
The Current State of Visualization Techniques in Endoscopic Skull Base Surgery

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
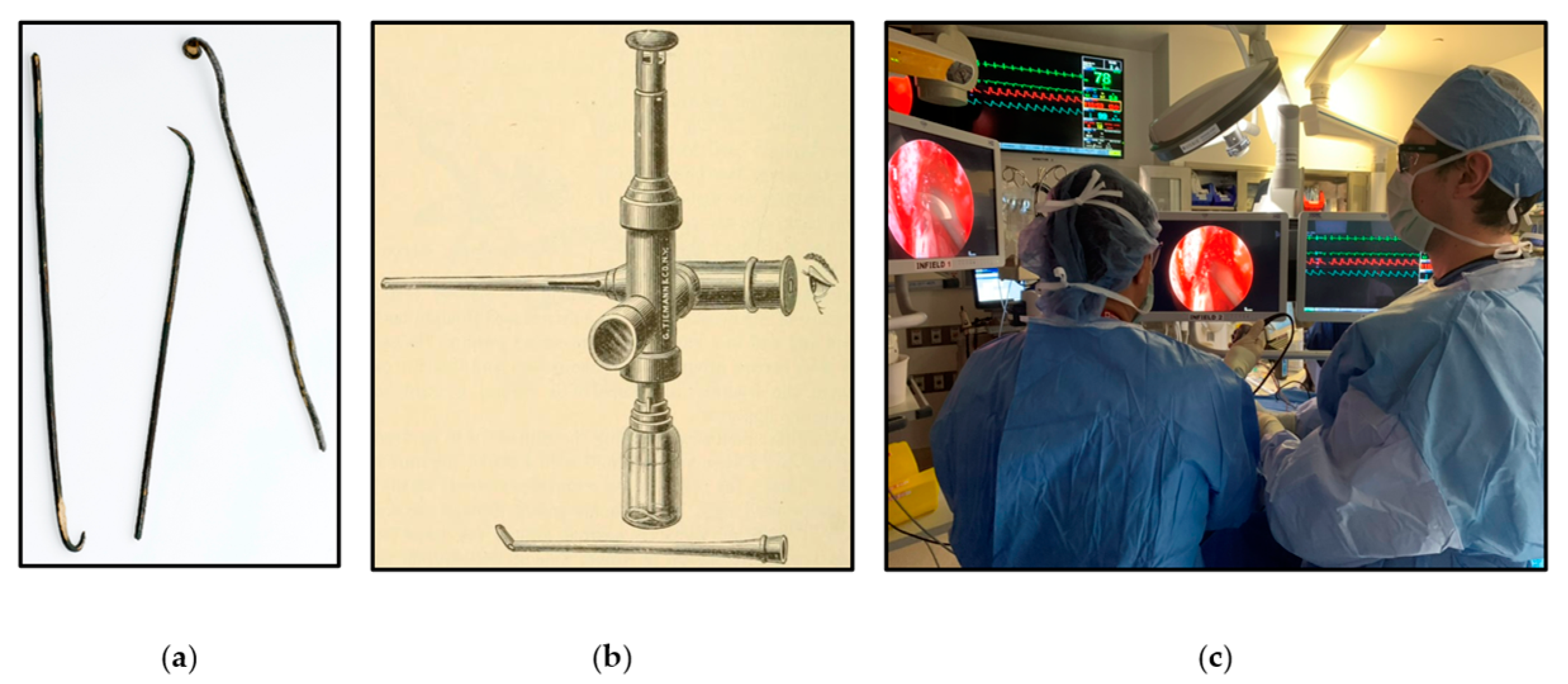
2. The History and Development of Endoscopic Skull Base Surgery
3. The Current State of Visualization Techniques in Endoscopic Skull Base Surgery
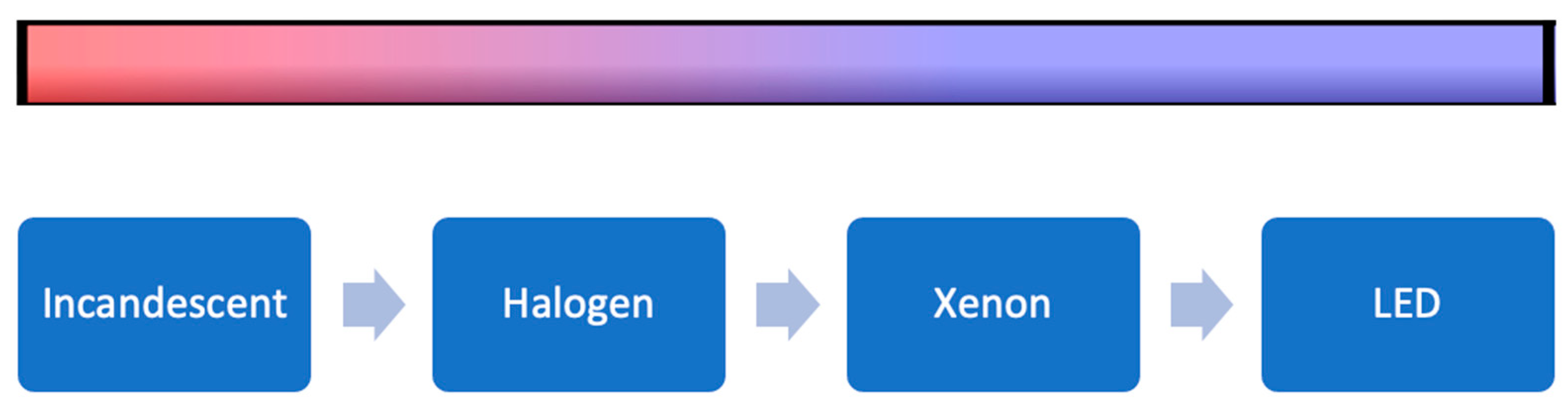
3.1. Illuminance and Brightness
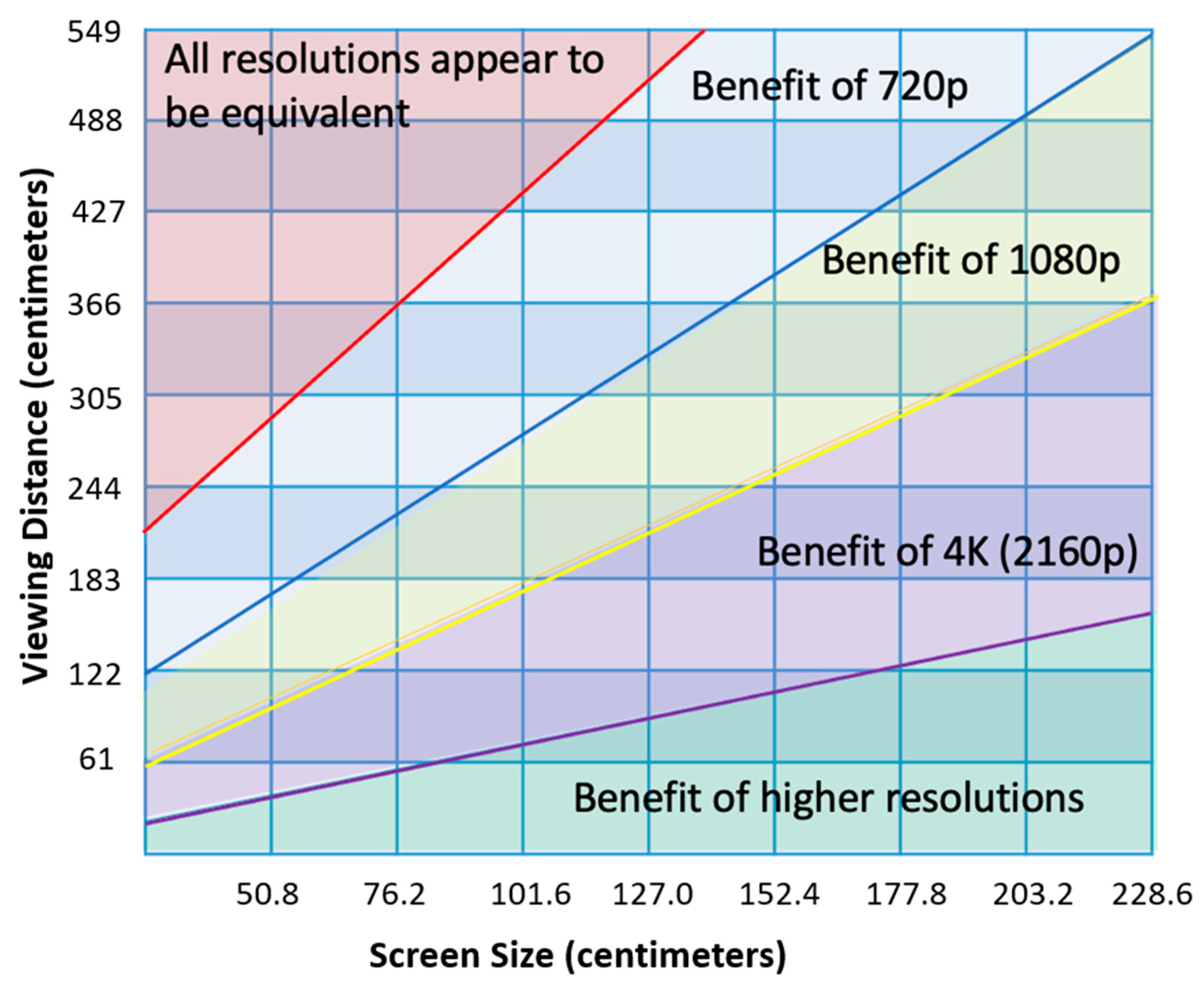
3.2. Resolution
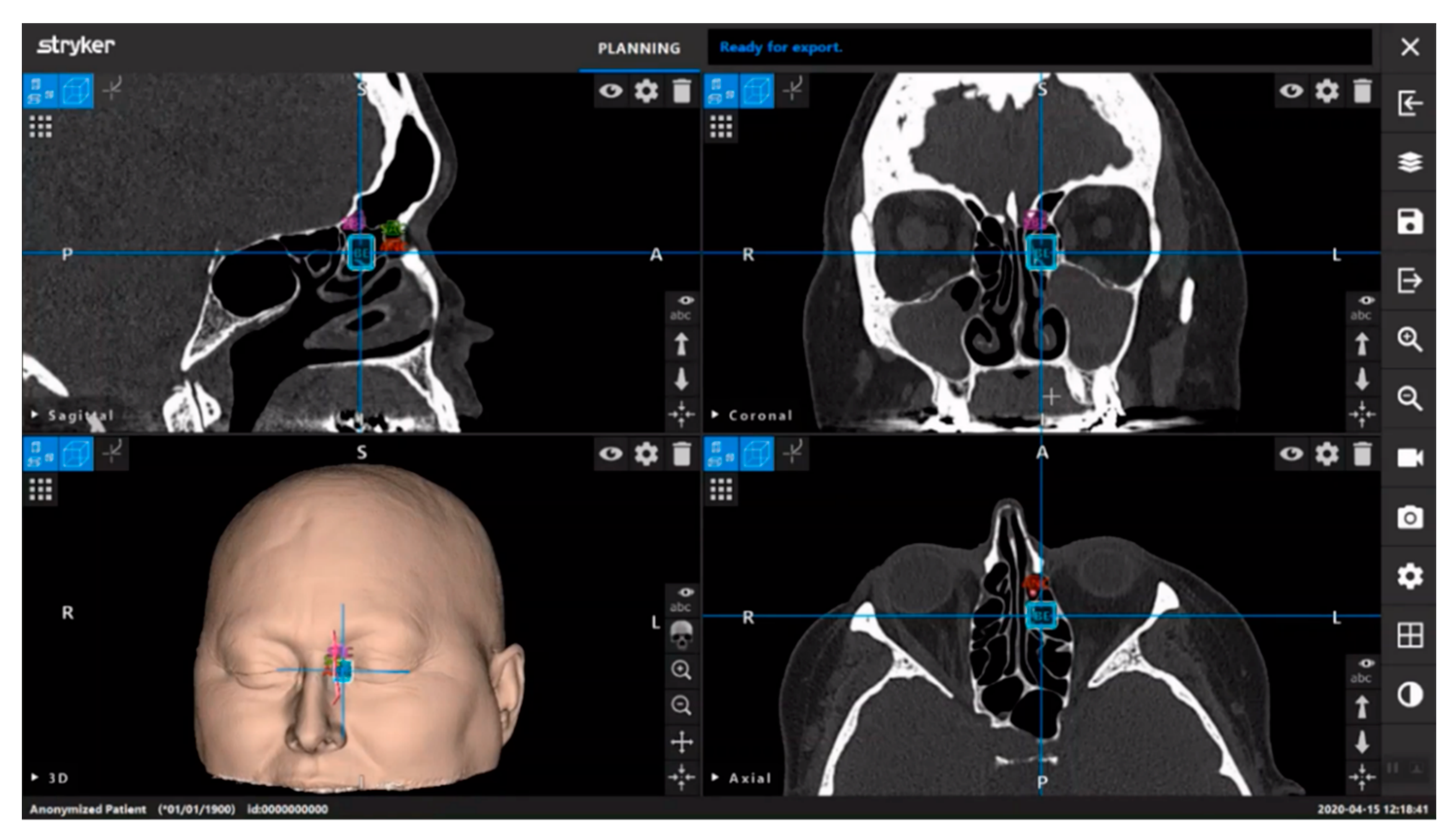
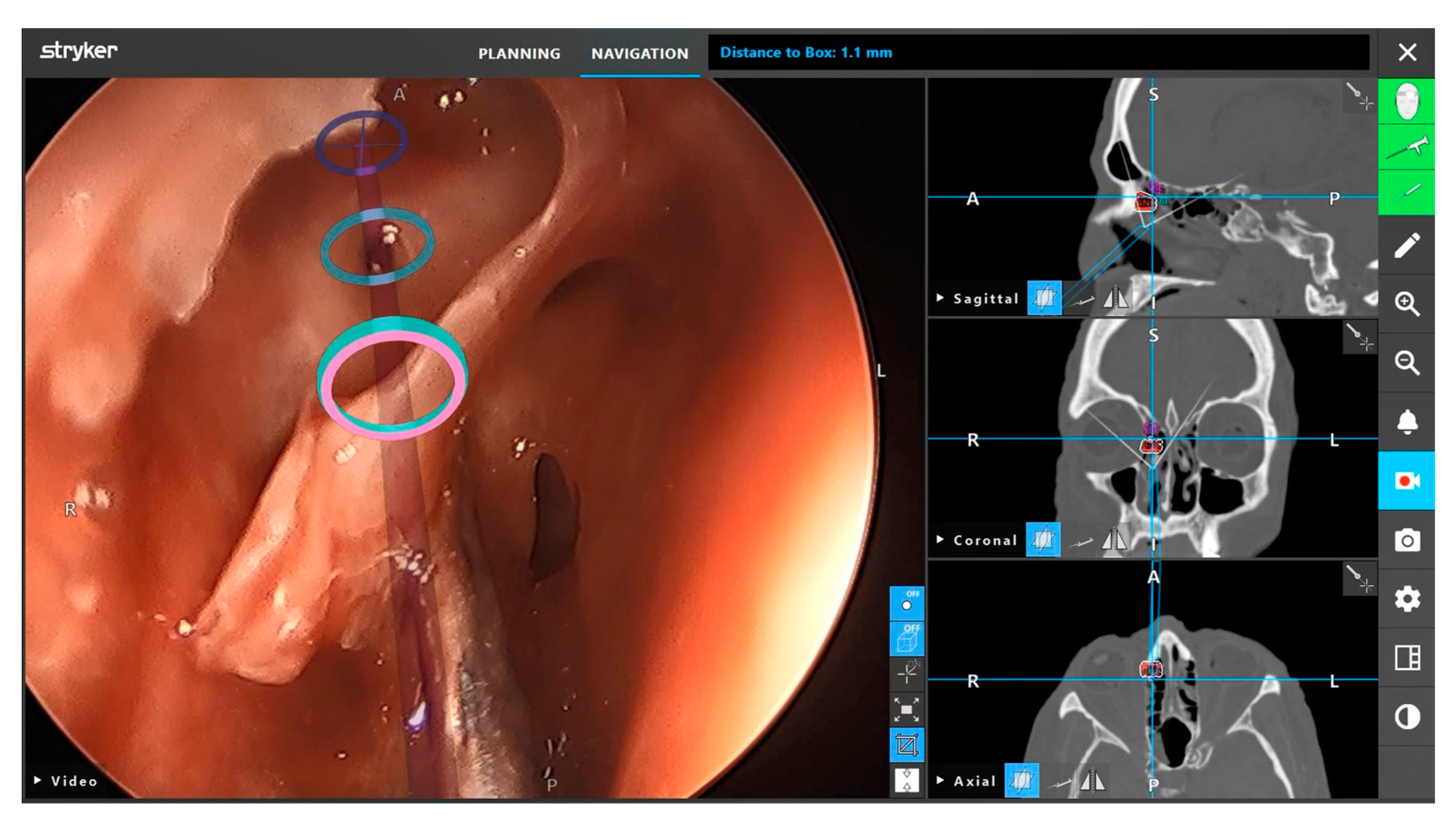
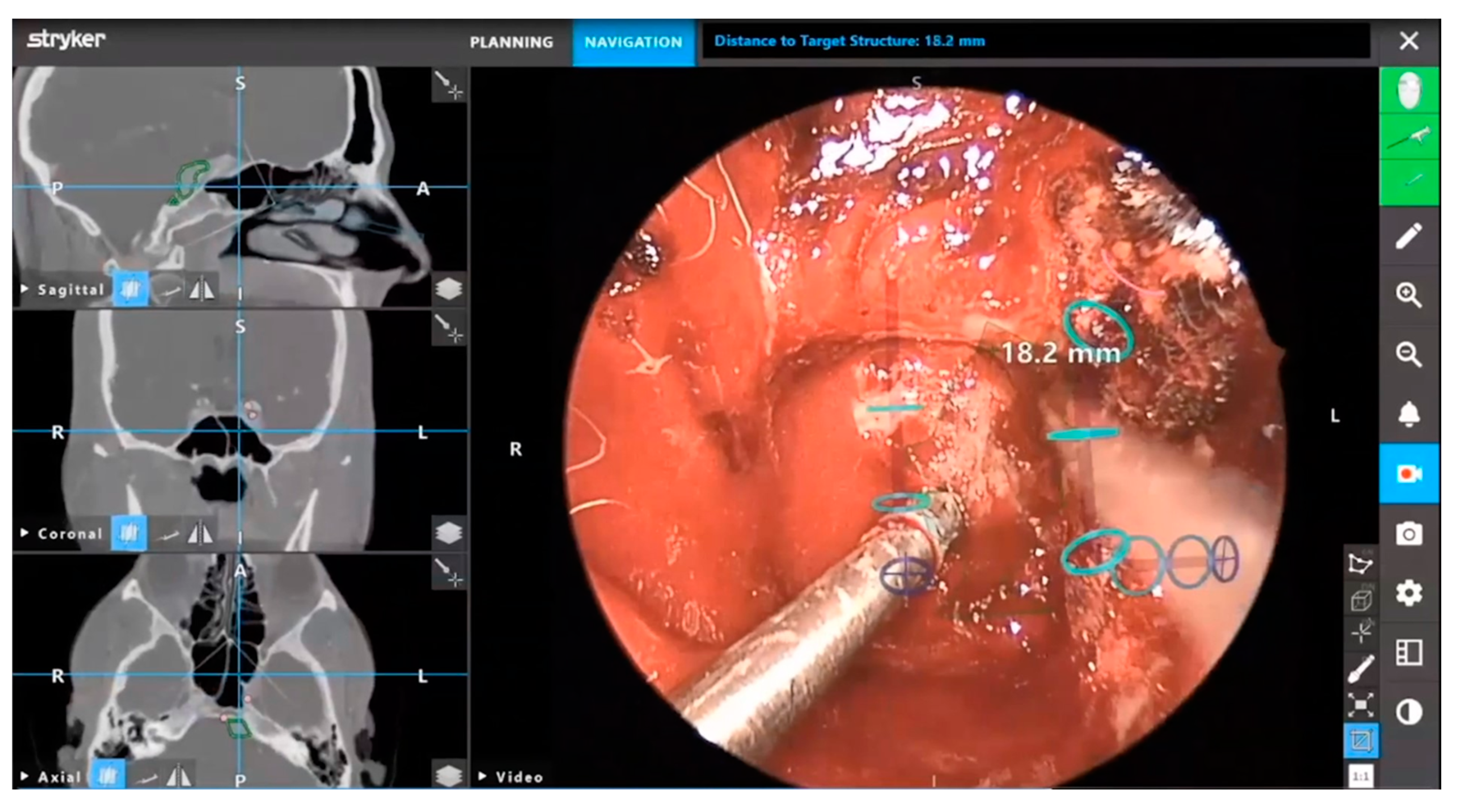
3.3. Neuronavigation
3.4. Robotics
3.5. Intraoperative Imaging
3.5.1. Real-Time Fluorescence Agents
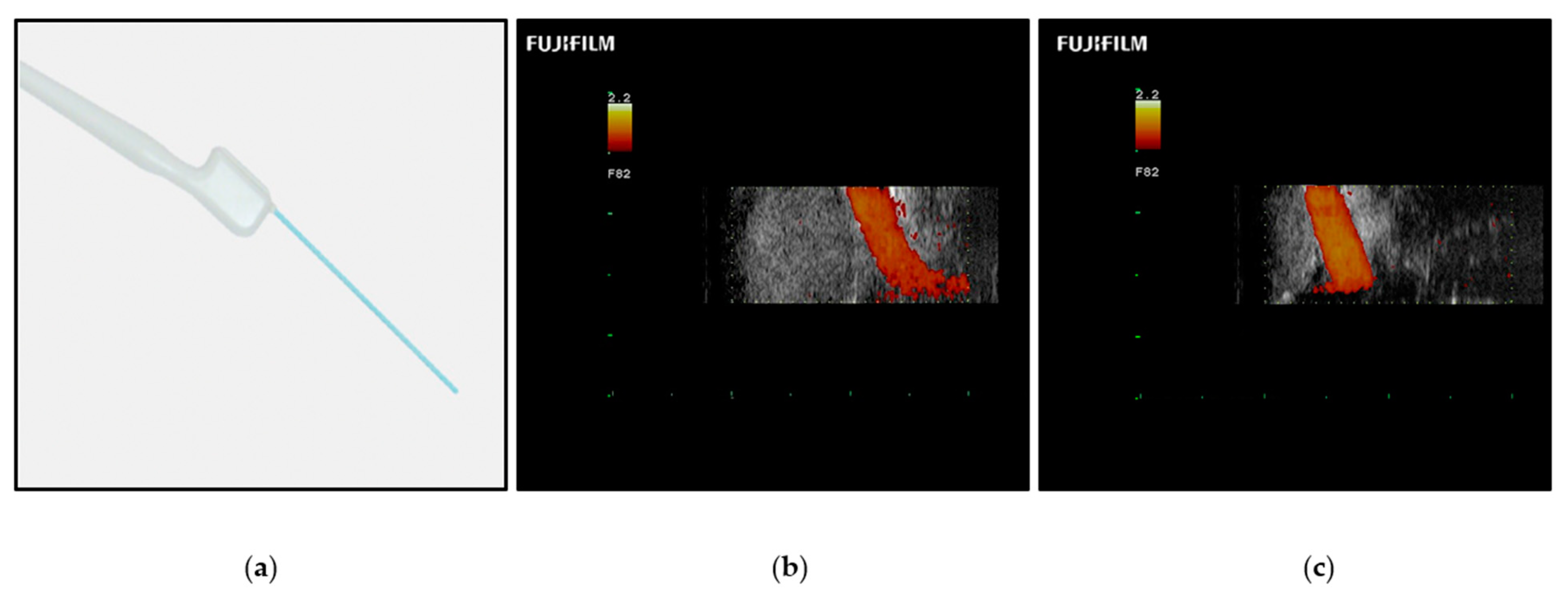
3.5.2. Ultrasonography
3.5.3. Computed Tomography and Magnetic Resonance Imaging
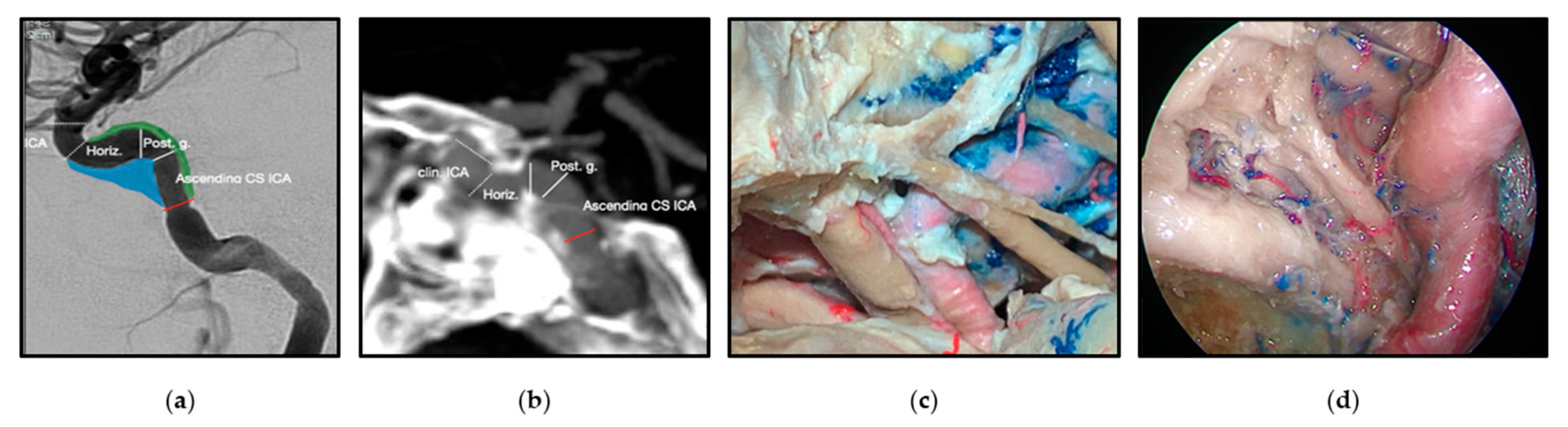
3.6. Neuroanatomy
3.7. The Exoscope
4. Future Innovations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jawad, B.; Vankoevering, K.; Carrau, R.; Patil, Y. Clinical Considerations for Open versus Endoscopic Approaches in Skull Base Surgery. Curr. Opin. Otolaryngol. Head Neck Surg. 2022, 30, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Wang, E.W.; Zanation, A.M.; Gardner, P.A.; Schwartz, T.H.; Eloy, J.A.; Adappa, N.D.; Bettag, M.; Bleier, B.S.; Cappabianca, P.; Carrau, R.L. ICAR: Endoscopic Skull-base Surgery. Int. Forum Allergy Rhinol. 2019, 9, 145–365. [Google Scholar] [CrossRef] [Green Version]
- Goshtasbi, K.; Lehrich, B.M.; Abouzari, M.; Abiri, A.; Birkenbeuel, J.; Lan, M.-Y.; Wang, W.-H.; Cadena, G.; Hsu, F.P.K.; Kuan, E.C. Endoscopic versus Nonendoscopic Surgery for Resection of Pituitary Adenomas: A National Database Study. J. Neurosurg. 2021, 134, 816–824. [Google Scholar] [CrossRef] [PubMed]
- Batra, P.S.; Lee, J.; Barnett, S.L.; Senior, B.A.; Setzen, M.; Kraus, D.H. Endoscopic Skull Base Surgery Practice Patterns: Survey of the North American Skull Base Society: Skull Base Surgery Survey of NASBS. Int. Forum Allergy Rhinol. 2013, 3, 659–663. [Google Scholar] [CrossRef] [PubMed]
- Kasemsiri, P.; Carrau, R.L.; Ditzel Filho, L.F.S.; Prevedello, D.M.; Otto, B.A.; Old, M.; de Lara, D.; Kassam, A.B. Advantages and Limitations of Endoscopic Endonasal Approaches to the Skull Base. World Neurosurg. 2014, 82, S12–S21. [Google Scholar] [CrossRef]
- Martinez-Perez, R.; Requena, L.C.; Carrau, R.L.; Prevedello, D.M. Modern Endoscopic Skull Base Neurosurgery. J. Neurooncol. 2021, 151, 461–475. [Google Scholar] [CrossRef]
- Borg, A.; Kirkman, M.A.; Choi, D. Endoscopic Endonasal Anterior Skull Base Surgery: A Systematic Review of Complications during the Past 65 Years. World Neurosurg. 2016, 95, 383–391. [Google Scholar] [CrossRef]
- Saleem, S.N.; Hawass, Z. Variability in Brain Treatment during Mummification of Royal Egyptians Dated to the 18th–20th Dynasties: MDCT Findings Correlated with the Archaeologic Literature. Am. J. Roentgenol. 2013, 200, W336–W344. [Google Scholar] [CrossRef]
- Ramai, D.; Zakhia, K.; Etienne, D.; Reddy, M. Philipp Bozzini (1773–1809): The Earliest Description of Endoscopy. J. Med. Biogr. 2018, 26, 137–141. [Google Scholar] [CrossRef]
- Ahmed, O.H.; Marcus, S.; Lebowitz, R.A.; Jacobs, J.B. Evolution in Visualization for Sinus and Skull Base Surgery: From Headlight to Endoscope. Otolaryngol. Clin. N. Am. 2017, 50, 505–519. [Google Scholar] [CrossRef]
- Apuzzo, M.L.J.; Heifetz, M.D.; Weiss, M.H.; Kurze, T. Neurosurgical Endoscopy Using the Side-Viewing Telescope: Technical Note. J. Neurosurg. 1977, 46, 398–400. [Google Scholar] [CrossRef] [Green Version]
- Welcome Collection. Available online: https://wellcomecollection.org/works/ej23b2n4 (accessed on 1 September 2022).
- Jankowski, R.; Auque, J.; Simon, C.; Marchal, J.C.; Hepner, H.; Wayoff, M. How I Do It: Head and Neck and Plastic Surgery: Endoscopic Pituitary Tumor Surgery. Laryngoscope 1992, 102, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Jho, H.-D.; Carrau, R.L. Endoscopic Endonasal Transsphenoidal Surgery: Experience with 50 Patients. J. Neurosurg. 1997, 87, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Rigante, L.; Borghei-Razavi, H.; Recinos, P.F.; Roser, F. An Overview of Endoscopy in Neurologic Surgery. CCJM 2019, 86, 16ME–24ME. [Google Scholar] [CrossRef] [PubMed]
- Bukshtab, M. Radiometric and Photometric Quantities and Notions. In Photometry, Radiometry, and Measurements of Optical Losses; Springer Series in Optical Sciences; Springer: Singapore, 2019; Volume 209, pp. 3–47. [Google Scholar] [CrossRef]
- Tomazic, P.V.; Hammer, G.P.; Gerstenberger, C.; Koele, W.; Stammberger, H. Heat Development at Nasal Endoscopes’ Tips: Danger of Tissue Damage? A Laboratory Study. Laryngoscope 2012, 122, 1670–1673. [Google Scholar] [CrossRef] [PubMed]
- de Andrade, E.J.; (Cleveland Clinic, Cleveland, OH, USA). Personal communication, 2022.
- Boese, A.; Wex, C.; Croner, R.; Liehr, U.B.; Wendler, J.J.; Weigt, J.; Walles, T.; Vorwerk, U.; Lohmann, C.H.; Friebe, M.; et al. Endoscopic Imaging Technology Today. Diagnostics 2022, 12, 1262. [Google Scholar] [CrossRef] [PubMed]
- van Det, M.J.; Meijerink, W.J.H.J.; Hoff, C.; Totté, E.R.; Pierie, J.P.E.N. Optimal Ergonomics for Laparoscopic Surgery in Minimally Invasive Surgery Suites: A Review and Guidelines. Surg. Endosc. 2009, 23, 1279–1285. [Google Scholar] [CrossRef] [PubMed]
- CARLTON BALE.COM. Available online: https://carltonbale.com/home-theater/home-theater-calculator/ (accessed on 1 September 2022).
- Riley, C.A.; Soneru, C.P.; Tabaee, A.; Kacker, A.; Anand, V.K.; Schwartz, T.H. Technological and Ideological Innovations in Endoscopic Skull Base Surgery. World Neurosurg. 2019, 124, 513–521. [Google Scholar] [CrossRef]
- Thomas, N.W.D.; Sinclair, J. Image-Guided Neurosurgery: History and Current Clinical Applications. J. Med. Imaging Radiat. Sci. 2015, 46, 331–342. [Google Scholar] [CrossRef]
- Jimenez, D.F.; Son, C.T. Endoscopic Neuronavigation and Image Guidance. In Endoscopic Neurological Surgery; Jaypee Brothers Medical Publishers: New Delhi, India, 2019; pp. 103–112. [Google Scholar]
- Stryker ENT; (Stryker Corporation, Kalamazoo, MI, USA). Personal communication, 2022.
- Mishra, R.; Narayanan, M.D.K.; Umana, G.E.; Montemurro, N.; Chaurasia, B.; Deora, H. Virtual Reality in Neurosurgery: Beyond Neurosurgical Planning. Int. J. Environ. Res. Public Health 2022, 19, 1719. [Google Scholar] [CrossRef]
- Kim, D.H.; Kim, Y.; Park, J.-S.; Kim, S.W. Virtual Reality Simulators for Endoscopic Sinus and Skull Base Surgery: The Present and Future. Clin. Exp. Otorhinolaryngol. 2019, 12, 12–17. [Google Scholar] [CrossRef] [Green Version]
- Zeiger, J.; Costa, A.; Bederson, J.; Shrivastava, R.K.; Iloreta, A.M.C. Use of Mixed Reality Visualization in Endoscopic Endonasal Skull Base Surgery. Oper. Surg. 2020, 19, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Carl, B.; Bopp, M.; Voellger, B.; Saß, B.; Nimsky, C. Augmented Reality in Transsphenoidal Surgery. World Neurosurg. 2019, 125, e873–e883. [Google Scholar] [CrossRef] [PubMed]
- Lai, M.; Skyrman, S.; Shan, C.; Babic, D.; Homan, R.; Edström, E.; Persson, O.; Burström, G.; Elmi-Terander, A.; Hendriks, B.H.W.; et al. Fusion of Augmented Reality Imaging with the Endoscopic View for Endonasal Skull Base Surgery; a Novel Application for Surgical Navigation Based on Intraoperative Cone Beam Computed Tomography and Optical Tracking. PLoS ONE 2020, 15, e0227312. [Google Scholar] [CrossRef] [Green Version]
- James, J.; Irace, A.L.; Gudis, D.A.; Overdevest, J.B. Simulation Training in Endoscopic Skull Base Surgery: A Scoping Review. World J. Otorhinolaryngol. Head Neck Surg. 2022, 8, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Paro, M.R.; Hersh, D.S.; Bulsara, K.R. History of Virtual Reality and Augmented Reality in Neurosurgical Training. World Neurosurg. 2022, 167, 37–43. [Google Scholar] [CrossRef]
- Ashour, R.; Reintjes, S.; Park, M.S.; Sivakanthan, S.; van Loveren, H.; Agazzi, S. Intraoperative Magnetic Resonance Imaging in Skull Base Surgery: A Review of 71 Consecutive Cases. World Neurosurg. 2016, 93, 183–190. [Google Scholar] [CrossRef]
- O’Malley, B.W.; Weinstein, G.S. Robotic Anterior and Midline Skull Base Surgery: Preclinical Investigations. Int. J. Radiat. Oncol. Biol. Phys. 2007, 69 (Suppl. 2), S125–S128. [Google Scholar] [CrossRef]
- Yin Tsang, R.K.; Ho, W.K.; Wei, W.I. Combined Transnasal Endoscopic and Transoral Robotic Resection of Recurrent Nasopharyngeal Carcinoma. Head Neck 2012, 34, 1190–1193. [Google Scholar] [CrossRef]
- Campbell, R.G. Robotic Surgery of the Anterior Skull Base. Int. Forum Allergy Rhinol. 2019, 9, 1508–1514. [Google Scholar] [CrossRef]
- Carrau, R.L.; Prevedello, D.M.; de Lara, D.; Durmus, K.; Ozer, E. Combined Transoral Robotic Surgery and Endoscopic Endonasal Approach for the Resection of Extensive Malignancies of the Skull Base. Head Neck 2013, 35, E351–E358. [Google Scholar] [CrossRef]
- Zappa, F.; Mattavelli, D.; Madoglio, A.; Rampinelli, V.; Ferrari, M.; Tampalini, F.; Fontanella, M.; Nicolai, P.; Doglietto, F.; Agosti, E.; et al. Hybrid Robotics for Endoscopic Skull Base Surgery: Preclinical Evaluation and Surgeon First Impression. World Neurosurg. 2020, 134, e572–e580. [Google Scholar] [CrossRef] [PubMed]
- Dimitrakakis, E.; Aylmore, H.; Lindenroth, L.; Dwyer, G.; Carmichael, J.; Khan, D.Z.; Dorward, N.L.; Marcus, H.J.; Stoyanov, D. Robotic Handle Prototypes for Endoscopic Endonasal Skull Base Surgery: Pre-Clinical Randomised Controlled Trial of Performance and Ergonomics. Ann. Biomed. Eng. 2022, 50, 549–563. [Google Scholar] [CrossRef] [PubMed]
- Pangal, D.J.; Cote, D.J.; Ruzevick, J.; Yarovinsky, B.; Kugener, G.; Wrobel, B.; Ference, E.H.; Swanson, M.; Hung, A.J.; Donoho, D.A.; et al. Robotic and Robot-Assisted Skull Base Neurosurgery: Systematic Review of Current Applications and Future Directions. Neurosurg. Focus 2022, 52, E15. [Google Scholar] [CrossRef]
- Campbell, R.G.; Harvey, R.J. How Close Are We to Anterior Robotic Skull Base Surgery? Curr. Opin. Otolaryngol. Head Neck Surg. 2021, 29, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Bi, W.L.; Dunn, I.F.; Laws, E.R. Image Guidance and Visualization in Pituitary Surgery. In Image-Guided Neurosurgery; Golby, A.J., Ed.; Academic Press: Boston, MA, USA, 2015; Chapter 10; pp. 245–261. [Google Scholar] [CrossRef]
- Lakomkin, N.; Van Gompel, J.J.; Post, K.D.; Cho, S.S.; Lee, J.Y.K.; Hadjipanayis, C.G. Fluorescence Guided Surgery for Pituitary Adenomas. J. Neurooncol. 2021, 151, 403–413. [Google Scholar] [CrossRef] [PubMed]
- Reinhart, M.B.; Huntington, C.R.; Blair, L.J.; Heniford, B.T.; Augenstein, V.A. Indocyanine Green: Historical Context, Current Applications, and Future Considerations. Surg. Innov. 2016, 23, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Jeon, J.W.; Cho, S.S.; Nag, S.; Buch, L.; Pierce, J.; Su, Y.S.; Adappa, N.D.; Palmer, J.N.; Newman, J.G.; Singhal, S.; et al. Near-Infrared Optical Contrast of Skull Base Tumors During Endoscopic Endonasal Surgery. Oper. Surg. 2019, 17, 32–42. [Google Scholar] [CrossRef]
- Hadjipanayis, C.G.; Stummer, W. 5-ALA and FDA Approval for Glioma Surgery. J. Neuro-Oncol. 2019, 141, 479–486. [Google Scholar] [CrossRef]
- Micko, A.; Rapoport, B.I.; Youngerman, B.E.; Fong, R.P.; Kosty, J.; Brunswick, A.; Shahrestani, S.; Zada, G.; Schwartz, T.H. Limited Utility of 5-ALA Optical Fluorescence in Endoscopic Endonasal Skull Base Surgery: A Multicenter Retrospective Study. J. Neurosurg. 2020, 135, 535–541. [Google Scholar] [CrossRef]
- Recinos, P.F. Editorial. Is the Use of 5-ALA in Endoscopic Skull Base Surgery Truly Limited or in Need of More Refined Evaluation? J. Neurosurg. 2020, 135, 532–533. [Google Scholar] [CrossRef]
- Predina, J.D.; Newton, A.D.; Connolly, C.; Dunbar, A.; Baldassari, M.; Deshpande, C.; Cantu, E.; Stadanlick, J.; Kularatne, S.A.; Low, P.S.; et al. Identification of a Folate Receptor-Targeted Near-Infrared Molecular Contrast Agent to Localize Pulmonary Adenocarcinomas. Mol. Ther. J. Am. Soc. Gene Ther. 2018, 26, 390–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, S.S.; Jeon, J.; Buch, L.; Nag, S.; Nasrallah, M.; Low, P.S.; Grady, M.S.; Singhal, S.; Lee, J.Y.K. Intraoperative Near-Infrared Imaging with Receptor-Specific versus Passive Delivery of Fluorescent Agents in Pituitary Adenomas. J. Neurosurg. 2018, 131, 1974–1984. [Google Scholar] [CrossRef] [Green Version]
- Zhang, D.Y.; Singhal, S.; Lee, J.Y.K. Optical Principles of Fluorescence-Guided Brain Tumor Surgery: A Practical Primer for the Neurosurgeon. Neurosurgery 2019, 85, 312–324. [Google Scholar] [CrossRef] [PubMed]
- Morris, A.E.; Adamson, R.; Frank, J. Ultrasonography: Principles and Basic Thoracic and Vascular Imaging. In Murray & Nadel’s Textbook of Respiratory Medicine; Elsevier: Amsterdam, The Netherlands, 2022; pp. 330–342. [Google Scholar]
- Machado, I.; Toews, M.; Luo, J.; Unadkat, P.; Essayed, W.; George, E.; Teodoro, P.; Carvalho, H.; Martins, J.; Golland, P.; et al. Non-Rigid Registration of 3D Ultrasound for Neurosurgery Using Automatic Feature Detection and Matching. Int. J. Comput. Assist. Radiol. Surg. 2018, 13, 1525–1538. [Google Scholar] [CrossRef] [PubMed]
- Alshareef, M.; Lowe, S.; Park, Y.; Frankel, B. Utility of Intraoperative Ultrasonography for Resection of Pituitary Adenomas: A Comparative Retrospective Study. Acta Neurochir. 2021, 163, 1725–1734. [Google Scholar] [CrossRef] [PubMed]
- AlQahtani, A.; Castelnuovo, P.; Nicolai, P.; Prevedello, D.M.; Locatelli, D.; Carrau, R.L. Injury of the Internal Carotid Artery During Endoscopic Skull Base Surgery. Otolaryngol. Clin. N. Am. 2016, 49, 237–252. [Google Scholar] [CrossRef]
- Prada, F.; Bene, M.D.; Casali, C.; Saladino, A.; Legnani, F.G.; Perin, A.; Moiraghi, A.; Richetta, C.; Rampini, A.; Mattei, L.; et al. Intraoperative Navigated Angiosonography for Skull Base Tumor Surgery. World Neurosurg. 2015, 84, 1699–1707. [Google Scholar] [CrossRef]
- Fujifilm Healthcare Americas Corp.; (Fujifilm Corp., Tokyo, Japan). Personal communication, 2022.
- Mikla, V.I.; Mikla, V.V. Medical Imaging Technology, 1st ed.; Elsevier: Amsterdam, The Netherlands, 2013. [Google Scholar] [CrossRef]
- Sylvester, P.T.; Evans, J.A.; Zipfel, G.J.; Chole, R.A.; Uppaluri, R.; Haughey, B.H.; Getz, A.E.; Silverstein, J.; Rich, K.M.; Kim, A.H.; et al. Combined High-Field Intraoperative Magnetic Resonance Imaging and Endoscopy Increase Extent of Resection and Progression-Free Survival for Pituitary Adenomas. Pituitary 2015, 18, 72–85. [Google Scholar] [CrossRef] [Green Version]
- Tomà, P.; Bartoloni, A.; Salerno, S.; Granata, C.; Cannatà, V.; Magistrelli, A.; Arthurs, O.J. Protecting Sensitive Patient Groups from Imaging Using Ionizing Radiation: Effects during Pregnancy, in Fetal Life and Childhood. Radiol. Med. 2019, 124, 736–744. [Google Scholar] [CrossRef]
- Zaidi, H.A.; De Los Reyes, K.; Barkhoudarian, G.; Litvack, Z.N.; Bi, W.L.; Rincon-Torroella, J.; Mukundan, S.; Dunn, I.F.; Laws, E.R. The Utility of High-Resolution Intraoperative MRI in Endoscopic Transsphenoidal Surgery for Pituitary Macroadenomas: Early Experience in the Advanced Multimodality Image Guided Operating Suite. FOC 2016, 40, E18. [Google Scholar] [CrossRef] [Green Version]
- Almeida, J.P.; de Andrade, E.; Reghin-Neto, M.; Radovanovic, I.; Recinos, P.F.; Kshettry, V.R. From above and below: The Microsurgical Anatomy of Endoscopic Endonasal and Transcranial Microsurgical Approaches to the Parasellar Region. World Neurosurg. 2022, 159, e139–e160. [Google Scholar] [CrossRef] [PubMed]
- Almeida, J.P.; Kalyvas, A.; Mohan, N.; Oswari, S.; Takami, H.; Velasquez, C.; Asha, M.; Zadeh, G.; Gentili, F. Current Results of Surgical Treatment of Craniopharyngiomas: The Impact of Endoscopic Endonasal Approaches. World Neurosurg. 2020, 142, 582–592. [Google Scholar] [CrossRef] [PubMed]
- Marigil, M.; Almeida, J.P.; Karekezi, C.; de Almeida, J.R.; Gentili, F. Expanded Endoscopic Endonasal Approach for Resection of Intradural Chordoma: Surgical and Anatomic Nuances: 2-Dimensional Operative Video. Oper. Neurosurg. 2019, 17, E66. [Google Scholar] [CrossRef] [PubMed]
- Almeida, J.P.; De Andrade, E.J.; Vescan, A.; Zadeh, G.; Recinos, P.F.; Kshettry, V.R.; Gentili, F. Surgical Anatomy and Technical Nuances of the Endoscopic Endonasal Approach to the Anterior Cranial Fossa. J. Neurosurg. Sci. 2021, 65, 103–117. [Google Scholar] [CrossRef] [PubMed]
- Scibilia, A.; Cebula, H.; Esposito, F.; Angileri, F.F.; Raffa, G.; Todeschi, J.; Koch, G.; Clavert, P.; Debry, C.; Germanò, A.; et al. Endoscopic Endonasal Approach to the Ventral-Medial Portion of Posterior Paramedian Skull Base: A Morphometric Perspective of Surgical and Radiologic Anatomy. World Neurosurg. 2021, 149, e687–e695. [Google Scholar] [CrossRef]
- Chibbaro, S.; Ganau, M.; Scibilia, A.; Todeschi, J.; Zaed, I.; Bozzi, M.T.; Ollivier, I.; Cebula, H.; des Neiges Santin, M.; Djennaoui, I.; et al. Endoscopic Transorbital Approaches to Anterior and Middle Cranial Fossa: Exploring the Potentialities of a Modified Lateral Retrocanthal Approach. World Neurosurg. 2021, 150, e74–e80. [Google Scholar] [CrossRef]
- Nannavecchia, B.A.; Ganau, M.; Cebula, H.; Scibilia, A.; Bozzi, M.T.; Zaed, I.; Gallinaro, P.; Boujan, F.; Dietemann, J.-L.; Djennaoui, I.; et al. Endoscopic Transorbital Approaches to Anterior and Middle Cranial Fossa: A Laboratory Investigation on Surgical Anatomy and Potential Routes. J. Neurol. Surg. B Skull Base 2021, 82, 443–449. [Google Scholar] [CrossRef]
- Almeida, J.P.; Sreenath, S.B.; de Andrade, E.J.; Recinos, P.F.; Woodard, T.D.; Kshettry, V.R. Endoscopic Transpterygoid Transcavernous Approach for Resection of a Petroclival Chondrosarcoma: 2-Dimensional Operative Video. Oper. Neurosurg. 2022, 23, e60–e61. [Google Scholar] [CrossRef]
- Silveira-Bertazzo, G.; Manjila, S.; London, N.R.; Prevedello, D.M. Techniques and Challenges of the Expanded Endoscopic Endonasal Access to the Ventrolateral Skull Base during the “Far-Medial” and “Extreme Medial” Approaches. Acta Neurochir. 2020, 162, 597–603. [Google Scholar] [CrossRef]
- Rastatter, J.C.; Snyderman, C.H.; Gardner, P.A.; Alden, T.D.; Tyler-Kabara, E. Endoscopic Endonasal Surgery for Sinonasal and Skull Base Lesions in the Pediatric Population. Otolaryngol. Clin. N. Am. 2015, 48, 79–99. [Google Scholar] [CrossRef]
- Mamelak, A.N.; Danielpour, M.; Black, K.L.; Hagike, M.; Berci, G. A High-Definition Exoscope System for Neurosurgery and Other Microsurgical Disciplines: Preliminary Report. Surg. Innov. 2008, 15, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Montemurro, N.; Scerrati, A.; Ricciardi, L.; Trevisi, G. The Exoscope in Neurosurgery: An Overview of the Current Literature of Intraoperative Use in Brain and Spine Surgery. J. Clin. Med. 2021, 11, 223. [Google Scholar] [CrossRef] [PubMed]
- Langer, D.J.; White, T.G.; Schulder, M.; Boockvar, J.A.; Labib, M.; Lawton, M.T. Advances in Intraoperative Optics: A Brief Review of Current Exoscope Platforms. Oper. Neurosurg. 2020, 19, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Murai, Y.; Shirokane, K.; Sato, S.; Higuchi, T.; Kubota, A.; Ozeki, T.; Matano, F.; Sasakai, K.; Yamaguchi, F.; Morita, A. Preliminary Clinical Surgical Experience with Temporary Simultaneous Use of an Endoscope during Exoscopic Neurosurgery: An Observational Study. JCM 2022, 11, 1753. [Google Scholar] [CrossRef] [PubMed]
- Iwami, K.; Watanabe, T.; Osuka, K.; Ogawa, T.; Miyachi, S.; Fujimoto, Y. Combined Exoscopic and Endoscopic Technique for Craniofacial Resection. Curr. Oncol. 2021, 28, 3945–3958. [Google Scholar] [CrossRef] [PubMed]
- Isaacson, B.; Killeen, D.E.; Bianconi, L.; Marchioni, D. Endoscopic Assisted Lateral Skull Base Surgery. Otolaryngol. Clin. N. Am. 2021, 54, 163–173. [Google Scholar] [CrossRef]
- Dijkstra, B.M.; Jeltema, H.-R.; Kruijff, S.; Groen, R.J.M. The Application of Fluorescence Techniques in Meningioma Surgery—A Review. Neurosurg. Rev. 2019, 42, 799–809. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.Y.K.; Cho, S.S.; Zeh, R.; Pierce, J.T.; Martinez-Lage, M.; Adappa, N.D.; Palmer, J.N.; Newman, J.G.; Learned, K.O.; White, C.; et al. Folate Receptor Overexpression Can Be Visualized in Real Time during Pituitary Adenoma Endoscopic Transsphenoidal Surgery with Near-Infrared Imaging. J. Neurosurg. 2018, 129, 390–403. [Google Scholar] [CrossRef] [Green Version]
- Sarris, C.E.; Santarelli, G.; Almefty, K.K.; Little, A.S. A Teaching Atlas of the Ultrasound Anatomy of The Skull Base: Implications for Future Applications of Intraoperative Ultrasound in Endoscopic Endonasal Skull Base Surgery. J. Neurol. Surg. B Skull Base 2022, 83, S1–S270. [Google Scholar] [CrossRef]
- Sekhar, L.N.; Juric-Sekhar, G.; Qazi, Z.; Patel, A.; McGrath, L.B.; Pridgeon, J.; Kalavakonda, N.; Hannaford, B. The Future of Skull Base Surgery: A View through Tinted Glasses. World Neurosurg. 2020, 142, 29–42. [Google Scholar] [CrossRef]
- Jakubovic, R.; Guha, D.; Gupta, S.; Lu, M.; Jivraj, J.; Standish, B.A.; Leung, M.K.; Mariampillai, A.; Lee, K.; Siegler, P.; et al. High Speed, High Density Intraoperative 3D Optical Topographical Imaging with Efficient Registration to MRI and CT for Craniospinal Surgical Navigation. Sci. Rep. 2018, 8, 14894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchioni, D.; Bisi, N.; Molteni, G.; Rubini, A. Exoscopic Surgery of Lateral Skull Base. In Exoscope-Assisted Surgery in Otorhinolaryngology; Elsevier: Amsterdam, The Netherland, 2022; pp. 77–96. [Google Scholar] [CrossRef]









Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jarmula, J.; de Andrade, E.J.; Kshettry, V.R.; Recinos, P.F. The Current State of Visualization Techniques in Endoscopic Skull Base Surgery. Brain Sci. 2022, 12, 1337. https://doi.org/10.3390/brainsci12101337
Jarmula J, de Andrade EJ, Kshettry VR, Recinos PF. The Current State of Visualization Techniques in Endoscopic Skull Base Surgery. Brain Sciences. 2022; 12(10):1337. https://doi.org/10.3390/brainsci12101337
Chicago/Turabian StyleJarmula, Jakub, Erion Junior de Andrade, Varun R. Kshettry, and Pablo F. Recinos. 2022. "The Current State of Visualization Techniques in Endoscopic Skull Base Surgery" Brain Sciences 12, no. 10: 1337. https://doi.org/10.3390/brainsci12101337