
Influence of Weight Loss on Cognitive Functions: A Pilot Study of a Multidisciplinary Intervention Program for Obesity Treatment

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
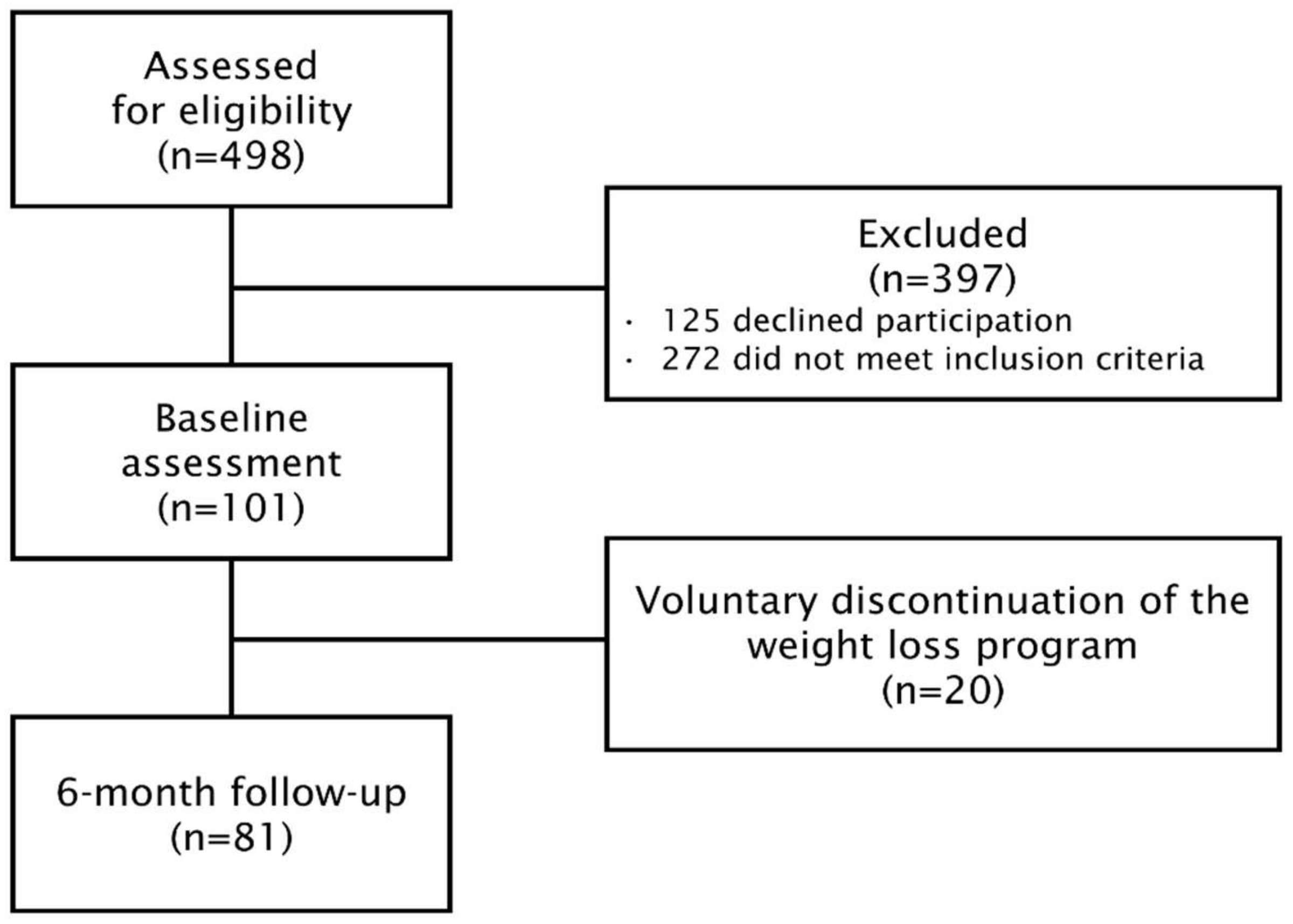
2.1. Population and Study Design
2.2. Demographic and Clinical Variables
2.3. Cognitive Assessments
2.4. Statistical Analysis
3. Results
3.1. Population Characteristics
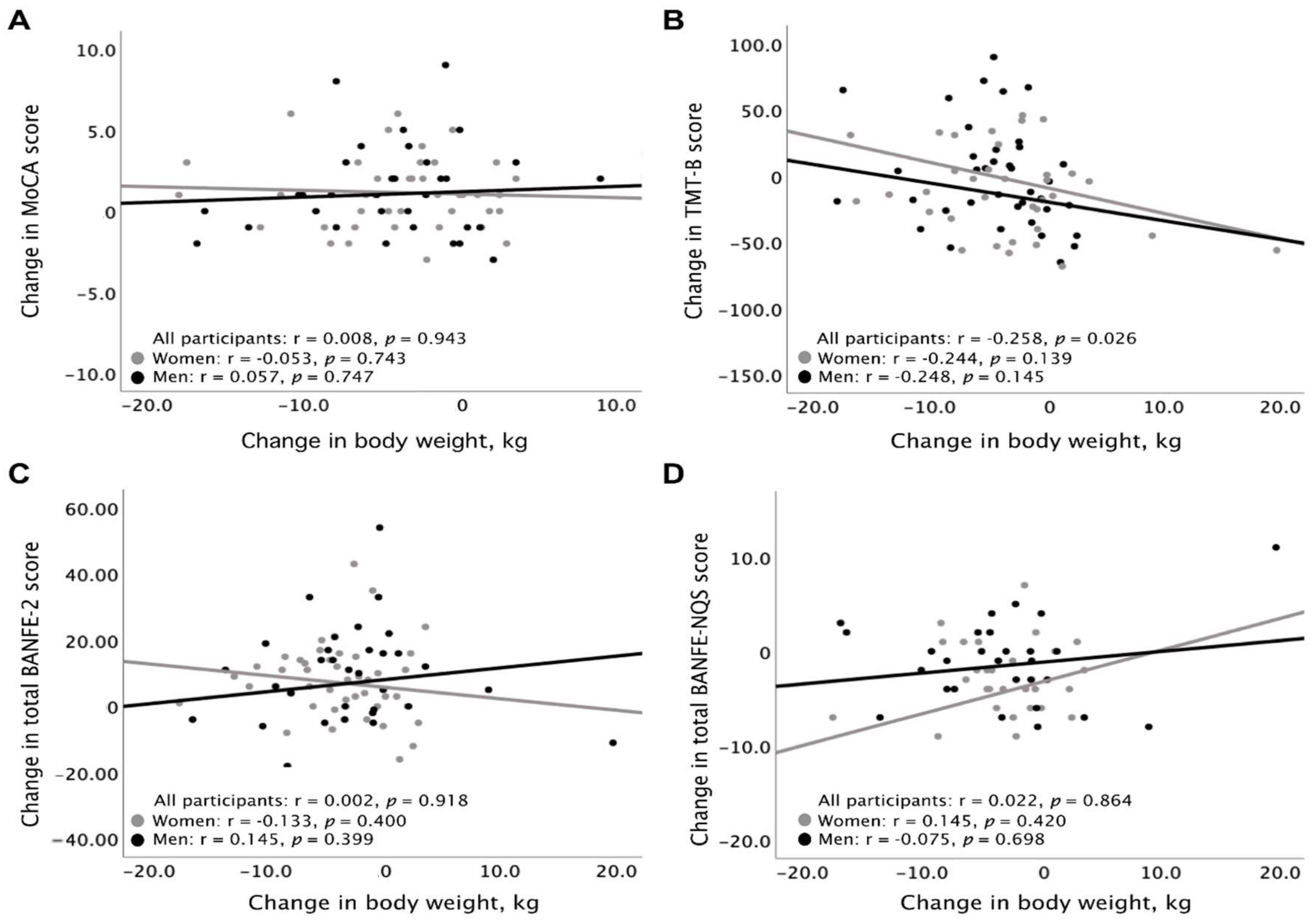
3.2. Cognitive Functioning
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Prospective Studies Collaboration; Whitlock, G.; Lewington, S.; Sherliker, P.; Clarke, R.; Emberson, J.; Halsey, J.; Qizilbash, N.; Collins, R.; Peto, R. Faculty Opinions recommendation of Body-mass index and cause-specific mortality in 900,000 adults: Collaborative analyses of 57 prospective studies. Fac. Opin. Post-Publ. Peer Rev. Biomed. Lit. 2009, 373, 1083–1096. [Google Scholar] [CrossRef]
- Held, M.; Mittnacht, M.; Kolb, M.; Karl, S.; Jany, B. Pulmonary and Cardiac Function in Asymptomatic Obese Subjects and Changes following a Structured Weight Reduction Program: A Prospective Observational Study. PLoS ONE 2014, 9, e107480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luppino, F.S.; de Wit, L.M.; Bouvy, P.F.; Stijnen, T.; Cuijpers, P.; Penninx, B.W.; Zitman, F.G. Overweight, obesity, and depression: A systematic review and meta-analysis of longitudinal studies. Arch Gen. Psychiatry 2010, 67, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Beydoun, M.A.; Wang, Y. Obesity and central obesity as risk factors for incident dementia and its subtypes: A systematic review and meta-analysis. Obes. Rev. 2008, 9, 204–218. [Google Scholar] [CrossRef] [PubMed]
- Gustafson, D.; Rothenberg, E.; Blennow, K.; Steen, B.; Skoog, I. An 18-Year Follow-up of Overweight and Risk of Alzheimer Disease. Arch. Intern. Med. 2003, 163, 1524–1528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dahl, A.K.; Hassing, L.B.; Fransson, E.; Gatz, M.; A Reynolds, C.; Pedersen, N.L. Body mass index across midlife and cognitive change in late life. Int. J. Obes. 2012, 37, 296–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loef, M.; Walach, H. Midlife obesity and dementia: Meta-analysis and adjusted forecast of dementia prevalence in the united states and china. Obesity 2013, 21, E51–E55. [Google Scholar] [CrossRef] [PubMed]
- Whitmer, R.A.; Gunderson, E.P.; Barrett-Connor, E.; Quesenberry, C.P., Jr.; Yaffe, K. Obesity in middle age and future risk of dementia: A 27 year longitudinal population based study. BMJ 2005, 330, 1360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, E.; Hay, P.; Campbell, L.; Trollor, J.N. A review of the association between obesity and cognitive function across the lifespan: Implications for novel approaches to prevention and treatment. Obes. Rev. 2011, 12, 740–755. [Google Scholar] [CrossRef] [PubMed]
- Barrett-Connor, E.; Edelstein, S.L.; Corey-Bloom, J.; Wiederholt, W.C. Weight Loss Precedes Dementia in Community-Dwelling Older Adults. J. Am. Geriatr. Soc. 1996, 44, 1147–1152. [Google Scholar] [CrossRef] [PubMed]
- Hughes, T.F.; Borenstein, A.R.; Schofield, E.; Wu, Y.; Larson, E.B. Association between late-life body mass index and dementia: The Kame Project. Neurology 2009, 72, 1741–1746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willmann, C.; Brockmann, K.; Wagner, R.; Kullmann, S.; Preissl, H.; Schnauder, G.; Maetzler, W.; Gasser, T.; Berg, D.; Eschweiler, G.W.; et al. Insulin sensitivity predicts cognitive decline in individuals with prediabetes. BMJ Open Diabetes Res. Care 2020, 8, e001741. [Google Scholar] [CrossRef] [PubMed]
- Hao, Z.; Wu, B.; Wang, D.; Liu, M. Association between metabolic syndrome and cognitive decline: A systematic review of prospective population-based studies. Acta Neuropsychiatr. 2011, 23, 69–74. [Google Scholar] [CrossRef]
- Qin, J.; He, Z.; Wu, L.; Wang, W.; Lin, Q.; Lin, Y.; Zheng, L. Prevalence of mild cognitive impairment in patients with hypertension: A systematic review and meta-analysis. Hypertens. Res. 2021, 44, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Alster, P.; Dunalska, A.; Migda, B.; Madetko, N.; Królicki, L. The Rate of Decrease in Brain Perfusion in Progressive Supranuclear Palsy and Corticobasal Syndrome May Be Impacted by Glycemic Variability—A Pilot Study. Front. Neurol. 2021, 12, 767480. [Google Scholar] [CrossRef]
- Shetty, A.K.; Madhu, L.N.; Kodali, M. Promise of metformin for preventing age-related cognitive dysfunction. Neural Regen. Res. 2022, 17, 503. [Google Scholar] [CrossRef]
- Yang, Y.; Shields, G.; Guo, C.; Liu, Y. Executive function performance in obesity and overweight individuals: A meta-analysis and review. Neurosci. Biobehav. Rev. 2018, 84, 225–244. [Google Scholar] [CrossRef] [PubMed]
- Prickett, C.; Brennan, L.; Stolwyk, R. Examining the relationship between obesity and cognitive function: A systematic literature review. Obes. Res. Clin. Pr. 2015, 9, 93–113. [Google Scholar] [CrossRef] [PubMed]
- Diamond, A Executive functions. Annu. Rev. Psychol. 2013, 64, 135–168. [CrossRef] [PubMed] [Green Version]
- Stuss, D.T.; Alexander, M.P. Executive functions and the frontal lobes: A conceptual view. Psychol. Res. 2000, 63, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Gettens, K.M.; Gorin, A.A. Executive function in weight loss and weight loss maintenance: A conceptual review and novel neuropsychological model of weight control. J. Behav. Med. 2017, 40, 687–701. [Google Scholar] [CrossRef] [PubMed]
- Ho, M.-C.; Chen, V.C.-H.; Chao, S.-H.; Fang, C.-T.; Liu, Y.-C.; Weng, J.-C. Neural correlates of executive functions in patients with obesity. PeerJ 2018, 6, e5002. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, A.J.; Shiri-Feshki, M. Rate of progression of mild cognitive impairment to dementia—meta-analysis of 41 robust inception cohort studies. Acta Psychiatr. Scand. 2009, 119, 252–265. [Google Scholar] [CrossRef] [PubMed]
- Hamman, R.F.; Wing, R.R.; Edelstein, S.L.; Lachin, J.M.; Bray, G.A.; Delahanty, L.; Hoskin, M.; Kriska, A.M.; Mayer-Davis, E.J.; Pi-Sunyer, X.; et al. Effect of Weight Loss With Lifestyle Intervention on Risk of Diabetes. Diabetes Care 2006, 29, 2102–2107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wing, R.R.; Lang, W.; Wadden, T.A.; Safford, M.; Knowler, W.C.; Bertoni, A.G.; Hill, J.O.; Brancati, F.L.; Peters, A.; Wagenknecht, L.; et al. Benefits of Modest Weight Loss in Improving Cardiovascular Risk Factors in Overweight and Obese Individuals With Type 2 Diabetes. Diabetes Care 2011, 34, 1481–1486. [Google Scholar] [CrossRef] [Green Version]
- Ma, C.; Avenell, A.; Bolland, M.; Hudson, J.; Stewart, F.; Robertson, C.; Sharma, P.; Fraser, C.; MacLennan, G. Effects of weight loss interventions for adults who are obese on mortality, cardiovascular disease, and cancer: Systematic review and meta-analysis. BMJ 2017, 359, j4849. [Google Scholar] [CrossRef] [Green Version]
- Kolotkin, R.L.; Norquist, J.M.; Crosby, R.D.; Suryawanshi, S.; Teixeira, P.J.; Heymsfield, S.B.; Erondu, N.; Nguyen, A.M. One-year health-related quality of life outcomes in weight loss trial participants: Comparison of three measures. Health Qual. Life Outcomes 2009, 7, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, T.; Dias, G.P.; Thuret, S. Effects of Diet on Brain Plasticity in Animal and Human Studies: Mind the Gap. Neural Plast. 2014, 2014, 1–32. [Google Scholar] [CrossRef] [Green Version]
- Veronese, N.; Facchini, S.; Stubbs, B.; Luchini, C.; Solmi, M.; Manzato, E.; Sergi, G.; Maggi, S.; Cosco, T.; Fontana, L. Weight loss is associated with improvements in cognitive function among overweight and obese people: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2017, 72, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Informe de Resultados de la Encuesta Nacional de Salud y Nutrición–2018. Available online: https://ensanut.insp.mx/encuestas/ensanut2018/doctos/informes/ensanut_2018_informe_final.pdf (accessed on 30 January 2022).
- The Look AHEAD Research Group. Look AHEAD (Action for Health in Diabetes): Design and methods for a clinical trial of weight loss for the prevention of cardiovascular disease in type 2 diabetes. Control Clin Trials. 2003, 24, 610–628. [Google Scholar] [CrossRef]
- Garvey, W.T.; Mechanick, J.I.; Brett, E.M.; Garber, A.J.; Hurley, D.L.; Jastreboff, A.M.; Nadolsky, K.; Pessah-Pollack, R.; Plodkowski, R. Reviewers of the AACE/ACE Obesity Clinical Practice Guidelines. American Association of Clinical Endocrinologists and American College of Endocrinology Comprehensive Clinical Practice Guidelines For Medical Care of Patients With Obesity. Endocr. Pract. 2016, 22 (Suppl. S3), 1–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- López-Alvarenga, J.C.; Vázquez-Velázquez, V.; Arcila-Martínez, D.; Sierra-Ovando, A.E.; González-Barranco, J.; Salín-Pascual, R.J. Accuracy and diagnostic utility of the Hospital Anxiety and Depression Scale (HAD) in a sample of obese Mexican patients. Rev. Investig. Clin. Organo Hosp. Enferm. Nutr. 2003, 54, 403–409. [Google Scholar]
- Aguilar-Navarro, S.G.; Mimenza-Alvarado, A.J.; Palacios-García, A.A.; Samudio-Cruz, A.; Gutiérrez-Gutiérrez, L.A.; Avila-Funes, J.A. Validity and reliability of the Spanish Version of the Montreal Cognitive Assessment (MoCA) for the detection of cognitive impairment in Mexico. Rev. Colomb. Psiquiatr. (Engl. Ed.) 2018, 47, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Flores-Lazaro, J.; Ostrosky-Solís, F.; Lozano, A. Bateria de funciones frontales y ejecutivas: Presentación. Rev. Neuropsicol. Neuropsiquiatría Neurocienc. 2008, 8, 141–158. [Google Scholar]
- Calderón-Garcidueñas, L.; Mukherjee, P.S.; Kulesza, R.J.; Torres-Jardón, R.; Hernández-Luna, J.; Ávila-Cervantes, R.; Macías-Escobedo, E.; González-González, O.; González-Maciel, A.; García-Hernández, K.; et al. Mild Cognitive Impairment and Dementia Involving Multiple Cognitive Domains in Mexican Urbanites. Adv. Alzheimer’s Dis. 2021, 68, 1113–1123. [Google Scholar] [CrossRef]
- Bauer, C.; Moreno-Garcia, M.B.; González-Santos, L.; Concha, L.; Barquera, S.; Barrios, F.A. Child overweight and obesity are associated with reduced executive cognitive performance and brain alterations: A magnetic resonance imaging study in Mexican children. Pediatr. Obes. 2014, 10, 196–204. [Google Scholar] [CrossRef]
- Nishi, S.K.; Babio, N.; Gómez-Martínez, C.; Martínez-González, M.Á.; Ros, E.; Corella, D.; Castañer, O.; Martínez, J.A.; Alonso-Gómez, Á.M.; Wärnberg, J.; et al. Mediterranean, DASH, and MIND Dietary Patterns and Cognitive Function: The 2-Year Longitudinal Changes in an Older Spanish Cohort. Front. Aging Neurosci. 2021, 13, 782067. [Google Scholar] [CrossRef]
- Siervo, M.; Arnold, R.; Wells, J.; Tagliabue, A.; Colantuoni, A.; Albanese, E.; Brayne, C.; Stephan, B. Intentional weight loss in overweight and obese individuals and cognitive function: A systematic review and meta-analysis. Obes. Rev. 2011, 12, 968–983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Northey, J.M.; Cherbuin, N.; Pumpa, K.L.; Smee, D.J.; Rattray, B. Exercise interventions for cognitive function in adults older than 50: A systematic review with meta-analysis. Br. J. Sports Med. 2018, 52, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Cukierman, T.; Gerstein, H.C.; Williamson, J.D. Cognitive decline and dementia in diabetes—Systematic overview of prospective observational studies. Diabetologia 2005, 48, 2460–2469. [Google Scholar] [CrossRef]
- Napoli, N.; Shah, K.; Waters, D.L.; Sinacore, D.R.; Qualls, C.; Villareal, D.T. Effect of weight loss, exercise, or both on cognition and quality of life in obese older adults. Am. J. Clin. Nutr. 2014, 100, 189–198. [Google Scholar] [CrossRef] [Green Version]
- Rehm, J.; Hasan, O.S.M.; Black, S.E.; Shield, K.D.; Schwarzinger, M. Alcohol use and dementia: A systematic scoping review. Alzheimer’s Res. Ther. 2019, 11, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Peters, R.; Peters, J.; Warner, J.; Beckett, N.; Bulpitt, C. Alcohol, dementia and cognitive decline in the elderly: A systematic review. Age Ageing 2008, 37, 505–512. [Google Scholar] [CrossRef] [Green Version]
- Olaithe, M.; Bucks, R.; Hillman, D.; Eastwood, P.R. Cognitive deficits in obstructive sleep apnea: Insights from a meta-review and comparison with deficits observed in COPD, insomnia, and sleep deprivation. Sleep Med. Rev. 2018, 38, 39–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaalema, D.E.; Dube, S.; Potter, A.; Elliott, R.J.; Mahoney, K.; Sigmon, S.C.; Higgins, S.T.; Ades, P.A. The effect of executive function on adherence with a cardiac secondary prevention program and its interaction with an incentive-based intervention. Prev. Med. 2019, 128, 105865. [Google Scholar] [CrossRef]
- Horie, N.C.; Serrao, V.T.; Simon, S.S.; Gascon, M.R.P.; dos Santos, A.X.; Zambone, M.A.; del Bigio de Freitas, M.M.; Cunha-Neto, E.; Marques, E.L.; Halpern, A.; et al. Cognitive Effects of Intentional Weight Loss in Elderly Obese Individuals With Mild Cognitive Impairment. J. Clin. Endocrinol. Metab. 2016, 101, 1104–1112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, W.; Tan, L.; Wang, H.-F.; Tan, M.-S.; Tan, L.; Li, J.-Q.; Zhao, Q.-F.; Yu, J.-T. Education and Risk of Dementia: Dose-Response Meta-Analysis of Prospective Cohort Studies. Mol. Neurobiol. 2015, 53, 3113–3123. [Google Scholar] [CrossRef] [PubMed]
- Baba, Y.; Putzke, J.D.; Whaley, N.R.; Wszolek, Z.K.; Uitti, R.J. Progressive supranuclear palsy: Phenotypic sex differences in a clinical cohort. Mov. Disord. 2006, 21, 689–692. [Google Scholar] [CrossRef]
- Dugger, B.N.; Malek-Ahmadi, M.; Monsell, S.E.; Kukull, W.A.; Woodruff, B.K.; Reiman, E.M.; Beach, T.G.; Wilson, J. A Cross-Sectional Analysis of Late-Life Cardiovascular Factors and Their Relation to Clinically Defined Neurodegenerative Diseases. Alzheimer Dis. Assoc. Disord. 2016, 30, 223–229. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| All Participants | Women | Men | p-Value † | |
|---|---|---|---|---|
| (n = 81) | (n = 45) | (n = 36) | ||
| Age, median (IQR), years | 40.0 (31.5–47) | 40 (31.7–46.2) | 40.0 (31.0–47.0) | 0.99 |
| Education, median (IQR), years | 16 (12–17) | 15 (12.0–17.0) | 16 (12.0–17.0) | 0.99 |
| Socioeconomic status, n (%) | ||||
| Low Middle High | 16 (15.8) 64 (63.4) 21 (20.8) | 9 (14.5) 40 (64.5) 13 (21.0) | 7 (19.9) 24 (61.5) 8 (20.5) | 0.99 |
| Education, n (%) | ||||
| 6 years of education 7 to 12 years of education 13 or more years of education | 15 (14.9) 30 (29.7) 56 (55.4) | 10 (16.1) 20 (32.3) 32 (51.6) | 5 (12.8) 10 (25.6) 24 (61.5) | 0.99 |
| Cigarette smoking, n (%) | ||||
| Absent Mild (≤5 cigarettes/day) Moderate (6–15 cigarettes/day) | 78 (77.2) 18 (17.8) 5 (6.17) | 52 (83.9) 9 (14.5) 1 (1.5) | 26 (66.7) 9 (23.1) 4 (11.1) | 0.99 |
| Alcohol consumption, n (%) | ||||
| Absent Mild (W: 1 d/day, M: 2 d/day) Moderate (W: 2 d/day, M: 3 d/day) | 55 (54.5) 10 (9.9) 36 (44.4) | 41 (66.1) 6 (9.70) 15 (33.3) | 14 (35.9) 4 (10.3) 21 (58.3) | 0.015 |
| Physical activity, n (%) | ||||
| Mild (<600 Mets/week) Moderate (600–1499 Mets/week) Heavy (≥1500 Mets/week) | 42 (41.6) 25 (24.8) 34 (33.7) | 26 (41.9) 18 (29.0) 18 (29.0) | 16 (41.0) 7(17.9) 16 (41.0) | 0.99 |
| Comorbidities, n (%) | ||||
| Metabolic syndrome | 81 (80.2) | 44 (71.0) | 37 (94.9) | 0.045 |
| Hypertension | 43 (53.1) | 22 (35.5) | 27 (69.2) | 0.0015 |
| Prediabetes | 44 (43.6) | 30 (48.9) | 14 (35.9) | 0.99 |
| Type 2 diabetes mellitus | 25 (30.9) | 12 (19.4) | 17 (43.6) | 0.195 |
| Hypertriglyceridemia | 42 (51.9) | 27 (44.3) | 25 (64.1) | 0.99 |
| Hypoalphalipoproteinemia | 63 (77.8) | 51 (82.3) | 29 (74.4) | 0.99 |
| Hypercholesterolemia | 26 (32.1) | 21 (33.9) | 15 (38.5) | 0.99 |
| Obstructive sleep apnea | 65 (80.2) | 40 (64.5) | 36 (92.3) | 0.0015 |
| Women (n = 45) | Men (n = 36) | Sex Comparison | |||
|---|---|---|---|---|---|
| Variables | Baseline | 6-Month Follow-Up | Baseline | 6-Month Follow-Up | † p-Value |
| Anthropometric, median (IQR) | |||||
| Weight, kg | 108.5 (93.8–116.0) | 101.9 (89.5–114.6) # | 135.4 (109.8–151.1) | 131.6 (104.0–149.0) # | 0.0017 |
| BMI, kg/m2 | 42.0 (36.4–44.9) | 40.1 (34.9–45.5) # | 42.3 (36.8–49.5) | 40.8 (34.7–49.1) # | 0.334 |
| Waist, cm | 115.9 (108.1–124.6) | 110.0 (103.0–120.0) # | 129.5 (115.143.9) | 121.7 (115.8–142.8) # | 0.0017 |
| Fat mass, % | 50.5 (47.1–54.0) | 49.9 (44.6–53.0) ** | 42.3 (38.8–46.6) | 41.2 (38.2–45.2) | 0.0017 |
| Fat–free mass, % | 49.4 (45.6–52.7) | 50.1 (47.0–55.4) | 57.8 (53.3–61.3) | 58.4 (53.6–61.0) # | 0.0017 |
| Systolic BP, mmHg | 120.0 (110.0–130.0) | 120.0 (110.0–120.0) | 130.0 (120.0–140.0) | 120.0 (120.0–130.0) * | 0.017 |
| Diastolic BP, mmHg | 80.0 (80.0–85.5) | 80.0 (70.0–80.0) ** | 89.0 (80.0–95.0) | 80.0 (80.0–85.7) ** | 0.068 |
| Biochemical, median (IQR) | |||||
| Glucose, mg/dL | 91.0 (83.5–103.5) | 91.0 (85.0–99.7) | 100.5 (83.5–114.7) | 95.0 (82.0–110.0) | 0.99 |
| Total cholesterol, mg/dL | 143.0 (111.0–206.5) | 159.0 (107.5–198.2) | 150.5 (130.7–267.2) | 178.0 (136.0–230.0) | 0.99 |
| LDL cholesterol, mg/dL | 108.0 (97.0–129.2) | 104.0 (91.5–112.0) | 111.5 (87.2–135.0) | 108.0 (95.0–136.0) | 0.99 |
| HDL cholesterol, mg/dL | 44.0 (37.5–49.0) | 44.0 (39.2–50.7) | 34.0 (32.0–40.7) | 36.5 (31.7–43.0) * | 0.0017 |
| Triglycerides, mg/dL | 108.0 (97.0–129.2) | 104.0 (91.5–112.0) | 111.5 (87.2–135.0) | 108.0 (95.0–136.0) | 0.99 |
| Psychopathology, n (%) | |||||
| Depressive disorder | 9 (20.0) | 3 (6.70) * | 3 (8.30) | 5 (13.9) | 0.595 |
| Anxiety disorder | 17 (37.8) | 11 (24.4) | 14 (38.9) | 12 (33.3) | 1.0 |
| Binge eating | 9 (20.0) | 5 (11.1) | 11 (30.6) | 5 (13.9) | 0.99 |
| HAD scale, median (IQR) | |||||
| Anxiety, score | 8.0 (3.0–10.7) | 5.0 (3.0–7.0) * | 7.0 (5.0–10.2) | 6.0 (3.0–7.75) * | 0.99 |
| Depression, score | 5.50 (3.0–90) | 4.0 (3.0–6.7) * | 7.0 (4.2–8.0) | 6.0 (4.0–8.0) | 0.99 |
| All Participants (n = 81) | † p-Value | |||
|---|---|---|---|---|
| Reference Value | Baseline | 6-Month Follow-Up | ||
| MoCA, median (IQR), score | 26–30 | 26.0 (23.5–28.0) | 27.0 (25.0–28.0) | 0.0024 |
| TMT-B | 75–273 | 85.0 (63.0–106.5) | 73.0 (58.0–100.0) | 0.99 |
| BANFE-2, median (IQR), score | ||||
| Medial orbital PFC | 80–115 | 97.0 (78.5–106.5) | 100.0 (85.0–112.0) | 0.888 |
| Dorsolateral PFC | 80–115 | 100 (90.0–109.5) | 103.0 (94.0–113.0) | 0.0024 |
| Anterior PFC | 80–115 | 101 (90–115.5) | 106.0 (97.0–118.0) | 0.168 |
| Total Score | 80–115 | 98.0 (87.0–108.0) | 103.0 (92.0–116.0) | 0.0024 |
| BANFE-2 performance grading, n (%) | ||||
| Severe | ≤69 | 6 (7.70) | 5(6.40) | 1.00 |
| Mild to moderate | 70–84 | 12 (14.8) | 13 (16.7) | 0.99 |
| Normal | 85–115 | 52 (64.2) | 54 (66.7) | 0.99 |
| Superior | ≥116 | 11 (12.8) | 9 (10.3) | 0.99 |
| BANFE-NQS, median (IQR), score | ||||
| Self-consciousness | <3 | 1.0 (0.0–1.0) | 0.0 (0.0–1.0) | 0.048 |
| Interests and motivations | <4 | 1.0 (0.0–3.0) | 0.0 (0.0–1.7) | 0.0024 |
| Behavioral Control | <4 | 3.0 (1.0–4.5) | 2.0 (1.0–3.0) | 0.096 |
| Frustration Tolerance | <3 | 1.0 (0.0–2.0) | 1.0 (0.0–1.0) | 0.552 |
| Mood | <3 | 1.0 (0.0–2.0) | 0.0 (0.0–1.0) | 0.696 |
| Executive Functioning | <4 | 2.0 (1.0–3.2) | 2.0 (1.0–3.0) | 0.99 |
| Total score | <15 | 10.0 (5.5–14.5) | 6.0 (3.0–10.0) | 0.0024 |
| EF Subdomain, median (IQR), score | ||||
| Planning | 11.0 (9.3–12.0) | 11.0 (9.91–12.0) | 0.99 | |
| Decision Making | 10.0 (8.0–12.0) | 10.2 (8.37–13.0) | 0.99 | |
| Verbal WM | 8.66 (7.6–10.0) | 9.16 (8.29–10.5) | 0.096 | |
| Visuospatial WM | 9.83 (9.0–11.0) | 9.83 (9.0–10.7) | 0.99 | |
| Cognitive Flexibility | 12.0 (9.66–13.0) | 12.5 (11.3–14.0) | 0.024 | |
| Inhibitory Control | 9.87 (8.65–10.7) | 10.3 (9.50–11.0) | 0.99 | |
| Metacognition | 10.0 (8.5–11.5) | 10.5 (9.50–11.0) | 0.99 | |
| Women | Men | Sex Comparison | |||
|---|---|---|---|---|---|
| Baseline | 6 Months | Baseline | 6 Months | † p-Value | |
| MoCA, median (IQR) | 26.0 (24.0–28.0) | 27.0 (25.0–28.0) * | 26.5 (23.0–28.0) | 27.0 (24.7–28.0) * | 0.99 |
| TMT–B, median (IQR) | 83.0 (56.7–94.5) | 74.0 (60.0–99) | 91.5 (68.0–125.7) | 71.0 (55.0–101.5) * | 0.99 |
| BANFE–2, median (IQR) | |||||
| Medial orbital PFC | 97.0 (80.5–105.2) | 103.0 (83.0–112.0) | 100.0 (765–107.0) | 100.0 (85.2–112.0) | 0.99 |
| Dorsolateral PFC | 99.0 (81.5–110.0) | 103.0 (90.0–111.0) & | 102.0 (91.2–109.7) | 103.5 (96.0–113.0) | 0.99 |
| Anterior PFC | 97.0 (85.5–111.0) | 104.0 (95.0–118.0) * | 105.0 (95.5–118.0) | 108.5 (104.0–118.0) | 0.99 |
| Total score | 96.0 (83.5–111.0) | 104.0 (90.0–113.0) & | 101.5 (87.5–107.0) | 102.0 (93.5–117.7) * | 0.99 |
| BANFE–2 global performance, n (%) | |||||
| Severe | 5 (11.9) | 2 (4.80) | 1 (2.80) | 3 (8.30) | 0.99 |
| Mild to moderate | 7 (15.4) | 10 (22.0) | 4 (12.1) | 4 (12.1) | 1.0 |
| Normal | 26 (57.1) | 30 (65.5) | 27 (73.0) | 24 (65.7) | 0.99 |
| Superior | 7 (15.6) | 3 (7.80) | 4 (12.1) | 5 (13.9) | 1.0 |
| BANFE–NQS, median (IQR) | |||||
| Self–consciousness | 1.0 (0.0–1.0) | 0.0 (0.0–1.0) ** | 1.0 (0.0–1.0) | 0.0 (0.0–0.5) | 0.99 |
| Interests & motivations | 1.0 (0.0–3.0) | 0.0 (0.0–1.0) & | 1.0 (0.0–3.0) | 0.0 (0.0–2.0) | 0.99 |
| Behavioral Control | 3.0 (1.0–5.0) | 1.0 (0.5–3.0) # | 1.0 (1.0–4.0) | 2.0 (1.0–3.0) | 0.88 |
| Frustration Tolerance | 2.0 (0.0–3.0) | 1.0 (0.0–1.0) ** | 1.0 (0.0–2.0) | 1.0 (0.0–1.0) | 0.378 |
| Mood | 1.0 (0.0–3.0) | 0.0 (0.0–2.0) * | 1.0 (0.0–1.0) | 0.0 (0.0–1.0) | 0.192 |
| Executive Functioning | 2.0 (1.0–4.0) | 2.0 (1.0–3.5) | 1.0 (1.0–3.0) | 1.0 (1.0–2.5) | 0.888 |
| Total score | 11.5 (6.7–16.2) | 5.0 (3.0–9.5) # | 7.0 (2.0–13.0) | 6.0 (3.0–10.0) | 0.576 |
| EF Subdomain, median (IQR) | |||||
| Planning | 10.6 (9.33–12.0) | 10.6 (8.33–12.0) | 11.3 (9.0–12.0) | 11.3 (10.33–12.0) | 0.99 |
| Decision Making | 9.50 (7.50–11.2) | 9.50 (7.50–12.5) | 10.5 (8.0–12.0) | 11.0 (8.75–13.2) | 0.99 |
| Verbal WM | 8.75 (7.79–9.91) | 9.16 (8.16–10.7) ** | 8.5 (7.62–10.3) | 9.33 (8.25–10.5) | 0.99 |
| Visuospatial WM | 10.3 (9.00–11.1) | 10.3 (9.08–10.6) | 9.7 (8.87–10.8) | 9.66 (9.00–11.0) | 0.99 |
| Cognitive Flexibility | 12.0 (8.16–13.3) | 12.6 (11.0–14.0) * | 11.8 (9.75–12.6) | 12.3 (11.5–13.8) ** | 0.99 |
| Inhibitory Control | 9.87 (8.87–10.8) | 10.3 (9.25–11.2) | 9.87 (8.37–10.7) | 10.5 (8.37–11.2) | 0.99 |
| Metacognition | 9.50 (8.0–11.0) | 10.0 (8.50–11.0) | 10.2 (9.50–11.5) | 10.5 (9.50–11.5) | 0.192 |
| B | Exp (B) | p-Value | |
|---|---|---|---|
| MoCA (score < 26) a | |||
| Constant | 2.624 | 13.790 | 0.151 |
| Female sex | −0.127 | 0.881 | 0.812 |
| Age | −0.013 | 0.987 | 0.667 |
| Weight change | −0.041 | 0.960 | 0.409 |
| Education years | −0.207 | 0.813 | 0.007 |
| Psychopathology | −0.072 | 0.931 | 0.894 |
| BANFE-2 (score < 85) b | |||
| Constant | 0.679 | 1.973 | 0.785 |
| Female sex | −0.091 | 0.913 | 0.903 |
| Age | −0.005 | 0.995 | 0.893 |
| Weight change | −0.051 | 0.950 | 0.397 |
| Education years | −0.167 | 0.847 | 0.110 |
| Psychopathology | −0.910 | 0.402 | 0.245 |
| BANFE-NQS (score < 15) c | |||
| Constant | −1.095 | 0.335 | 0.736 |
| Female sex | −0.857 | 0.424 | 0.377 |
| Age | −0.036 | 0.964 | 0.459 |
| Weight change | 0.032 | 1.033 | 0.635 |
| Education years | 0.122 | 1.020 | 0.874 |
| Psychopathology | 1.636 | 5.133 | 0.151 |
| Weight Loss ≥ 5% | Weight Loss < 5% | Weigh Gain ≥ 0.1% | p-Value | ||
|---|---|---|---|---|---|
| Neurocognitive Test | ReferenceScore | (n = 24) | (n = 38) | (n = 19) | |
| MoCA performance | |||||
| - MoCA normal | ≥26 | 17 (69.6) | 18 (48.6) | 11 (58.8) | |
| - MoCA impaired | <26 | 7 (30.4) | 20 (51.4) | 8 (41.2) | 0.272 |
| TMT-B performance | |||||
| - TMT-B normal | ≤273 | 21 (100) | 35 (100) | 19 (100) | |
| - TMT-B impaired | >273 | 0 (0.0) | 0 (0.0) | 0 (0.0) | - |
| BANFE-2 performance | |||||
| - BANFE-2 global normal | ≥85 | 19 (79.2) | 30 (78.9) | 16 (84.2) | |
| - BANFE-2 global impaired | <85 | 5 (20.8) | 8 (21.1) | 3 (15.8) | 0.661 |
| - Medial orbital PFC normal | ≥85 | 20 (83.3) | 25 (68.8) | 12 (63.2) | |
| - Medial orbital PFC impaired | <85 | 4 (16.7) | 13 (31.2) | 7 (36.8) | 0.565 |
| - Dorsolateral PFC normal | ≥85 | 17 (70.8) | 30 (78.9) | 17 (89.5) | |
| - Dorsolateral PFC impaired | <85 | 7 (29.2) | 8 (21.1) | 2 (10.5) | 0.356 |
| - Anterior PFC normal | ≥85 | 21 (87.5) | 27 (77.1) | 18 (94.7) | |
| - Anterior PFC impaired | <85 | 3 (12.5) | 11 (22.9) | 1 (5.30) | 0.216 |
| BANFE–NQS performance | |||||
| - BANFE–NQS normal | <15 | 19 (79.2) | 29 (76.3) | 16 (84.2) | |
| - BANFE–NQS impaired | ≥15 | 5 (20.8) | 9 (23.7) | 3 (15.8) | 0.870 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chávez-Manzanera, E.; Ramírez-Flores, M.; Duran, M.; Torres, M.; Ramírez, M.; Kaufer-Horwitz, M.; Stephano, S.; Quiroz-Casian, L.; Cantú-Brito, C.; Chiquete, E. Influence of Weight Loss on Cognitive Functions: A Pilot Study of a Multidisciplinary Intervention Program for Obesity Treatment. Brain Sci. 2022, 12, 509. https://doi.org/10.3390/brainsci12040509
Chávez-Manzanera E, Ramírez-Flores M, Duran M, Torres M, Ramírez M, Kaufer-Horwitz M, Stephano S, Quiroz-Casian L, Cantú-Brito C, Chiquete E. Influence of Weight Loss on Cognitive Functions: A Pilot Study of a Multidisciplinary Intervention Program for Obesity Treatment. Brain Sciences. 2022; 12(4):509. https://doi.org/10.3390/brainsci12040509
Chicago/Turabian StyleChávez-Manzanera, Emma, Maura Ramírez-Flores, Michelle Duran, Mariana Torres, Mariana Ramírez, Martha Kaufer-Horwitz, Sylvana Stephano, Lizette Quiroz-Casian, Carlos Cantú-Brito, and Erwin Chiquete. 2022. "Influence of Weight Loss on Cognitive Functions: A Pilot Study of a Multidisciplinary Intervention Program for Obesity Treatment" Brain Sciences 12, no. 4: 509. https://doi.org/10.3390/brainsci12040509