 54.9 (33.4–89.7) | 17 in Eloquent Areas, 29 Near-Eloquent, and 22 Non-Eloquent | NA | 5-ALA, neuronavigation, IONM, i-CT, and i-US | No difference in post-KPS | FLAIRectomy was associated with improved OS |
| Esquenazi et al., 2017 | Resection beyond T1c edges | ≈37.5 months more | 35.5 (0.4–107) | 33% Frontal, 42% Temporal, 22% Parietal, an d3% Occipital | NA | Neuronavigation | NA | The subpial technique permitted an SMR with an improved OS, without new deficits |
| Eyopoglu et al., 2016 | Resection until 5-ALA is not detectable anymore (DIVA Technique) | ≈4.5 months more | 30 ± 24 | Advantages in Non-Eloquent and Near-Eloquent areas | NA | IONM, 5-ALA, and iMRI | No difference with control-group | DIVA technique was associated with better OS in non-eloquent and near-eloquent areas |
| Gleen et al., 2018 | Resection of 1 cm beyond T1c | ≈13 months more | 39 (until 120) | Temporal | NA | Awake surgery | No difference between GTR and SMR groups | Temporal SMR was associated with better OS and PFS |
| Mampre et al., 2018 | Resection beyond T1c edges | None | 31.9 (13.9–56.1) | NA | NA | IONM and awake surgery | No significant correlation with FLAIR resection | Post-operative FLAIR volume was not associated either with PFS or OS |
| Pessina et al., 2017 | Maximal safe resection of FLAIR volume | ≈12.6 months more | 59.1 (9.1–399.4) | 20 in Eloquent areas, 198 Near-Eloquent, and 64 Non-Eloquent | NA | IONM, iUS | No difference between GTR and STR groups | A >45% resection of FLAIR volume was associated with significantly improved OS |
| Shah et al., 2020 | Lobectomy in right frontal, temporal occipital, and left occipital lobes | ≈16 months more | NA | 59.5% Temporal, 25% Occipital, and 15.6% Frontal | NA | NA | No difference in post-KPS | Lobectomy in case of non-eloquent areas was associated with improved OS |
| Altieri et al., 2019 | Altered signal intensity in FLAIR sequences | None | 23.14 (0–106.56) | NA | NA | IONM and 5-ALA | NA | Resection of FLAIR areas did not affect Glioblastoma patients’ OS |
| Aldave et al., 2013 | Resection until 5-ALA is not detectable anymore | ≈9.5 months more | 43.2 | NA | NA | IONM and 5-ALA | Non-significant worse functional outcome | The absence of fluorescent residue was associated with improved OS |
| Schneider et al., 2019 | Anterior temporal lobectomy | ≈12 months more | ≈30 | Temporal | NA | 5-ALA | No difference in post-KPS | Anterior temporal lobectomy was linked to lingering OS and PFS |
| Figueroa et al., 2020 | Minimally invasive anterior temporal lobectomy | No difference | NA | Temporal | NA | IONM | No difference in post-KPS | Minimally invasive anterior temporal lobectomy was a feasible and safe technique |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Guerrini, F.; Roca, E.; Spena, G. Supramarginal Resection for Glioblastoma: It Is Time to Set Boundaries! A Critical Review on a Hot Topic. Brain Sci. 2022, 12, 652. https://doi.org/10.3390/brainsci12050652
AMA Style
Guerrini F, Roca E, Spena G. Supramarginal Resection for Glioblastoma: It Is Time to Set Boundaries! A Critical Review on a Hot Topic. Brain Sciences. 2022; 12(5):652. https://doi.org/10.3390/brainsci12050652
Chicago/Turabian StyleGuerrini, Francesco, Elena Roca, and Giannantonio Spena. 2022. "Supramarginal Resection for Glioblastoma: It Is Time to Set Boundaries! A Critical Review on a Hot Topic" Brain Sciences 12, no. 5: 652. https://doi.org/10.3390/brainsci12050652
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.