
Factors Related to Hemifacial Spasm Recurrence in Patients Undergoing Microvascular Decompression—A Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Review Question
2.2. Inclusion Criteria and Outcome Measure
- −
- Demographic and clinical data: sex, age at surgery, affected side, reported improvement after surgery, presence of post-op facial weakness, symptoms duration (less or more than 2 years);
- −
- Radiological data: offender vessel (AICA, PICA, VA, veins, multiple vessels).
- −
- Intraoperative neurophysiological monitoring data: lateral spread response (LSR) (if disappearing or being present after surgery).
2.3. Statistical Analysis
3. Results
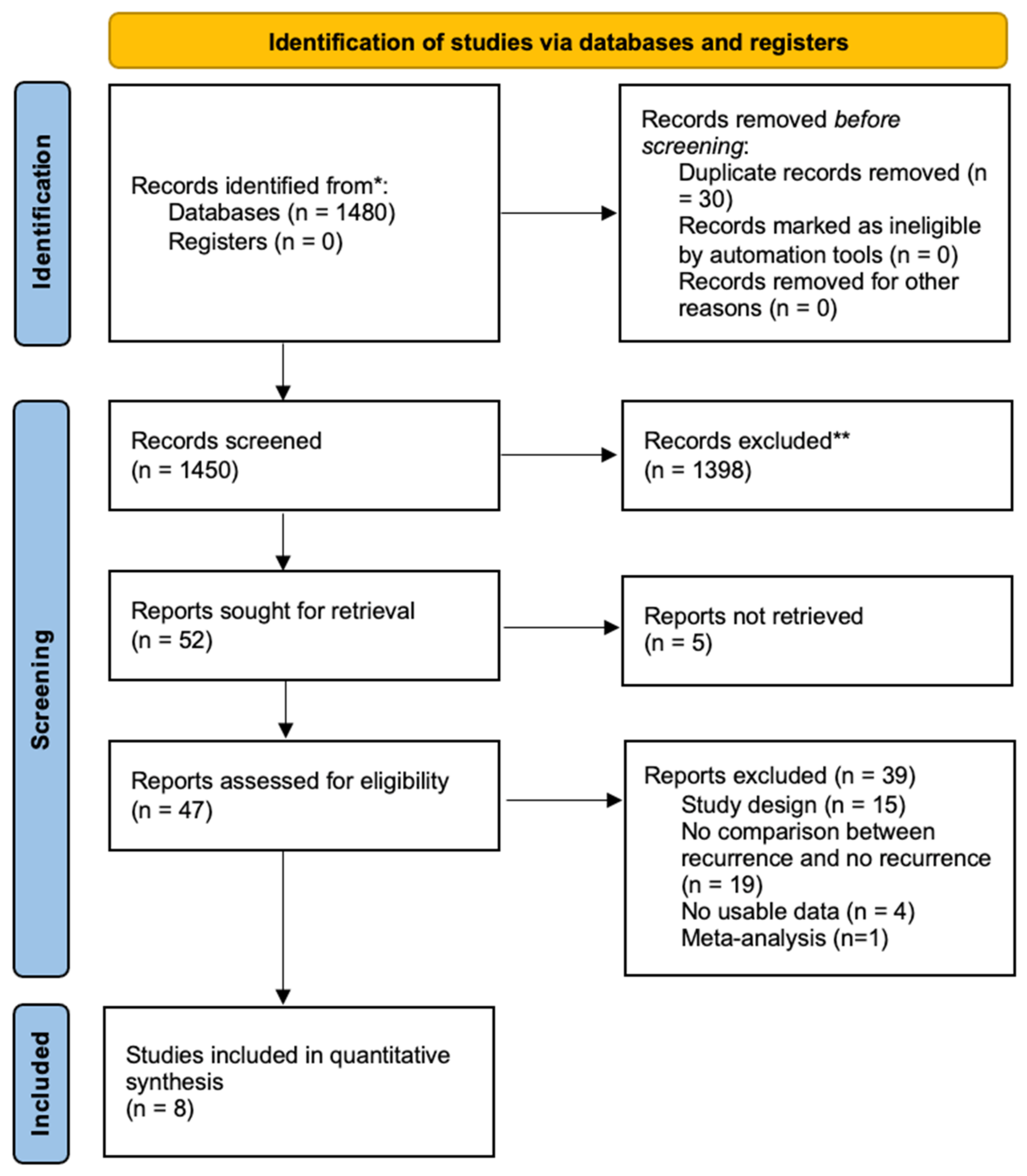
3.1. Systematic Review
3.2. Meta-Analysis
4. Discussion
4.1. Hemifacial Spasm: An Overview
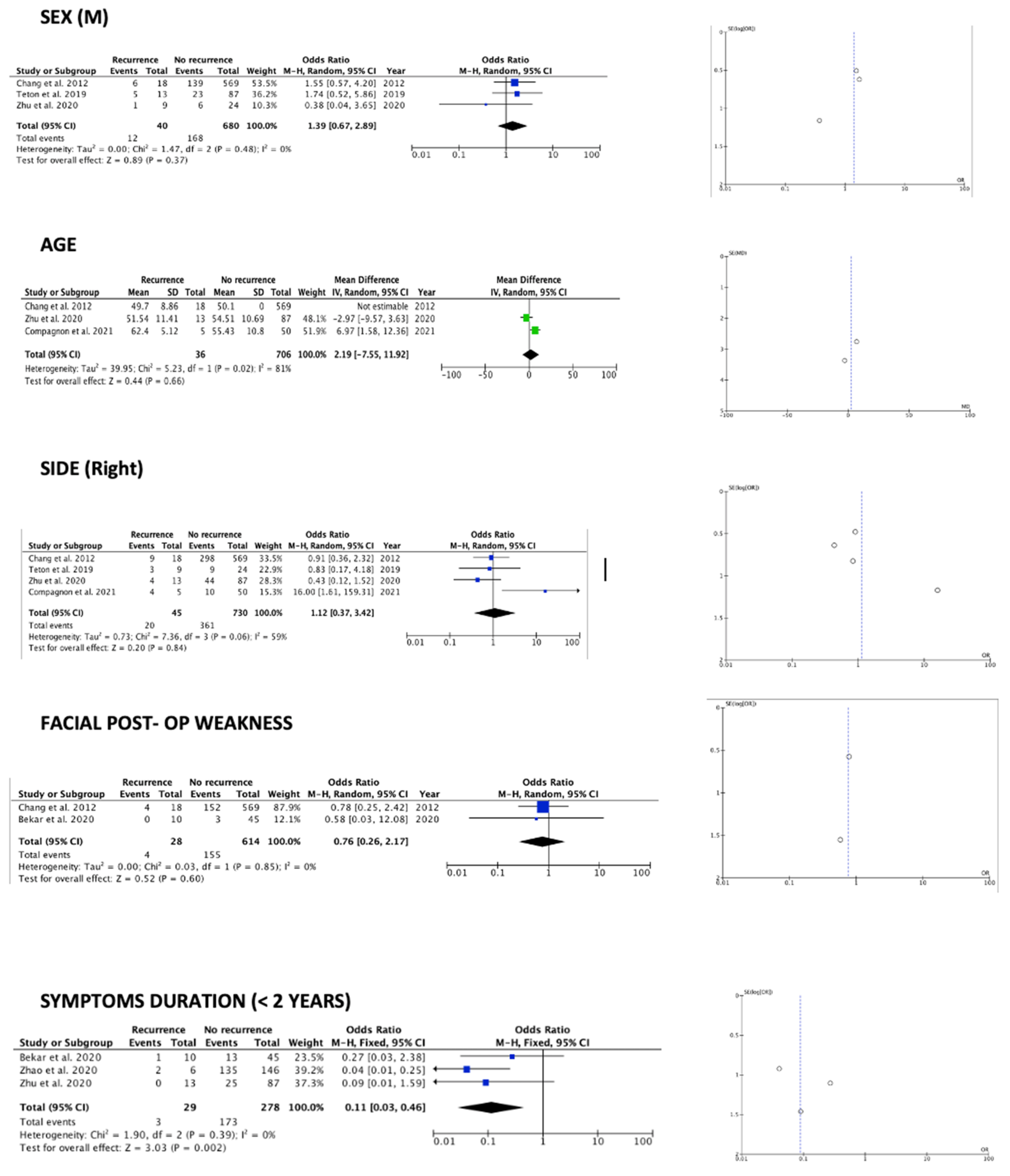
4.1.1. Demographic and Clinical Data
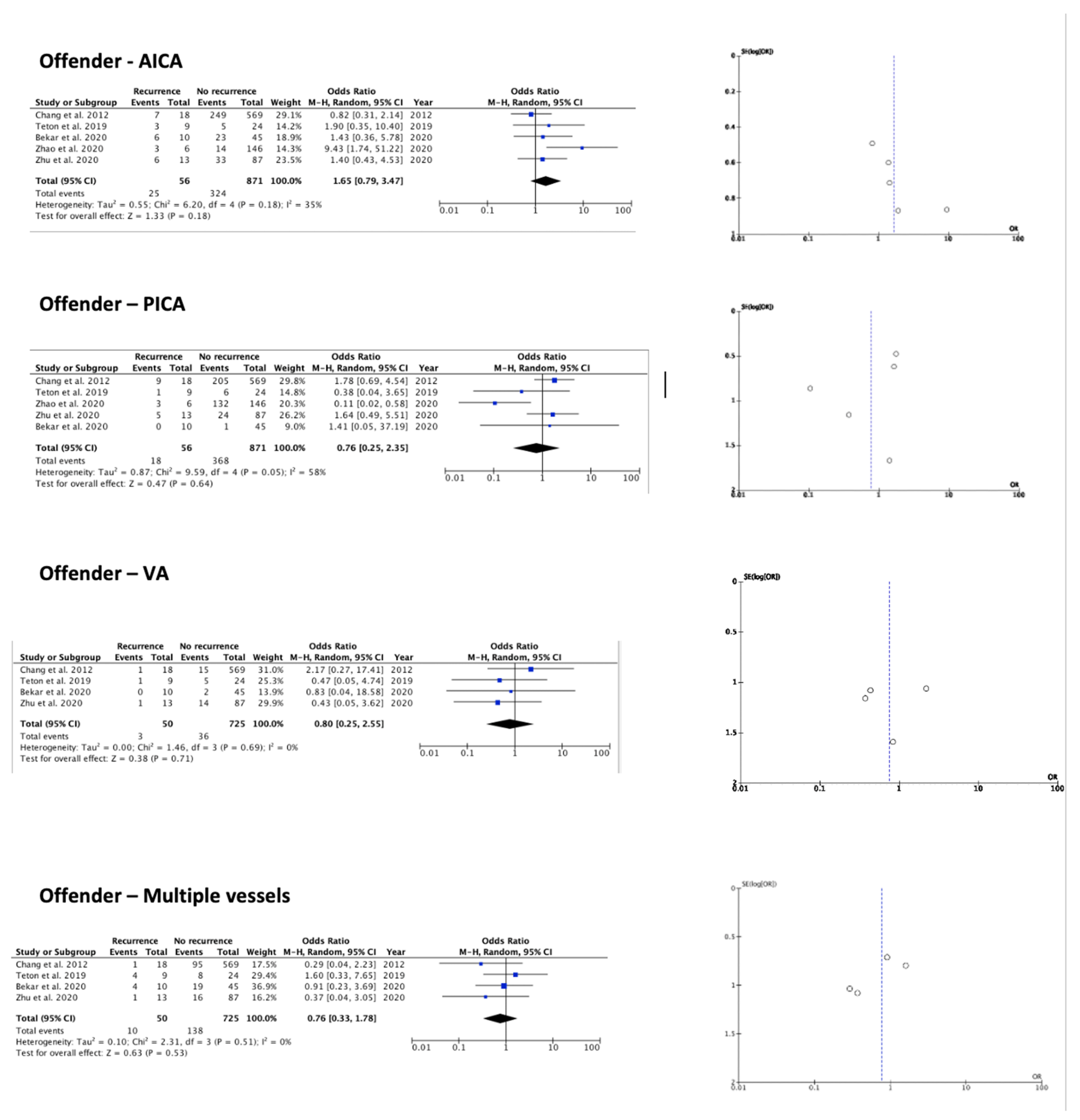
4.1.2. Radiological Data
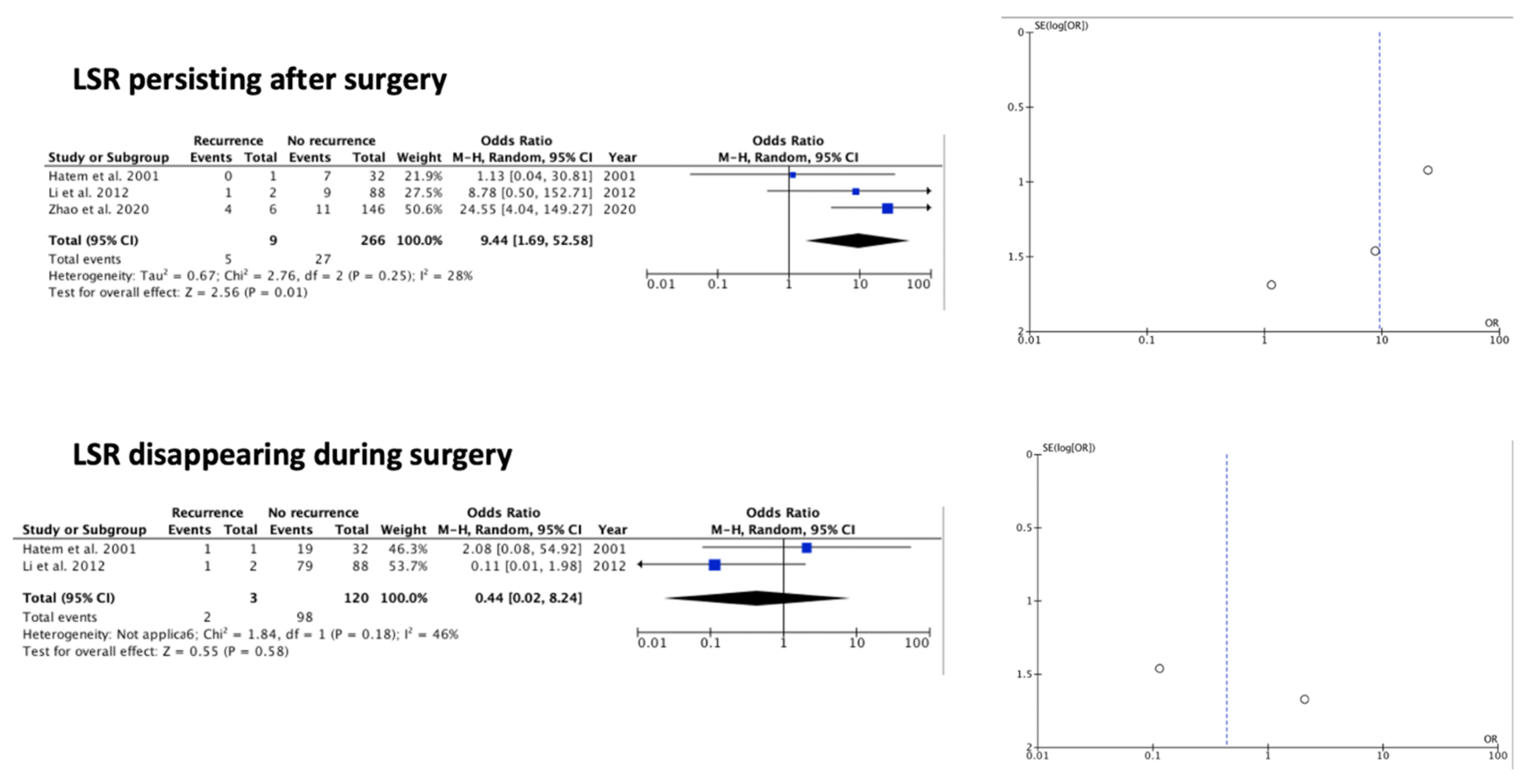
4.1.3. Intraoperative Neurophysiological Data
4.1.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nilsen, B.; Le, K.D.; Dietrichs, E. Prevalence of hemifacial spasm in Oslo, Norway. Neurology 2004, 63, 1532–1533. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Davidson, A.L.; Pan, T.; Jankovic, J. Asian over-representation among patients with hemifacial spasm compared to patients with cranial-cervical dystonia. J. Neurol. Sci. 2010, 298, 61–63. [Google Scholar] [CrossRef] [PubMed]
- Tan, E.K.; Chan, L.L. Young onset hemifacial spasm. Acta Neurol. Scand. 2006, 114, 59–62. [Google Scholar] [CrossRef] [PubMed]
- Abbruzzese, G.; Berardelli, A.; Defazio, G. Hemifacial spasm. Handb. Clin. Neurol. 2011, 100, 675–680. [Google Scholar] [CrossRef] [PubMed]
- Chaudhry, N.; Srivastava, A.; Joshi, L. Hemifacial spasm: The past, present and future. J. Neurol. Sci. 2015, 356, 27–31. [Google Scholar] [CrossRef]
- Yaltho, T.C.; Jankovic, J. The many faces of hemifacial spasm: Differential diagnosis of unilateral facial spasms. Mov. Disord. 2011, 26, 1582–1592. [Google Scholar] [CrossRef]
- Bendtsen, L.; Zakrzewska, J.M.; Abbott, J.A.; Braschinsky, M.; Di Stefano, G.; Donnet, A.; Eide, P.K.; Leal, P.R.L.; Maarbjerg, S.; May, A.; et al. European Academy of Neurology guideline on trigeminal neuralgia. Eur. J. Neurol. 2019, 26, 831–849. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J. Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Hatem, J.; Sindou, M.; Vial, C. Intraoperative monitoring of facial EMG responses during microvascular decompression for hemifacial spasm. Prognostic value for long-term outcome: A study in a 33-patient series. Br. J. Neurosurg. 2001, 15, 496–499. [Google Scholar] [CrossRef]
- Chang, W.S.; Chung, J.C.; Kim, J.P.; Chung, S.S.; Chang, J.W. Delayed recurrence of hemifacial spasm after successful microvascular decompression: Follow-up results at least 5 years after surgery. Acta Neurochir. 2012, 154, 1613–1619. [Google Scholar] [CrossRef]
- Zhu, W.; Shen, J.; Tang, T.; Chang, B.; Li, S.; Chen, M. Evaluation of pre-operative neuroimaging characteristics in patients with primary hemifacial spasm as a prognostic factor of microvascular decompression. Clin. Neurol. Neurosurg. 2020, 195, 105874. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Zhang, Y.; Zhu, H.; Li, Y. Prognostic value of intra-operative abnormal muscle response monitoring during microvascular decompression for long-term outcome of hemifacial spasm. J. Clin. Neurosci. 2012, 19, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Teton, Z.E.; Blatt, D.; Holste, K.; Raslan, A.M.; Burchiel, K.J. Utilization of 3D imaging reconstructions and assessment of symptom-free survival after microvascular decompression of the facial nerve in hemifacial spasm. J. Neurosurg. 2019, 133, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Bekar, A.; Kuytu, T.; Turkkan, A.; Altunyuva, O.; Eser Ocak, P. The Efficacy and Safety of Microvascular Decompression for Hemifacial Spasm: A Retrospective Analysis of Surgical Outcomes and Complications. Turk. Neurosurg. 2020, 30, 231–236. [Google Scholar] [CrossRef]
- Compagnon, C.; Labrousse, M.; Brenet, E.; Chays, A.; Bazin, A.; Kleiber, J.C.; Dubernard, X. Efficacy and Complications of Microsurgical Neurovascular Decompression in 55 Patients With Hemifacial Spasm. Otolaryngol. Head Neck Surg. 2021, 164, 1299–1306. [Google Scholar] [CrossRef]
- Zhao, K.; Wang, J.; Liu, W.; Zhang, J.; Shu, K.; Lei, T. Flat-shaped posterior cranial fossa was associated with poor outcomes of microvascular decompression for primary hemifacial spasm. Acta Neurochir. 2020, 162, 2801–2809. [Google Scholar] [CrossRef]
- Huh, R.; Han, I.B.; Moon, J.Y.; Chang, J.W.; Chung, S.S. Microvascular decompression for hemifacial spasm: Analyses of operative complications in 1582 consecutive patients. Surg. Neurol. 2008, 69, 153–157. [Google Scholar] [CrossRef]
- Jannetta, P.J.; Abbasy, M.; Maroon, J.C.; Ramos, F.M.; Albin, M.S. Etiology and definitive microsurgical treatment of hemifacial spasm. Operative techniques and results in 47 patients. J. Neurosurg. 1977, 47, 321–328. [Google Scholar] [CrossRef]
- Janetta, P.J. Cranial Rhizopathies. In Neurological Surgery, 3rd ed.; W.B. Saunders: Philadelphia, PA, USA, 1990; pp. 4169–4182. [Google Scholar]
- Hanakita, J.; Kondo, A. Serious complications of microvascular decompression operations for trigeminal neuralgia and hemifacial spasm. Neurosurgery 1988, 22, 348–352. [Google Scholar] [CrossRef]
- Miller, L.E.; Miller, V.M. Safety and effectiveness of microvascular decompression for treatment of hemifacial spasm: A systematic review. Br. J. Neurosurg. 2012, 26, 438–444. [Google Scholar] [CrossRef]
- Chen, F.; Niu, Y.; Meng, F.; Xu, P.; Zhang, C.; Xue, Y.; Wu, S.; Wang, L. Recurrence Rates After Microvascular Decompression in Patients with Primary Trigeminal Neuralgia and Its Influencing Factors: A Systematic Review and Meta-Analysis Based on 8172 Surgery Patients. Front. Neurol. 2021, 12, 738032. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Park, S.K.; Lee, S.; Lee, J.A.; Park, K. Lateral spread response of different facial muscles during microvascular decompression in hemifacial spasm. Clin. Neurophysiol. 2021, 132, 2503–2509. [Google Scholar] [CrossRef] [PubMed]
- Sethi, K.D.; Rodriguez, R.; Olayinka, B. Satisfaction with botulinum toxin treatment: A cross-sectional survey of patients with cervical dystonia. J. Med. Econ. 2012, 15, 419–423, reprinted in J. Med. Econ. 2013, 16, 327. [Google Scholar] [CrossRef] [PubMed]
- Chan, R.W.; Chiang, Y.H.; Chen, Y.Y.; Chen, Y.C.; Lin, J.H.; Tsou, Y.S. Predicting Early Loss of Lateral Spread Response before Decompression in Hemifacial Spasm Surgery. Life 2021, 12, 40. [Google Scholar] [CrossRef] [PubMed]
- Trosch, R.M.; Misra, V.P.; Maisonobe, P.; Om, S. Impact of abobotulinumtoxinA on the clinical features of cervical dystonia in routine practice. Clin. Park. Relat. Disord. 2020, 3, 100063. [Google Scholar] [CrossRef] [PubMed]
- Lefaucheur, J.P.; Ben, D.N.; Sangla, S.; Le Guerinel, C. Diagnosis of primary hemifacial spasm. Neurochirurgie 2018, 64, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Hermier, M. Imaging of hemifacial spasm. Neurochirurgie 2018, 64, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Rosenstengel, C.; Matthes, M.; Baldauf, J.; Fleck, S.; Schroeder, H. Hemifacial spasm: Conservative and surgical treatment options. Dtsch. Arztebl. Int. 2012, 109, 667–673. [Google Scholar] [CrossRef]
- Lu, A.Y.; Yeung, J.T.; Gerrard, J.L.; Michaelides, E.M.; Sekula, R.F., Jr.; Bulsara, K.R. Hemifacial spasm and neurovascular compression. Sci. World J. 2014, 2014, 349319. [Google Scholar] [CrossRef]
- Sindou, M.; Mercier, P. Microvascular decompression for hemifacial spasm: Surgical techniques and intraoperative monitoring. Neurochirurgie 2018, 64, 133–143. [Google Scholar] [CrossRef]
- Green, K.E.; Rastall, D.; Eggenberger, E. Treatment of Blepharospasm/Hemifacial Spasm. Curr. Treat. Options Neurol. 2017, 19, 41. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name | Type of Study | Total Number of Patients (Recurrence/No Recurrence) |
|---|---|---|
| Hatem et al., 2001 [9] | Prospective | 33 (1/32) |
| Chang et al., 2012 [10] | Retrospective | 587 (18/569) |
| Li et al., 2012 [12] | Retrospective | 90 (2/88) |
| Teton et al., 2019 [13] | Retrospective | 33 (9/24) |
| Bekar et al., 2020 [14] | Retrospective | 55 (10/45) |
| Zhao et al., 2020 [16] | Retrospective | 152 (6/143) |
| Zhu et al., 2020 [11] | Prospective | 100 (13/87) |
| Compagnon et al., 2021 [15] | Retrospective | 55 (5/50) |
| Factor | Or | 95% CI | p Value | I2 | I2 p Value |
|---|---|---|---|---|---|
| Demographic and clinical data | |||||
| Sex (M) | 1.39 | 0.67–2.89 | 0.37 | 0 | 0.48 |
| Mean age at surgery (years) | 2.19 | −7.55–11.92 | 0.66 | 81% | 0.02 |
| Side (Right) | 1.12 | 0.37–3.42 | 0.84 | 59% | 0.06 |
| Facial post-op weakness | 0.76 | 0.26–2.17 | 0.6 | 0 | 0.85 |
| Symptoms duration (<2 years) | 0.11 | 0.03–0.46 | 0.02 | 0 | 0.39 |
| Radiological data (offender vessel) | |||||
| AICA | 1.65 | 0.79–3.47 | 0.18 | 35% | 0.18 |
| PICA | 0.76 | 0.25–2.35 | 0.64 | 58% | 0.05 |
| VA | 0.80 | 0.25–2.55 | 0.71 | 0% | 0.69 |
| Multiple veins | 0.76 | 0.33–1.78 | 0.53 | 0% | 0.51 |
| Intraoperative neurophysiological data | |||||
| LSR disappearing during surgery | 0.44 | 0.02–8.24 | 0.58 | 46% | 0.18 |
| LSR present after surgery | 9.44 | 1.69–52.58 | 0.01 | 28% | 0.25 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Menna, G.; Battistelli, M.; Rapisarda, A.; Izzo, A.; D’Ercole, M.; Olivi, A.; Montano, N. Factors Related to Hemifacial Spasm Recurrence in Patients Undergoing Microvascular Decompression—A Systematic Review and Meta-Analysis. Brain Sci. 2022, 12, 583. https://doi.org/10.3390/brainsci12050583
Menna G, Battistelli M, Rapisarda A, Izzo A, D’Ercole M, Olivi A, Montano N. Factors Related to Hemifacial Spasm Recurrence in Patients Undergoing Microvascular Decompression—A Systematic Review and Meta-Analysis. Brain Sciences. 2022; 12(5):583. https://doi.org/10.3390/brainsci12050583
Chicago/Turabian StyleMenna, Grazia, Marco Battistelli, Alessandro Rapisarda, Alessandro Izzo, Manuela D’Ercole, Alessandro Olivi, and Nicola Montano. 2022. "Factors Related to Hemifacial Spasm Recurrence in Patients Undergoing Microvascular Decompression—A Systematic Review and Meta-Analysis" Brain Sciences 12, no. 5: 583. https://doi.org/10.3390/brainsci12050583