
Earlier Age at Surgery for Brain Cavernous Angioma-Related Epilepsy May Achieve Complete Seizure Freedom without Aid of Anti-Seizure Medication


Abstract
:1. Introduction
2. Methods
2.1. Study Design and Ethics Approval
2.2. Clinical Information
2.3. Magnetic Resonance Imaging of the Brain
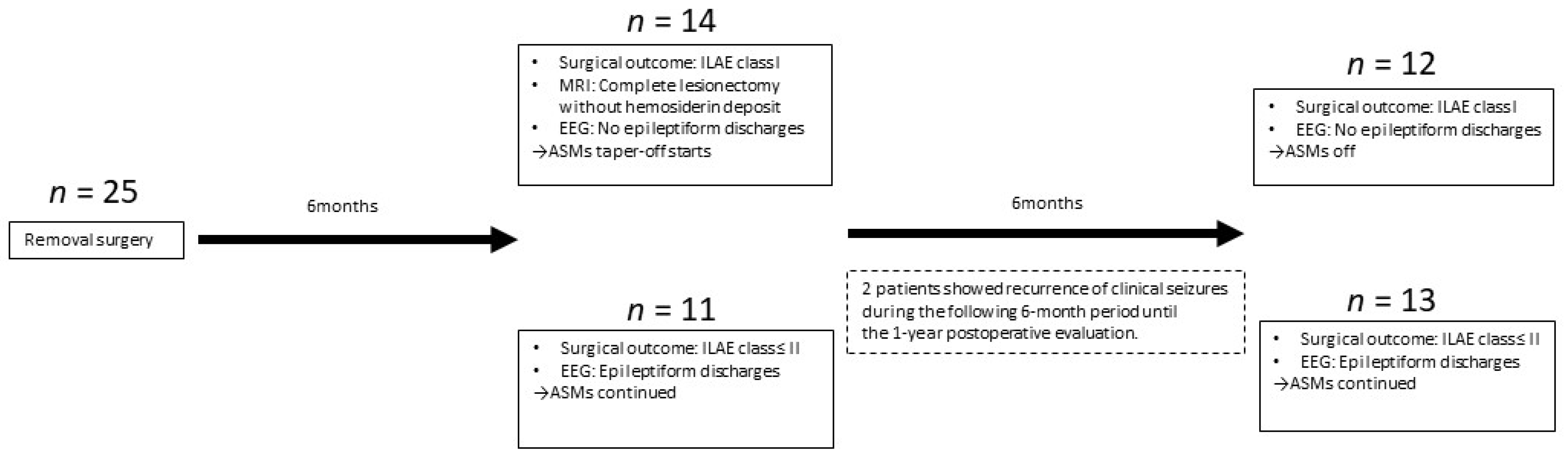
2.4. Surgery and Surgical Outcome
2.5. Follow-Up Evaluation
2.6. Primary Outcome Measurement
2.7. Secondary Outcome Measurement
2.8. Statistical Analysis
3. Results
3.1. Clinical Information
3.2. Primary Outcome
3.3. Secondary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alexiou, G.A.; Mpairamidis, E.; Sfakianos, G.; Prodromou, N. Surgical management of brain cavernomas in children. Pediatr. Neurosurg. 2009, 45, 375–378. [Google Scholar] [CrossRef] [PubMed]
- Raychaudhuri, R.; Batjer, H.H.; Awad, I.A. Intracranial cavernous angioma: A practical review of clinical and biological aspects. Surg. Neurol. 2005, 63, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Flemming, K.D.; Graff-Radford, J.; Aakre, J.; Kantarci, K.; Lanzino, G.; Brown, R.D., Jr.; Mielke, M.M.; Roberts, R.O.; Kremers, W.; Knopman, D.S.; et al. Population-Based Prevalence of Cerebral Cavernous Malformations in Older Adults: Mayo Clinic Study of Aging. JAMA Neurol. 2017, 74, 801–805. [Google Scholar] [CrossRef] [PubMed]
- Zabramski, J.M.; Wascher, T.M.; Spetzler, R.F.; Johnson, B.; Golfinos, J.; Drayer, B.P.; Brown, B.; Rigamonti, D.; Brown, G. The natural history of familial cavernous malformations: Results of an ongoing study. J. Neurosurg. 1994, 80, 422–432. [Google Scholar] [CrossRef] [PubMed]
- Kashiwagi, S.; van Loveren, H.R.; Tew, J.M., Jr.; Wiot, J.G.; Weil, S.M.; Lukin, R.A. Diagnosis and treatment of vascular brain-stem malformations. J. Neurosurg. 1990, 72, 27–34. [Google Scholar] [CrossRef] [Green Version]
- Zyck, S.; Gould, G.C. Cavernous Venous Malformation. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2022. [Google Scholar]
- Rumalla, K.; Srinivasan, V.M.; Gaddis, M.; Kvint, S.; Patel, A.J.; Kan, P.; Lawton, M.T.; Burkhardt, J.K. Cavernous Malformation Surgery in the United States: Validation of a Novel International Classification of Disease, 10th Edition, Clinical Modification Code Search Algorithm and Volume-Driven Surgical Outcomes. World Neurosurg. 2021, 150, e66–e73. [Google Scholar] [CrossRef]
- Zafar, A.; Quadri, S.A.; Farooqui, M.; Ikram, A.; Robinson, M.; Hart, B.L.; Mabray, M.C.; Vigil, C.; Tang, A.T.; Kahn, M.L.; et al. Familial Cerebral Cavernous Malformations. Stroke 2019, 50, 1294–1301. [Google Scholar] [CrossRef]
- Hong, T.; Xiao, X.; Ren, J.; Cui, B.; Zong, Y.; Zou, J.; Kou, Z.; Jiang, N.; Meng, G.; Zeng, G.; et al. Somatic MAP3K3 and PIK3CA mutations in sporadic cerebral and spinal cord cavernous malformations. Brain 2021, 144, 2648–2658. [Google Scholar] [CrossRef]
- Hart, B.L.; Mabray, M.C.; Morrison, L.; Whitehead, K.J.; Kim, H. Systemic and CNS manifestations of inherited cerebrovascular malformations. Clin. Imaging 2021, 75, 55–66. [Google Scholar] [CrossRef]
- Huang, W.Q.; Lu, C.X.; Zhang, Y.; Yi, K.H.; Cai, L.L.; Li, M.L.; Wang, H.; Lin, Q.; Tzeng, C.M. A Novel CCM2 Gene Mutation Associated with Familial Cerebral Cavernous Malformation. Front. Aging Neurosci. 2016, 8, 220. [Google Scholar] [CrossRef]
- Yang, I.Y.; Yum, M.S.; Kim, E.H.; Choi, H.W.; Yoo, H.W.; Ko, T.S. Two cases of familial cerebral cavernous malformation caused by mutations in the CCM1 gene. Korean J. Pediatr. 2016, 59, 280–284. [Google Scholar] [CrossRef] [Green Version]
- Noushad, M.; Bhattacharjee, S.; Weatherby, S.J.; Whitefield, P. A British family with familial cerebral cavernous malformation due to a rare mutation of the CCM2 gene. Acta Neurol. Belg. 2020, 120, 1227–1229. [Google Scholar] [CrossRef] [PubMed]
- Eren Gozel, H.; Kök, K.; Ozlen, F.; Isler, C.; Pence, S. A novel insight into differential expression profiles of sporadic cerebral cavernous malformation patients with different symptoms. Sci. Rep. 2021, 11, 19351. [Google Scholar] [CrossRef] [PubMed]
- Arkar, U.; Vipotnik Vesnaver, T.; Maver, A.; Perković Benedik, M.; Peterlin, B.; Osredkar, D. Children with cavernous malformations of the central nervous system. Eur. J. Paediatr. Neurol. 2021, 35, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Orlev, A.; Feghali, J.; Kimchi, G.; Salomon, M.; Berkowitz, S.; Oxman, L.; Levitan, I.; Knoller, N.; Auriel, E.; Huang, J.; et al. Neurological event prediction for patients with symptomatic cerebral cavernous malformation: The BLED2 score. J. Neurosurg. 2021, 1–8. [Google Scholar] [CrossRef]
- Chou, C.J.; Lee, C.C.; Chen, C.J.; Yang, H.C.; Peng, S.J. Displacement of Gray Matter and Incidence of Seizures in Patients with Cerebral Cavernous Malformations. Biomedicines 2021, 9, 1872. [Google Scholar] [CrossRef] [PubMed]
- Moriarity, J.L.; Wetzel, M.; Clatterbuck, R.E.; Javedan, S.; Sheppard, J.M.; Hoenig-Rigamonti, K.; Crone, N.E.; Breiter, S.N.; Lee, R.R.; Rigamonti, D. The natural history of cavernous malformations: A prospective study of 68 patients. Neurosurgery 1999, 44, 1166–1171. [Google Scholar]
- Cossu, M.; Raneri, F.; Casaceli, G.; Gozzo, F.; Pelliccia, V.; Lo Russo, G. Surgical treatment of cavernoma-related epilepsy. J. Neurosurg. Sci. 2015, 59, 237–253. [Google Scholar]
- Schuss, P.; Marx, J.; Borger, V.; Brandecker, S.; Güresir, Á.; Hadjiathanasiou, A.; Hamed, M.; Schneider, M.; Surges, R.; Vatter, H.; et al. Cavernoma-related epilepsy in cavernous malformations located within the temporal lobe: Surgical management and seizure outcome. Neurosurg. Focus 2020, 48, E6. [Google Scholar] [CrossRef] [Green Version]
- Gross, B.A.; Lin, N.; Du, R.; Day, A.L. The natural history of intracranial cavernous malformations. Neurosurg. Focus 2011, 30, E24. [Google Scholar] [CrossRef]
- Schneble, H.M.; Soumare, A.; Hervé, D.; Bresson, D.; Guichard, J.P.; Riant, F.; Tournier-Lasserve, E.; Tzourio, C.; Chabriat, H.; Stapf, C. Antithrombotic therapy and bleeding risk in a prospective cohort study of patients with cerebral cavernous malformations. Stroke 2012, 43, 3196–3199. [Google Scholar] [CrossRef] [Green Version]
- Baumann, C.R.; Acciarri, N.; Bertalanffy, H.; Devinsky, O.; Elger, C.E.; Lo Russo, G.; Cossu, M.; Sure, U.; Singh, A.; Stefan, H.; et al. Seizure outcome after resection of supratentorial cavernous malformations: A study of 168 patients. Epilepsia 2007, 48, 559–563. [Google Scholar] [CrossRef] [PubMed]
- Stavrou, I.; Baumgartner, C.; Frischer, J.M.; Trattnig, S.; Knosp, E. Long-term seizure control after resection of supratentorial cavernomas: A retrospective single-center study in 53 patients. Neurosurgery 2008, 63, 888–896. [Google Scholar] [CrossRef] [PubMed]
- Dammann, P.; Wrede, K.; Jabbarli, R.; Neuschulte, S.; Menzler, K.; Zhu, Y.; Özkan, N.; Müller, O.; Forsting, M.; Rosenow, F.; et al. Outcome after conservative management or surgical treatment for new-onset epilepsy in cerebral cavernous malformation. J. Neurosurg. 2017, 126, 1303–1311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozlen, F.; Isler, C.; Akgun, M.Y.; Ozkara, C.; Karabacak, M.; Delil, S.; Yilmaz Oz, B.; Tahmazoglu, B.; Uzan, M. Factors Affecting Seizure Outcomes After Surgery for Cavernoma Related Epilepsy. Turk. Neurosurg. 2021. [Google Scholar] [CrossRef]
- Churchyard, A.; Khangure, M.; Grainger, K. Cerebral cavernous angioma: A potentially benign condition? Successful treatment in 16 cases. J. Neurol. Neurosurg. Psychiatry 1992, 55, 1040–1045. [Google Scholar] [CrossRef] [Green Version]
- Simard, J.M.; Garcia-Bengochea, F.; Ballinger, W.E., Jr.; Mickle, J.P.; Quisling, R.G. Cavernous angioma: A review of 126 collected and 12 new clinical cases. Neurosurgery 1986, 18, 162–172. [Google Scholar] [CrossRef]
- Ferroli, P.; Casazza, M.; Marras, C.; Mendola, C.; Franzini, A.; Broggi, G. Cerebral cavernomas and seizures: A retrospective study on 163 patients who underwent pure lesionectomy. Neurol. Sci. 2006, 26, 390–394. [Google Scholar] [CrossRef]
- Rosenow, F.; Alonso-Vanegas, M.A.; Baumgartner, C.; Blümcke, I.; Carreño, M.; Gizewski, E.R.; Hamer, H.M.; Knake, S.; Kahane, P.; Lüders, H.O.; et al. Cavernoma-related epilepsy: Review and recommendations for management–Report of the Surgical Task Force of the ILAE Commission on Therapeutic Strategies. Epilepsia 2013, 54, 2025–2035. [Google Scholar] [CrossRef]
- Noto, S.; Fujii, M.; Akimura, T.; Imoto, H.; Nomura, S.; Kajiwara, K.; Kato, S.; Fujisawa, H.; Suzuki, M. Management of patients with cavernous angiomas presenting epileptic seizures. Surg. Neurol. 2005, 64, 495–498; discussion 498–499. [Google Scholar] [CrossRef]
- Josephson, C.B.; Leach, J.P.; Duncan, R.; Roberts, R.C.; Counsell, C.E.; Al-Shahi Salman, R. Seizure risk from cavernous or arteriovenous malformations: Prospective population-based study. Neurology 2011, 76, 1548–1554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janmohamed, M.; Brodie, M.J.; Kwan, P. Pharmacoresistance—Epidemiology, mechanisms, and impact on epilepsy treatment. Neuropharmacology 2020, 168, 107790. [Google Scholar] [CrossRef] [PubMed]
- Wieser, H.G.; Blume, W.T.; Fish, D.; Goldensohn, E.; Hufnagel, A.; King, D.; Sperling, M.R.; Lüders, H.; Pedley, T.A. ILAE Commission Report. Proposal for a new classification of outcome with respect to epileptic seizures following epilepsy surgery. Epilepsia 2001, 42, 282–286. [Google Scholar] [CrossRef] [PubMed]
- Di Gennaro, G.; Quarato, P.P.; Sebastiano, F.; Esposito, V.; Onorati, P.; Mascia, A.; Romanelli, P.; Grammaldo, L.G.; Falco, C.; Scoppetta, C.; et al. Postoperative EEG and seizure outcome in temporal lobe epilepsy surgery. Clin. Neurophysiol. 2004, 115, 1212–1219. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.S.; Kim, S.H.; Chang, J.H.; Park, M.; Cha, Y.J. Clinicopathological differences in radiation-induced organizing hematomas of the brain based on type of radiation treatment and primary lesions. J. Pathol. Transl. Med. 2022, 56, 16–21. [Google Scholar] [CrossRef]
- Nimjee, S.M.; Powers, C.J.; Bulsara, K.R. Review of the literature on de novo formation of cavernous malformations of the central nervous system after radiation therapy. Neurosurg. Focus 2006, 21, e4. [Google Scholar] [CrossRef]
- Willmore, L.J.; Sypert, G.W.; Munson, J.V.; Hurd, R.W. Chronic focal epileptiform discharges induced by injection of iron into rat and cat cortex. Science 1978, 200, 1501–1503. [Google Scholar] [CrossRef]
- Seiffert, E.; Dreier, J.P.; Ivens, S.; Bechmann, I.; Tomkins, O.; Heinemann, U.; Friedman, A. Lasting blood-brain barrier disruption induces epileptic focus in the rat somatosensory cortex. J. Neurosci. 2004, 24, 7829–7836. [Google Scholar] [CrossRef] [Green Version]
- Seifert, G.; Schilling, K.; Steinhäuser, C. Astrocyte dysfunction in neurological disorders: A molecular perspective. Nat. Rev. Neurosci. 2006, 7, 194–206. [Google Scholar] [CrossRef]
- Dammann, P.; Schaller, C.; Sure, U. Should we resect peri-lesional hemosiderin deposits when performing lesionectomy in patients with cavernoma-related epilepsy (CRE)? Neurosurg. Rev. 2017, 40, 39–43. [Google Scholar] [CrossRef]
- Baumann, C.R.; Schuknecht, B.; Lo Russo, G.; Cossu, M.; Citterio, A.; Andermann, F.; Siegel, A.M. Seizure outcome after resection of cavernous malformations is better when surrounding hemosiderin-stained brain also is removed. Epilepsia 2006, 47, 563–566. [Google Scholar] [CrossRef] [PubMed]
- Maciunas, J.A.; Syed, T.U.; Cohen, M.L.; Werz, M.A.; Maciunas, R.J.; Koubeissi, M.Z. Triple pathology in epilepsy: Coexistence of cavernous angiomas and cortical dysplasias with other lesions. Epilepsy Res. 2010, 91, 106–110. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, Y.; Sato, Y.; Sugiyama, T.; Mizutani, T. Intraoperative epileptogenic network visualization using gamma oscillation regularity correlation analysis in epilepsy surgery. Surg. Neurol. Int. 2021, 12, 254. [Google Scholar] [CrossRef] [PubMed]
- D’Cruz, J.; Hefner, M.; Ledbetter, C.; Frilot, C.; Howard, B.; Zhu, P.; Riel-Romero, R.; Notarianni, C.; Toledo, E.G.; Nanda, A.; et al. Focal epilepsy caused by single cerebral cavernous malformation (CCM) is associated with regional and global resting state functional connectivity (FC) disruption. Neuroimage Clin. 2019, 24, 102072. [Google Scholar] [CrossRef]
- Sevy, A.; Gavaret, M.; Trebuchon, A.; Vaugier, L.; Wendling, F.; Carron, R.; Regis, J.; Chauvel, P.; Gonigal, A.M.; Bartolomei, F. Beyond the lesion: The epileptogenic networks around cavernous angiomas. Epilepsy Res. 2014, 108, 701–708. [Google Scholar] [CrossRef]
- Kobayashi, E.; Bagshaw, A.P.; Gotman, J.; Dubeau, F. Metabolic correlates of epileptic spikes in cerebral cavernous angiomas. Epilepsy Res. 2007, 73, 98–103. [Google Scholar] [CrossRef]
- Kapadia, M.; Walwema, M.; Smith, T.R.; Bellinski, I.; Batjer, H.; Getch, C.; Rosenow, J.M.; Bendok, B.R.; Schuele, S.U. Seizure outcome in patients with cavernous malformation after early surgery. Epilepsy Behav. 2021, 115, 107662. [Google Scholar] [CrossRef]
- von der Brelie, C.; Malter, M.P.; Niehusmann, P.; Elger, C.E.; von Lehe, M.; Schramm, J. Surgical management and long-term seizure outcome after epilepsy surgery for different types of epilepsy associated with cerebral cavernous malformations. Epilepsia 2013, 54, 1699–1706. [Google Scholar] [CrossRef]
- von der Brelie, C.; Kuczaty, S.; von Lehe, M. Surgical management and long-term outcome of pediatric patients with different subtypes of epilepsy associated with cerebral cavernous malformations. J. Neurosurg. Pediatr. 2014, 13, 699–705. [Google Scholar] [CrossRef] [Green Version]
- Yang, P.F.; Pei, J.S.; Jia, Y.Z.; Lin, Q.; Xiao, H.; Zhang, T.T.; Zhong, Z.H. Surgical Management and Long-Term Seizure Outcome After Surgery for Temporal Lobe Epilepsy Associated with Cerebral Cavernous Malformations. World Neurosurg. 2018, 110, e659–e670. [Google Scholar] [CrossRef]


{kind=link}
| Seizuire Freedom | ILAE Class I (Complete Seizure Freedome) without Epileptiform Discharges | ILAE Class ≤II and/or Epileptiform discharges | p-Value |
|---|---|---|---|
| Number of patients | 12(48%) | 13(52%) | n/a |
| Sex (Female: Male) | 3:9 | 4:9 | 0.75 |
| Age at surgery (mean, range, SD) | 28.6, 10–45, 11.1 | 43.6, 9–62, 17.7 | 0.018 * |
| Epilepsy history (year) [mean, range, SD] | 9.2, 2–31, 9.1 | 11.5, 2–35, 12.0 | 0.64 |
| Single vs. Multiple lesions (Single: Multiple) | 12:0 | 11:2 | 0.34 |
| Pre-perative ASM (mean, range, SD) | 2.4, 1–4, 1.2 | 2.9, 1–5, 1.0 | 0.28 |
| Number of Post-operative ASM (mean, range, SD) | n/a | 1.5, 1–3, 0.7 | n/a |
| Size of BCA (mm) [mean, range, SD] | 28.4,1.5–190, 51.8 | 8.9, 5–16.1, 3.3 | 0.15 |
| Post operative follow-up period (year) | 7.3, 1–18, 4.9 | 6.2, 1–12, 3.5 | 0.55 |
| Location of BCA | 0.08 | ||
| Frontal | 4 | 1 | |
| Temporal | 8 | 11 | |
| Occipital | 0 | 1 | |
| Coefficient | Standard Error | p-Value | |
|---|---|---|---|
| Multi-variate logistic regression analysis | |||
| Age at surgery (year old) | 0.133 | 0.066 | 0.043 * |
| Size of BCA | −0.072 | 0.124 | 0.562 |
| Epilepsy history (years) | −0.028 | 0.051 | 0.581 |
| Location of BCA | 3.204 | 2.122 | 0.131 |
| Univariate-logistic regression analysis | |||
| Age at surgery (year old) | 0.0144 | 0.006 | 0.019 * |
| Size of BCA | −0.004 | 0.003 | 0.191 |
| Epilepsy history (years) | 0.006 | 0.01 | 0.585 |
| Location of BCA | 0.296 | 0.166 | 0.088 |
| Coefficient | Standard Error | p-Value | |
|---|---|---|---|
| Multi-variate logistic regression analysis | |||
| Age at surgery (year old) | 0.130 | 0.065 | 0.046 * |
| Size of BCA | −0.075 | 0.123 | 0.543 |
| Epilepsy history (years) | −0.026 | 0.051 | 0.61 |
| Location of BCA | 2.787 | 2.497 | 0.264 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fujimoto, A.; Enoki, H.; Hatano, K.; Sato, K.; Okanishi, T. Earlier Age at Surgery for Brain Cavernous Angioma-Related Epilepsy May Achieve Complete Seizure Freedom without Aid of Anti-Seizure Medication. Brain Sci. 2022, 12, 403. https://doi.org/10.3390/brainsci12030403
Fujimoto A, Enoki H, Hatano K, Sato K, Okanishi T. Earlier Age at Surgery for Brain Cavernous Angioma-Related Epilepsy May Achieve Complete Seizure Freedom without Aid of Anti-Seizure Medication. Brain Sciences. 2022; 12(3):403. https://doi.org/10.3390/brainsci12030403
Chicago/Turabian StyleFujimoto, Ayataka, Hideo Enoki, Keisuke Hatano, Keishiro Sato, and Tohru Okanishi. 2022. "Earlier Age at Surgery for Brain Cavernous Angioma-Related Epilepsy May Achieve Complete Seizure Freedom without Aid of Anti-Seizure Medication" Brain Sciences 12, no. 3: 403. https://doi.org/10.3390/brainsci12030403