

The Impact of Sleep and Mental Health on Working Memory and Academic Performance: A Longitudinal Study
 ,
,
Abstract
:1. Introduction
2. Methodology
2.1. Ethical Statement
2.2. Participants
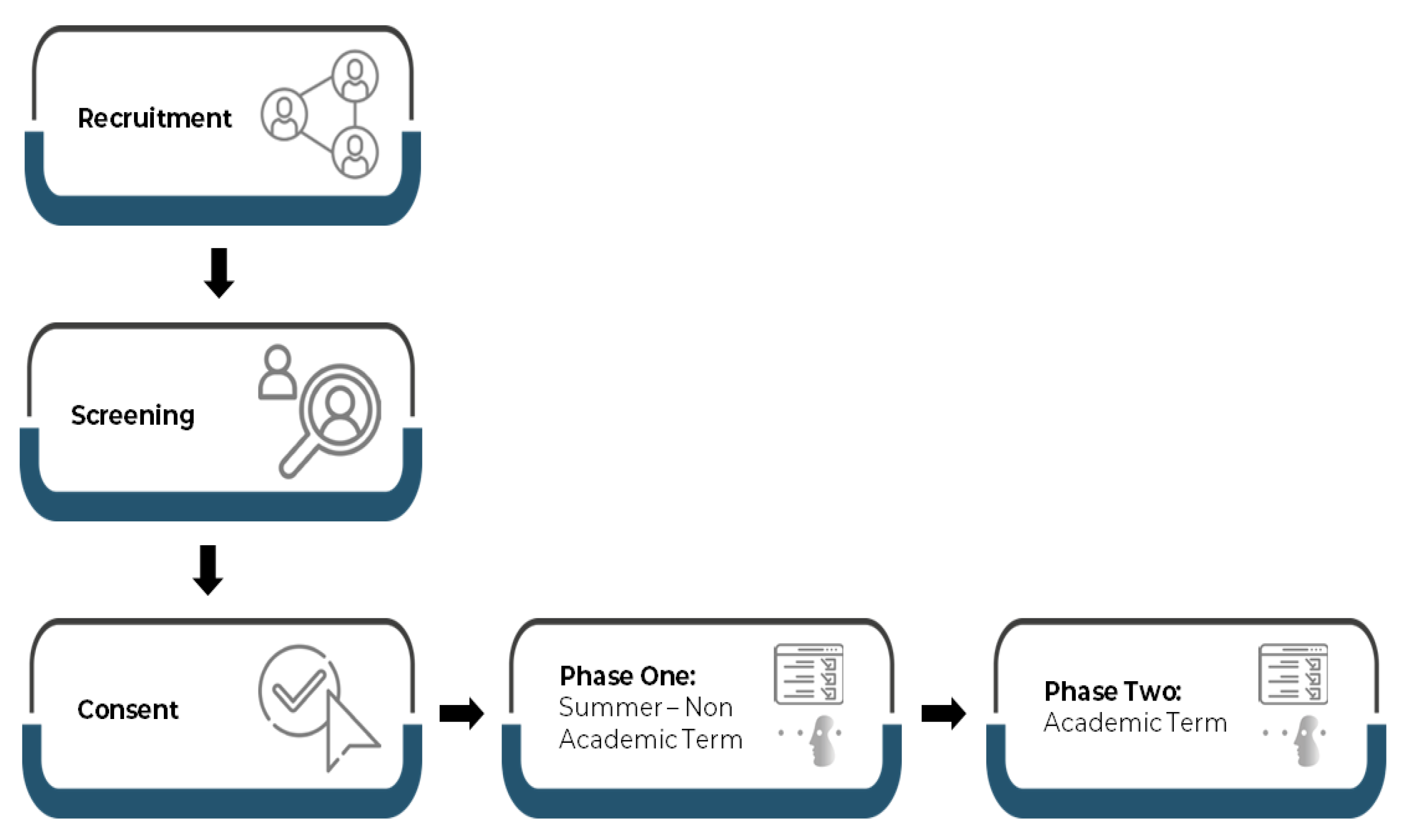
2.3. Study Design
2.4. Data Collection Methods
2.4.1. Demographic Data and Academic Performance
2.4.2. Sleep Assessment
2.4.3. Mental Health Assessments
2.4.4. Working Memory Assessment
2.4.5. Data Analysis
3. Results
3.1. Participant Demographics and Sleep Characteristics
3.2. Working Memory Scores
3.3. Mental Health Correlations with Sleep and Working Memory
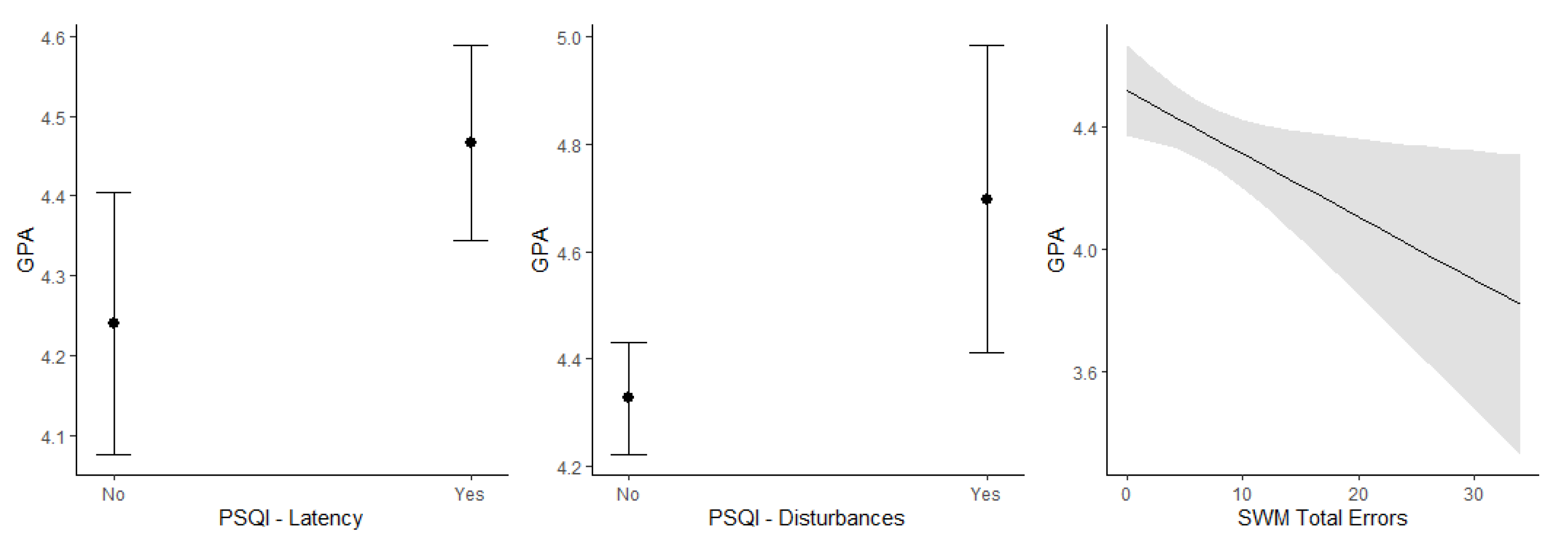
3.4. Association of Academic Performance with Sleep, Mental Well-Being, and Working Memory
4. Discussion
4.1. Sleep Habits among University Students
4.2. Sleep Habits and Their Relationship to Academic Performance
4.3. Working Memory, Academic Performance, and Sleep
4.4. Mental Health, Sleep, and Academic Performance
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Doygun, O.; Gulec, S. The Problems Faced by University Students and Proposals for Solution. Procedia—Soc. Behav. Sci. 2012, 47, 1115–1123. [Google Scholar] [CrossRef] [Green Version]
- Christiansen, A.; Salamonson, Y.; Crawford, R.; McGrath, B.; Roach, D.; Wall, P.; Kelly, M.; Ramjan, L.M. “Juggling many balls”: Working and studying among first-year nursing students. J. Clin. Nurs. 2019, 28, 4035–4043. [Google Scholar] [CrossRef]
- Kinash, S.; Crane, L.; Capper, J.; Young, M.A.; Stark, A. When do university students and graduates know what careers they want: A research-derived framework. J. Teach. Learn. 2017, 8, 3–21. [Google Scholar] [CrossRef] [Green Version]
- Gripshi, S.; Rustami, E.; Pula, A. Challenges of Nursing Students in Relation to Academic Performance at the Faculty of Technical Medical Sciences. Eur. J. Med. Nat. Sci. 2022, 5, 70–80. [Google Scholar] [CrossRef]
- Lo, S.M.; Wong, H.C.; Lam, C.Y.; Shek, D.T.L. Common Mental Health Challenges in a University Context in Hong Kong: A Study Based on a Review of Medical Records. Appl. Res. Qual. Life 2020, 15, 207–218. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Rodríguez, C.; Soto-López, T.; Cuesta, M. Needs and demands for psychological care in university students. Psicothema 2019, 31, 414–421. [Google Scholar] [CrossRef]
- Dessauvagie, A.S.; Dang, H.-M.; Nguyen, T.A.T.; Groen, G. Mental Health of University Students in Southeastern Asia: A Systematic Review. Asia Pac. J. Public Health 2022, 34, 172–181. [Google Scholar] [CrossRef]
- Grandner, M.A.; Jackson, N.J.; Izci-Balserak, B.; Gallagher, R.A.; Murray-Bachmann, R.; Williams, N.J.; Patel, N.P.; Jean-Louis, G. Social and Behavioral Determinants of Perceived Insufficient Sleep. Front. Neurol. 2015, 6, 112. [Google Scholar] [CrossRef] [Green Version]
- Phillips, A.J.K.; Clerx, W.M.; O’Brien, C.S.; Sano, A.; Barger, L.K.; Picard, R.W.; Lockley, S.W.; Klerman, E.B.; Czeisler, C.A. Irregular sleep/wake patterns are associated with poorer academic performance and delayed circadian and sleep/wake timing. Sci. Rep. 2017, 7, 3216. [Google Scholar] [CrossRef]
- Brinkman, J.E.; Reddy, V.; Sharma, S. Physiology of Sleep; StatPearls: Tampa, FL, USA, 2022. [Google Scholar]
- Killgore, W.D.S. Effects of sleep deprivation on cognition. Prog. Brain Res. 2010, 185, 105–129. [Google Scholar] [CrossRef]
- Baddeley, A. Working Memory: Theories, Models, and Controversies. Annu. Rev. Psychol. 2012, 63, 1–29. [Google Scholar] [CrossRef] [Green Version]
- Cowan, N. Working Memory Underpins Cognitive Development, Learning, and Education. Educ. Psychol. Rev. 2014, 26, 197–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siquara, G.M.; Lima, C.S.; Abreu, N. Working memory and intelligence quotient: Which best predicts on school achievement? Psico 2018, 49, 365–374. [Google Scholar] [CrossRef] [Green Version]
- Roberts, G.; Quach, J.; Gold, L.; Anderson, P.; Rickards, F.; Mensah, F.; Ainley, J.; Gathercole, S.; Wake, M. Can improving working memory prevent academic difficulties? A school based randomised controlled trial. BMC Pediatr. 2011, 11, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, Z.; Dai, C.; Ba, Y.; Zhang, L.; Shao, Y.; Tian, J. Effect of Sleep Deprivation on the Working Memory-Related N2-P3 Components of the Event-Related Potential Waveform. Front. Neurosci. 2020, 14, 469. [Google Scholar] [CrossRef]
- Vandekerckhove, M.; Wang, Y.-l. Emotion, emotion regulation and sleep: An intimate relationship. AIMS Neurosci. 2018, 1, 1–22. [Google Scholar] [CrossRef]
- Babson, K.A.; Trainor, C.D.; Feldner, M.T.; Blumenthal, H. A test of the effects of acute sleep deprivation on general and specific self-reported anxiety and depressive symptoms: An experimental extension. J. Behav. Ther. Exp. Psychiatry 2010, 41, 297–303. [Google Scholar] [CrossRef] [Green Version]
- Dimitriou, D.; Le Cornu Knight, F.; Milton, P. The Role of Environmental Factors on Sleep Patterns and School Performance in Adolescents. Front. Psychol. 2015, 6, 1717. [Google Scholar] [CrossRef] [Green Version]
- Alhusseini, N.K.; Ramadan, M.; Almasry, Y.; Atout, M.; Hamsho, K.; Mahmoud, M.; Alnasser, S.; Shakir, I. Effects of Sleep Quality on Academic Performance and Psychological Distress Among Medical Students in Saudi Arabia. Health Scope 2022, 11, e123801. [Google Scholar] [CrossRef]
- Vedaa, Ø.; Erevik, E.K.; Hysing, M.; Hayley, A.C.; Sivertsen, B. Insomnia, sleep duration and academic performance: A national survey of Norwegian college and university students. Sleep Med. X 2019, 1, 100005. [Google Scholar] [CrossRef]
- Ahrberg, K.; Dresler, M.; Niedermaier, S.; Steiger, A.; Genzel, L. The interaction between sleep quality and academic performance. J. Psychiatr. Res. 2012, 46, 1618–1622. [Google Scholar] [CrossRef]
- Ibrahim, N.K.; Badawi, F.; Mansouri, Y.; Ainousa, A.; Jambi, S.; Fatani, A.N. Sleep Quality among Medical Students at King Abdulaziz University: A Cross-sectional Study. J. Community Med. Health Educ. 2017, 7, 2161–2711. [Google Scholar] [CrossRef] [Green Version]
- Al-Khani, A.M.; Sarhandi, M.I.; Zaghloul, M.S.; Ewid, M.; Saquib, N. A cross-sectional survey on sleep quality, mental health, and academic performance among medical students in Saudi Arabia. BMC Res. Notes 2019, 12, 665. [Google Scholar] [CrossRef]
- Alotaibi, A.D.; Alosaimi, F.M.; Alajlan, A.A.; Bin Abdulrahman, K.A. The relationship between sleep quality, stress, and academic performance among medical students. J. Fam. Community Med. 2020, 27, 23–28. [Google Scholar] [CrossRef]
- Mehta, K.J. Effect of sleep and mood on academic performance—At interface of physiology, psychology, and education. Humanit. Soc. Sci. Commun. 2022, 9, 16. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder. Arch. Intern. Med. 2006, 166, 1092. [Google Scholar] [CrossRef] [Green Version]
- Kessler, R.C.; Andrews, G.; Colpe, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.-L.T.; Walters, E.E.; Zaslavsky, A.M. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef]
- van den Eijnden, R.J.J.M.; Lemmens, J.S.; Valkenburg, P.M. The Social Media Disorder Scale. Comput. Hum. Behav. 2016, 61, 478–487. [Google Scholar] [CrossRef]
- Robbins, T.W.; James, M.; Owen, A.M.; Sahakian, B.J.; McInnes, L.; Rabbitt, P. Cambridge Neuropsychological Test Automated Battery (CANTAB): A Factor Analytic Study of a Large Sample of Normal Elderly Volunteers. Dement. Geriatr. Cogn. Disord. 1994, 5, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Blankenship, T.L.; O’Neill, M.; Ross, A.; Bell, M.A. Working memory and recollection contribute to academic achievement. Learn. Individ. Differ. 2015, 43, 164–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Owens, M.; Stevenson, J.; Hadwin, J.A.; Norgate, R. Anxiety and depression in academic performance: An exploration of the mediating factors of worry and working memory. Sch. Psychol. Int. 2012, 33, 433–449. [Google Scholar] [CrossRef]
- Irish, L.A.; Kline, C.E.; Gunn, H.E.; Buysse, D.J.; Hall, M.H. The role of sleep hygiene in promoting public health: A review of empirical evidence. Sleep Med. Rev. 2015, 22, 23–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, M.X.; Wu, A.M.S. Effects of smartphone addiction on sleep quality among Chinese university students: The mediating role of self-regulation and bedtime procrastination. Addict. Behav. 2020, 111, 106552. [Google Scholar] [CrossRef]
- Jniene, A.; Errguig, L.; El Hangouche, A.J.; Rkain, H.; Aboudrar, S.; El Ftouh, M.; Dakka, T. Perception of Sleep Disturbances due to Bedtime Use of Blue Light-Emitting Devices and Its Impact on Habits and Sleep Quality among Young Medical Students. BioMed Res. Int. 2019, 2019, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Hoefelmann, L.P.; Lopes, A.d.S.; da Silva, K.S.; Moritz, P.; Nahas, M.V. Sociodemographic factors associated with sleep quality and sleep duration in adolescents from Santa Catarina, Brazil: What changed between 2001 and 2011? Sleep Med. 2013, 14, 1017–1023. [Google Scholar] [CrossRef]
- Cross, Z.R.; Kohler, M.J.; Schlesewsky, M.; Gaskell, M.G.; Bornkessel-Schlesewsky, I. Sleep-Dependent Memory Consolidation and Incremental Sentence Comprehension: Computational Dependencies during Language Learning as Revealed by Neuronal Oscillations. Front. Hum. Neurosci. 2018, 12, 18. [Google Scholar] [CrossRef] [Green Version]
- Medic, G.; Wille, M.; Hemels, M. Short- and long-term health consequences of sleep disruption. Nat. Sci. Sleep 2017, 9, 151–161. [Google Scholar] [CrossRef] [Green Version]
- El Hangouche, A.J.; Jniene, A.; Aboudrar, S.; Errguig, L.; Rkain, H.; Cherti, M.; Dakka, T. Relationship between poor quality sleep, excessive daytime sleepiness and low academic performance in medical students. Adv. Med. Educ. Pract. 2018, 9, 631–638. [Google Scholar] [CrossRef]
- Rasekhi, S.; Ashouri, F.P.; Pirouzan, A. Effects of Sleep Quality on the Academic Performance of Undergraduate Medical Students. Health Scope 2016, 5, e31641. [Google Scholar] [CrossRef] [Green Version]
- Okano, K.; Kaczmarzyk, J.R.; Dave, N.; Gabrieli, J.D.E.; Grossman, J.C. Sleep quality, duration, and consistency are associated with better academic performance in college students. NPJ Sci. Learn. 2019, 4, 16. [Google Scholar] [CrossRef] [Green Version]
- Armand, M.A.; Biassoni, F.; Corrias, A. Sleep, Well-Being and Academic Performance: A Study in a Singapore Residential College. Front. Psychol. 2021, 12, 1866. [Google Scholar] [CrossRef]
- Jalali, R.; Khazaie, H.; Khaledi Paveh, B.; Hayrani, Z.; Menati, L. The Effect of Sleep Quality on Students’ Academic Achievement. Adv. Med. Educ. Pract. 2020, 11, 497–502. [Google Scholar] [CrossRef]
- Hennecke, E.; Lange, D.; Steenbergen, F.; Fronczek-Poncelet, J.; Elmenhorst, D.; Bauer, A.; Aeschbach, D.; Elmenhorst, E.M. Adverse interaction effects of chronic and acute sleep deficits on spatial working memory but not on verbal working memory or declarative memory. J. Sleep Res. 2021, 30, e13225. [Google Scholar] [CrossRef]
- Rana, B.K.; Panizzon, M.S.; Franz, C.E.; Spoon, K.M.; Jacobson, K.C.; Xian, H.; Ancoli-Israel, S.; Lyons, M.; Kremen, W.S. Association of Sleep Quality on Memory-Related Executive Functions in Middle Age. J. Int. Neuropsychol. Soc. 2018, 24, 67–76. [Google Scholar] [CrossRef]
- Pasula, E.Y.; Brown, G.G.; McKenna, B.S.; Mellor, A.; Turner, T.; Anderson, C.; Drummond, S.P.A. Effects of sleep deprivation on component processes of working memory in younger and older adults. Sleep 2018, 41, zsx213. [Google Scholar] [CrossRef]
- Xie, W.; Berry, A.; Lustig, C.; Deldin, P.; Zhang, W. Poor Sleep Quality and Compromised Visual Working Memory Capacity. J. Int. Neuropsychol. Soc. 2019, 25, 583–594. [Google Scholar] [CrossRef]
- Keyes, C.L.M. Promoting and Protecting Positive Mental Health: Early and Often Throughout the Lifespan. In Mental Well-Being; Springer: Dordrecht, The Netherlands, 2013; pp. 3–28. [Google Scholar] [CrossRef]
- Steele, R.G.; Hall, J.A.; Christofferson, J.L. Conceptualizing Digital Stress in Adolescents and Young Adults: Toward the Development of an Empirically Based Model. Clin. Child Fam. Psychol. Rev. 2020, 23, 15–26. [Google Scholar] [CrossRef]
- Seiffge-Krenke, I.; Persike, M.; Karaman, N.G.; Cok, F.; Herrera, D.; Rohail, I.; Macek, P.; Hyeyoun, H. Stress With Parents and Peers: How Adolescents From Six Nations Cope With Relationship Stress. J. Res. Adolesc. 2013, 23, 103–117. [Google Scholar] [CrossRef]
- Zhu, X.; Haegele, J.A.; Liu, H.; Yu, F. Academic Stress, Physical Activity, Sleep, and Mental Health among Chinese Adolescents. Int. J. Environ. Res. Public Health 2021, 18, 7257. [Google Scholar] [CrossRef] [PubMed]
- Almojali, A.I.; Almalki, S.A.; Alothman, A.S.; Masuadi, E.M.; Alaqeel, M.K. The prevalence and association of stress with sleep quality among medical students. J. Epidemiol. Glob. Health 2017, 7, 169. [Google Scholar] [CrossRef] [PubMed]
- Al-Maddah, E.M.; Al-Dabal, B.K.; Khalil, M.S. Prevalence of Sleep Deprivation and Relation with Depressive Symptoms among Medical Residents in King Fahd University Hospital, Saudi Arabia. Sultan Qaboos Univ. Med. J. 2015, 15, e78–e84. [Google Scholar] [PubMed]
- Krystal, A.D. Psychiatric Disorders and Sleep. Neurol. Clin. 2012, 30, 1389–1413. [Google Scholar] [CrossRef] [Green Version]
- Agnafors, S.; Barmark, M.; Sydsjö, G. Mental health and academic performance: A study on selection and causation effects from childhood to early adulthood. Soc. Psychiatry Psychiatr. Epidemiol. 2021, 56, 857–866. [Google Scholar] [CrossRef]
- Zapata-Lamana, R.; Sanhueza-Campos, C.; Stuardo-Álvarez, M.; Ibarra-Mora, J.; Mardones-Contreras, M.; Reyes-Molina, D.; Vásquez-Gómez, J.; Lasserre-Laso, N.; Poblete-Valderrama, F.; Petermann-Rocha, F.; et al. Anxiety, Low Self-Esteem and a Low Happiness Index Are Associated with Poor School Performance in Chilean Adolescents: A Cross-Sectional Analysis. Int. J. Environ. Res. Public Health 2021, 18, 11685. [Google Scholar] [CrossRef]
- Grøtan, K.; Sund, E.R.; Bjerkeset, O. Mental Health, Academic Self-Efficacy and Study Progress Among College Students—The SHoT Study, Norway. Front. Psychol. 2019, 10, 45. [Google Scholar] [CrossRef] [Green Version]
- Bemath, N.; Cockcroft, K.; Theron, L. Working memory and psychological resilience in South African emerging adults. S. Afr. J. Psychol. 2020, 50, 493–506. [Google Scholar] [CrossRef]
- Chunming, W.M.; Harrison, R.; MacIntyre, R.; Travaglia, J.; Balasooriya, C. Burnout in medical students: A systematic review of experiences in Chinese medical schools. BMC Med. Educ. 2017, 17, 217. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Summer Period | Academic Term | Difference | Significance | |
|---|---|---|---|---|
| Sample size | 83 | 83 | ||
| Age in years—Mean (SD) | 21.82 (1.59) | 22.05 (1.37) | ||
| Gender—Male—No. (%) | 35 (42.2) | 35 (42.2) | ||
| Marital status—Single—No. (%) | 81 (97.6) | 80 (96.4) | ||
| Smoker—Yes—No. (%) | 10 (12.0) | 12 (14.5) | ||
| Caffeinated Drinks Yes—No. (%) | 49 (92.5) | 49 (96.1%) | ||
| Confirmed illness—Yes—No. (%) | 15 (18.1) | 10 (12.0) | ||
| Year number—Mean (SD) | 4.36 (1.30) | 4.43 (1.29) | ||
| GPA—Mean (SD) | 4.37 (0.53) | 4.39 (0.46) | 0.02 | t (81) = −0.23, p = 0.816 |
| PSQI—Total—Mean (SD) | 6.99 (3.28) | 7.98 (2.86) | 0.99 | t (82) = −2.64, p = 0.010 * |
| 1.25 (0.71) | 1.34 (0.74) | 0.08 | t (82) = −0.93, p = 0.357 |
| 1.58 (1.07) | 1.58 (0.96) | 0.00 | t (82) = 0.00, p = 1.000 |
| 1.00 (1.01) | 1.51 (1.00) | 0.51 | t (82) = −3.93, p = 0.000 * |
| 0.74 (1.12) | 0.57 (0.88) | −0.16 | t (74) = 0.78, p = 0.439 |
| 1.17 (0.50) | 1.11 (0.47) | −0.06 | t (74) = 1.15, p = 0.254 |
| 0.27 (0.75) | 0.47 (0.87) | 0.20 | t (82) = −2.06, p = 0.043 * |
| 1.14 (0.91) | 1.42 (0.89) | 0.28 | t (82) = −2.33, p = 0.023 * |
| Distress (K10)—Mean (SD) | 22.27 (7.55) | 25.63 (8.68) | 3.36 | t (82) = −4.01, p = 0.000 * |
| Anxiety (GAD-7)—Mean (SD) | 6.94 (5.13) | 7.86 (4.75) | 0.92 | t (82) = −1.63, p = 0.107 |
| Depression (PHQ-9)—Mean (SD) | 7.59 (6.23) | 8.75 (5.77) | 1.16 | t (82) = −1.71, p = 0.091 |
| Social Media (SMD)—Mean (SD) | 2.60 (1.93) | 2.24 (1.90) | −0.36 | t (82) = 1.68, p = 0.097 |
| Summer Period | Academic Term | Difference | Significance | |
|---|---|---|---|---|
| SWM Strategy | ||||
| 6-token trials | 3.17 (0.96) | 2.87 (1.16) | −0.3 | t (82) = 2.35, p = 0.021 * |
| 6–8-token trials | 7.42 (2.18) | 6.66 (2.72) | −0.76 | t (82) = 3.01, p = 0.003 * |
| 6–12-token trials | 13.64 (3.75) | 12.52 (4.58) | −1.12 | t (82) = 2.83, p = 0.006 * |
| SWM Total Errors | ||||
| 4-token trials | 0.35 (0.76) | 0.31 (0.85) | −0.04 | t (82) = 0.40, p = 0.694 |
| 6-token trials | 1.63 (2.64) | 1.60 (2.88) | −0.02 | t (82) = 0.07, p = 0.944 |
| 8-token trials | 4.72 (5.68) | 5.04 (5.93) | 0.31 | t (82) = −0.55, p = 0.582 |
| 4–8-token trials | 6.70 (7.48) | 6.95 (8.10) | 0.25 | t (82) = −0.36, p = 0.721 |
| 12-token trials | 25.30 (15.03) | 22.64 (14.84) | −2.66 | t (82) = 1.25, p = 0.217 |
| Academic Term | ||||||
|---|---|---|---|---|---|---|
| Measure | Distress | Anxiety | Depression | Distress | Anxiety | Depression |
| Total | r = 0.433 * | r = 0.360 * | r = 0.498 * | r = 0.400 * | r = 0.322 * | r = 0.264 * |
| Quality | r = 0.418 * | r = 0.221 * | r = 0.389 * | r = 0.253 * | r = 0.213 | r = 0.184 |
| Latency | r = 0.395 * | r = 0.235 * | r = 0.438 * | r = 0.143 | r = 0.263 * | r = 0.136 |
| Duration | r = −0.099 | r = −0.063 | r = −0.050 | r = 0.151 | r = −0.010 | r = 0.056 |
| Efficiency | r = −0.035 | r = −0.031 | r = 0.098 | r = −0.057 | r = −0.007 | r = 0.006 |
| Disturbances | r = 0.540 * | r = 0.608 * | r = 0.513 * | r = 0.385 * | r = 0.307 * | r = 0.370 * |
| Medication | r = 0.091 | r = 0.178 | r = 0.063 | r = 0.144 | r = 0.175 | r = −0.012 |
| Dysfunction | r = 0.630 * | r = 0.499 * | r = 0.644 * | r = 0.442 * | r = 0.241 * | r = 0.274 * |
| SWM Strategy | r = −0.126 | r = −0.042 | r = −0.034 | r = −0.007 | r = −0.123 | r = 0.028 |
| SWM Errors | r = 0.027 | r = 0.01 | r = 0.114 | r = 0.148 | r = −0.041 | r = 0.098 |
| Summer Period | Academic Term | |
|---|---|---|
| PSQI—Total | F (1,62) = 0.13, p = 0.719 | F (1,67) = 0.21, p = 0.646 |
| F (1,62) = 0.42, p = 0.521 | F (1,67) = 0.99, p = 0.323 |
| F (1,62) = 2.81, p = 0.099 | F (1,67) = 4.47, p = 0.038 * |
| F (1,62) = 3.98, p = 0.050 | F (1,67) = 2.81, p = 0.098 |
| F (1,62) = 1.60, p = 0.210 | F (1,67) = 0.56, p = 0.456 |
| F (1,62) = 0.51, p = 0.478 | F (1,67) = 5.45, p = 0.023 * |
| F (1,62) = 0.41, p = 0.522 | F (1,67) = 3.76, p = 0.057 |
| F (1,62) = 3.08, p = 0.084 | F (1,67) = 0.04, p = 0.834 |
| Distress (K10) | F (1,62) = 1.27, p = 0.263 | F (1,67) = 0.54, p = 0.464 |
| Anxiety (GAD-7) | F (1,62) = 0.28, p = 0.601 | F (1,67) = 0.22, p = 0.642 |
| Depression (PHQ-9) | F (1,62) = 1.03, p = 0.314 | F (1,67) = 1.41, p = 0.239 |
| SWM Strategy | F (1,62) = 1.11, p = 0.296 | F (1,67) = 0.27, p = 0.602 |
| SWM Errors | F (1,62) = 0.03, p = 0.868 | F (1,67) = 5.50, p = 0.022 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almarzouki, A.F.; Mandili, R.L.; Salloom, J.; Kamal, L.K.; Alharthi, O.; Alharthi, S.; Khayyat, N.; Baglagel, A.M. The Impact of Sleep and Mental Health on Working Memory and Academic Performance: A Longitudinal Study. Brain Sci. 2022, 12, 1525. https://doi.org/10.3390/brainsci12111525
Almarzouki AF, Mandili RL, Salloom J, Kamal LK, Alharthi O, Alharthi S, Khayyat N, Baglagel AM. The Impact of Sleep and Mental Health on Working Memory and Academic Performance: A Longitudinal Study. Brain Sciences. 2022; 12(11):1525. https://doi.org/10.3390/brainsci12111525
Chicago/Turabian StyleAlmarzouki, Abeer F., Rahaf L. Mandili, Joud Salloom, Lujain K. Kamal, Omimah Alharthi, Samah Alharthi, Nusaiba Khayyat, and Alaa M. Baglagel. 2022. "The Impact of Sleep and Mental Health on Working Memory and Academic Performance: A Longitudinal Study" Brain Sciences 12, no. 11: 1525. https://doi.org/10.3390/brainsci12111525