
Endoscopic Endonasal Skull Base Surgery Complication Avoidance: A Contemporary Review

{kind=link}
Abstract
:1. Introduction
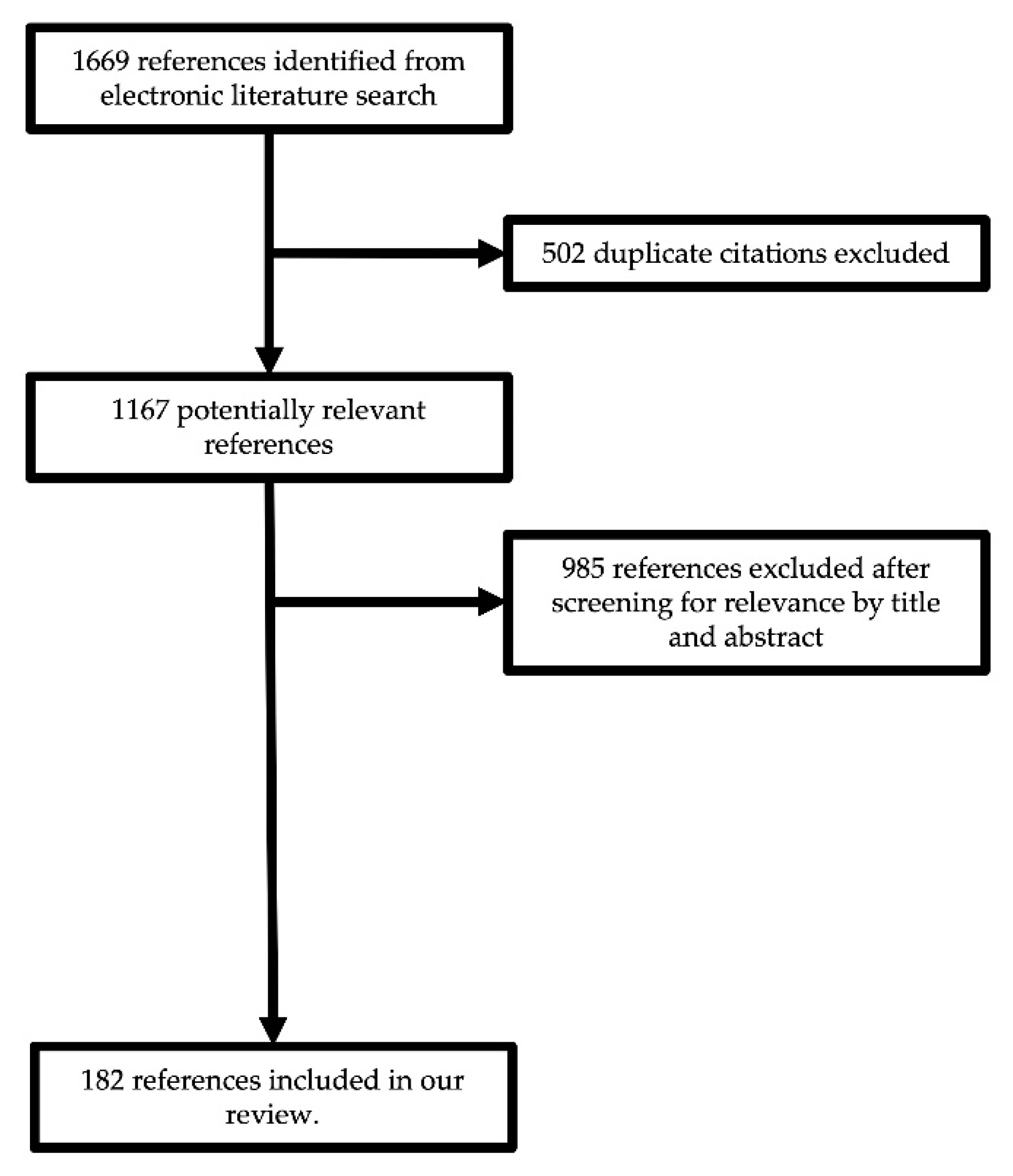
2. Materials and Methods
3. CSF Leak
3.1. Pre-Operative Risk Factors
3.2. Intra-Operative Risk Factors
4. Optic Nerve Damage
5. Other Cranial Nerve Deficits
6. Pituitary Gland Dysfunction
7. Internal Carotid Artery Injury
8. Infection
9. Other Complications and Peri-Operative Considerations
9.1. Venous Thromboembolism
9.2. Cerebral Infarction
9.3. Pneumocephalus
9.4. Peri-Operative Considerations
10. Sinonasal Morbidities and Postoperative Quality of Life
10.1. Nasoseptal Flap Reconstruction
10.2. Olfaction
10.3. Sensory Changes
10.4. Aesthetic
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carrau, R.L.; Jho, H.D.; Ko, Y. Transnasal-Transsphenoidal Endoscopic Surgery of the Pituitary Gland. Laryngoscope 1996, 106, 914–918. [Google Scholar] [CrossRef] [PubMed]
- Jankowski, R.; Auque, J.; Simon, C.; Marchal, J.C.; Hepner, H.; Wayoff, M. Endoscopic Pituitary Tumor Surgery. Laryngoscope 1992, 102, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Halves, E.; Bushe, K.A. Transsphenoidal Operation on Craniopharyngiomas with Extrasellar Extensions. The Advantage of the Operating Endoscope [Proceedings]. Acta Neurochir. Suppl. 1979, 28, 362. [Google Scholar] [PubMed]
- Eloy, J.A.; Vivero, R.J.; Hoang, K.; Civantos, F.J.; Weed, D.T.; Morcos, J.J.; Casiano, R.R. Comparison of Transnasal Endoscopic and Open Craniofacial Resection for Malignant Tumors of the Anterior Skull Base. Laryngoscope 2009, 119, 834–840. [Google Scholar] [CrossRef] [PubMed]
- Moussazadeh, N.; Prabhu, V.; Bander, E.D.; Cusic, R.C.; Tsiouris, A.J.; Anand, V.K.; Schwartz, T.H. Endoscopic Endonasal versus Open Transcranial Resection of Craniopharyngiomas: A Case-Matched Single-Institution Analysis. Neurosurg. Focus 2016, 41, E7. [Google Scholar] [CrossRef] [Green Version]
- Laws, E.R.; Kanter, A.S.; Jane, J.A.; Dumont, A.S. Extended Transsphenoidal Approach. J. Neurosurg. 2005, 102, 825–827, discussion 827–828. [Google Scholar] [CrossRef]
- Paluzzi, A.; Fernandez-Miranda, J.C.; Tonya Stefko, S.; Challinor, S.; Snyderman, C.H.; Gardner, P.A. Endoscopic Endonasal Approach for Pituitary Adenomas: A Series of 555 Patients. Pituitary 2014, 17, 307–319. [Google Scholar] [CrossRef]
- Kerr, E.E.; Prevedello, D.M.; Jamshidi, A.; Ditzel Filho, L.F.; Otto, B.A.; Carrau, R.L. Immediate Complications Associated with High-Flow Cerebrospinal Fluid Egress during Endoscopic Endonasal Skull Base Surgery. Neurosurg. Focus 2014, 37, E3. [Google Scholar] [CrossRef] [Green Version]
- Lai, L.T.; Trooboff, S.; Morgan, M.K.; Harvey, R.J. The Risk of Meningitis Following Expanded Endoscopic Endonasal Skull Base Surgery: A Systematic Review. J. Neurol. Surg. B Skull Base 2014, 75, 18–26. [Google Scholar] [CrossRef] [Green Version]
- Ivan, M.E.; Iorgulescu, J.B.; El-Sayed, I.; McDermott, M.W.; Parsa, A.T.; Pletcher, S.D.; Jahangiri, A.; Wagner, J.; Aghi, M.K. Risk Factors for Postoperative Cerebrospinal Fluid Leak and Meningitis after Expanded Endoscopic Endonasal Surgery. J. Clin. Neurosci. 2015, 22, 48–54. [Google Scholar] [CrossRef]
- Rizvi, Z.H.; Ferrandino, R.; Luu, Q.; Suh, J.D.; Wang, M.B. Nationwide Analysis of Unplanned 30-Day Readmissions after Transsphenoidal Pituitary Surgery. Int. Forum Allergy Rhinol. 2019, 9, 322–329. [Google Scholar] [CrossRef]
- Grotenhuis, J.A. Costs of Postoperative Cerebrospinal Fluid Leakage: 1-Year, Retrospective Analysis of 412 Consecutive Nontrauma Cases. Surg. Neurol. 2005, 64, 490–493, discussion 493–494. [Google Scholar] [CrossRef] [PubMed]
- Fraser, S.; Gardner, P.A.; Koutourousiou, M.; Kubik, M.; Fernandez-Miranda, J.C.; Snyderman, C.H.; Wang, E.W. Risk Factors Associated with Postoperative Cerebrospinal Fluid Leak after Endoscopic Endonasal Skull Base Surgery. J. Neurosurg. 2018, 128, 1066–1071. [Google Scholar] [CrossRef] [PubMed]
- Karnezis, T.T.; Baker, A.B.; Soler, Z.M.; Wise, S.K.; Rereddy, S.K.; Patel, Z.M.; Oyesiku, N.M.; DelGaudio, J.M.; Hadjipanayis, C.G.; Woodworth, B.A.; et al. Factors Impacting Cerebrospinal Fluid Leak Rates in Endoscopic Sellar Surgery. Int. Forum Allergy Rhinol. 2016, 6, 1117–1125. [Google Scholar] [CrossRef] [PubMed]
- Boling, C.C.; Karnezis, T.T.; Baker, A.B.; Lawrence, L.A.; Soler, Z.M.; Vandergrift, W.A.; Wise, S.K.; DelGaudio, J.M.; Patel, Z.M.; Rereddy, S.K.; et al. Multi-Institutional Study of Risk Factors for Perioperative Morbidity Following Transnasal Endoscopic Pituitary Adenoma Surgery. Int. Forum Allergy Rhinol. 2016, 6, 101–107. [Google Scholar] [CrossRef]
- Dlouhy, B.J.; Madhavan, K.; Clinger, J.D.; Reddy, A.; Dawson, J.D.; O’Brien, E.K.; Chang, E.; Graham, S.M.; Greenlee, J.D.W. Elevated Body Mass Index and Risk of Postoperative CSF Leak Following Transsphenoidal Surgery. J. Neurosurg. 2012, 116, 1311–1317. [Google Scholar] [CrossRef]
- Cohen, S.; Jones, S.H.; Dhandapani, S.; Negm, H.M.; Anand, V.K.; Schwartz, T.H. Lumbar Drains Decrease the Risk of Postoperative Cerebrospinal Fluid Leak Following Endonasal Endoscopic Surgery for Suprasellar Meningiomas in Patients with High Body Mass Index. Oper. Neurosurg. 2018, 14, 66–71. [Google Scholar] [CrossRef]
- Jeon, C.; Hong, S.D.; Seol, H.J.; Lee, J.-I.; Nam, D.-H.; Hwang, Y.J.; Kong, D.-S. Reconstructive Outcome of Intraoperative Cerebrospinal Fluid Leak after Endoscopic Endonasal Surgery for Tumors Involving Skull Base. J. Clin. Neurosci. 2017, 45, 227–231. [Google Scholar] [CrossRef]
- Mortuaire, G.; Vandeville, S.; Assaker, R.; Chevalier, D. Endoscopic Repair of Anterior or Middle Skull Base Cerebrospinal Fluid Leaks after Tumour Resection. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2012, 129, 77–81. [Google Scholar] [CrossRef] [Green Version]
- Thawani, J.P.; Ramayya, A.G.; Pisapia, J.M.; Abdullah, K.G.; Lee, J.Y.-K.; Grady, M.S. Operative Strategies to Minimize Complications Following Resection of Pituitary Macroadenomas. J. Neurol. Surg. B Skull Base 2017, 78, 184–190. [Google Scholar] [CrossRef]
- Zhou, Q.; Yang, Z.; Wang, X.; Wang, Z.; Zhao, C.; Zhang, S.; Li, P.; Li, S.; Liu, P. Risk Factors and Management of Intraoperative Cerebrospinal Fluid Leaks in Endoscopic Treatment of Pituitary Adenoma: Analysis of 492 Patients. World Neurosurg. 2017, 101, 390–395. [Google Scholar] [CrossRef] [PubMed]
- Gruss, C.L.; Al Komser, M.; Aghi, M.K.; Pletcher, S.D.; Goldberg, A.N.; McDermott, M.; El-Sayed, I.H. Risk Factors for Cerebrospinal Leak after Endoscopic Skull Base Reconstruction with Nasoseptal Flap. Otolaryngol. Head Neck Surg. 2014, 151, 516–521. [Google Scholar] [CrossRef] [PubMed]
- Przybylowski, C.J.; Dallapiazza, R.F.; Williams, B.J.; Pomeraniec, I.J.; Xu, Z.; Payne, S.C.; Laws, E.R.; Jane, J.A. Primary versus Revision Transsphenoidal Resection for Nonfunctioning Pituitary Macroadenomas: Matched Cohort Study. J. Neurosurg. 2017, 126, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Fomichev, D.; Kalinin, P.; Kutin, M.; Sharipov, O. Extended Transsphenoidal Endoscopic Endonasal Surgery of Suprasellar Craniopharyngiomas. World Neurosurg. 2016, 94, 181–187. [Google Scholar] [CrossRef]
- Stapleton, A.L.; Tyler-Kabara, E.C.; Gardner, P.A.; Snyderman, C.H.; Wang, E.W. Risk Factors for Cerebrospinal Fluid Leak in Pediatric Patients Undergoing Endoscopic Endonasal Skull Base Surgery. Int. J. Pediatr. Otorhinolaryngol. 2017, 93, 163–166. [Google Scholar] [CrossRef]
- Shikary, T.; Andaluz, N.; Meinzen-Derr, J.; Edwards, C.; Theodosopoulos, P.; Zimmer, L.A. Operative Learning Curve After Transition to Endoscopic Transsphenoidal Pituitary Surgery. World Neurosurg. 2017, 102, 608–612. [Google Scholar] [CrossRef]
- Soudry, E.; Turner, J.H.; Nayak, J.V.; Hwang, P.H. Endoscopic Reconstruction of Surgically Created Skull Base Defects: A Systematic Review. Otolaryngol. Head Neck Surg. 2014, 150, 730–738. [Google Scholar] [CrossRef]
- Pereira, E.A.C.; Grandidge, C.A.; Nowak, V.A.; Cudlip, S.A. Cerebrospinal Fluid Leaks after Transsphenoidal Surgery—Effect of a Polyethylene Glycol Hydrogel Dural Sealant. J. Clin. Neurosci. 2017, 44, 6–10. [Google Scholar] [CrossRef]
- Magro, E.; Graillon, T.; Lassave, J.; Castinetti, F.; Boissonneau, S.; Tabouret, E.; Fuentes, S.; Velly, L.; Gras, R.; Dufour, H. Complications Related to the Endoscopic Endonasal Transsphenoidal Approach for Nonfunctioning Pituitary Macroadenomas in 300 Consecutive Patients. World Neurosurg. 2016, 89, 442–453. [Google Scholar] [CrossRef]
- Clark, A.J.; Jahangiri, A.; Garcia, R.M.; George, J.R.; Sughrue, M.E.; McDermott, M.W.; El-Sayed, I.H.; Aghi, M.K. Endoscopic Surgery for Tuberculum Sellae Meningiomas: A Systematic Review and Meta-Analysis. Neurosurg. Rev. 2013, 36, 349–359. [Google Scholar] [CrossRef]
- Turel, M.K.; Tsermoulas, G.; Reddy, D.; Andrade-Barazarte, H.; Zadeh, G.; Gentili, F. Endonasal Endoscopic Transsphenoidal Excision of Tuberculum Sellae Meningiomas: A Systematic Review. J. Neurosurg. Sci 2016, 60, 463–475. [Google Scholar] [PubMed]
- Mascarenhas, L.; Moshel, Y.A.; Bayad, F.; Szentirmai, O.; Salek, A.A.; Leng, L.Z.; Hofstetter, C.P.; Placantonakis, D.G.; Tsiouris, A.J.; Anand, V.K.; et al. The Transplanum Transtuberculum Approaches for Suprasellar and Sellar-Suprasellar Lesions: Avoidance of Cerebrospinal Fluid Leak and Lessons Learned. World Neurosurg. 2014, 82, 186–195. [Google Scholar] [CrossRef] [PubMed]
- Little, R.E.; Taylor, R.J.; Miller, J.D.; Ambrose, E.C.; Germanwala, A.V.; Sasaki-Adams, D.M.; Ewend, M.G.; Zanation, A.M. Endoscopic Endonasal Transclival Approaches: Case Series and Outcomes for Different Clival Regions. J. Neurol. Surg. B Skull Base 2014, 75, 247–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cutler, A.R.; Mundi, J.S.; Solomon, N.; Suh, J.D.; Wang, M.B.; Bergsneider, M. Critical Appraisal of Extent of Resection of Clival Lesions Using the Expanded Endoscopic Endonasal Approach. J. Neurol. Surg. B Skull Base 2013, 74, 217–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, N.C.-W.; Naidoo, Y.; Oue, S.; Alexander, H.; Robinson, S.; Wickremesekera, A.; Floreani, S.; Vrodos, N.; Santoreneos, S.; Ooi, E.; et al. Endoscopic Surgery of Skull Base Chordomas. J. Neurol. Surg. B Skull Base 2012, 73, 379–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chibbaro, S.; Cebula, H.; Aldea, S.; Baussart, B.; Tigan, L.; Todeschi, J.; Romano, A.; Ganau, M.; Debry, C.; Servadei, F.; et al. Endonasal Endoscopic Odontoidectomy in Ventral Diseases of the Craniocervical Junction: Results of a Multicenter Experience. World Neurosurg. 2017, 106, 382–393. [Google Scholar] [CrossRef]
- Zwagerman, N.T.; Tormenti, M.J.; Tempel, Z.J.; Wang, E.W.; Snyderman, C.H.; Fernandez-Miranda, J.C.; Gardner, P.A. Endoscopic Endonasal Resection of the Odontoid Process: Clinical Outcomes in 34 Adults. J. Neurosurg. 2018, 128, 923–931. [Google Scholar] [CrossRef]
- Shriver, M.F.; Kshettry, V.R.; Sindwani, R.; Woodard, T.; Benzel, E.C.; Recinos, P.F. Transoral and Transnasal Odontoidectomy Complications: A Systematic Review and Meta-Analysis. Clin. Neurol Neurosurg. 2016, 148, 121–129. [Google Scholar] [CrossRef]
- Zanation, A.M.; Carrau, R.L.; Snyderman, C.H.; Germanwala, A.V.; Gardner, P.A.; Prevedello, D.M.; Kassam, A.B. Nasoseptal Flap Reconstruction of High Flow Intraoperative Cerebral Spinal Fluid Leaks during Endoscopic Skull Base Surgery. Am. J. Rhinol. Allergy 2009, 23, 518–521. [Google Scholar] [CrossRef]
- Oakley, G.M.; Alt, J.A.; Schlosser, R.J.; Harvey, R.J.; Orlandi, R.R. Diagnosis of Cerebrospinal Fluid Rhinorrhea: An Evidence-Based Review with Recommendations. Int. Forum Allergy Rhinol. 2016, 6, 8–16. [Google Scholar] [CrossRef]
- Thorp, B.D.; Sreenath, S.B.; Ebert, C.S.; Zanation, A.M. Endoscopic Skull Base Reconstruction: A Review and Clinical Case Series of 152 Vascularized Flaps Used for Surgical Skull Base Defects in the Setting of Intraoperative Cerebrospinal Fluid Leak. Neurosurg. Focus 2014, 37, E4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harvey, R.J.; Parmar, P.; Sacks, R.; Zanation, A.M. Endoscopic Skull Base Reconstruction of Large Dural Defects: A Systematic Review of Published Evidence. Laryngoscope 2012, 122, 452–459. [Google Scholar] [CrossRef]
- Roxbury, C.R.; Saavedra, T.; Ramanathan, M.; Lim, M.; Ishii, M.; Gallia, G.L.; Reh, D.D. Layered Sellar Reconstruction with Avascular Free Grafts: Acceptable Alternative to the Nasoseptal Flap for Repair of Low-Volume Intraoperative Cerebrospinal Fluid Leak. Am. J. Rhinol. Allergy 2016, 30, 367–371. [Google Scholar] [CrossRef] [PubMed]
- Shahangian, A.; Soler, Z.M.; Baker, A.; Wise, S.K.; Rereddy, S.K.; Patel, Z.M.; Oyesiku, N.M.; DelGaudio, J.M.; Hadjipanayis, C.G.; Woodworth, B.A.; et al. Successful Repair of Intraoperative Cerebrospinal Fluid Leaks Improves Outcomes in Endoscopic Skull Base Surgery. Int. Forum Allergy Rhinol. 2017, 7, 80–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaskes, M.B.; Barton, B.; Karsy, M.; Chitguppi, C.; McKnight, T.; McCambridge, J.; Flanders, A.; Toskala, E.; Rabinowitz, M.R.; Nyquist, G.G.; et al. An Algorithm for Sellar Reconstruction Following Endoscopic Transsphenoidal Surgery for Pituitary Adenoma: A Review of 582 Cases. Int. Forum Allergy Rhinol. 2022, 12, 1120–1130. [Google Scholar] [CrossRef]
- Ransom, E.R.; Palmer, J.N.; Kennedy, D.W.; Chiu, A.G. Assessing Risk/Benefit of Lumbar Drain Use for Endoscopic Skull-Base Surgery. Int. Forum Allergy Rhinol. 2011, 1, 173–177. [Google Scholar] [CrossRef]
- Wang, E.W.; Zanation, A.M.; Gardner, P.A.; Schwartz, T.H.; Eloy, J.A.; Adappa, N.D.; Bettag, M.; Bleier, B.S.; Cappabianca, P.; Carrau, R.L.; et al. ICAR: Endoscopic Skull-Base Surgery. Int. Forum Allergy Rhinol. 2019, 9, S145–S365. [Google Scholar] [CrossRef] [PubMed]
- D’Anza, B.; Tien, D.; Stokken, J.K.; Recinos, P.F.; Woodard, T.R.; Sindwani, R. Role of Lumbar Drains in Contemporary Endonasal Skull Base Surgery: Meta-Analysis and Systematic Review. Am. J. Rhinol. Allergy 2016, 30, 430–435. [Google Scholar] [CrossRef]
- Zwagerman, N.T.; Wang, E.W.; Shin, S.S.; Chang, Y.-F.; Fernandez-Miranda, J.C.; Snyderman, C.H.; Gardner, P.A. Does Lumbar Drainage Reduce Postoperative Cerebrospinal Fluid Leak after Endoscopic Endonasal Skull Base Surgery? A Prospective, Randomized Controlled Trial. J. Neurosurg. 2018, 131, 1172–1178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrante, E.; Ferraroni, M.; Castrignanò, T.; Menicatti, L.; Anagni, M.; Reimondo, G.; Del Monte, P.; Bernasconi, D.; Loli, P.; Faustini-Fustini, M.; et al. Non-Functioning Pituitary Adenoma Database: A Useful Resource to Improve the Clinical Management of Pituitary Tumors. Eur. J. Endocrinol. 2006, 155, 823–829. [Google Scholar] [CrossRef]
- Laws, E.R.; Thapar, K. Pituitary Surgery. Endocrinol. Metab. Clin. N. Am. 1999, 28, 119–131. [Google Scholar] [CrossRef] [PubMed]
- Molitch, M.E. Nonfunctioning Pituitary Tumors and Pituitary Incidentalomas. Endocrinol. Metab. Clin. N. Am. 2008, 37, 151–171, xi. [Google Scholar] [CrossRef]
- De Witte, O.; Carlot, S.; Devuyst, E.; Choufani, G.; Hassid, S. Minimally Invasive Endoscopic Unilateral Transsphenoidal Surgery for Pituitary Adenomas. B-ENT 2011, 7 (Suppl. S17), 27–32. [Google Scholar] [PubMed]
- Anderson, D.; Faber, P.; Marcovitz, S.; Hardy, J.; Lorenzetti, D. Pituitary Tumors and the Ophthalmologist. Ophthalmology 1983, 90, 1265–1270. [Google Scholar] [CrossRef] [PubMed]
- Newman, S.A.; Turbin, R.E.; Bodach, M.E.; Tumialan, L.M.; Oyesiku, N.M.; Litvack, Z.; Zada, G.; Patil, C.G.; Aghi, M.K. Congress of Neurological Surgeons Systematic Review and Evidence-Based Guideline on Pretreatment Ophthalmology Evaluation in Patients with Suspected Nonfunctioning Pituitary Adenomas. Neurosurgery 2016, 79, E530–E532. [Google Scholar] [CrossRef] [Green Version]
- Thotakura, A.K.; Patibandla, M.R.; Panigrahi, M.K.; Addagada, G.C. Predictors of Visual Outcome with Transsphenoidal Excision of Pituitary Adenomas Having Suprasellar Extension: A Prospective Series of 100 Cases and Brief Review of the Literature. Asian J. Neurosurg. 2017, 12, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Nakao, N.; Itakura, T. Surgical Outcome of the Endoscopic Endonasal Approach for Non-Functioning Giant Pituitary Adenoma. J. Clin. Neurosci. 2011, 18, 71–75. [Google Scholar] [CrossRef]
- Anik, I.; Anik, Y.; Koc, K.; Ceylan, S.; Genc, H.; Altintas, O.; Ozdamar, D.; Baykal Ceylan, D. Evaluation of Early Visual Recovery in Pituitary Macroadenomas after Endoscopic Endonasal Transphenoidal Surgery: Quantitative Assessment with Diffusion Tensor Imaging (DTI). Acta Neurochir. 2011, 153, 831–842. [Google Scholar] [CrossRef]
- Muskens, I.S.; Zamanipoor Najafabadi, A.H.; Briceno, V.; Lamba, N.; Senders, J.T.; van Furth, W.R.; Verstegen, M.J.T.; Smith, T.R.S.; Mekary, R.A.; Eenhorst, C.A.E.; et al. Visual Outcomes after Endoscopic Endonasal Pituitary Adenoma Resection: A Systematic Review and Meta-Analysis. Pituitary 2017, 20, 539–552. [Google Scholar] [CrossRef] [Green Version]
- Ciric, I.; Ragin, A.; Baumgartner, C.; Pierce, D. Complications of Transsphenoidal Surgery: Results of a National Survey, Review of the Literature, and Personal Experience. Neurosurgery 1997, 40, 225–236, discussion 236–237. [Google Scholar] [CrossRef]
- Chabot, J.D.; Chakraborty, S.; Imbarrato, G.; Dehdashti, A.R. Evaluation of Outcomes After Endoscopic Endonasal Surgery for Large and Giant Pituitary Macroadenoma: A Retrospective Review of 39 Consecutive Patients. World Neurosurg. 2015, 84, 978–988. [Google Scholar] [CrossRef] [PubMed]
- Juraschka, K.; Khan, O.H.; Godoy, B.L.; Monsalves, E.; Kilian, A.; Krischek, B.; Ghare, A.; Vescan, A.; Gentili, F.; Zadeh, G. Endoscopic Endonasal Transsphenoidal Approach to Large and Giant Pituitary Adenomas: Institutional Experience and Predictors of Extent of Resection. J. Neurosurg. 2014, 121, 75–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bokhari, A.R.; Davies, M.A.; Diamond, T. Endoscopic Transsphenoidal Pituitary Surgery: A Single Surgeon Experience and the Learning Curve. Br. J. Neurosurg. 2013, 27, 44–49. [Google Scholar] [CrossRef]
- Chi, F.; Wang, Y.; Lin, Y.; Ge, J.; Qiu, Y.; Guo, L. A Learning Curve of Endoscopic Transsphenoidal Surgery for Pituitary Adenoma. J. Craniofac. Surg. 2013, 24, 2064–2067. [Google Scholar] [CrossRef]
- Leach, P.; Abou-Zeid, A.H.; Kearney, T.; Davis, J.; Trainer, P.J.; Gnanalingham, K.K. Endoscopic Transsphenoidal Pituitary Surgery: Evidence of an Operative Learning Curve. Neurosurgery 2010, 67, 1205–1212. [Google Scholar] [CrossRef] [Green Version]
- Trautmann, J.C.; Laws, E.R. Visual Status after Transsphenoidal Surgery at the Mayo Clinic, 1971–1982. Am. J. Ophthalmol. 1983, 96, 200–208. [Google Scholar] [CrossRef]
- Baijal, V.; Gurunadh, V.S.; Palit, M.G.; Sunder, S.; Thakur, P.K. Pupil Involving Complete III N Palsy in Pituitary Adenoma: Case Report. Med. J. Armed Forces India 1999, 55, 69–70. [Google Scholar] [CrossRef] [Green Version]
- Saul, R.F.; Hilliker, J.K. Third Nerve Palsy: The Presenting Sign of a Pituitary Adenoma in Five Patients and the Only Neurological Sign in Four Patients. J. Clin. Neuroophthalmol. 1985, 5, 185–193. [Google Scholar]
- Lau, K.K.W.; Joshi, S.M.; Ellamushi, H.; Afshar, F. Isolated Bilateral Oculomotor Nerve Palsy in Pituitary Apoplexy: Case Report and Review. Br. J. Neurosurg. 2007, 21, 399–402. [Google Scholar] [CrossRef]
- Robert, C.M.; Feigenbaum, J.A.; Stern, E.W. Ocular Palsy Occurring with Pituitary Tumors. J. Neurosurg. 1973, 38, 17–19. [Google Scholar] [CrossRef] [Green Version]
- Barges-Coll, J.; Fernandez-Miranda, J.C.; Prevedello, D.M.; Gardner, P.; Morera, V.; Madhok, R.; Carrau, R.L.; Snyderman, C.H.; Rhoton, A.L.; Kassam, A.B. Avoiding Injury to the Abducens Nerve during Expanded Endonasal Endoscopic Surgery: Anatomic and Clinical Case Studies. Neurosurgery 2010, 67, 144–154, discussion 154. [Google Scholar] [CrossRef] [PubMed]
- Fatemi, N.; Dusick, J.R.; Gorgulho, A.A.; Mattozo, C.A.; Moftakhar, P.; De Salles, A.A.F.; Kelly, D.F. Endonasal Microscopic Removal of Clival Chordomas. Surg. Neurol. 2008, 69, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Brinar, V.V.; Habek, M.; Ozretić, D.; Djaković, V.; Matijević, V. Isolated Nontraumatic Abducens Nerve Palsy. Acta Neurol. Belg. 2007, 107, 126–130. [Google Scholar] [PubMed]
- Göksu, E.; Akyüz, M.; Gürkanlar, D.; Tuncer, R. Bilateral Abducens Nerve Palsy Following Ruptured Anterior Communicating Artery Aneurysm: Report of 2 Cases. Neurocirugia 2007, 18, 420–422. [Google Scholar] [CrossRef] [Green Version]
- Conti, M.; Prevedello, D.M.; Madhok, R.; Faure, A.; Ricci, U.M.; Schwarz, A.; Robert, R.; Kassam, A.B. The Antero-Medial Triangle: The Risk for Cranial Nerves Ischemia at the Cavernous Sinus Lateral Wall. Anatomic Cadaveric Study. Clin. Neurol. Neurosurg. 2008, 110, 682–686. [Google Scholar] [CrossRef]
- Bejjani, G.K.; Nora, P.C.; Vera, P.L.; Broemling, L.; Sekhar, L.N. The Predictive Value of Intraoperative Somatosensory Evoked Potential Monitoring: Review of 244 Procedures. Neurosurgery 1998, 43, 491–498, discussion 498–500. [Google Scholar] [CrossRef]
- Prass, R.L.; Lüders, H. Acoustic (Loudspeaker) Facial Electromyographic Monitoring: Part 1. Evoked Electromyographic Activity during Acoustic Neuroma Resection. Neurosurgery 1986, 19, 392–400. [Google Scholar] [CrossRef]
- Prass, R.L.; Kinney, S.E.; Hardy, R.W.; Hahn, J.F.; Lüders, H. Acoustic (Loudspeaker) Facial EMG Monitoring: II. Use of Evoked EMG Activity during Acoustic Neuroma Resection. Otolaryngol. Head Neck Surg. 1987, 97, 541–551. [Google Scholar] [CrossRef]
- Thirumala, P.D.; Mohanraj, S.K.; Habeych, M.; Wichman, K.; Chang, Y.-F.; Gardner, P.; Snyderman, C.; Crammond, D.J.; Balzer, J. Value of Free-Run Electromyographic Monitoring of Lower Cranial Nerves in Endoscopic Endonasal Approach to Skull Base Surgeries. J. Neurol. Surg. B Skull Base 2012, 73, 236–244. [Google Scholar] [CrossRef] [Green Version]
- Thirumala, P.; Lai, D.; Engh, J.; Habeych, M.; Crammond, D.; Balzer, J. Predictive Value of Somatosensory Evoked Potential Monitoring during Resection of Intraparenchymal and Intraventricular Tumors Using an Endoscopic Port. J. Clin. Neurol. 2013, 9, 244–251. [Google Scholar] [CrossRef] [Green Version]
- Schlake, H.P.; Goldbrunner, R.; Siebert, M.; Behr, R.; Roosen, K. Intra-Operative Electromyographic Monitoring of Extra-Ocular Motor Nerves (Nn. III, VI) in Skull Base Surgery. Acta Neurochir. 2001, 143, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Nelson, K.R.; Vasconez, H.C. Nerve Transection without Neurotonic Discharges during Intraoperative Electromyographic Monitoring. Muscle Nerve 1995, 18, 236–238. [Google Scholar] [CrossRef] [PubMed]
- Isaacson, B.; Kileny, P.R.; El-Kashlan, H.K. Prediction of Long-Term Facial Nerve Outcomes with Intraoperative Nerve Monitoring. Otol. Neurotol. 2005, 26, 270–273. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Zhang, M.; Jiang, Y. Intraoperative Oculomotor Nerve Monitoring Predicts Outcome Following Clipping of Posterior Communicating Artery Aneurysms. J. Clin. Neurosci. 2012, 19, 706–711. [Google Scholar] [CrossRef]
- Kawaguchi, M.; Ohnishi, H.; Sakamoto, T.; Shimizu, K.; Touho, H.; Monobe, T.; Karasawa, J. Intraoperative Electrophysiologic Monitoring of Cranial Motor Nerves in Skull Base Surgery. Surg. Neurol. 1995, 43, 177–181. [Google Scholar] [CrossRef]
- Acioly, M.A.; Liebsch, M.; de Aguiar, P.H.P.; Tatagiba, M. Facial Nerve Monitoring during Cerebellopontine Angle and Skull Base Tumor Surgery: A Systematic Review from Description to Current Success on Function Prediction. World Neurosurg. 2013, 80, e271–e300. [Google Scholar] [CrossRef]
- Fukuda, M.; Takao, T.; Hiraishi, T.; Yajima, N.; Saito, A.; Fujii, Y. Pharyngeal Motor Evoked Potential Monitoring During Skull Base Surgery Predicts Postoperative Recovery from Swallowing Dysfunction. World Neurosurg. 2015, 84, 555–560. [Google Scholar] [CrossRef]
- Kullmann, M.; Tatagiba, M.; Liebsch, M.; Feigl, G.C. Evaluation of the Predictive Value of Intraoperative Changes in Motor-Evoked Potentials of Caudal Cranial Nerves for the Postoperative Functional Outcome. World Neurosurg. 2016, 95, 329–334. [Google Scholar] [CrossRef]
- Ito, E.; Ichikawa, M.; Itakura, T.; Ando, H.; Matsumoto, Y.; Oda, K.; Sato, T.; Watanabe, T.; Sakuma, J.; Saito, K. Motor Evoked Potential Monitoring of the Vagus Nerve with Transcranial Electrical Stimulation during Skull Base Surgeries. J. Neurosurg. 2013, 118, 195–201. [Google Scholar] [CrossRef] [Green Version]
- Akagami, R.; Dong, C.C.J.; Westerberg, B.D. Localized Transcranial Electrical Motor Evoked Potentials for Monitoring Cranial Nerves in Cranial Base Surgery. Neurosurgery 2005, 57, 78–85, discussion 78–85. [Google Scholar] [CrossRef]
- Acioly, M.A.; Liebsch, M.; Carvalho, C.H.; Gharabaghi, A.; Tatagiba, M. Transcranial Electrocortical Stimulation to Monitor the Facial Nerve Motor Function during Cerebellopontine Angle Surgery. Neurosurgery 2010, 66, 354–361, discussion 362. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, P.M.; DiNapoli, V.; Su, S.Y.; Raza, S.M. Complication Avoidance in Endoscopic Skull Base Surgery. Otolaryngol. Clin. N. Am. 2016, 49, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Nomikos, P.; Ladar, C.; Fahlbusch, R.; Buchfelder, M. Impact of Primary Surgery on Pituitary Function in Patients with Non-Functioning Pituitary Adenomas—A Study on 721 Patients. Acta Neurochir. 2004, 146, 27–35. [Google Scholar] [CrossRef]
- Arafah, B.M. Reversible Hypopituitarism in Patients with Large Nonfunctioning Pituitary Adenomas. J. Clin. Endocrinol. Metab. 1986, 62, 1173–1179. [Google Scholar] [CrossRef]
- Arafah, B.M.; Prunty, D.; Ybarra, J.; Hlavin, M.L.; Selman, W.R. The Dominant Role of Increased Intrasellar Pressure in the Pathogenesis of Hypopituitarism, Hyperprolactinemia, and Headaches in Patients with Pituitary Adenomas. J. Clin. Endocrinol. Metab. 2000, 85, 1789–1793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kristof, R.A.; Rother, M.; Neuloh, G.; Klingmüller, D. Incidence, Clinical Manifestations, and Course of Water and Electrolyte Metabolism Disturbances Following Transsphenoidal Pituitary Adenoma Surgery: A Prospective Observational Study. J. Neurosurg. 2009, 111, 555–562. [Google Scholar] [CrossRef]
- Schreckinger, M.; Walker, B.; Knepper, J.; Hornyak, M.; Hong, D.; Kim, J.-M.; Folbe, A.; Guthikonda, M.; Mittal, S.; Szerlip, N.J. Post-Operative Diabetes Insipidus after Endoscopic Transsphenoidal Surgery. Pituitary 2013, 16, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Berker, M.; Hazer, D.B.; Yücel, T.; Gürlek, A.; Cila, A.; Aldur, M.; Onerci, M. Complications of Endoscopic Surgery of the Pituitary Adenomas: Analysis of 570 Patients and Review of the Literature. Pituitary 2012, 15, 288–300. [Google Scholar] [CrossRef]
- Cote, D.J.; Alzarea, A.; Acosta, M.A.; Hulou, M.M.; Huang, K.T.; Almutairi, H.; Alharbi, A.; Zaidi, H.A.; Algrani, M.; Alatawi, A.; et al. Predictors and Rates of Delayed Symptomatic Hyponatremia after Transsphenoidal Surgery: A Systematic Review [Corrected]. World Neurosurg. 2016, 88, 1–6. [Google Scholar] [CrossRef]
- Jahangiri, A.; Wagner, J.; Han, S.W.; Tran, M.T.; Miller, L.M.; Tom, M.W.; Ostling, L.R.; Kunwar, S.; Blevins, L.; Aghi, M.K. Rate and Time Course of Improvement in Endocrine Function after More than 1000 Pituitary Operations. Neurosurgery 2014, 61 (Suppl. S1), 163–166. [Google Scholar] [CrossRef]
- Staiger, R.D.; Sarnthein, J.; Wiesli, P.; Schmid, C.; Bernays, R.L. Prognostic Factors for Impaired Plasma Sodium Homeostasis after Transsphenoidal Surgery. Br. J. Neurosurg. 2013, 27, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Hussain, N.S.; Piper, M.; Ludlam, W.G.; Ludlam, W.H.; Fuller, C.J.; Mayberg, M.R. Delayed Postoperative Hyponatremia after Transsphenoidal Surgery: Prevalence and Associated Factors. J. Neurosurg. 2013, 119, 1453–1460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gardner, P.A.; Tormenti, M.J.; Pant, H.; Fernandez-Miranda, J.C.; Snyderman, C.H.; Horowitz, M.B. Carotid Artery Injury during Endoscopic Endonasal Skull Base Surgery: Incidence and Outcomes. Neurosurgery 2013, 73, ons261–ons269, discussion ons269–ons270. [Google Scholar] [CrossRef] [PubMed]
- Cavallo, L.M.; Briganti, F.; Cappabianca, P.; Maiuri, F.; Valente, V.; Tortora, F.; Volpe, A.; Messina, A.; Elefante, A.; De Divitiis, E. Hemorrhagic Vascular Complications of Endoscopic Transsphenoidal Surgery. Minim. Invasive Neurosurg. 2004, 47, 145–150. [Google Scholar] [CrossRef]
- Gondim, J.A.; Almeida, J.P.C.; Albuquerque, L.A.F.; Schops, M.; Gomes, E.; Ferraz, T.; Sobreira, W.; Kretzmann, M.T. Endoscopic Endonasal Approach for Pituitary Adenoma: Surgical Complications in 301 Patients. Pituitary 2011, 14, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.-K.; Ma, N.; Sun, X.-C.; Wang, D.-H. Endoscopic Repair of the Injured Internal Carotid Artery Utilizing Oxidized Regenerated Cellulose and a Free Fascia Lata Graft. J. Craniofac. Surg. 2016, 27, 1021–1024. [Google Scholar] [CrossRef]
- Chin, O.Y.; Ghosh, R.; Fang, C.H.; Baredes, S.; Liu, J.K.; Eloy, J.A. Internal Carotid Artery Injury in Endoscopic Endonasal Surgery: A Systematic Review. Laryngoscope 2016, 126, 582–590. [Google Scholar] [CrossRef]
- Rowan, N.R.; Turner, M.T.; Valappil, B.; Fernandez-Miranda, J.C.; Wang, E.W.; Gardner, P.A.; Snyderman, C.H. Injury of the Carotid Artery during Endoscopic Endonasal Surgery: Surveys of Skull Base Surgeons. J. Neurol. Surg. B Skull Base 2018, 79, 302–308. [Google Scholar] [CrossRef]
- AlQahtani, A.; Castelnuovo, P.; Nicolai, P.; Prevedello, D.M.; Locatelli, D.; Carrau, R.L. Injury of the Internal Carotid Artery During Endoscopic Skull Base Surgery: Prevention and Management Protocol. Otolaryngol. Clin. N. Am 2016, 49, 237–252. [Google Scholar] [CrossRef]
- Inamasu, J.; Guiot, B.H. Iatrogenic Carotid Artery Injury in Neurosurgery. Neurosurg. Rev. 2005, 28, 239–247, discussion 248. [Google Scholar] [CrossRef]
- Gardner, P.A.; Snyderman, C.H.; Fernandez-Miranda, J.C.; Jankowitz, B.T. Management of Major Vascular Injury During Endoscopic Endonasal Skull Base Surgery. Otolaryngol. Clin. N. Am. 2016, 49, 819–828. [Google Scholar] [CrossRef] [PubMed]
- Solares, C.A.; Ong, Y.K.; Carrau, R.L.; Fernandez-Miranda, J.; Prevedello, D.M.; Snyderman, C.H.; Kassam, A.B. Prevention and Management of Vascular Injuries in Endoscopic Surgery of the Sinonasal Tract and Skull Base. Otolaryngol. Clin. N. Am. 2010, 43, 817–825. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Carrau, R.L.; Prevedello, D.M.; Yang, B.; Rowan, N.; Han, D.; London, N.R. Intercarotid Artery Distance in the Pediatric Population: Implications for Endoscopic Transsphenoidal Approaches to the Skull Base. Int. J. Pediatr. Otorhinolaryngol. 2021, 140, 110520. [Google Scholar] [CrossRef] [PubMed]
- Weidenbecher, M.; Huk, W.J.; Iro, H. Internal Carotid Artery Injury during Functional Endoscopic Sinus Surgery and Its Management. Eur. Arch. Otorhinolaryngol. 2005, 262, 640–645. [Google Scholar] [CrossRef]
- Fujii, K.; Chambers, S.M.; Rhoton, A.L. Neurovascular Relationships of the Sphenoid Sinus. A Microsurgical Study. J. Neurosurg. 1979, 50, 31–39. [Google Scholar] [CrossRef]
- Fernandez-Miranda, J.C.; Prevedello, D.M.; Madhok, R.; Morera, V.; Barges-Coll, J.; Reineman, K.; Snyderman, C.H.; Gardner, P.; Carrau, R.; Kassam, A.B. Sphenoid Septations and Their Relationship with Internal Carotid Arteries: Anatomical and Radiological Study. Laryngoscope 2009, 119, 1893–1896. [Google Scholar] [CrossRef]
- Sylvester, P.T.; Moran, C.J.; Derdeyn, C.P.; Cross, D.T.; Dacey, R.G.; Zipfel, G.J.; Kim, A.H.; Uppaluri, R.; Haughey, B.H.; Tempelhoff, R.; et al. Endovascular Management of Internal Carotid Artery Injuries Secondary to Endonasal Surgery: Case Series and Review of the Literature. J. Neurosurg. 2016, 125, 1256–1276. [Google Scholar] [CrossRef] [Green Version]
- Mathis, J.M.; Barr, J.D.; Jungreis, C.A.; Yonas, H.; Sekhar, L.N.; Vincent, D.; Pentheny, S.L.; Horton, J.A. Temporary Balloon Test Occlusion of the Internal Carotid Artery: Experience in 500 Cases. AJNR Am. J. Neuroradiol. 1995, 16, 749–754. [Google Scholar]
- Zada, G.; Cavallo, L.M.; Esposito, F.; Fernandez-Jimenez, J.C.; Tasiou, A.; De Angelis, M.; Cafiero, T.; Cappabianca, P.; Laws, E.R. Transsphenoidal Surgery in Patients with Acromegaly: Operative Strategies for Overcoming Technically Challenging Anatomical Variations. Neurosurg. Focus 2010, 29, E8. [Google Scholar] [CrossRef] [Green Version]
- Padhye, V.; Valentine, R.; Wormald, P.-J. Management of Carotid Artery Injury in Endonasal Surgery. Int. Arch. Otorhinolaryngol. 2014, 18, S173–S178. [Google Scholar] [CrossRef] [Green Version]
- Dolati, P.; Eichberg, D.; Golby, A.; Zamani, A.; Laws, E. Multimodal Navigation in Endoscopic Transsphenoidal Resection of Pituitary Tumors Using Image-Based Vascular and Cranial Nerve Segmentation: A Prospective Validation Study. World Neurosurg. 2016, 95, 406–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dusick, J.R.; Esposito, F.; Malkasian, D.; Kelly, D.F. Avoidance of Carotid Artery Injuries in Transsphenoidal Surgery with the Doppler Probe and Micro-Hook Blades. Neurosurgery 2007, 60, 322–328, discussion 328–329. [Google Scholar] [CrossRef] [PubMed]
- Iacoangeli, M.; Di Rienzo, A.; Re, M.; Alvaro, L.; Nocchi, N.; Gladi, M.; De Nicola, M.; Scerrati, M. Endoscopic Endonasal Approach for the Treatment of a Large Clival Giant Cell Tumor Complicated by an Intraoperative Internal Carotid Artery Rupture. Cancer Manag. Res. 2013, 5, 21–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romero, A.D.C.B.; Lal Gangadharan, J.; Bander, E.D.; Gobin, Y.P.; Anand, V.K.; Schwartz, T.H. Managing Arterial Injury in Endoscopic Skull Base Surgery: Case Series and Review of the Literature. Oper. Neurosurg. 2017, 13, 138–149. [Google Scholar] [CrossRef]
- Ramakrishnan, V.R.; Feazel, L.M.; Gitomer, S.A.; Ir, D.; Robertson, C.E.; Frank, D.N. The Microbiome of the Middle Meatus in Healthy Adults. PLoS ONE 2013, 8, e85507. [Google Scholar] [CrossRef]
- Rosen, S.A.B.; Getz, A.E.; Kingdom, T.; Youssef, A.S.; Ramakrishnan, V.R. Systematic Review of the Effectiveness of Perioperative Prophylactic Antibiotics for Skull Base Surgeries. Am. J. Rhinol. Allergy 2016, 30, e10–e16. [Google Scholar] [CrossRef]
- Orlando, R.; Cappabianca, P.; Tosone, G.; Esposito, F.; Piazza, M.; de Divitiis, E. Retrospective Analysis of a New Antibiotic Chemoprophylaxis Regimen in 170 Patients Undergoing Endoscopic Endonasal Transsphenoidal Surgery. Surg. Neurol. 2007, 68, 145–148, discussion 148. [Google Scholar] [CrossRef]
- Brown, S.M.; Anand, V.K.; Tabaee, A.; Schwartz, T.H. Role of Perioperative Antibiotics in Endoscopic Skull Base Surgery. Laryngoscope 2007, 117, 1528–1532. [Google Scholar] [CrossRef]
- Somma, T.; Maraolo, A.E.; Esposito, F.; Cavallo, L.M.; Tosone, G.; Orlando, R.; Cappabianca, P. Efficacy of Ultra-Short Single Agent Regimen Antibiotic Chemo-Prophylaxis in Reducing the Risk of Meningitis in Patients Undergoing Endoscopic Endonasal Transsphenoidal Surgery. Clin. Neurol. Neurosurg. 2015, 139, 206–209. [Google Scholar] [CrossRef]
- Milanese, L.; Zoli, M.; Sollini, G.; Martone, C.; Zenesini, C.; Sturiale, C.; Farneti, P.; Frank, G.; Pasquini, E.; Mazzatenta, D. Antibiotic Prophylaxis in Endoscopic Endonasal Pituitary and Skull Base Surgery. World Neurosurg. 2017, 106, 912–918. [Google Scholar] [CrossRef]
- Little, A.S.; Kshettry, V.R.; Rosen, M.R.; Rehl, R.M.; Haegen, T.W.; Rabinowitz, M.R.; Nyquist, G.G.; Recinos, P.F.; Sindwani, R.; Woodard, T.D.; et al. Postoperative Oral Antibiotics and Sinonasal Outcomes Following Endoscopic Transsphenoidal Surgery for Pituitary Tumors Study: A Multicenter, Prospective, Randomized, Double-Blinded, Placebo-Controlled Study. Neurosurgery 2021, 89, 769–776. [Google Scholar] [CrossRef] [PubMed]
- Spinazzi, E.F.; Pines, M.J.; Fang, C.H.; Raikundalia, M.D.; Baredes, S.; Liu, J.K.; Eloy, J.A. Impact and Cost of Care of Venous Thromboembolism Following Pituitary Surgery. Laryngoscope 2015, 125, 1563–1567. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Kim, Y.H.; Phi, J.H.; Kim, S.-K.; Wang, K.-C. Complications of Endoscopic Skull Base Surgery for Sellar and Parasellar Tumors in Pediatric Population; Neurosurgical Perspectives. Front. Oncol. 2022, 12, 769576. [Google Scholar] [CrossRef] [PubMed]
- Shields, C.B.; Valdes-Rodriguez, A.G. Tension Pneumocephalus after Trans-Sphenoidal Hypophysectomy: Case Report. Neurosurgery 1982, 11, 687–689. [Google Scholar] [CrossRef] [PubMed]
- Solomiichuk, V.O.; Lebed, V.O.; Drizhdov, K.I. Posttraumatic Delayed Subdural Tension Pneumocephalus. Surg. Neurol. Int. 2013, 4, 37. [Google Scholar] [CrossRef] [PubMed]
- Laws, E.R.; Wong, J.M.; Smith, T.R.; de Los Reyes, K.; Aglio, L.S.; Thorne, A.J.; Cote, D.J.; Esposito, F.; Cappabianca, P.; Gawande, A. A Checklist for Endonasal Transsphenoidal Anterior Skull Base Surgery. J. Neurosurg. 2016, 124, 1634–1639. [Google Scholar] [CrossRef] [Green Version]
- Rowan, N.R.; Mukherjee, D. Quality of Life Outcomes and Approach-Specific Morbidities in Endoscopic Endonasal Skull Base Surgery. Curr. Otorhinolaryngol. Rep. 2020, 8, 160–169. [Google Scholar] [CrossRef]
- Pant, H.; Bhatki, A.; Snyderman, C.; Vescan, A.; Carrau, R.; Gardner, P.; Prevedello, D.; Kassam, A. Quality of Life Following Endonasal Skull Base Surgery. Skull Base 2010, 20, 035–040. [Google Scholar] [CrossRef]
- de Almeida, J.R.; Vescan, A.D. Outcomes and Quality of Life Following Skull Base Surgery. Curr. Otorhinolaryngol. Rep. 2013, 1, 214–220. [Google Scholar] [CrossRef] [Green Version]
- de Almeida, J.R.; Snyderman, C.H.; Gardner, P.A.; Carrau, R.L.; Vescan, A.D. Nasal Morbidity Following Endoscopic Skull Base Surgery: A Prospective Cohort Study. Head Neck 2011, 33, 547–551. [Google Scholar] [CrossRef]
- de Almeida, J.R.; Witterick, I.J.; Vescan, A.D. Functional Outcomes for Endoscopic and Open Skull Base Surgery: An Evidence-Based Review. Otolaryngol. Clin. N. Am. 2011, 44, 1185–1200. [Google Scholar] [CrossRef] [PubMed]
- Bhenswala, P.N.; Schlosser, R.J.; Nguyen, S.A.; Munawar, S.; Rowan, N.R. Sinonasal Quality-of-Life Outcomes after Endoscopic Endonasal Skull Base Surgery. Int. Forum Allergy Rhinol. 2019, 9, 1105–1118. [Google Scholar] [CrossRef] [PubMed]
- Suberman, T.A.; Zanation, A.M.; Ewend, M.G.; Senior, B.A.; Ebert, C.S. Sinonasal Quality-of-Life before and after Endoscopic, Endonasal, Minimally Invasive Pituitary Surgery. Int. Forum Allergy Rhinol. 2011, 1, 161–166. [Google Scholar] [CrossRef] [PubMed]
- McCoul, E.D.; Bedrosian, J.C.; Akselrod, O.; Anand, V.K.; Schwartz, T.H. Preservation of Multidimensional Quality of Life after Endoscopic Pituitary Adenoma Resection. J. Neurosurg. 2015, 123, 813–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Little, A.S.; Kelly, D.; Milligan, J.; Griffiths, C.; Prevedello, D.M.; Carrau, R.L.; Rosseau, G.; Barkhoudarian, G.; Otto, B.A.; Jahnke, H.; et al. Predictors of Sinonasal Quality of Life and Nasal Morbidity after Fully Endoscopic Transsphenoidal Surgery. J. Neurosurg. 2015, 122, 1458–1465. [Google Scholar] [CrossRef] [Green Version]
- Lavigne, P.; Faden, D.L.; Wang, E.W.; Snyderman, C.H. Complications of Nasoseptal Flap Reconstruction: A Systematic Review. J. Neurol. Surg. B Skull Base 2018, 79, S291–S299. [Google Scholar] [CrossRef] [Green Version]
- Kimple, A.J.; Leight, W.D.; Wheless, S.A.; Zanation, A.M. Reducing Nasal Morbidity after Skull Base Reconstruction with the Nasoseptal Flap: Free Middle Turbinate Mucosal Grafts. Laryngoscope 2012, 122, 1920–1924. [Google Scholar] [CrossRef]
- Pinheiro-Neto, C.; Rowan, N.R.; Celda, M.P.; Mukherjee, D.; Gompel, J.J.V.; Choby, G. Optimizing Quality of Life and Minimizing Morbidity through Nasal Preservation in Endoscopic Skull Base Surgery: A Contemporary Review. J. Neurol. Surg. B Skull Base 2022, 83, s-0042-1749654. [Google Scholar] [CrossRef]
- Velasquez, N.; Ahmed, O.H.; Lavigne, P.; Goldschmidt, E.; Gardner, P.A.; Snyderman, C.H.; Wang, E.W. Utility of Nasal Access Guides in Endoscopic Endonasal Skull Base Surgery: Assessment of Use during Cadaveric Dissection and Workflow Analysis in Surgery. J. Neurol. Surg. B Skull Base 2021, 82, 540–546. [Google Scholar] [CrossRef]
- Gompel, J.J.V.; Janus, J.R.; Hughes, J.D.; Stokken, J.K.; Moore, E.J.; Ryan, T.; Price, D.L.; Link, M.J. Esthesioneuroblastoma and Olfactory Preservation: Is It Reasonable to Attempt Smell Preservation? J. Neurol. Surg. B Skull Base 2018, 79, 184–188. [Google Scholar] [CrossRef]
- Lu, V.M.; Goyal, A.; Rovin, R.A. Olfactory Groove and Tuberculum Sellae Meningioma Resection by Endoscopic Endonasal Approach versus Transcranial Approach: A Systematic Review and Meta-Analysis of Comparative Studies. Clin. Neurol. Neurosurg. 2018, 174, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Yin, L.X.; Low, C.M.; Puccinelli, C.L.; O’Brien, E.K.; Stokken, J.K.; Van Abel, K.M.; Janus, J.R.; Link, M.J.; Van Gompel, J.J.; Choby, G. Olfactory Outcomes after Endoscopic Skull Base Surgery: A Systematic Review and Meta-Analysis. Laryngoscope 2019, 129, 1998–2007. [Google Scholar] [CrossRef] [PubMed]
- Purohit, A.; Jha, R.; Khalafallah, A.M.; Price, C.; Rowan, N.R.; Mukherjee, D. Endoscopic Endonasal versus Transcranial Approach to Resection of Olfactory Groove Meningiomas: A Systematic Review. Neurosurg. Rev. 2020, 43, 1465–1471. [Google Scholar] [CrossRef] [PubMed]
- Puccinelli, C.L.; Yin, L.X.; O’Brien, E.K.; Van Gompel, J.J.; Choby, G.W.; Van Abel, K.M.; Janus, J.R.; Stokken, J.K. Long-Term Olfaction Outcomes in Transnasal Endoscopic Skull-Base Surgery: A Prospective Cohort Study Comparing Electrocautery and Cold Knife Upper Septal Limb Incision Techniques. Int. Forum Allergy Rhinol. 2019, 9, 493–500. [Google Scholar] [CrossRef]
- Jalessi, M.; Jahanbakhshi, A.; Amini, E.; Kamrava, S.K.; Farhadi, M. Impact of Nasoseptal Flap Elevation on Sinonasal Quality of Life in Endoscopic Endonasal Approach to Pituitary Adenomas. Eur. Arch. Otorhinolaryngol. 2016, 273, 1199–1205. [Google Scholar] [CrossRef]
- Tajudeen, B.A.; Adappa, N.D.; Kuan, E.C.; Schwartz, J.S.; Suh, J.D.; Wang, M.B.; Palmer, J.N. Smell Preservation Following Endoscopic Unilateral Resection of Esthesioneuroblastoma: A Multi-Institutional Experience. Int. Forum Allergy Rhinol. 2016, 6, 1047–1050. [Google Scholar] [CrossRef]
- Chislett, S.P.; Limjuco, A.P.; Solyar, A.Y.; Lanza, D.C. Cranial Nerve V2 and Vidian Nerve Trauma Secondary to Lateral Pterygoid Recess Encephalocele Repair. Int. Forum Allergy Rhinol. 2020, 10, 81–88. [Google Scholar] [CrossRef]
- Choi, J.-E.; Noh, Y.-S.; Lee, K.E.; Jung, Y.G.; Chung, S.-K.; Kim, H.Y.; Kong, D.-S.; Nam, D.-H.; Hong, S.D. Morbidities Associated with the Endoscopic Transnasal Transpterygoid Approach: Focusing on Postoperative Sequelae. World Neurosurg. 2020, 137, e43–e51. [Google Scholar] [CrossRef]
- Geltzeiler, M.; Turner, M.; Rimmer, R.; Zenonos, G.; Hebert, A.; Snyderman, C.; Gardner, P.; Fernandez-Miranda, J.; Wang, E.W. Endoscopic Nasopharyngectomy Combined with a Nerve-Sparing Transpterygoid Approach. Laryngoscope 2020, 130, 2343–2348. [Google Scholar] [CrossRef]
- Alves-Belo, J.T.; Mangussi-Gomes, J.; Truong, H.Q.; Cohen, S.; Gardner, P.A.; Snyderman, C.H.; Stefko, S.T.; Wang, E.W.; Fernandez-Miranda, J.C. Lateral Transorbital Versus Endonasal Transpterygoid Approach to the Lateral Recess of the Sphenoid Sinus-A Comparative Anatomic Study. Oper. Neurosurg. 2019, 16, 600–606. [Google Scholar] [CrossRef]
- Rowan, N.R.; Valappil, B.; Chen, J.; Wang, E.W.; Gardner, P.A.; Snyderman, C.H. Prospective Characterization of Postoperative Nasal Deformities in Patients Undergoing Endoscopic Endonasal Skull-Base Surgery. Int. Forum Allergy Rhinol. 2020, 10, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Rowan, N.R.; Wang, E.W.; Gardner, P.A.; Fernandez-Miranda, J.C.; Snyderman, C.H. Nasal Deformities Following Nasoseptal Flap Reconstruction of Skull Base Defects. J. Neurol. Surg. B Skull Base 2016, 77, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Chin, D.; Harvey, R.J. Endoscopic Reconstruction of Frontal, Cribiform and Ethmoid Skull Base Defects. Adv. Otorhinolaryngol. 2013, 74, 104–118. [Google Scholar] [CrossRef] [PubMed]
- Nayak, J.V.; Rathor, A.; Grayson, J.W.; Bravo, D.T.; Velasquez, N.; Noel, J.; Beswick, D.M.; Riley, K.O.; Patel, Z.M.; Cho, D.-Y.; et al. Porcine Small Intestine Submucosal Grafts Improve Remucosalization and Progenitor Cell Recruitment to Sites of Upper Airway Tissue Remodeling. Int. Forum Allergy Rhinol. 2018, 8, 1162–1168. [Google Scholar] [CrossRef]
- Caicedo-Granados, E.; Carrau, R.; Snyderman, C.H.; Prevedello, D.; Fernandez-Miranda, J.; Gardner, P.; Kassam, A. Reverse Rotation Flap for Reconstruction of Donor Site after Vascular Pedicled Nasoseptal Flap in Skull Base Surgery. Laryngoscope 2010, 120, 1550–1552. [Google Scholar] [CrossRef]
- Lepänluoma, M.; Takala, R.; Kotkansalo, A.; Rahi, M.; Ikonen, T.S. Surgical Safety Checklist Is Associated with Improved Operating Room Safety Culture, Reduced Wound Complications, and Unplanned Readmissions in a Pilot Study in Neurosurgery. Scand J. Surg. 2014, 103, 66–72. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Pinheiro-Neto, C.D.; Yang, D.; Wang, E.; Gardner, P.A.; Hirsch, B.E.; Snyderman, C.H.; Fernandez-Miranda, J.C. Comparison of Endoscopic Endonasal Approach and Lateral Microsurgical Infratemporal Fossa Approach to the Jugular Foramen: An Anatomical Study. J. Neurol. Surg. B Skull Base 2022, 83, e474–e483. [Google Scholar] [CrossRef]
- Muskens, I.S.; Briceno, V.; Ouwehand, T.L.; Castlen, J.P.; Gormley, W.B.; Aglio, L.S.; Zamanipoor Najafabadi, A.H.; van Furth, W.R.; Smith, T.R.; Mekary, R.A.; et al. The Endoscopic Endonasal Approach Is Not Superior to the Microscopic Transcranial Approach for Anterior Skull Base Meningiomas—A Meta-Analysis. Acta Neurochir. 2018, 160, 59–75. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Liu, H.; Man, S.; Liu, G.; Li, Q.; Zuo, Q.; Huo, L.; Li, W.; Deng, W. Endoscopic vs. Microscopic Transsphenoidal Surgery for the Treatment of Pituitary Adenoma: A Meta-Analysis. Front. Surg. 2021, 8, 806855. [Google Scholar] [CrossRef]
- Ishikawa, M.; Ota, Y.; Naritaka, H.; Katoh, S. Endoscopic Ultrasound Imaging with High Flow Mode for Endonasal Transsphenoidal Pituitary Surgery. J. Clin. Neurosci. 2021, 89, 329–335. [Google Scholar] [CrossRef]
- Trévillot, V.; Garrel, R.; Dombre, E.; Poignet, P.; Sobral, R.; Crampette, L. Robotic Endoscopic Sinus and Skull Base Surgery: Review of the Literature and Future Prospects. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2013, 130, 201–207. [Google Scholar] [CrossRef] [Green Version]
- Ogiwara, T.; Hori, T.; Fujii, Y.; Nakamura, T.; Suzuki, Y.; Watanabe, G.; Hanaoka, Y.; Goto, T.; Hongo, K.; Horiuchi, T. Effectiveness of the Intraoperative Magnetic Resonance Imaging during Endoscopic Endonasal Approach for Acromegaly. Pituitary 2021, 24, 690–697. [Google Scholar] [CrossRef] [PubMed]
- Singh, H.; Rote, S.; Jada, A.; Bander, E.D.; Almodovar-Mercado, G.J.; Essayed, W.I.; Härtl, R.; Anand, V.K.; Schwartz, T.H.; Greenfield, J.P. Endoscopic Endonasal Odontoid Resection with Real-Time Intraoperative Image-Guided Computed Tomography: Report of 4 Cases. J. Neurosurg. 2018, 128, 1486–1491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, M.; Skyrman, S.; Shan, C.; Babic, D.; Homan, R.; Edström, E.; Persson, O.; Burström, G.; Elmi-Terander, A.; Hendriks, B.H.W.; et al. Fusion of Augmented Reality Imaging with the Endoscopic View for Endonasal Skull Base Surgery; a Novel Application for Surgical Navigation Based on Intraoperative Cone Beam Computed Tomography and Optical Tracking. PLoS ONE 2020, 15, e0227312. [Google Scholar] [CrossRef] [Green Version]
- Jean, W.C.; Singh, A. Expanded Endoscopic Endonasal Transtuberculum Approach for Tuberculum Sellae Meningioma: Operative Video with 360-Degree Fly-Through and Surgical Rehearsal in Virtual Reality: 2-Dimensional Operative Video. Oper. Neurosurg. 2020, 19, E179–E180. [Google Scholar] [CrossRef]
- Kahilogullari, G.; Bahadır, B.; Bozkurt, M.; Akcalar, S.; Balci, S.; Arat, A. Carotid Artery-Cavernous Segment Injury during an Endoscopic Endonasal Surgery: A Case Report and Literature Review of the Overlooked Option for Surgical Trapping in the Hyperacute Phase. J. Neurol. Surg. Rep. 2021, 82, e53–e62. [Google Scholar] [CrossRef]
- Meyer, J.; Perry, A.; Graffeo, C.S.; Carlstrom, L.P.; Marcellino, C.R.; Burrows, A.; Bancos, I.; Driscoll, C.; Meyer, F.B. Carotid Artery Injury during Transsphenoidal Pituitary Surgery: Lessons from a 15-Year Modern Microsurgery Cohort. J. Neurol. Surg. B Skull Base 2020, 81, 594–602. [Google Scholar] [CrossRef]
- Cathelinaud, O.; Bizeau, A.; Rimbot, A.; Arteaga, C.; Verdalle, P. Endoscopic endonasal surgery complication: New methods of intracavernous internal carotid artery injury treatment. Rev. Laryngol. Otol. Rhinol. 2008, 129, 305–308. [Google Scholar]
- Beer-Furlan, A.; Balsalobre, L.; de Vellutini, E.A.S.; Stamm, A.C.; Pahl, F.H.; Gentil, A.F. Endoscopic Endonasal Management of Cerebrospinal Fluid Rhinorrhea after Anterior Clinoidectomy for Aneurysm Surgery: Changing the Paradigm of Complication Management. Arq. Neuropsiquiatr. 2016, 74, 580–586. [Google Scholar] [CrossRef] [Green Version]
- Carrau, R.L.; Snyderman, C.H.; Kassam, A.B. The Management of Cerebrospinal Fluid Leaks in Patients at Risk for High-Pressure Hydrocephalus. Laryngoscope 2005, 115, 205–212. [Google Scholar] [CrossRef] [Green Version]
- Kono, Y.; Prevedello, D.M.; Snyderman, C.H.; Gardner, P.A.; Kassam, A.B.; Carrau, R.L.; Byers, K.E. One Thousand Endoscopic Skull Base Surgical Procedures Demystifying the Infection Potential: Incidence and Description of Postoperative Meningitis and Brain Abscesses. Infect. Control Hosp. Epidemiol. 2011, 32, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Koutourousiou, M.; Gardner, P.A.; Fernandez-Miranda, J.C.; Tyler-Kabara, E.C.; Wang, E.W.; Snyderman, C.H. Endoscopic Endonasal Surgery for Craniopharyngiomas: Surgical Outcome in 64 Patients. J. Neurosurg. 2013, 119, 1194–1207. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Porras, J.L.; Rowan, N.R.; Mukherjee, D. Endoscopic Endonasal Skull Base Surgery Complication Avoidance: A Contemporary Review. Brain Sci. 2022, 12, 1685. https://doi.org/10.3390/brainsci12121685
Porras JL, Rowan NR, Mukherjee D. Endoscopic Endonasal Skull Base Surgery Complication Avoidance: A Contemporary Review. Brain Sciences. 2022; 12(12):1685. https://doi.org/10.3390/brainsci12121685
Chicago/Turabian StylePorras, Jose L., Nicholas R. Rowan, and Debraj Mukherjee. 2022. "Endoscopic Endonasal Skull Base Surgery Complication Avoidance: A Contemporary Review" Brain Sciences 12, no. 12: 1685. https://doi.org/10.3390/brainsci12121685