
The Efficacy of Extended Metacognitive Training on Neurocognitive Function in Schizophrenia: A Randomized Controlled Trial

Abstract
:1. Introduction
2. Materials and Methods
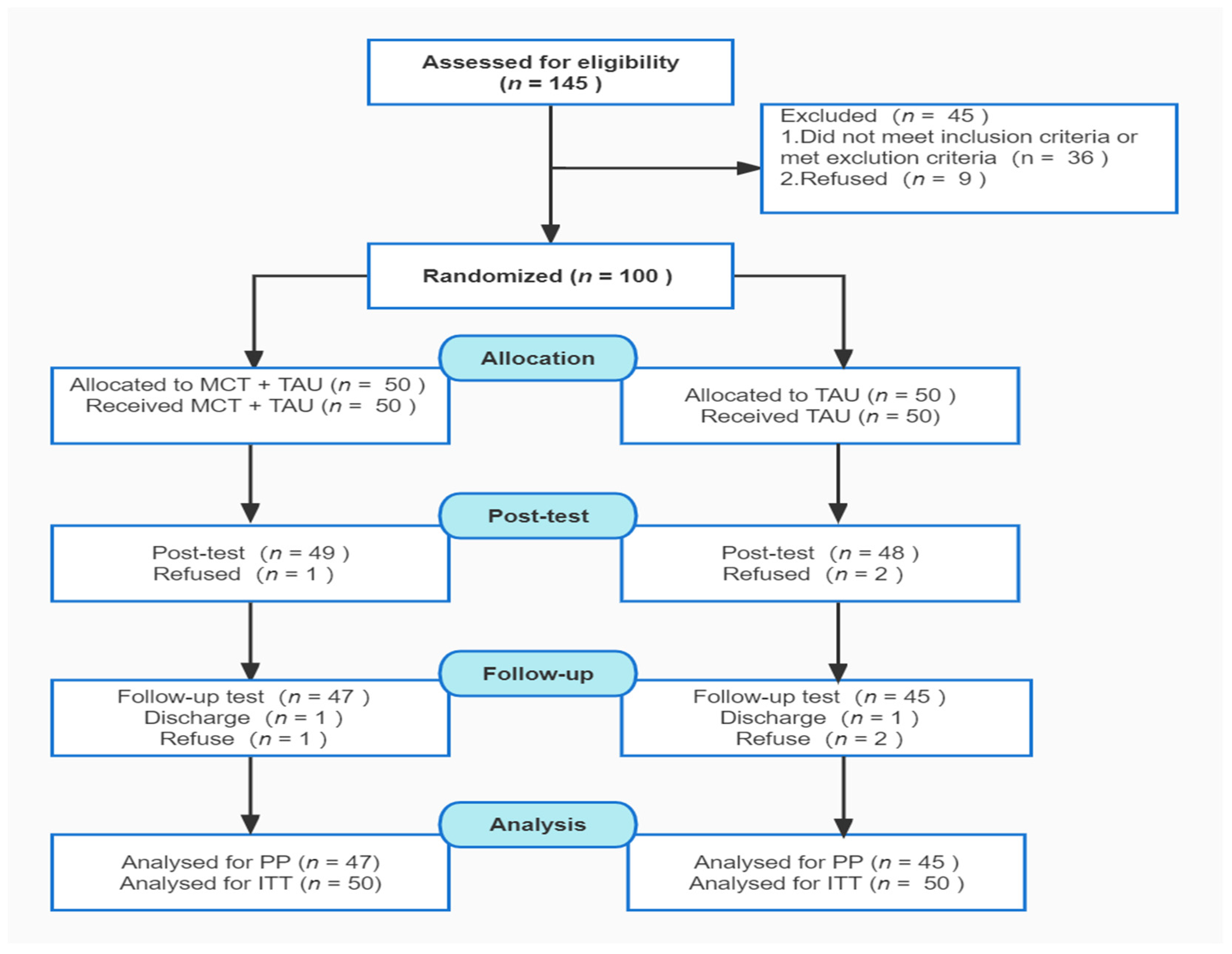
2.1. Procedure and Design
2.2. Participants
2.3. Sample Size
2.4. Data Collection and Outcome Measures
2.4.1. Primary Outcomes
2.4.2. Secondary Outcomes
2.4.3. Outcome Measures
2.5. Study Intervention
2.5.1. Control Group
2.5.2. Intervention Group
2.6. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Primary Outcomes
3.3. Secondary Outcomes
3.4. Completion and Subjective Assessment of the Training
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Lambert, M.; Kraft, V.; Rohenkohl, A.; Ruppelt, F.; Schröter, R.; Lüdecke, D.; Linschmann, B.; Eich, S.; Tlach, L.; Lion, D.; et al. Innovative care models for people with schizophrenia. Bundesgesundheitsblatt Gesundh. Gesundh. 2019, 62, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Charlson, F.J.; Ferrari, A.J.; Santomauro, D.F.; Diminic, S.; Stockings, E.; Scott, J.G.; McGrath, J.J.; Whiteford, H.A. Global Epidemiology and Burden of Schizophrenia: Findings From the Global Burden of Disease Study 2016. Schizophr. Bull. 2018, 44, 1195–1203. [Google Scholar] [CrossRef] [PubMed]
- Simon, G.E.; Stewart, C.; Yarborough, B.J.; Lynch, F.; Coleman, K.J.; Beck, A.; Operskalski, B.H.; Penfold, R.B.; Hunkeler, E.M. Mortality Rates After the First Diagnosis of Psychotic Disorder in Adolescents and Young Adults. JAMA Psychiatry 2018, 75, 254–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plana-Ripoll, O.; Pedersen, C.B.; Agerbo, E.; Holtz, Y.; Erlangsen, A.; Canudas-Romo, V.; Andersen, P.K.; Charlson, F.J.; Christensen, M.K.; Erskine, H.E.; et al. A comprehensive analysis of mortality-related health metrics associated with mental disorders: A nationwide, register-based cohort study. Lancet 2019, 394, 1827–1835. [Google Scholar] [CrossRef]
- McCutcheon, R.A.; Reis Marques, T.; Howes, O.D. Schizophrenia-An Overview. JAMA Psychiatry 2020, 77, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Owen, M.J.; Sawa, A.; Mortensen, P.B. Schizophrenia. Lancet 2016, 388, 86–97. [Google Scholar] [CrossRef] [Green Version]
- Carrión, R.E.; Walder, D.J.; Auther, A.M.; McLaughlin, D.; Zyla, H.O.; Adelsheim, S.; Calkins, R.; Carter, C.S.; McFarland, B.; Melton, R.; et al. From the psychosis prodrome to the first-episode of psychosis: No evidence of a cognitive decline. J. Psychiatr. Res. 2018, 96, 231–238. [Google Scholar] [CrossRef]
- Fett, A.J.; Velthorst, E.; Reichenberg, A.; Ruggero, C.J.; Callahan, J.L.; Fochtmann, L.J.; Carlson, G.A.; Perlman, G.; Bromet, E.J.; Kotov, R. Long-term Changes in Cognitive Functioning in Individuals With Psychotic Disorders: Findings From the Suffolk County Mental Health Project. JAMA Psychiatry 2020, 77, 387–396. [Google Scholar] [CrossRef]
- McCleery, A.; Nuechterlein, K.H. Cognitive impairment in psychotic illness: Prevalence, profile of impairment, developmental course, and treatment considerations. Dialogues Clin. Neurosci. 2019, 21, 239–248. [Google Scholar]
- Green, M.F.; Horan, W.P.; Lee, J. Nonsocial and social cognition in schizophrenia: Current evidence and future directions. World Psychiatry 2019, 18, 146–161. [Google Scholar] [CrossRef] [Green Version]
- Seidman, L.J.; Mirsky, A.F. Evolving Notions of Schizophrenia as a Developmental Neurocognitive Disorder. J. Int. Neuropsychol. Soc. 2017, 23, 881–892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monteleone, P.; Cascino, G.; Monteleone, A.M.; Rocca, P.; Rossi, A.; Bertolino, A.; Aguglia, E.; Amore, M.; Collantoni, E.; Corrivetti, G.; et al. Prevalence of antipsychotic-induced extrapyramidal symptoms and their association with neurocognition and social cognition in outpatients with schizophrenia in the “real-life”. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 109, 110250. [Google Scholar] [CrossRef] [PubMed]
- MacKenzie, N.E.; Kowalchuk, C.; Agarwal, S.M.; Costa-Dookhan, K.A.; Caravaggio, F.; Gerretsen, P.; Chintoh, A.; Remington, G.J.; Taylor, V.H.; Müeller, D.J.; et al. Antipsychotics, Metabolic Adverse Effects, and Cognitive Function in Schizophrenia. Front. Psychiatry 2018, 9, 622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sohlberg, M.M.; Mateer, C.A. Training use of compensatory memory books: A three stage behavioral approach. J. Clin. Exp. Neuropsychol. 1989, 11, 871–891. [Google Scholar] [CrossRef]
- van der Gaag, M.; van den Berg, D.; Ising, H. CBT in the prevention of psychosis and other severe mental disorders in patients with an at risk mental state: A review and proposed next steps. Schizophr. Res. 2019, 203, 88–93. [Google Scholar] [CrossRef]
- Bellani, M.; Ricciardi, C.; Rossetti, M.G.; Zovetti, N.; Perlini, C.; Brambilla, P. Cognitive remediation in schizophrenia: The earlier the better? Epidemiol. Psychiatr. Sci. 2019, 29, e57. [Google Scholar] [CrossRef] [Green Version]
- Cella, M.; Price, T.; Corboy, H.; Onwumere, J.; Shergill, S.; Preti, A. Cognitive remediation for inpatients with psychosis: A systematic review and meta-analysis. Psychol. Med. 2020, 50, 1062–1076. [Google Scholar] [CrossRef]
- Moritz, S.; Woodward, T.S. Metacognitive training in schizophrenia: From basic research to knowledge translation and intervention. Curr. Opin. Psychiatry 2007, 20, 619–625. [Google Scholar] [CrossRef] [Green Version]
- Philipp, R.; Kriston, L.; Kühne, F.; Härter, M.; Meister, R. Concepts of Metacognition in the Treatment of Patients with Mental Disorders. J. Ration.-Emot. Cogn.-Behav. Ther. 2019, 38, 173–183. [Google Scholar] [CrossRef]
- Bright, M.; Parker, S.; French, P.; Fowler, D.; Gumley, A.; Morrison, A.P.; Birchwood, M.; Jones, P.B.; Stewart, S.L.K.; Wells, A. Metacognitive beliefs as psychological predictors of social functioning: An investigation with young people at risk of psychosis. Psychiatry Res. 2018, 262, 520–526. [Google Scholar] [CrossRef]
- Han, M.; Lee, K.; Kim, M.; Heo, Y.; Choi, H. Metacognitive Rating Scale: A Study Applying a Korean Translation to Individuals with Schizophrenia. Int. J. Environ. Res. Public Health 2021, 18, 6853. [Google Scholar] [CrossRef] [PubMed]
- González-Blanch, C.; Birulés, I.; Pousa, E.; Barrigon, M.L.; López-Carrilero, R.; Lorente-Rovira, E.; Ayesa-Arriola, R.; Setien-Suero, E.; Barajas, A.; Grasa, E.M.; et al. Moderators of cognitive insight outcome in metacognitive training for first-episode psychosis. J. Psychiatr. Res. 2021, 141, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Birulés, I.; López-Carrilero, R.; Cuadras, D.; Pousa, E.; Barrigón, M.L.; Barajas, A.; Lorente-Rovira, E.; González-Higueras, F.; Grasa, E.; Ruiz-Delgado, I.; et al. Cognitive Insight in First-Episode Psychosis: Changes during Metacognitive Training. J. Pers. Med. 2020, 10, 253. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, R.; Ishigaki, T.; Shimada, T.; Tanoue, H.; Yoshinaga, N.; Oribe, N.; Morimoto, T.; Matsumoto, T.; Hosono, M. The efficacy of extended metacognitive training for psychosis: A randomized controlled trial. Schizophr. Res. 2020, 215, 399–407. [Google Scholar] [CrossRef] [PubMed]
- de Pinho, L.M.G.; Sequeira, C.; Sampaio, F.M.C.; Rocha, N.B.; Ozaslan, Z.; Ferre-Grau, C. Assessing the efficacy and feasibility of providing metacognitive training for patients with schizophrenia by mental health nurses: A randomized controlled trial. J. Adv. Nurs. 2021, 77, 999–1012. [Google Scholar] [CrossRef]
- Simón-Expósito, M.; Felipe-Castaño, E. Effects of Metacognitive Training on Cognitive Insight in a Sample of Patients with Schizophrenia. Int. J. Environ. Res. Public Health 2019, 16, 4541. [Google Scholar] [CrossRef] [Green Version]
- Vita, A.; Barlati, S.; Ceraso, A.; Nibbio, G.; Ariu, C.; Deste, G.; Wykes, T. Effectiveness, Core Elements, and Moderators of Response of Cognitive Remediation for Schizophrenia: A Systematic Review and Meta-analysis of Randomized Clinical Trials. JAMA Psychiatry 2021, 78, 848–858. [Google Scholar] [CrossRef]
- Lejeune, J.A.; Northrop, A.; Kurtz, M.M. A Meta-analysis of Cognitive Remediation for Schizophrenia: Efficacy and the Role of Participant and Treatment Factors. Schizophr. Bull. 2021, 47, 997–1006. [Google Scholar] [CrossRef]
- Montemagni, C.; Del Favero, E.; Riccardi, C.; Canta, L.; Toye, M.; Zanalda, E.; Rocca, P. Effects of Cognitive Remediation on Cognition, Metacognition, and Social Cognition in Patients With Schizophrenia. Front. Psychiatry 2021, 12, 649737. [Google Scholar] [CrossRef]
- Moritz, S.; Kerstan, A.; Veckenstedt, R.; Randjbar, S.; Vitzthum, F.; Schmidt, C.; Heise, M.; Woodward, T.S. Further evidence for the efficacy of a metacognitive group training in schizophrenia. Behav. Res. Ther. 2011, 49, 151–157. [Google Scholar] [CrossRef]
- Moritz, S.; Veckenstedt, R.; Andreou, C.; Bohn, F.; Hottenrott, B.; Leighton, L.; Köther, U.; Woodward, T.S.; Treszl, A.; Menon, M.; et al. Sustained and “sleeper” effects of group metacognitive training for schizophrenia: A randomized clinical trial. JAMA Psychiatry 2014, 71, 1103–1111. [Google Scholar] [CrossRef] [PubMed]
- Moritz, S.; Veckenstedt, R.; Bohn, F.; Hottenrott, B.; Scheu, F.; Randjbar, S.; Aghotor, J.; Köther, U.; Woodward, T.S.; Treszl, A.; et al. Complementary group Metacognitive Training (MCT) reduces delusional ideation in schizophrenia. Schizophr. Res. 2013, 151, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Pankowski, D.; Kowalski, J.; Gawęda, Ł. The effectiveness of metacognitive training for patients with schizophrenia: A narrative systematic review of studies published between 2009 and 2015. Psychiatr. Pol. 2016, 50, 787–803. [Google Scholar] [CrossRef] [PubMed]
- Ochoa, S.; Haro, J.M.; Huerta-Ramos, E.; Cuevas-Esteban, J.; Stephan-Otto, C.; Usall, J.; Nieto, L.; Brebion, G. Relation between jumping to conclusions and cognitive functioning in people with schizophrenia in contrast with healthy participants. Schizophr. Res. 2014, 159, 211–217. [Google Scholar] [CrossRef]
- Shan, X.; Liao, R.; Ou, Y.; Pan, P.; Ding, Y.; Liu, F.; Chen, J.; Zhao, J.; Guo, W.; He, Y. Increased regional homogeneity modulated by metacognitive training predicts therapeutic efficacy in patients with schizophrenia. Eur. Arch. Psychiatry Clin. Neurosci. 2021, 271, 783–798. [Google Scholar] [CrossRef] [Green Version]
- Murray, R.J.; Schaer, M.; Debbané, M. Degrees of separation: A quantitative neuroimaging meta-analysis investigating self-specificity and shared neural activation between self- and other-reflection. Neurosci. Biobehav. Rev. 2012, 36, 1043–1059. [Google Scholar] [CrossRef]
- Ye, Q.; Zou, F.; Lau, H.; Hu, Y.; Kwok, S.C. Causal Evidence for Mnemonic Metacognition in Human Precuneus. J. Neurosci. 2018, 38, 6379–6387. [Google Scholar] [CrossRef] [Green Version]
- Randolph, C.; Tierney, M.C.; Mohr, E.; Chase, T.N. The Repeatable Battery for the Assessment of Neuropsychological Status (RBANS): Preliminary clinical validity. J. Clin. Exp. Neuropsychol. 1998, 20, 310–319. [Google Scholar] [CrossRef]
- Gold, J.M.; Queern, C.; Iannone, V.N.; Buchanan, R.W. Repeatable battery for the assessment of neuropsychological status as a screening test in schizophrenia I: Sensitivity, reliability, and validity. Am. J. Psychiatry 1999, 156, 1944–1950. [Google Scholar]
- Saykin, A.J.; Shtasel, D.L.; Gur, R.E.; Kester, D.B.; Mozley, L.H.; Stafiniak, P.; Gur, R.C. Neuropsychological deficits in neuroleptic naive patients with first-episode schizophrenia. Arch. Gen. Psychiatry 1994, 51, 124–131. [Google Scholar] [CrossRef]
- Zheng, W.; Jiang, W.L.; Zhang, X.; Cai, D.B.; Sun, J.W.; Yin, F.; Ren, P.C.; Zhao, M.; Wu, H.W.; Xiang, Y.Q.; et al. Use of the RBANS to Evaluate Cognition in Patients with Schizophrenia and Metabolic Syndrome: A Meta-Analysis of Case-Control Studies. Psychiatr. Q. 2021, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Li, C.; Cheng, Y.; Yi, Z.; Long, B.; Wang, J. A preliminary study on the reliability and validity of a repeatable neuropsychological state test in patients with schizophrenia. Shanghai Psychiatry 2009, 21, 265–268. [Google Scholar]
- Aghotor, J.; Pfueller, U.; Moritz, S.; Weisbrod, M.; Roesch-Ely, D. Metacognitive training for patients with schizophrenia (MCT): Feasibility and preliminary evidence for its efficacy. J. Behav. Ther. Exp. Psychiatry 2010, 41, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Holthausen, E.A.; Wiersma, D.; Sitskoorn, M.M.; Dingemans, P.M.; Schene, A.H.; van den Bosch, R.J. Long-term memory deficits in schizophrenia: Primary or secondary dysfunction? Neuropsychology 2003, 17, 539–547. [Google Scholar] [CrossRef] [Green Version]
- Hauser, M.; Zhang, J.P.; Sheridan, E.M.; Burdick, K.E.; Mogil, R.; Kane, J.M.; Auther, A.; Carrión, R.E.; Cornblatt, B.A.; Correll, C.U. Neuropsychological Test Performance to Enhance Identification of Subjects at Clinical High Risk for Psychosis and to Be Most Promising for Predictive Algorithms for Conversion to Psychosis: A Meta-Analysis. J. Clin. Psychiatry 2017, 78, e28–e40. [Google Scholar] [CrossRef]
- Rocha, N.B.; Queirós, C. Metacognitive and social cognition training (MSCT) in schizophrenia: A preliminary efficacy study. Schizophr. Res. 2013, 150, 64–68. [Google Scholar] [CrossRef] [Green Version]
- Gawęda, Ł.; Krężołek, M.; Olbryś, J.; Turska, A.; Kokoszka, A. Decreasing self-reported cognitive biases and increasing clinical insight through meta-cognitive training in patients with chronic schizophrenia. J. Behav. Ther. Exp. Psychiatry 2015, 48, 98–104. [Google Scholar] [CrossRef]
- Bachman, P.; Reichenberg, A.; Rice, P.; Woolsey, M.; Chaves, O.; Martinez, D.; Maples, N.; Velligan, D.I.; Glahn, D.C. Deconstructing processing speed deficits in schizophrenia: Application of a parametric digit symbol coding test. Schizophr. Res. 2010, 118, 6–11. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristic | TAU + MCT n (%) | TAU n (%) | Statistics | p Value |
|---|---|---|---|---|
| Demographic data | ||||
| Sex | χ2 = 0.162 | 0.687 | ||
| Male | 23 (46.0%) | 21 (42.0%) | ||
| Female | 27 (54.0%) | 29 (58.0%) | ||
| Treatment-related data | ||||
| Hospitalizations (including present) | χ2 = 1.296 | 0.523 | ||
| Once | 15 (30.0%) | 15 (30.0%) | ||
| 1–5 times | 25 (50.0%) | 29 (58.0%) | ||
| >5 times | 10 (20.0%) | 6 (12.0%) | ||
| Years of disease | χ2 = 1.213 | 0.545 | ||
| <5 | 17 (34.7%) | 20 (40.0%) | ||
| 5–10 | 21 (42.9%) | 23 (46.0%) | ||
| >10 | 11 (22.4%) | 7 (14.0%) | ||
| Mean (SD) | Mean (SD) | |||
| Age (years) | 44.66 (9.612) | 44.34 (8.530) | t = 0.726 | 0.469 |
| RBANS | 70.00 (11.884) | 69.84 (13.312) | t = 0.063 | 0.950 |
| Immediate memory | 73.64 (18.098) | 70.96 (11.480) | t = 0.884 | 0.379 |
| Visual spatial | 77.12 (10.634) | 77.32 (16.918) | t = 0.071 | 0.994 |
| Language | 78.22 (10.620) | 78.28 (12.636) | t = 0.026 | 0.980 |
| Attention | 77.78 (13.146) | 78.06 (12.369) | t = 0.110 | 0.913 |
| Delayed memory | 74.70 (18.010) | 75.42 (17.182) | t = 0.205 | 0.838 |
| Variables | Group | Mean (SD) | Per-Protocol Statistics Mean Differences (95% Cl) across Time and MANCOVAs | Intention-to-Treat Statistics Mean Differences (95% Cl) across Time and MANCOVAs | ||||
|---|---|---|---|---|---|---|---|---|
| Baseline | Post-Treatment | Follow-Up | Baseline-Post | Baseline-Follow-Up | Baseline-Post | Baseline-Follow-Up | ||
| RBANS | TAU + MCT | 69.81 (12.24) | 74.51 (12.45) | 76.36 (12.97) | 4.702 (4.045–5.359) | 6.556 (5.975–7.137) | 4.755 (4.114–5.397) | 6.490 (5.946–67.033) |
| TAU | 70.22 (13.97) | 71.78 (14.16) | 73.13 (13.94) | 1.555 (0.884–2.227) | 2.908 (2.314–3.502) | 1.583 (0.935–2.231) | 2.896 (2.347–3.446) | |
| F = 44.327, ηp2 = 0.332 p < 0.001 | F = 76.028, ηp2 = 0.461 p < 0.001 | F = 44.846, ηp2 = 0.316 p < 0.001 | F = 83.356, ηp2 = 0.462 p < 0.001 | |||||
| Variables | Group | Mean (SD) | Per-Protocol Statistics MD (95% CI) across Time and MANCOVAs | Intention-to-Treat Statistics MD (95% Cl) across Time and MANCOVAs | ||||
|---|---|---|---|---|---|---|---|---|
| Baseline | Post-Treatment | Follow-Up | Post-Treatment | Follow-Up | Post-Treatment | Follow-Up | ||
| Immediate memory | MCT | 73.64 (18.10) | 74.79 (17.19) | 77.04 (17.79) | 1.845 (1.016–2.647) | 4.083 (3.096–5.070) | 1.747 (0.946–2.549) | 3.701 (2.993–4.408) |
| TAU | 70.96 (11.48) | 72.58 (11.10) | 74.73 (11.17) | 1.384 (0.537–2.231) | 3.558 (2.549–4.566) | 1.279 (0.469–2.089) | 3.014 (2.299–3.729) | |
| F = 0.595, ηp2 = 0.007 p < 0.443 | F = 0.547, ηp2 = 0.006 p < 0.462 | F = 0.665, ηp2 = 0.007 p < 0.417 | F = 1.835, ηp2 = 0.019 p < 0.179 | |||||
| Visual–spatial structure | MCT | 76.83 (10.75) | 80.68 (11.44) | 81.60 (11.76) | 3.851 (3.164–4.538) | 4.766 (4.030–5.502) | 3.779 (3.112–4.447) | 4.821 (4.152–5.490) |
| TAU | 77.60 (17.28) | 78.96 (17.47) | 79.60 (17.35) | 1.356 (0.653–2.058) | 2.000 (1.248–2.752) | 1.308 (0.634–1.983) | 1.975 (1.299–2.651) | |
| F = 25.520, ηp2 = 0.223 p < 0.001 | F = 27.384, ηp2 = 0.235 p < 0.001 | F = 26.715, ηp2 = 0.221 p < 0.001 | F = 35.283, ηp2 = 0.273 p < 0.001 | |||||
| Verbal function | MCT | 78.55 (10.57) | 81.00 (10.91) | 82.15 (10.37) | 3.856 (3.167–4.545) | 4.772 (4.034–5.509) | 2.976 (2.010–3.941) | 4.090 (3.145–5.035) |
| TAU | 79.42 (12.15) | 81.22 (12.50) | 82.38 (11.94) | 1.350 (0.646–2.055) | 1.994 (1.240–2.748) | 1.775 (0.800–2.750) | 2.866 (1.911–3.821) | |
| F = 1.277, ηp2 = 0.014 p < 0.261 | F = 1.657, ηp2 = 0.018 p < 0.201 | F = 3.017, ηp2 = 0.031 p < 0.086 | F = 3.274, ηp2 = 0.034 p < 0.074 | |||||
| Attention | MCT | 77.32 (13.38) | 83.28 (13.97) | 85.17 (14.28) | 5.953 (4.913–6.993) | 7.848 (6.825–8.871) | 5.918 (4.919–6.917) | 7.714 (6.741–8.687) |
| TAU | 77.60 (12.51) | 79.67 (11.99) | 80.60 (11.81) | 2.071 (1.008–3.135) | 3.003 (1.958–4.049) | 2.084 (1.074–3.094) | 3.021 (2.038–4.004) | |
| F = 26.879, ηp2 = 0.232 p < 0.001 | F = 43.279, ηp2 = 0.327 p < 0.001 | F = 28.715, ηp2 = 0.234 p < 0.001 | F = 45.357, ηp2 = 0.325 p < 0.001 | |||||
| Delayed memory | MCT | 74.98 (18.37) | 80.96 (17.21) | 82.55 (18.04) | 5.956 (4.905–7.007) | 7.556 (6.519–8.593) | 5.975 (4.959–6.991) | 7.527 (6.680–8.373) |
| TAU | 75.60 (17.01) | 77.31 (16.28) | 78.07 (15.88) | 1.735 (0.661–2.809) | 2.486 (1.426–3.546) | 1.838 (0.812–2.864) | 2.962 (2.107–3.817) | |
| F=31.132, ηp2 = 0.259 p < 0.001 | F = 46.142, ηp2 = 0.34 p < 0.001 | F = 32.364, ηp2 = 0.256 p < 0.001 | F = 56.741, ηp2 = 0.376 p < 0.001 | |||||
| Yes | No | |
|---|---|---|
| The training was useful and sensible. | 47 (100%) | 0 |
| I had to force myself to go to the training regularly. | 18 (17%) | 29 (63%) |
| In everyday life, I do not apply the lessons learned. | 20 (43%) | 27 (57%) |
| The training was an important part of my treatment program. | 43 (91%) | 4 (9%) |
| I would have liked to spend the time doing something else. | 15 (32%) | 32 (68%) |
| The training was fun. | 44 (94%) | 3 (6%) |
| A lot of what I learned during training is useful for daily life. | 44 (94%) | 3 (6%) |
| The goals and rationale of the training were clear to me. | 42 (90%) | 5 (10%) |
| I would recommend the training to others. | 47 (100%) | 0 |
| I found it beneficial that the training was administered in a group. | 47 (100%) | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, C.; Chong, Y.; Zhang, J.; Cao, Y.; Wang, Y. The Efficacy of Extended Metacognitive Training on Neurocognitive Function in Schizophrenia: A Randomized Controlled Trial. Brain Sci. 2022, 12, 413. https://doi.org/10.3390/brainsci12030413
Wang C, Chong Y, Zhang J, Cao Y, Wang Y. The Efficacy of Extended Metacognitive Training on Neurocognitive Function in Schizophrenia: A Randomized Controlled Trial. Brain Sciences. 2022; 12(3):413. https://doi.org/10.3390/brainsci12030413
Chicago/Turabian StyleWang, Can, Yue Chong, Jiechun Zhang, Yili Cao, and Yanbo Wang. 2022. "The Efficacy of Extended Metacognitive Training on Neurocognitive Function in Schizophrenia: A Randomized Controlled Trial" Brain Sciences 12, no. 3: 413. https://doi.org/10.3390/brainsci12030413