
Can Incobotulinumtoxin-A Treatment Improve Quality of Life Better Than Conventional Therapy in Spastic Muscle Post-Stroke Patients? Results from a Pilot Study from a Single Center



Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Issues
2.2. Participants
2.3. Methodology
2.3.1. Measures
2.3.2. 15D-Instrument
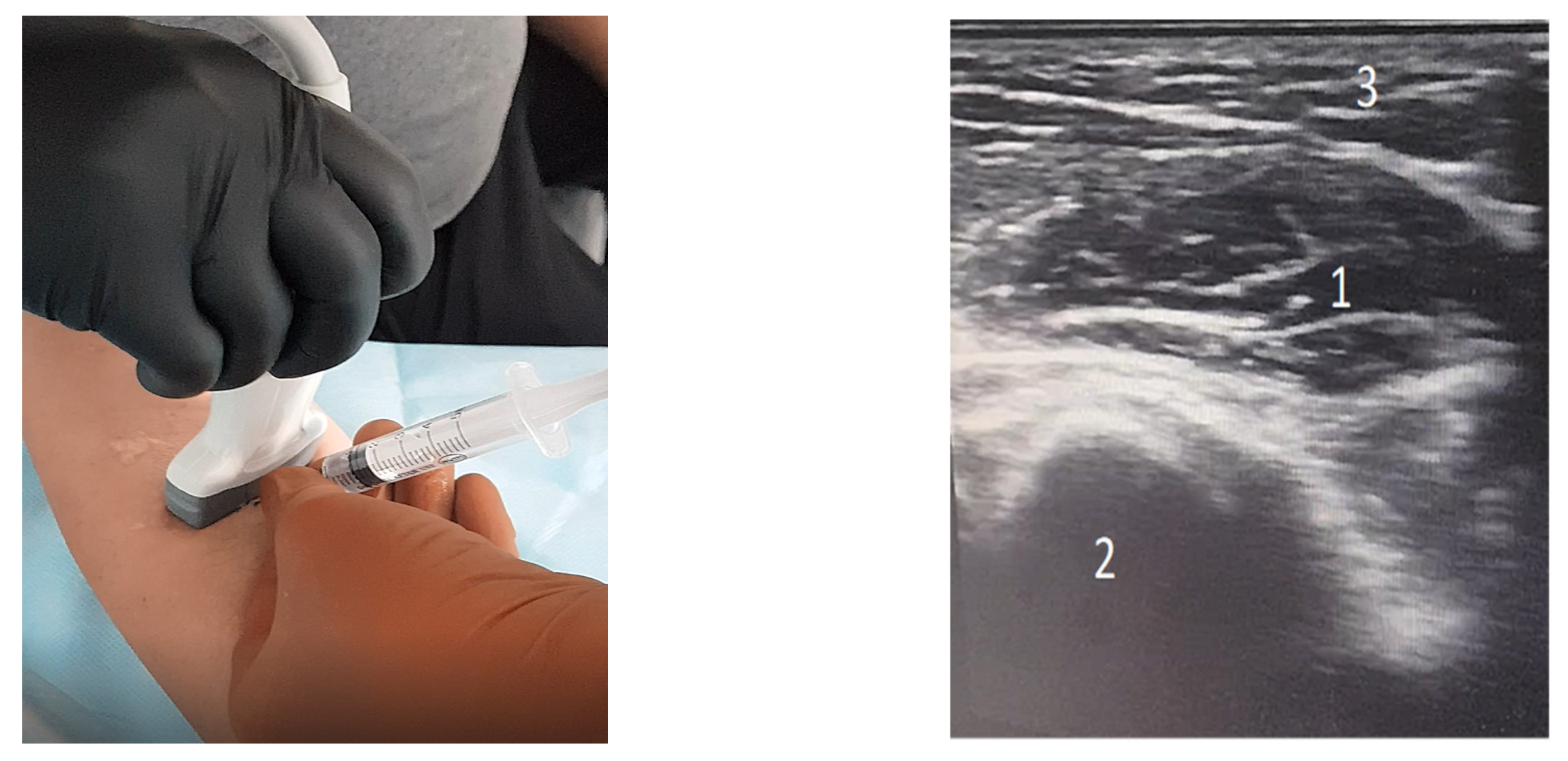
2.4. Treatment
2.5. Statistical Analysis
3. Results
3.1. Health Characteristics
3.2. Baseline and Post-Treatment Changes in 15D Scores
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ramos-Lima, M.J.M.; de Carvalho Brasileiro, I.; de Lima, T.L.; Braga-Neto, P. Quality of life after stroke: Impact of clinical and sociodemographic factors. Clinics 2018, 73, e418. [Google Scholar] [CrossRef]
- Parikh, S.; Parekh, S.; Vaghela, N. Impact of stroke on quality of life and functional independence. Natl. J. Physiol. Pharm. Pharmacol. 2018, 8, 1595–1598. [Google Scholar] [CrossRef]
- Neagoe, M.A. Accidentele vasculare cerebrale—Problemă de sănătate publică. Acta Med. Transilv. 2013, 2, 17–20. [Google Scholar]
- Bajenaru, O. Ghid de Diagnostic şi Tratament Pentru Bolile Cerebrovasculare. Available online: https://www.cardioiliescu.ro/doc/ghid%201_8292_5994.pdf (accessed on 4 May 2021).
- Schinwelski, M.; Sławek, J. Prevalence of spasticity following stroke and its impact on quality of life with emphasis on disability in activities of daily living. Systematic review. Neurol. Neurochir. Pol. 2010, 44, 404–411. [Google Scholar] [CrossRef] [Green Version]
- Pandey, K.; Spasticity Treatment & Management. Drugs & Diseases Neurology. 2019. Available online: https://emedicine.medscape.com/article/2207448-treatment (accessed on 4 May 2021).
- Baricich, A.; Santamato, A.; Picelli, A.; Morone, G.; Smania, N.; Paolucci, S.; Fiore, P. Spasticity Treatment During COVID-19 Pandemic: Clinical Recommendations. Front. Neurol. 2020, 11, 719. [Google Scholar] [CrossRef]
- Kandasamy, M. Perspectives for the use of therapeutic Botulinum toxin as a multifaceted candidate drug to attenuate COVID-19. Med. Drug Discov. 2020, 6, 100042. [Google Scholar] [CrossRef]
- Turcu-Stiolica, A.; Subtirelu, M.S. Cost-effectiveness of treating Romanian post-stroke patients with upper limb spasticity with incobotulinum-A against conventional therapy. Value Health 2018, 21, S206–S207. [Google Scholar] [CrossRef]
- Strilciuc, S.; Grad, D.; Mixich, V.; Stan, A.; Buzoianu, A.D.; Vladescu, C.; Virtan, M.A. Soci-etal cost of ischemic stroke in Romania: Results from a retrospective county-level study. Brain Sci. 2021, 11, 689. [Google Scholar] [CrossRef]
- Lorenzovici, L.; Székely, A.; Csanádi, M.; Gaál, P. Cost Assessment of Inpatient Care Episodes of Stroke in Romania. Front. Public Health 2020, 8, 605919. [Google Scholar] [CrossRef]
- Turcu-Stiolica, A.; Subtirelu, M.-S.; Bumbea, A.M. Cost-utility analysis of incobotulinumtoxin-A compared with conventional therapy in the management of post-stroke spasticity in Romania. Front. Pharmacol. 2020, 10, 1516. [Google Scholar] [CrossRef] [Green Version]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [Green Version]
- Bohannon, R.W.; Smith, M.B. Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys. Ther. 1987, 67, 206–207. [Google Scholar] [CrossRef]
- Rehabilitation Measures Databases. Available online: https://www.sralab.org/rehabilitation-measures/tardieu-scalemodified-tardieu-scale#:~:text=Tardieu%20is%20a%20scale%20for,Haugh%20and%20Pandyan%2C%202006 (accessed on 4 June 2021).
- Gracies, J.M. Coefficients of impairment in deforming spastic paresis. Ann. Phys. Rehabil. Med. 2015, 58, 173–178. [Google Scholar] [CrossRef] [Green Version]
- Barthel Index for Activities of Daily Living (ADL). Available online: https://www.mdcalc.com/barthel-index-activities-daily-living-adl (accessed on 4 June 2021).
- Muscle Strength Testing. Available online: https://www.physio-pedia.com/Muscle_Strength_Testing (accessed on 4 June 2021).
- Mini-Mental State Examination (MMSE). Available online: http://www.fammed.usouthal.edu/Guides&JobAids/Geriatric/MMSE.pdf (accessed on 4 June 2021).
- Subtirelu, M.S.; Turcu-Stiolica, A.; Sintonen, H. Translation and cultural adaptation of 15D quality of life questionnaire from English to Romanian language. Value Health 2019, 22, S731. [Google Scholar] [CrossRef]
- Dressler, D.; Rychlik, R.; Kreimendahl, F.; Schnur, N.; Lambert-Baumann, J. Long-term efficacy and safety of incobotulinumtoxinA and conventional treatment of poststroke arm spasticity: A prospective, noninterventional, open-label, parallel-group study. BMJ Open 2015, 5, e009358. [Google Scholar] [CrossRef]
- Rychlik, R.; Kreimendahl, F.; Schnur, N.; Lambert-Baumann, J.; Dressler, D. Quality of life and costs of spasticity treatment in German stroke patients. Health Econ. Rev. 2016, 6, 27. [Google Scholar] [CrossRef] [Green Version]
- Barnes, M.; Kocer, S.; Murie Fernandez, M.; Balcaitiene, J.; Fheodoroff, K. An international survey of patients living with spasticity. Disabil. Rehabil. 2017, 39, 1428–1434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turner-Stokes, L.; Fheodoroff, K.; Jacinto, J.; Maisonobe, P.; Ashford, S. ULIS (Upper Limb International Spasticity), a 10-year Odyssey: An international, multicentric, longitudinal cohort of person-centered spasticity management in real-life practice. J. Int. Soc. Phys. Rehabil. Med. 2019, 2, 138–150. [Google Scholar] [CrossRef]
- Turner-Stokes, L.; Fheodoroff, K.; Jacinto, J.; Maisonobe, P. Results from the Upper Limb International Spasticity Study-II (ULIS-II): A large, international, prospective cohort study investigating practice and goal attainment following treatment with botulinum toxin A in real-life clinical management. BMJ Open 2013, 3, e002771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohammadi, B.; Abdoulrahmani Balouch, S.; Dengler, R.; Kollewe, K. Long-term treatment of spasticity with botulinum toxin type A: An analysis of 1221 treatments in 137 patients. Neurol. Res. 2010, 32, 309–313. [Google Scholar] [CrossRef]
- Masakado, Y.; Abo, M.; Kondo, K.; Saeki, S.; Saitoh, E.; Dekundy, A.; Hanschmann, A.; Kaji, R.; J-PURE Study Group. Efficacy and safety of incobotulinumtoxinA in post-stroke upper-limb spasticity in Japanese subjects: Results from a randomized, double-blind, placebo-controlled study (J-PURE). J. Neurol. 2020, 267, 2029–2041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marciniak, C.; Munin, M.C.; Brashear, A.; Rubin, B.S.; Patel, A.T.; Slawek, J.; Hanschmann, A.; Hiersemenzel, R.; Elovic, E.P. IncobotulinumtoxinA Efficacy and Safety in Adults with Upper-Limb Spasticity Following Stroke: Results from the Open-Label Extension Period of a Phase 3 Study. Adv. Ther. 2019, 36, 187–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaňovský, P.; Slawek, J.; Denes, Z.; Platz, T.; Comes, G.; Grafe, S.; Pulte, I. Efficacy and safety of treatment with incobotulinum toxin A (botulinum neurotoxin type A free from complexing proteins; NT 201) in post-stroke upper limb spasticity. J. Rehabil. Med. 2011, 43, 486–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levy, J.; Molteni, F.; Cannaviello, G.; Lansaman, T.; Roche, N.; Bensmail, D. Does botulinum toxin treatment improve upper limb active function? Ann. Phys. Rehabil. Med. 2019, 62, 234–240. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Patient Group | p-Value | |||
|---|---|---|---|---|---|
| BOT (N = 17) | CON (N = 17) | ||||
| Count | Mean (±SD) | Count | Mean (±SD) | ||
| Age, years | 59.53 (±8.94) | 60.91 (±12.86) | 0.002 * | ||
| Gender | 1.00 | ||||
| Men (n = 21) | 9 (52.9%) | 8 (47.1%) | |||
| Women (n = 13) | 8 (47.1%) | 9 (52.9%) | |||
| Married (yes) | 17 (100%) | 17 (100%) | 1.00 | ||
| Employment status | 1.00 | ||||
| Retired | 17 (100%) | 17 (100%) | |||
| Environmental | 0.494 | ||||
| Rural | 10 (58.8%) | 7 (41.2%) | |||
| Urban | 7 (41.2%) | 10 (58.8%) | |||
| Education | 0.001 | ||||
| Faculty | 1 (5.9%) | ||||
| Highschool | 17 (100%) | 7 (41.2%) | |||
| Elementary school | 9 (52.9%) | ||||
| Patient Group | |||||
|---|---|---|---|---|---|
| BOT (N = 17) | CON (N = 17) | ||||
| Count | Mean (±SD) | Count | Mean (±SD) | p-Value | |
| Type | 0.175 | ||||
| Ischaemic | 12 (70.6%) | 16 (99.94%) | |||
| Hemorrhagic | 5 (29.4%) | 1 (0.06%) | |||
| Hypertension (yes) | 16 (94.1%) | 17 (100%) | 0.310 | ||
| Diabetes (yes) | 2 (11.8%) | 9 (52.9%) | 0.026 | ||
| Ischemic heart disease (yes) | 14 (82.4%) | 17 (100%) | 0.227 | ||
| Jacksonism (yes) | 4 (23.5%) | 3 (11.8%) | 1.000 | ||
| Haemipareshis (right) | 10 (58.8%) | 5 (29.4%) | 0.166 | ||
| Ashworth_T0 | 0.001 | ||||
| 1 | 0 | 2 (11.8%) | |||
| 2 | 1 (5.9%) | 11 (64.7%) | |||
| 3 | 10 (58.8%) | 3 (17.6%) | |||
| 3/4 | 6 (35.3%) | 1 (5.9%) | |||
| Ashworth_T1 | 0.198 | ||||
| 1 | 4 (23.5%) | 2 (11.8%) | |||
| 2 | 8 (47.1%) | 9 (52.9%) | |||
| 2/3 | 3 (17.7%) | 0 | |||
| 3 | 2 (11.8%) | 5 (29.4%) | |||
| 4 | 0 | 1 (5.9%) | |||
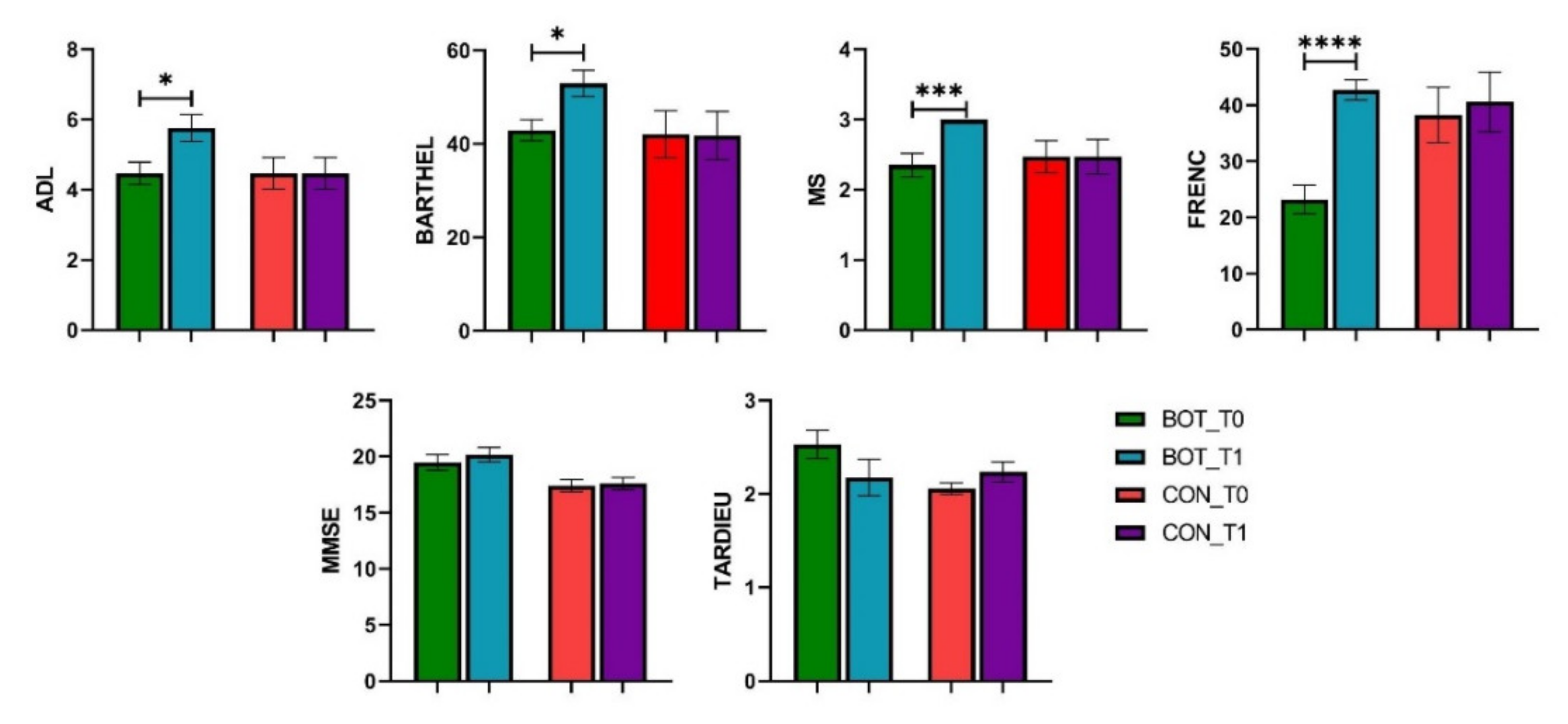
| ADL_T0 | 4.47 (±1.33) | 4.47 (±1.58) | 0.413 | ||
| ADL_T1 | 5.76 (±1.56) | 5.12 (±1.81) | 0.099 | ||
| Barthel_T0 | 42.94 (±9.36) | 42.50 (±15.82) | 0.786 | ||
| Barthel_T1 | 52.94 (±11.6) | 47.35 (±17.81) | 0.092 | ||
| MS_T0 | 2.35 (±0.70) | 2.41 (±0.82) | 0.563 | ||
| MS_T1 | 3.00 (±0.00) | 2.74 (±0.75) | 0.150 | ||
| MMSE_T0 | 19.47 (±2.85) | 18.44 (±2.72) | 0.041 * | ||
| MMSE_T1 | 20.18 (±2.68) | 18.88 (±2.77) | 0.008 * | ||
| Tardieu_T0 | 2.53 (±0.62) | 2.29 (±0.52) | 0.038 * | ||
| Tardieu_T1 | 2.18 (±0.81) | 2.21 (±0.64) | 0.76 | ||
| FRENC_T0 | 23.18 (±10.45) | 30.71 (±17.69) | 0.031 * | ||
| FRENC_T1 | 42.71 (±7.53) | 41.65 (±16.18) | 0.540 | ||
| Dimensions | BOT (Mean ± SD) | CON (Mean ± SD) | p-Value for T0 | p-Value for Difference between Scores | ||||
|---|---|---|---|---|---|---|---|---|
| T0 | T1 | Difference between Scores | T0 | T1 | Difference between Scores | |||
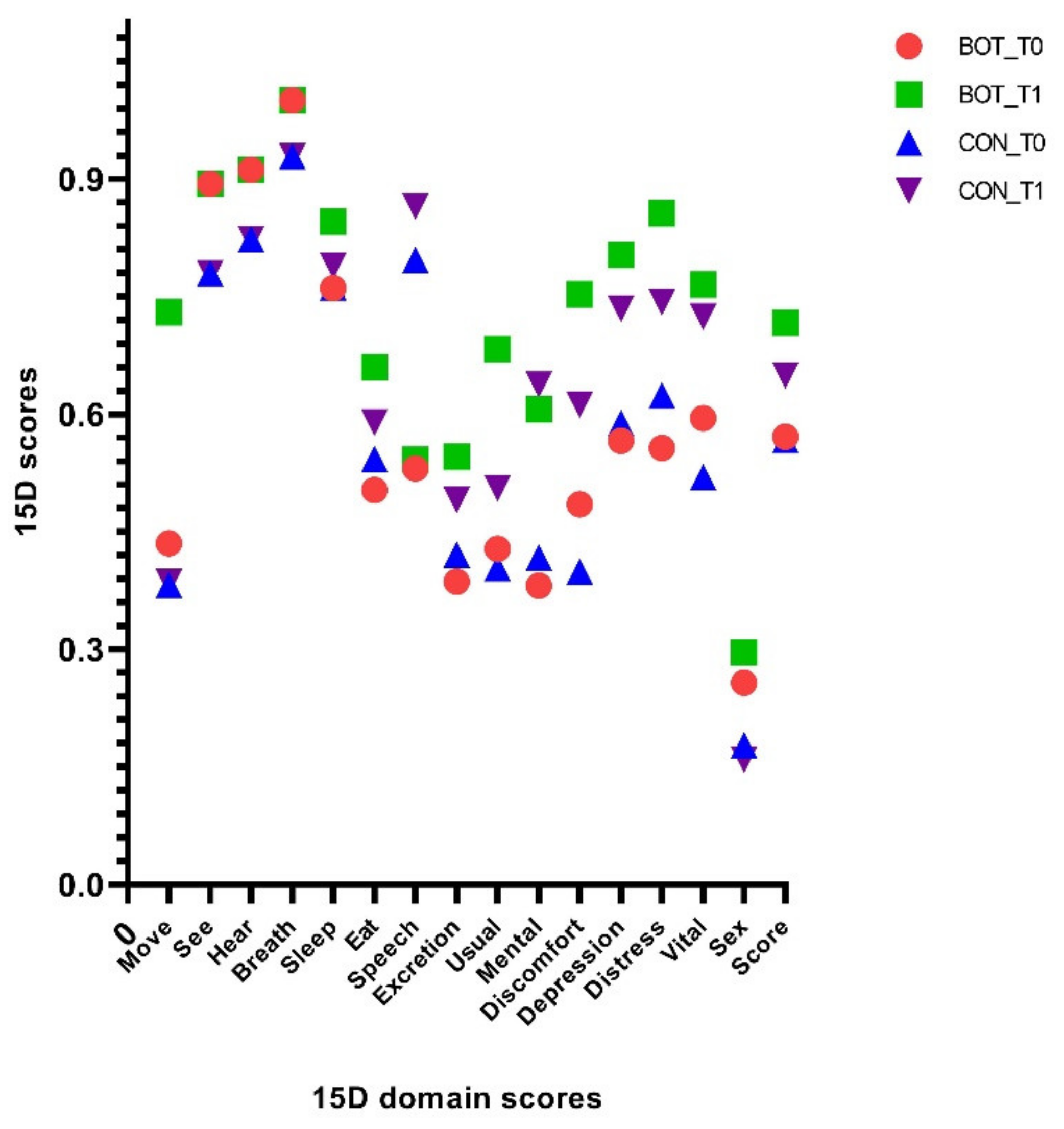
| Move | 0.44(±0.12) | 0.69(±0.12) | 0.09(±0.13) | 0.41(±0.12) | 0.54(±0.21) | 0.13(±0.16) | 0.306 | <0.001 * |
| See | 0.89(±0.15) | 0.89(±0.15) | 0 | 0.84(±0.13) | 0.84(±0.13) | 0 | 0.012 * | 1.000 |
| Hear | 0.91(±0.12) | 0.91(±0.12) | 0 | 0.87(±0.13) | 0.87(±0.13) | 0 | 0.079 | 1.000 |
| Breath | 1 | 1 | 0 | 0.96(±0.09) | 0.96(±0.09) | 0 | 0.245 | 1.000 |
| Sleep | 0.76(±0.09) | 0.85(±0.12) | 0.06(±0.11) | 0.76(±0.06) | 0.82(±0.12) | 0.06(±0.12) | 1.000 | 0.274 |
| Eat | 0.50(±0.16) | 0.66(±0.24) | 0.12(±0.17) | 0.52(±0.14) | 0.62(±0.20) | 0.10(±0.15) | 0.586 | 0.053 |
| Speech | 0.53(±0.29) | 0.54(±0.28) | 0.02(±0.07) | 0.66(±0.29) | 0.70(±0.29) | 0.04(±0.09) | 0.009 * | 0.357 |
| Excretion | 0.39(±0.19) | 0.55(±0.23) | 0.11(±0.16) | 0.40(±0.17) | 0.52(±0.22) | 0.11(±0.14) | 0.496 | 0.140 |
| Usual Activities | 0.43(±0.19) | 0.68(±0.15) | 0.10(±0.14) | 0.42(±0.17) | 0.59(±0.19) | 0.18(±0.16) | 0.865 | 0.018 * |
| Mental Function | 0.38(±0.15) | 0.61(±0.25) | 0.19(±0.15) | 0.39(±0.14) | 0.62(±0.21) | 0.22(±0.11) | 0.496 | 0.838 |
| Discomfort | 0.48(±0.22) | 0.75(±0.24) | 0.25(±0.12) | 0.44(±0.19) | 0.68(±0.21) | 0.24(±0.16) | 0.357 | 0.540 |
| Depression | 0.57(±0.17) | 0.75(±0.20) | 0.16(±0.12) | 0.58(±0.14) | 0.74(±0.16) | 0.16(±0.12) | 0.760 | 0.760 |
| Distress | 0.56(±0.18) | 0.86(±0.17) | 0.11(±0.14) | 0.59(±0.16) | 0.79(±0.15) | 0.21(±0.14) | 0.357 | <0.001 * |
| Vitality | 0.59(±0.17) | 0.77(±0.21) | 0.14(±0.15) | 0.56(±0.15) | 0.74(±0.17) | 0.19(±0.12) | 0.205 | 0.122 |
| Sexual Activity | 0.26(±0.13) | 0.29(±0.18) | 0.00(±0.15) | 0.22(±0.12) | 0.23(±0.15) | 0.01(±0.09) | 0.085 | 0.193 |
| Total 15D score | 0.57(±0.12) | 0.72(±0.14) | 0.13(±0.05) | 0.57(±0.09) | 0.68(±0.12) | 0.11(±0.05) | 0.838 | <0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Turcu-Stiolica, A.; Subtirelu, M.-S.; Bumbea, A.-M. Can Incobotulinumtoxin-A Treatment Improve Quality of Life Better Than Conventional Therapy in Spastic Muscle Post-Stroke Patients? Results from a Pilot Study from a Single Center. Brain Sci. 2021, 11, 934. https://doi.org/10.3390/brainsci11070934
Turcu-Stiolica A, Subtirelu M-S, Bumbea A-M. Can Incobotulinumtoxin-A Treatment Improve Quality of Life Better Than Conventional Therapy in Spastic Muscle Post-Stroke Patients? Results from a Pilot Study from a Single Center. Brain Sciences. 2021; 11(7):934. https://doi.org/10.3390/brainsci11070934
Chicago/Turabian StyleTurcu-Stiolica, Adina, Mihaela-Simona Subtirelu, and Ana-Maria Bumbea. 2021. "Can Incobotulinumtoxin-A Treatment Improve Quality of Life Better Than Conventional Therapy in Spastic Muscle Post-Stroke Patients? Results from a Pilot Study from a Single Center" Brain Sciences 11, no. 7: 934. https://doi.org/10.3390/brainsci11070934