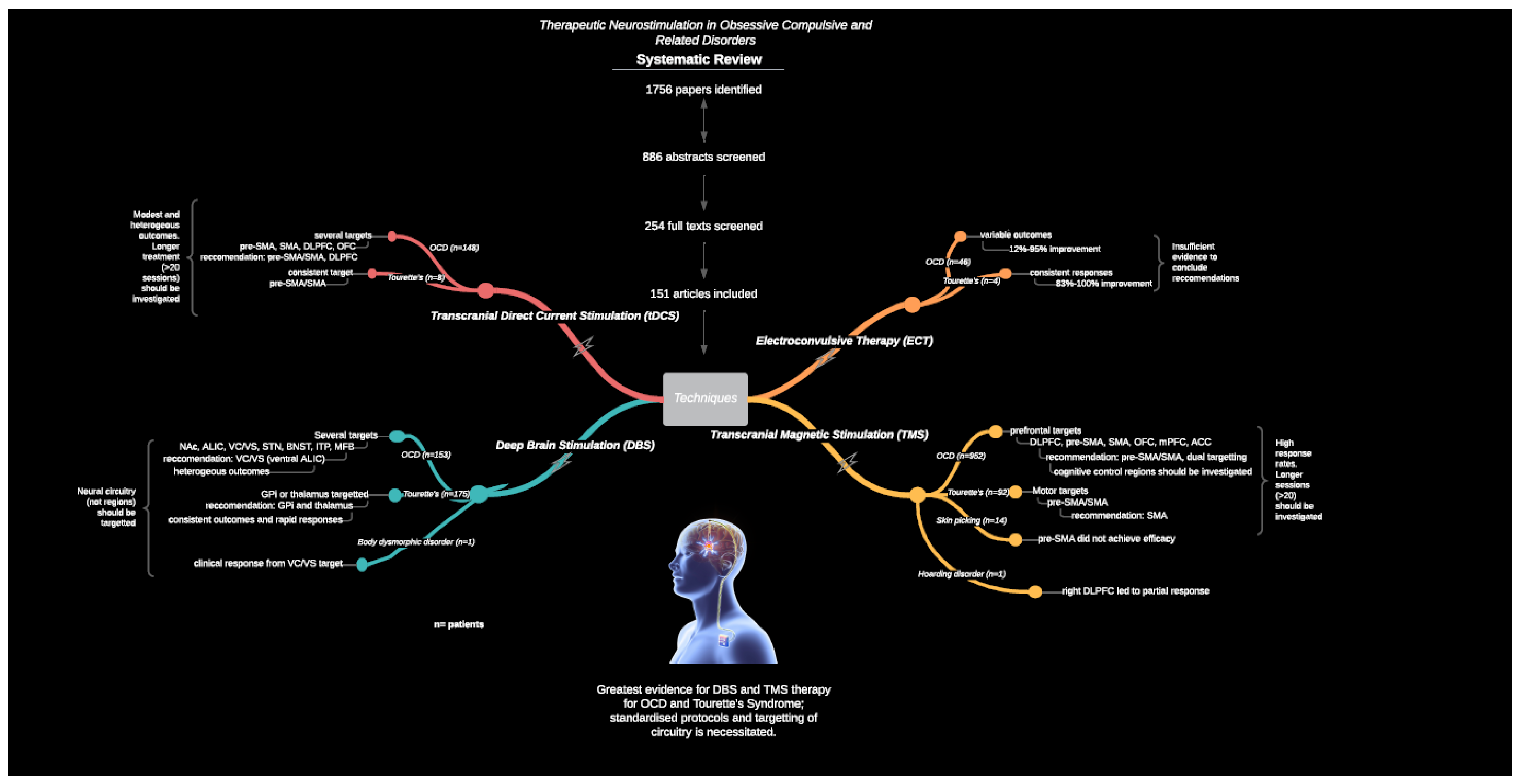
Correction: Acevedo et al. Therapeutic Neurostimulation in Obsessive-Compulsive and Related Disorders: A Systematic Review. Brain Sci. 2021, 11, 948




{kind=link}
| Study (Country) | N (m:f) | Study Design | Baseline YBOCS | Rx | Stimulation Parameters | YBOCS Outcomes % Change from Pre-Treatment | Comments/Conclusions | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Target (span of trajectory if reported) | Pulse width, Frequency | Stimulation intensity, and configuration (n) | Post treatment (≤6 months, or phase 1) | Follow up (>6 months, or phase 2) | Responders (Criterion, if reported) | ||||||
| Gabriels et al., 2003 (Belgium) [152] | 3 (1;2) | Case series | P1: 38 P2: 33 P3: 30 | ✓ | ALIC | ✗ | 9–10.5 V ✗ | ✗ | 12 months: P2: ~27% P3: ~46% + 32 months: P2: ~45% + P3: ~73% + | 12 months: 33.3% 32 months: 66.6% (35%) | 12 months of ALIC DBS led to response in one patient, partial response in another, and the other had DBS explanted. At 32 months of treatment, efficacy increased and 2 reached response. |
| Nuttin et al., 2003 (Belgium) [153] | 4(✗) | Phase 1: RCT, cross over design Phase 2: OL trial | 35 ± 4 | ✓ | ALIC (E0 in NAc) | 210/450 µs 100 Hz | 4–10.5 V Multipolar (4) Bipolar (1) | A: 43.4% + S: 7.7% | 21 months: 56% + | Phase 1: A: 75% S: 0% Phase 2: ✗ (35%) | 3 months of closed label ALIC DBS achieved a mean improvement of 43%, and response in 3/4 patients compared to 7.7% improvement and no responders in sham. 2 patients reached phase 2 and improved by 56% at 21 month FU. |
| Greenberg et al., 2006 (USA) [154] | 10(6;4) | OL trial | 34.6 ± 0.6 | VC/VS | 90–210 µs 100–130 Hz | 8–17 mA Monopolar (4) Bipolar (6) Unilateral (2) | 27.7% | 36 months: 35.5% +,* | 50% full 75% partial (35% full, 25% partial) | 3 months of ALIC DBS led to a mean improvement of 28% and 36 months led to 36% improvement. 20% achieved response at 6 months (2/10), and 50% (4/8) at 36 months. | |
| Greenberg et al., 2010 (Belgium, USA) [155] Long-term FU of Gabriels (2003), Nuttin (2003) and Greenberg (2006) cohorts 26(14;12) Multi-site OL follow up | 34 ± 0.5 | ✓ | VC/VS (E0 in Nac) | ✗ 100–130 Hz | ≤10.5 V ✗ | 38.2% +,* | 36 months: 38.5% +,* | 1 month: 28% Last FU: 61.5% (35%) | 3 months of VC/VS DBS led to mean improvement of 38%, and no further change at 36 months. 12 patients reached 36 month FU, all were included in the last FU (average 34 months), in which 62% reached response. Depression, anxiety and global functioning significantly improved by 53%, 50% and 69%, respectively, at last FU. CBT was resumed or initiated after 6–12 months. Outcomes of this cohort led to FDA and CE approval or ALIC DBS for TR-OCD. | ||
| Luyten et al., 2016 (Belgium, USA) [156] RCT and long-term follow up of Nuttin (2003), Gabriels (2003), Greenberg (2006; 2010) cohorts 24(12;12) Phase 1: Multi-site RCT, cross over design Phase 2: OL follow up | 35 ^ | ✓ | ALIC (6), BNST (15) ALIC + BNST (3) | 90–450 µs 85–130 Hz | 3–10.5 V Multipolar (5) Monopolar (4) Bipolar (8) | A: 42% #,*,+ S: 11% * | 48 months: BNST: 50% + ALIC: 22% ALL: 66% +,* | Phase 1: A: 70% S: 26% Phase 2: BNST: 80% ALIC: 16.6% ALIC + BNST: 100% (35%) | 3 months of closed label ALIC-BNST DBS (n = 17) led to 42% improvement compared to 11% in sham. 18 patients reached the 4-year FU, in which 66% improvement occurred. The optimised target shifted posterior with E0 in the BNST. BNST DBS led to an average of 50% improvement, compared to 22% from ALIC DBS, and 66% from both BNST and ALIC DBS. Anxiety, depression and global functioning improved by 45%, 49%, and 86%, respectively at last FU (54–171 months). | ||
| Abelson et al., 2005 (France) [157] | 4 (2;2) | Phase 1: RCT, cross over design Phase 2: OL | 32.75 ± 5.8 | ✓ | ALIC (E0 in NAc) | 60/210 μs 130/150 Hz | 4–10.5 V Monopolar (1) Bipolar (3) | A: 19.8% S: 10.5% | Phase 2: 30.2% | Phase 1: A: 25% S: 0% Phase 2: 50% (35%) | Average improvement from two 3-week cycles of ALIC DBS was 20% compared to 11% from sham. The best outcome was reported in phase 2 (4–23 months), individually these were 0% (device explanted), 44% (committed suicide), 73%, and 4%. 2 reached response in phase 2. |
| Mallet et al., 2008 (France) [158] | 16 (9;7) | Multi-site RCT, cross over design | On-off: 30–28 ^ Off-on: 28–31 ^ | 14/16 | amSTN | 60 µs 130 Hz | 2.0 ± 0.8 V Monopolar (14) Bipolar (1) Mono- and bipolar (1) Unilateral (1) | A: 25.4% #,+ S: 4.1% | ✗ | A: 75% S: 37.5% (25%) | 3 months of closed label amSTN DBS led to median improvement of 25% compared to 4% from sham. Global functioning (but not depression and anxiety) significantly improved in active compared to sham. |
| Mallet et al., 2019 (France) [13] Long-term FU of Mallet (2009) cohort 14 (6;8) OL follow up | 32.4 ± 3.6 | ✗ | amSTN | 60 µs 130 Hz | 1.2–4 V Monpolar (all) | ✗ | 16 months: 35.4% + 48 months: 51.2% + | 48 months: 75% full 92% partial (35% full, 25% partial) | 16 and 48 months of amSTN led to mean improvement of 35% and 52%, respectively. Depression and anxiety improved by 53% and 61%, respectively at 4 years. 2 withdrew from the previous report. | ||
| Goodman et al., 2010 (USA) [159] | 6 (2;4) | Phase 1: Pilot trial, staggered switch on (30 or 60 days post-op) Phase 2: OL | 33.2 ± 2.1 | ✓ | ALIC (E0 in VC/VS) | 90–210 µs 130/135 Hz | 2.5–8.5 V Monopolar (6) | Phase 1: ✗ | 12 months: 52.8% +,* | Phase 1: 50% Phase 2: 66.6% (35%) | 2 or 3 months of ALIC DBS led to response in 3/6 patients (values not reported). At 12 months, mean improvement was 53%, which was not affected by staggered switch on. 2 remained as severe on the CGI, but requested DBS be maintained due to subjective relief of anxiety, depression and tic symptoms. |
| Fayad et al., 2016 (USA) [160] Long-term follow of Goodman (2010) cohort 6 (2;4) OL follow up | ✗ | 5/6 | VC/VS | 150–210 µs 130/135 Hz | 4–8.5 V Multipolar (2) Monopolar (1) Bipolar (1) | ✗ | ✗ | Last FU: 66.6% (35%) | 6–9 years of VC/VS DBS led to response in the same 4 patients that achieved response from 12 months of treatment. 1 patient reached partial response of 26% improvement, and the other patient had the device switched off. | ||
| Huff et al., 2010 (Germany) [161] | 10 (6;4) | Phase 1: RCT, cross over design Phase 2: OL | 32.2 ± 4 | ✓ | NAc (E2,3 in ALIC) | 90 µs 145 Hz | 4.5 V Multipolar (all) | A: 13.3% * S: 3.4% | 6 months: 21.1%* | 12 months: 10% full 50% partial (35% full, 25% partial) | 3 months of closed label, unilateral NAc DBS led to mean improvement of 13.3% compared to 3.4% from sham. Following 3 and 6 months of open label DBS, improvements were 12.4% and 21.1%, respectively. At 12 month FU, 1 patient reached full response. |
| Mantione et al., 2014 (Netherlands) [162] | 16 (9;7) | Phase 1: OL trial, then CBT added Phase 2: RCT, cross over design | 33.7 ± 3.6 | 12/16 | NAc (E3 in ALIC) | 90 μs 130 Hz | Up to 5 V ✗ | Phase 1: 24.6% * Phase 1, CBT: 46% +,* | Phase 2: A: 1.9% (deterioration) S: 44.9% (deterioration) 21 months: 52% + | Phase 1: 37.5% Phase 1, CBT: 56% (35%) | 8 months of open label NAc DBS led to 25% improvement. A subsequent 24-week cycle with adjunct CBT led to a further significant improvement, reaching 46% change from pre-op, yet no significant change in depression or anxiety. The subsequent 4 week closed label phase (with CBT) led to deterioration of 1.9% from active and 44.9% from and sham. At 21 months post-op, mean improvement for OCD, anxiety and depression scores were 52%, 57%, and 46%, respectively. |
| Islam et al., 2015 (Italy) [163] | 8 (7;1) | OL trial of 2 targets | Nac: 34.6 ± 4.1 BNST: 35.8 ± 2.2 | ✗ | NAc (3) BNST (5) | 90/210 µs 130/180 Hz | 4.5–5.5 V Monopolar (4) Bipoar (4) | ✗ | 6 months: Nac: 11.6% BNST: 38.5% + | ✗ | 6 months of BNST DBS led to individual improvements of 25%, 10%, 0% in 3 patients, and NAc DBS led to improvements of 27.5%, 55%, 56%, 25%, 29% in 5 patients. Responders are reported from the last FU (6 months–5 years); 1 NAc patient had the device switched off, the other 2 reached 75% and 60% change at 5 years, 1 BNST patient was reported at 5 years with 30% change, the other 4 reached 6 month FU. |
| Farrand et al., 2018 (Australia) [164] | 7 (3;4) | OL trial | 32.4 ± 3.8 | ✓ | NAc (3) BNST (3) NAc-left, BNST-right (1) | ✗ | ✗ Monopolar (all) | ✗ | Last FU: BNST: 24.4% NAc: 23.4% BNST/NAc: 47.1% + All: 27.3% * | Last FU: BNST: 33.3% NAc: 33% BNST/NAc: 100% ALL: 42.8% (35% full) | Long-term (8–54 months) DBS of the BNST, NAc or both led to an average improvement of 24%, 23%, 47%, respectively. Individual change varied between 7–47%. Depression improved by 23% and anxiety deteriorated by 54% on average. |
| Barcia et al., 2019 (Spain) [165] | 7 (3;4) | RCT, cross over design | 32.2 ± 5 | ✓ | NAc (E2-3 in caudate) | 60 µs 130 Hz | 4.5 V ✗ | A: 51.3% +,* S: 25% * | ✗ | A: 85% S: ✗ (35%) | 3 months of closed label NAc DBS with the optimal contact, achieved mean improvement of 52% compared to 25% from sham. The non-responder had a partial response of 25% improvement. 1 patient reached 93% improvement after 3 months (YBOCS = 1). Anxiety did not significantly change from any contact. |
| Lee et al., 2019 (USA) [166] | 5 (2;3) | OL pilot study | 35 ± 1.9 | ✓ | ITP | 90 µs 130 Hz | 5–8.5 V Monopolar (all) | ✗ | 12 months: 52% +,* Last FU: 54% +,* | 12 months: 100% (35%) | 1 year of ITP DBS led to 52% improvement in OC symptoms and response in all 5 patients, and 54% improvement at last FU (duration was not specified). Anxiety symptoms had a significant improvement at 2 year FU (but not 1 year). |
| Huys et al., 2019 (Germany) [167] | 20 (10;10) | OL trial | 30.9 ^ | ✗ | NAc (E0,1), ALIC (E2,3) | 90–210 µs 120–180 Hz | 3–6 V Multipolar (all) | 11.5% * | 12 months: 33.3% * | 12 months: 40% full 70% partial (35% full, 25% partial) | 6 and 12 months of NAc-ALIC DBS led to median improvement of 12% and 33%, respectively. A further significant improvement at 6 and 12 months occurred. Anxiety and depressive symptoms did not significantly improve, and no predictors of response were identified. |
| Tyagi et al., 2019 (UK) [168] | 6 (5;1) | Phase 1: RCT, cross over design of 2 targets Phase 2: OL trial; amSTN, VC/VS amSTN + VC/VS DBS (COMB), optimised settings (OPT), OPT + CBT | 36.17 ± 0.75 | ✓ | VC/VS (NAc-ALIC) + amSTN | 60 µs 130 Hz | amSTN:1.4–2.6 V VC/VS: 5.4–7 V Monopolar (all) | Phase 1: amSTN: 45.2% +,* VC/VS: 52.9% +,* | Phase 2: COMB: 60.1% +,* OPT: 60.3% +,* OPT + CBT: 74.2% +,* | amSTN: 50% VC/VS: 83.3% COMB: 83.3% OPT: 100% OPT + CBT: 100% (35%) | 3 months of closed label amSTN and VC/VS DBS led to mean improvement of 45% and 53%, respectively. There was no statistical effect of conditions (amSTN vs. VC/VS, single vs. both targets, COMB vs. OPT + CBT) on OC symptoms, however the optimised stimulation condition, and adjunct CBT had clinical superiority. Depressive symptoms significantly improved from VC/VS DBS and set shifting significantly improved from amSTN DBS. |
Reference
- Acevedo, N.; Bosanac, P.; Pikoos, T.; Rossell, S.; Castle, D. Therapeutic Neurostimulation in Obsessive-Compulsive and Related Disorders: A Systematic Review. Brain Sci. 2021, 11, 948. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Acevedo, N.; Bosanac, P.; Pikoos, T.; Rossell, S.; Castle, D. Correction: Acevedo et al. Therapeutic Neurostimulation in Obsessive-Compulsive and Related Disorders: A Systematic Review. Brain Sci. 2021, 11, 948. Brain Sci. 2022, 12, 450. https://doi.org/10.3390/brainsci12040450
Acevedo N, Bosanac P, Pikoos T, Rossell S, Castle D. Correction: Acevedo et al. Therapeutic Neurostimulation in Obsessive-Compulsive and Related Disorders: A Systematic Review. Brain Sci. 2021, 11, 948. Brain Sciences. 2022; 12(4):450. https://doi.org/10.3390/brainsci12040450
Chicago/Turabian StyleAcevedo, Nicola, Peter Bosanac, Toni Pikoos, Susan Rossell, and David Castle. 2022. "Correction: Acevedo et al. Therapeutic Neurostimulation in Obsessive-Compulsive and Related Disorders: A Systematic Review. Brain Sci. 2021, 11, 948" Brain Sciences 12, no. 4: 450. https://doi.org/10.3390/brainsci12040450