
Food-Induced Brain Activity in Children with Overweight or Obesity versus Normal Weight: An Electroencephalographic Pilot Study
 , and
, and
Abstract
:1. Introduction
Aims and Hypotheses
2. Materials and Methods
2.1. Participants and Study Design
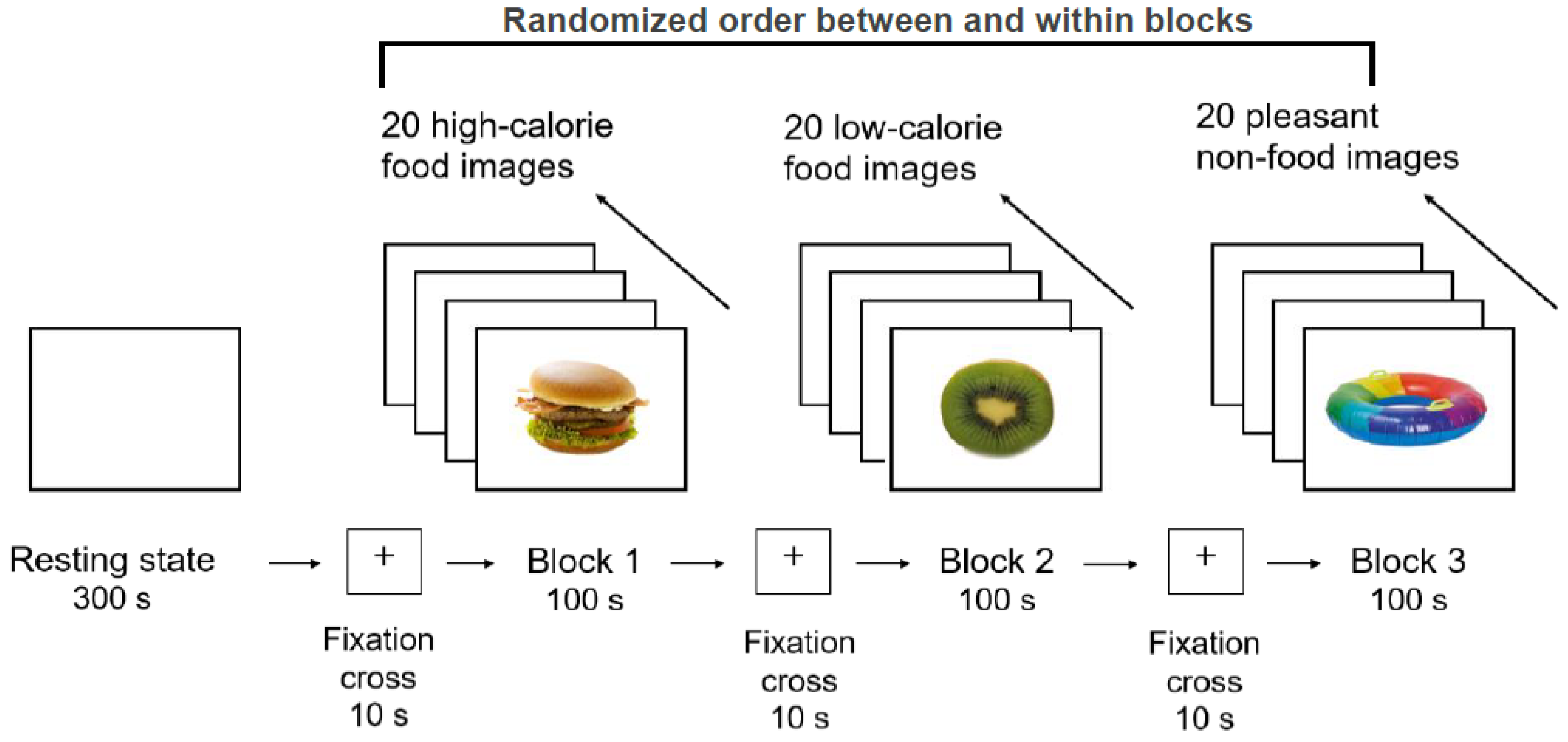
2.2. Procedure
2.3. EEG Recordings
2.4. EEG Stimuli
2.5. Pre-Processing and Analysis of EEG Recordings
2.6. Control Variables
2.7. Data Analysis
3. Results
3.1. Preliminary Analyses
3.2. EEG Activity
3.2.1. Theta
3.2.2. Alpha
3.2.3. Beta
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kromeyer-Hauschild, K.; Wabitsch, M.; Kunze, D.; Geller, F.; Geiss, H.C.; Hesse, V.; von Hippel, A.; Jaeger, U.; Johnsen, D.; Korte, W.D.; et al. Perzentile für den Body-mass-Index für das Kindes- und Jugendalter unter Heranziehung verschiedener deutscher Stichproben [Percentiles for the body mass index for childhood and adolescence using various German samples]. Monatsschr. Kinderheilkd. 2001, 149, 807–818. [Google Scholar] [CrossRef] [Green Version]
- Garrido-Miguel, M.; Cavero-Redondo, I.; Álvarez-Bueno, C.; Rodríguez-Artalejo, F.; Moreno, L.A.; Ruiz, J.R.; Ahrens, W.; Martínez-Vizcaíno, V. Prevalence and trends of overweight and obesity in European children From 1999 to 2016: A systematic review and meta-analysis. JAMA Pediatr. 2019, 173, e192430. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization: Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 12 November 2022).
- Simmonds, M.; Llewellyn, A.; Owen, C.G.; Woolacott, N. Predicting adult obesity from childhood obesity: A systematic review and meta-analysis. Obes Rev. 2016, 17, 95–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flegal, K.M.; Kit, B.K.; Orpana, H.; Graubard, B.I. Association of all-cause mortality with overweight and obesity using standard body mass index categories: A systematic review and meta-analysis. JAMA 2013, 309, 71–82. [Google Scholar] [CrossRef] [Green Version]
- Morales Camacho, W.J.; Molina Díaz, J.M.; Plata Ortiz, S.; Plata Ortiz, J.E.; Morales Camacho, M.A.; Calderón, B.P. Childhood obesity: Aetiology, comorbidities, and treatment. Diabetes Metab. Res. Rev. 2019, 35, e3203. [Google Scholar] [CrossRef] [PubMed]
- Halfon, N.; Larson, K.; Slusser, W. Associations between obesity and comorbid mental health, developmental, and physical health conditions in a nationally representative sample of US children aged 10 to 17. Acad. Pediatr. 2013, 13, 6–13. [Google Scholar] [CrossRef]
- Association of the Scientific Medical Societies: S3-Guideline for the Treatment and Prevention of Obesity in Children and Adolescents. Available online: https://register.awmf.org/assets/guidelines/050-002l_S3_Therapie-Praevention-Adipositas-Kinder-Jugendliche_2019-11.pdf (accessed on 12 November 2022).
- Kobes, A.; Kretschmer, T.; Timmerman, G.; Schreuder, P. Interventions aimed at preventing and reducing overweight/obesity among children and adolescents: A meta-synthesis. Obes. Rev. 2018, 19, 1065–1079. [Google Scholar] [CrossRef] [Green Version]
- Boswell, R.G.; Kober, H. Food cue reactivity and craving predict eating and weight gain: A meta-analytic review. Obes. Rev. 2016, 17, 159–177. [Google Scholar] [CrossRef]
- Jansen, A.; Theunissen, N.; Slechten, K.; Nederkoorn, C.; Boon, B.; Mulkens, S.; Roefs, A. Overweight children overeat after exposure to food cues. Eat Behav. 2003, 4, 197–209. [Google Scholar] [CrossRef]
- Jiang, Q.; He, D.; Guan, W.; He, X. “Happy goat says”: The effect of a food selection inhibitory control training game of children’s response inhibition on eating behavior. Appetite 2016, 107, 86–92. [Google Scholar] [CrossRef]
- Buijzen, M.; Schuurman, J.; Bomhof, E. Associations between children’s television advertising exposure and their food consumption patterns: A household diary-survey study. Appetite 2008, 50, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Folkvord, F.; Anschutz, D.J.; Nederkoorn, C.; Westerik, H.; Buijzen, M. Impulsivity, “advergames,” and food intake. Pediatrics 2014, 133, 1007–1012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, J.L.; Speers, S.E.; Schwartz, M.B.; Brownell, K.D. US Food Company Branded Advergames on the Internet: Children’s exposure and effects on snack consumption. J. Child Media 2012, 6, 51–68. [Google Scholar] [CrossRef] [Green Version]
- Bruce, A.S.; Holsen, L.M.; Chambers, R.J.; Martin, L.E.; Brooks, W.M.; Zarcone, J.R.; Butler, M.G.; Savage, C.R. Obese children show hyperactivation to food pictures in brain networks linked to motivation, reward and cognitive control. Int. J. Obes. 2010, 34, 1494–1500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gearhardt, A.N.; Yokum, S.; Stice, E.; Harris, J.L.; Brownell, K.D. Relation of obesity to neural activation in response to food commercials. Soc. Cogn. Affect. Neurosci. 2014, 9, 932–938. [Google Scholar] [CrossRef]
- Holsen, L.M.; Zarcone, J.R.; Thompson, T.I.; Brooks, W.M.; Anderson, M.F.; Ahluwalia, J.S.; Nollen, N.L.; Savage, C.R. Neural mechanisms underlying food motivation in children and adolescents. Neuroimage 2005, 27, 669–676. [Google Scholar] [CrossRef] [Green Version]
- Luo, S.; Alves, J.; Hardy, K.; Wang, X.; Monterosso, J.; Xiang, A.H.; Page, K.A. Neural processing of food cues in pre-pubertal children. Pediatr. Obes. 2019, 14, e12435. [Google Scholar] [CrossRef]
- Yokum, S.; Gearhardt, A.N.; Harris, J.L.; Brownell, K.D.; Stice, E. Individual differences in striatum activity to food commercials predict weight gain in adolescents. Obesity 2014, 22, 2544–2551. [Google Scholar] [CrossRef] [Green Version]
- Samara, A.; Li, X.; Pivik, R.T.; Badger, T.M.; Ou, X. Brain activation to high-calorie food images in healthy normal weight and obese children: A fMRI study. BMC Obes. 2018, 5, 31. [Google Scholar] [CrossRef] [Green Version]
- van Meer, F.; van der Laan, L.N.; Charbonnier, L.; Viergever, M.A.; Adan, R.A.; Smeets, P.A.; I. Family Consortium. Developmental differences in the brain response to unhealthy food cues: An fMRI study of children and adults. Am. J. Clin. Nutr. 2016, 104, 1515–1522. [Google Scholar] [CrossRef]
- van Meer, F.; van der Laan, L.N.; Eiben, G.; Lissner, L.; Wolters, M.; Rach, S.; Herrmann, M.; Erhard, P.; Molnar, D.; Orsi, G.; et al. Development and body mass inversely affect children’s brain activation in dorsolateral prefrontal cortex during food choice. Neuroimage 2019, 201, 116016. [Google Scholar] [CrossRef] [PubMed]
- Davids, S.; Lauffer, H.; Thoms, K.; Jagdhuhn, M.; Hirschfeld, H.; Domin, M.; Hamm, A.; Lotze, M. Increased dorsolateral prefrontal cortex activation in obese children during observation of food stimuli. Int. J. Obes. 2010, 34, 94–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newson, J.J.; Thiagarajan, T.C. EEG frequency bands in psychiatric disorders: A review of resting state studies. Front. Hum. Neurosci. 2019, 12, 521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babiloni, C.; Marzano, N.; Lizio, R.; Valenzano, A.; Triggiani, A.I.; Petito, A.; Bellomo, A.; Lecce, B.; Mundi, C.; Soricelli, A.; et al. Resting state cortical electroencephalographic rhythms in subjects with normal and abnormal body weight. Neuroimage 2011, 58, 698–707. [Google Scholar] [CrossRef] [PubMed]
- Del Percio, C.; Triggiani, A.I.; Marzano, N.; Valenzano, A.; De Rosas, M.; Petito, A.; Bellomo, A.; Lecce, B.; Mundi, C.; Infarinato, F.; et al. Poor desynchronisation of resting-state eyes-open cortical alpha rhythms in obese subjects without eating disorders. Clin. Neurophysiol. 2013, 124, 1095–1105. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, R.; Sebert, C.; Kösling, C.; Grunwald, M.; Hilbert, A.; Hübner, C.; Schäfer, L. Neuropsychological and neurophysiological indicators of general and food-specific impulsivity in children with overweight and obesity: A pilot study. Nutrients 2018, 10, 1983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tammela, L.I.; Pääkkönen, A.; Karhunen, L.J.; Karhu, J.; Uusitupa, M.I.; Kuikka, J.T. Brain electrical activity during food presentation in obese binge-eating women. Clin. Physiol. Funct. Imaging 2010, 30, 135–140. [Google Scholar] [CrossRef]
- Bauer, L.O.; Manning, K.J. Challenges in the Detection of Working Memory and Attention Decrements among Overweight Adolescent Girls. Neuropsychobiology 2016, 73, 43–51. [Google Scholar] [CrossRef] [Green Version]
- Hume, D.J.; Howells, F.M.; Karpul, D.; Rauch, H.G.; Kroff, J.; Lambert, E.V. Cognitive control over visual food cue saliency is greater in reduced-overweight/obese but not in weight relapsed women: An EEG study. Eat Behav. 2015, 19, 76–80. [Google Scholar] [CrossRef]
- Hume, D.J.; Howells, F.M.; Rauch, H.G.; Kroff, J.; Lambert, E.V. Electrophysiological indices of visual food cue-reactivity. Differences in obese, overweight and normal weight women. Appetite 2015, 85, 126–137. [Google Scholar] [CrossRef]
- Kumar, S.; Grundeis, F.; Brand, C.; Hwang, H.J.; Mehnert, J.; Pleger, B. Differences in Insula and Pre-/Frontal Responses during Reappraisal of Food in Lean and Obese Humans. Front. Hum. Neurosci. 2016, 10, 233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blume, M.; Schmidt, R.; Hilbert, A. Abnormalities in the EEG power spectrum in bulimia nervosa, binge-eating disorder, and obesity: A systematic review. Eur. Eat Disord. Rev. 2019, 27, 124–136. [Google Scholar] [CrossRef] [PubMed]
- Imperatori, C.; Fabbricatore, M.; Innamorati, M.; Farina, B.; Quintiliani, M.I.; Lamis, D.A.; Mazzucchi, E.; Contardi, A.; Vollono, C.; Della Marca, G. Modification of EEG functional connectivity and EEG power spectra in overweight and obese patients with food addiction: An eLORETA study. Brain Imaging Behav. 2015, 9, 703–716. [Google Scholar] [CrossRef] [PubMed]
- Kurth, B.M.; Schaffrath Rosario, A. Übergewicht und Adipositas bei Kindern und Jugendlichen in Deutschland [Overweight and obesity in children and adolescents in Germany]. Bundesgesundheitsblatt Gesundh. Gesundh. 2010, 53, 643–652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lange, M.; Kamtsiuris, P.; Lange, C.; Schaffrath Rosario, A.; Stolzenberg, H.; Lampert, T. Messung soziodemographischer Merkmale im Kinder- und Jugendgesundheitssurvey (KiGGS) und ihre Bedeutung am Beispiel der Einschätzung des allgemeinen Gesundheitszustands [Sociodemographic characteristics in the German Health Interview and Examination Survey for Children and Adolescents (KiGGS)—Operationalisation and public health significance, taking as an example the assessment of general state of health]. Bundesgesundheitsblatt Gesundh. Gesundh. 2007, 50, 578–589. [Google Scholar] [CrossRef]
- Bryant-Waugh, R.J.; Cooper, P.J.; Taylor, C.L.; Lask, B.D. The use of the eating disorder examination with children: A pilot study. Int. J. Eat Disord. 1996, 19, 391–397. [Google Scholar] [CrossRef]
- Hilbert, A. Eating Disorder Examination für Kinder: Deutschsprachige Übersetzung [Eating Disorder Examination for Children: German Translation]; DGVT-Verlag: Tübingen, Germany, 2016. [Google Scholar]
- Schneider, S.; Unnewehr, S.; Margraf, J. Kinder-DIPS: Diagnostisches Interview bei Psychischen Störungen im Kindes- und jugendalter [Diagnostic Interview for Mental Disorders in Childhood and Adolescence], 2nd ed.; Springer: Berlin/Heidelberg, Germany, 2009. [Google Scholar]
- Blechert, J.; Lender, A.; Polk, S.; Busch, N.A.; Ohla, K. Food-Pics_Extended-An image database for experimental research on eating and appetite: Additional images, normative ratings and an updated review. Front. Psychol. 2019, 10, 307. [Google Scholar] [CrossRef] [Green Version]
- Gratton, G.; Coles, M.G.; Donchin, E. A new method for off-line removal of ocular artifact. Electroencephalogr. Clin. Neurophysiol. 1983, 55, 468–484. [Google Scholar] [CrossRef]
- Wechsler, D. The Wechsler Intelligence Scale for Children, 4th ed.; Pearson: London, UK, 2003. [Google Scholar]
- Marzbani, H.; Marateb, H.R.; Mansourian, M. Neurofeedback: A comprehensive review on system design, methodology and clinical applications. Basic Clin. Neurosci. 2016, 7, 143–158. [Google Scholar] [CrossRef] [Green Version]
- Anderson, V. Assessing executive functions in children: Biological, psychological, and developmental considerations. Pediatr. Rehabil. 2001, 4, 119–136. [Google Scholar] [CrossRef]
- Bunge, S.A.; Dudukovic, N.M.; Thomason, M.E.; Vaidya, C.J.; Gabrieli, J.D. Immature frontal lobe contributions to cognitive control in children: Evidence from fMRI. Neuron 2002, 33, 301–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barriga-Paulino, C.I.; Rojas Benjumea, M.Á.; Rodríguez-Martínez, E.I.; Gómez González, C.M. Fronto-temporo-occipital activity changes with age during a visual working memory developmental study in children, adolescents and adults. Neurosci. Lett. 2015, 599, 26–31. [Google Scholar] [CrossRef] [PubMed]
- St. Louis, E.K.; Frey, L.C.; Britton, J.W.; Frey, L.C.; Hopp, J.L.; Korb, P.; Koubeissi, M.Z.; Lievens, W.E.; Pestana-Knight, E.M.; St. Louis, E.K. (Eds.) Electroencephalography (EEG): An introductory Text and Atlas of Normal and Abnormal Findings in Adults, Children, and Infants; American Epilepsy Society: Chicago, IL, USA, 2016. [Google Scholar]
- Boutelle, K.N.; Kuckertz, J.M.; Carlson, J.; Amir, N. A pilot study evaluating a one-session attention modification training to decrease overeating in obese children. Appetite 2014, 76, 180–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verbeken, S.; Braet, C.; Naets, T.; Houben, K.; Boendermaker, W.; Zeepreventorium, V. Computer training of attention and inhibition for youngsters with obesity: A pilot study. Appetite 2018, 123, 439–447. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| OO (n = 9) | NW (n = 16) | Test Statistics | |||
|---|---|---|---|---|---|
| M (SD) | M (SD) | t (23) | p | g or V | |
| Sociodemographics | |||||
| Age, years | 11.18 (2.16) | 10.63 (1.58) | −0.73 | 0.475 | 0.31 |
| Sex, female, n (%) | 5 (56) | 6 (38) | Fisher’s Exact Test | 0.434 | 0.18 |
| SES, n (%) | Fisher’s Exact Test | 0.397 | 0.24 | ||
| Medium SES | 5 (56) | 5 (31) | |||
| High SES | 4 (44) | 11 (69) | |||
| Anthropometrics | |||||
| Height, cm | 152.40 (14.28) | 148.76 (13.44) | −0.64 | 0.531 | 0.27 |
| Weight, kg | 63.36 (21.65) | 40.01 (9.42) | −3.08 | 0.012 | 1.57 |
| BMI percentile (0−100) | 96.78 (3.23) | 55.60 (20.45) | −7.88 | <0.001 | 2.48 |
| BMI-SDS | 2.15 (0.51) | 0.16 (0.59) | −8.51 | <0.001 | 3.53 |
| Intelligence estimate | |||||
| Matrix reasoning (1–19) | 11.22 (3.23) | 12.44 (1.75) | 1.05 | 0.319 | −0.51 |
| Pre-EEG | |||||
| I wish to eat (1–7) | 1.33 (1.00) | 2.50 (1.59) | 1.98 | 0.060 | 0.83 |
| I am hungry (1–7) | 1.44 (0.73) | 2.13 (1.63) | 1.44 | 0.165 | 0.50 |
| I am tired (1–7) | 2.89 (1.54) | 2.63 (1.86) | −0.36 | 0.721 | 0.15 |
| I am bored (1–7) | 2.56 (2.13) | 2.19 (1.87) | −0.45 | 0.657 | 0.19 |
| Post-EEG picture rating, high-calorie | |||||
| Recognizability (1–6) | 1.26 (0.31) | 1.30 (0.30) | 0.28 | 0.780 | 0.13 |
| Liking (1–6) | 2.67 (1.12) | 2.00 (0.97) | −1.57 | 0.131 | 0.65 |
| Desire to eat (1–6) | 3.22 (1.39) | 2.44 (1.26) | −1.44 | 0.164 | 0.60 |
| Post-EEG picture rating, low-calorie | |||||
| Recognizability (1–6) | 1.23 (0.28) | 1.27 (0.35) | 0.28 | 0.780 | 0.12 |
| Liking (1–6) | 2.67 (0.87) | 2.00 (0.97) | −1.72 | 0.100 | 0.72 |
| Desire to eat (1–6) | 3.67 (1.23) | 2.56 (0.73) | −2.85 | 0.009 | 1.19 |
| Post-EEG picture rating, neutral | |||||
| Recognizability (1–6) | 1.20 (0.26) | 1.27 (0.28) | 0.63 | 0.538 | 0.26 |
| Liking (1–6) | 2.44 (0.73) | 1.88 (0.89) | −1.64 | 0.115 | 0.67 |
| OO (n = 9) | NW (n = 16) | |||||
|---|---|---|---|---|---|---|
| High-Calorie | Low-Calorie | Neutral | High-Calorie | Low-Calorie | Neutral | |
| M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | |
| Theta | ||||||
| Frontal | 3.54 (0.06) | 3.55 (0.07) | 3.55 (0.09) | 3.49 (0.16) | 3.50 (0.14) | 3.49 (0.15) |
| Central | 2.88 (0.09) | 2.87 (0.09) | 2.88 (0.11) | 2.94 (0.17) | 2.94 (0.16) | 2.92 (0.20) |
| Temporal | 3.09 (0.08) | 3.07 (0.06) | 3.03 (0.07) | 3.03 (0.10) | 3.02 (0.08) | 3.02 (0.09) |
| Parietal | 2.72 (0.16) | 2.74 (0.16) | 2.79 (0.15) | 2.82 (0.10) | 2.80 (0.12) | 2.82 (0.10) |
| Occipital | 2.32 (0.10) | 2.30 (0.13) | 2.32 (0.08) | 2.31 (0.14) | 2.33 (0.12) | 2.34 (0.14) |
| Alpha | ||||||
| Frontal | 3.41 (0.10) | 3.40 (0.09) | 3.39 (0.08) | 3.34 (0.15) | 3.32 (0.16) | 3.35 (0.16) |
| Central | 2.88 (0.13) | 2.89 (0.14) | 2.91 (0.10) | 2.97 (0.16) | 2.94 (0.17) | 2.97 (0.19) |
| Temporal | 3.04 (0.10) | 3.04 (0.08) | 3.05 (0.08) | 2.97 (0.12) | 2.98 (0.14) | 2.97 (0.14) |
| Parietal | 3.00 (0.09) | 2.98 (0.08) | 2.98 (0.07) | 3.02 (0.12) | 3.03 (0.14) | 3.01 (0.11) |
| Occipital | 2.33 (0.23) | 2.38 (0.24) | 2.34 (0.22) | 2.41 (0.30) | 2.46 (0.28) | 2.41 (0.28) |
| Beta | ||||||
| Frontal | 3.75 (0.15) | 3.77 (0.15) | 3.75 (0.17) | 3.79 (0.17) | 3.79 (0.18) | 3.78 (0.19) |
| Central | 2.61 (0.12) | 2.61 (0.10) | 2.60 (0.11) | 2.45 (0.19) | 2.45 (0.21) | 2.44 (0.18) |
| Temporal | 3.07 (0.11) | 3.08 (0.13) | 3.11 (0.17) | 3.16 (0.17) | 3.16 (0.17) | 3.17 (0.20) |
| Parietal | 2.50 (0.15) | 2.47 (0.15) | 2.45 (0.12) | 2.39 (0.23) | 2.38 (0.24) | 2.37 (0.23) |
| Occipital | 2.17 (0.33) | 2.14 (0.29) | 2.14 (0.31) | 2.08 (0.33) | 2.07 (0.34) | 2.09 (0.36) |
| Omnibus Test | Region | Condition | Group | Region × Condition × Group | Post Hoc Tests | |
|---|---|---|---|---|---|---|
| Wald χ2 (df = 29) | χ2 (df = 4) | χ2 (df = 2) | χ2 (df = 1) | χ2 (df = 22) | ||
| Theta | 906.80 *** | 4525.426 *** | 0.032 | 0.421 | 23.545 | Frontal > temporal > central > parietal > occipital |
| Alpha | 580.00 *** | 1170.744 *** | 0.068 | 0.168 | 22.578 | Frontal > temporal = parietal > central > occipital |
| Beta | 829.33 *** | 3723.751 *** | 0.090 | 4.629 * | 31.033 † | Frontal > temporal > central > parietal > occipital; OO > NW |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kösling, C.; Schäfer, L.; Hübner, C.; Sebert, C.; Hilbert, A.; Schmidt, R. Food-Induced Brain Activity in Children with Overweight or Obesity versus Normal Weight: An Electroencephalographic Pilot Study. Brain Sci. 2022, 12, 1653. https://doi.org/10.3390/brainsci12121653
Kösling C, Schäfer L, Hübner C, Sebert C, Hilbert A, Schmidt R. Food-Induced Brain Activity in Children with Overweight or Obesity versus Normal Weight: An Electroencephalographic Pilot Study. Brain Sciences. 2022; 12(12):1653. https://doi.org/10.3390/brainsci12121653
Chicago/Turabian StyleKösling, Christine, Lisa Schäfer, Claudia Hübner, Caroline Sebert, Anja Hilbert, and Ricarda Schmidt. 2022. "Food-Induced Brain Activity in Children with Overweight or Obesity versus Normal Weight: An Electroencephalographic Pilot Study" Brain Sciences 12, no. 12: 1653. https://doi.org/10.3390/brainsci12121653