
Microsurgical Anatomy of the Inferomedial Paraclival Triangle: Contents, Topographical Relationships and Anatomical Variations

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
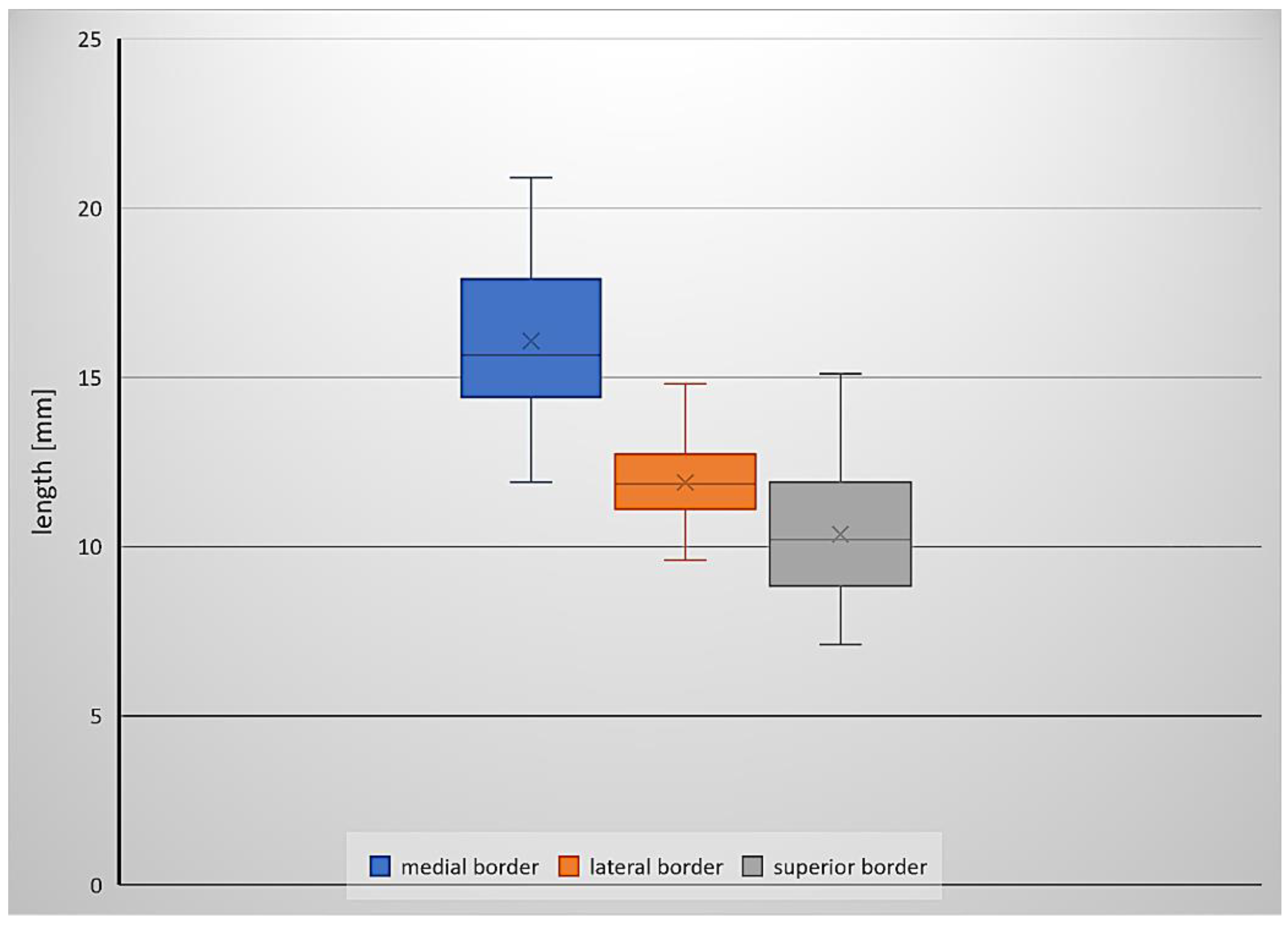
3.1. Inferomedial Triangle Measurements and Area
3.2. Topography and Anatomical Variations within the Inferomedial Triangle
3.3. Histological Examination
4. Discussion
Study Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dolenc, V.V. Microsurgical Anatomy and Surgery of the Central Skull Base; Springer: Wien, Austria, 2003; pp. 29–31. [Google Scholar]
- Rhoton, A.L., Jr. The Cavernous Sinus, the Cavernous Venous Plexus, and the Carotid Collar. Neurosurgery 2002, 51, S1-375–S1-410. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, A.; Nagaseki, Y.; Ohkubo, S.; Ohhashi, Y.; Horikoshi, T.; Nishigaya, K.; Nukui, H. Anatomical variations of the ten triangles around the cavernous sinus. Clin. Anat. 2003, 16, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Isolan, G.R.; Krayenbühl, N.; de Oliveira, E.; Al-Mefty, O. Microsurgical Anatomy of the Cavernous Sinus: Measurements of the Triangles in and around It. Skull Base 2007, 17, 357–367. [Google Scholar] [CrossRef] [Green Version]
- Isolan, G.R.; Souza Braga, F.L.; Campero, A.; Landeiro, J.A.; de Araújo, R.M.L.; Adjer, P.; Sakaya, G.R.; Rabelo, N.N.; da Silva Brito, J.; Teixeira, M.J.; et al. Microsurgical and Endoscopic Anatomy of the Cavernous Sinus. Arq. Bras. Neurocir. Braz. Neurosurg. 2020, 39, 83–94. [Google Scholar] [CrossRef] [Green Version]
- Drazin, D.; Wang, J.M.; Alonso, F.; Patel, D.M.; Granger, A.; Shoja, M.M.; Loukas, M.; Oskouian, R.J.; Tubbs, R.S. Intracranial Anatomical Triangles: A Comprehensive Illustrated Review. Cureus 2017, 9, e1741. [Google Scholar] [CrossRef] [Green Version]
- Dalgiç, A.; Boyaci, S.; Aksoy, K. Anatomical study of the cavernous sinus emphasizing operative approaches. Turk. Neurosurg. 2010, 20, 186–204. [Google Scholar] [CrossRef] [Green Version]
- Destrieux, C.; Velut, S.; Kakou, M.K.; Lefrancq, T.; Arbeille, B.; Santini, J.J. A new concept in Dorello’s canal microanatomy: The petroclival venous confluence. J. Neurosurg. 1997, 87, 67–72. [Google Scholar] [CrossRef]
- Kimball, H.; Kimball, D.; Blihar, D.; Zurada, A.; Tubbs, R.S.; Loukas, M. The Inferolateral Surgical Triangle of the Cavernous Sinus: A Cadaveric and MRI Study width Neurosurgical Significance. World Neurosurg. 2021, 19. [Google Scholar] [CrossRef]
- Chung, B.S.; Ahn, Y.H.; Park, J.S. Ten Triangles around Cavernous Sinus for Surgical Approach, Described by Schematic Diagram and Three Dimensional Models with the Sectioned Images. J. Korean. Med. Sci. 2016, 31, 1455–1463. [Google Scholar] [CrossRef] [Green Version]
- Youssef, A.S.; van Loveren, H.R. Posterior clinoidectomy: Dural tailoring technique and clinical application. Skull Base 2009, 19, 183–191. [Google Scholar] [CrossRef] [Green Version]
- Iaconetta, G.; Fusco, M.; Cavallo, L.M.; Cappabianca, P.; Samii, M.; Tschabitscher, M. The abducens nerve: Microanatomic and endoscopic study. Neurosurgery 2007, 61 (Suppl. 3), 7–14. [Google Scholar] [CrossRef] [PubMed]
- Wysiadecki, G.; Orkisz, S.; Gałązkiewicz-Stolarczyk, M.; Brzeziński, P.; Polguj, M.; Topol, M. The abducens nerve: Its topography and anatomical variations in intracranial course with clinical commentary. Folia Morphol. 2015, 74, 236–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wysiadecki, G.; Haładaj, R.; Polguj, M.; Żytkowski, A.; Topol, M. Bilateral Extensive Ossification of the Posterior Petroclinoid Ligament: An Anatomical Case Report and Literature Review. J. Neurol. Surg. A Cent. Eur. Neurosurg. 2019, 80, 122–126. [Google Scholar] [CrossRef]
- Skrzat, J.; Walocha, J.; Jaworek, J.K.; Mróz, I. The clinical significance of the petroclinoid ligament. Folia Morphol. 2007, 66, 39–43. [Google Scholar]
- Cederberg, R.A.; Benson, B.W.; Nunn, M.; English, J.D. Calcification of the interclinoid and petroclinoid ligaments of sella turcica: A radiographic study of the prevalence. Orthod. Craniofac. Res. 2003, 6, 227–232. [Google Scholar] [CrossRef]
- Kimball, D.; Kimball, H.; Matusz, P.; Tubbs, R.S.; Loukas, M.; Cohen-Gadol, A.A. Ossification of the Posterior Petroclinoid Dural Fold: A Cadaveric Study with Neurosurgical Significance. J. Neurol. Surg. B Skull Base 2015, 76, 272–277. [Google Scholar] [CrossRef] [Green Version]
- Touska, P.; Hasso, S.; Oztek, A.; Chinaka, F.; Connor, S.E.J. Skull base ligamentous mineralisation: Evaluation using computed tomography and a review of the clinical relevance. Insights Imaging 2019, 10, 55. [Google Scholar] [CrossRef] [PubMed]
- Kıroğlu, Y.; Callı, C.; Karabulut, N.; Oncel, C. Intracranial calcifications on CT. Diagn. Interv. Radiol. 2010, 16, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Barges-Coll, J.; Fernandez-Miranda, J.C.; Prevedello, D.M.; Gardner, P.; Morera, V.; Madhok, R.; Carrau, R.L.; Snyderman, C.H.; Rhoton, A.L., Jr.; Kassam, A.B. Avoiding injury to the abducens nerve during expanded endonasal endoscopic surgery: Anatomic and clinical case studies. Neurosurgery 2010, 67, 144–154. [Google Scholar] [CrossRef]
- Nathan, H.; Ouaknine, G.; Kosary, I.Z. The abducens nerve. Anatomical variations in its course. J. Neurosurg. 1974, 41, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Umansky, F.; Elidan, J.; Valarezo, A. Dorello’s canal: A microanatomical study. J. Neurosurg. 1991, 75, 294–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomio, R.; Toda, M.; Sutiono, A.B.; Horiguchi, T.; Aiso, S.; Yoshida, K. Grüber’s ligament as a useful landmark for the abducens nerve in the transnasal approach. J. Neurosurg. 2015, 122, 499–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inal, M.; Muluk, N.B.; Burulday, V.; Akgül, M.H.; Ozveren, M.F.; Çelebi, U.O.; Şimşek, G.; Daphan, B.Ü. Investigation of the calcification at the petroclival region through Multi-slice Computed Tomography of the skull base. J. Craniomaxillofac. Surg. 2016, 44, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Icke, C.; Ozer, E.; Arda, N. Microanatomical characteristics of the petrosphenoidal ligament of Gruber. Turk. Neurosurg. 2010, 20, 323–327. [Google Scholar] [CrossRef] [Green Version]
- Iwanaga, J.; Altafulla, J.J.; Gutierrez, S.; Dupont, G.; Watanabe, K.; Litvack, Z.; Tubbs, R.S. The Petroclinoid Ligament: Its Morphometrics, Relationships, Variations, and Suggestion for New Terminology. J. Neurol. Surg. B Skull Base 2020, 81, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Tubbs, R.S.; Radcliff, V.; Shoja, M.M.; Naftel, R.P.; Mortazavi, M.M.; Zurada, A.; Loukas, M.; Cohen Gadol, A.A. Dorello canal revisited: An observation that potentially explains the frequency of abducens nerve injury after head injury. World Neurosurg. 2012, 77, 119–121. [Google Scholar] [CrossRef]
- Ozveren, M.F.; Uchida, K.; Tekdemir, I.; Cobanoglu, B.; Akdemir, I.; Kawase, T.; Deda, H. Dural and arachnoid membraneous protection of the abducens nerve at the petroclival region. Skull Base 2002, 12, 181–188. [Google Scholar] [CrossRef] [Green Version]
- Isolan, G.; de Oliveira, E.; Mattos, J.P. Microsurgical anatomy of the arterial compartment of the cavernous sinus: Analysis of 24 cavernous sinus. Arq. Neuropsiquiatr. 2005, 63, 259–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tran-Dinh, H. Cavernous branches of the internal carotid artery: Anatomy and nomenclature. Neurosurgery 1987, 20, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Vutskits, L.; Reisch, R.; Patonay, L.; Fries, G. The “rete mirabile” of the clivus and the dorsum sellae. A microanatomical study. Minim. Invasive Neurosurg. 1996, 39, 138–140. [Google Scholar] [CrossRef] [PubMed]
- Arbolay, O.L.; González, J.G.; González, R.H.; Gálvez, Y.H. Extended endoscopic endonasal approach to the skull base. Minim. Invasive Neurosurg. 2009, 52, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Kassam, A.B.; Gardner, P.; Snyderman, C.; Mintz, A.; Carrau, R. Expanded endonasal approach: Fully endoscopic, completely transnasal approach to the middle third of the clivus, petrous bone, middle cranial fossa, and infratemporal fossa. Neurosurg. Focus. 2005, 19, E6. [Google Scholar] [CrossRef] [Green Version]
- Cavallo, L.M.; Cappabianca, P.; Messina, A.; Esposito, F.; Stella, L.; de Divitiis, E.; Tschabitscher, M. The extended endoscopic endonasal approach to the clivus and cranio-vertebral junction: Anatomical study. Childs Nerv. Syst. 2007, 23, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Oertel, J.; Senger, S.; Linsler, S. The extended endoscopic approach to perisellar and skull base lesions: Is one nostril enough? Neurosurg. Rev. 2020, 43, 1519–1529. [Google Scholar] [CrossRef]
- Iwanaga, J.; Singh, V.; Ohtsuka, A.; Hwang, Y.; Kim, H.J.; Moryś, J.; Ravi, K.S.; Ribatti, D.; Trainor, P.A.; Sañudo, J.R.; et al. Acknowledging the use of human cadaveric tissues in research papers: Recommendations from anatomical journal editors. Clin. Anat. 2021, 34, 2–4. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Medial Border (mm) | Lateral Border (mm) | Superior Border (mm) | Area (mm2) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| This Study | Isolan et al. | Watanabe et al. | This Study | Isolan et al. | Watanabe et al. | This study | Isolan et al. | Watanabe et al. | This Study | Isolan et al. | Watanabe et al. | |
| Min. | 11.9 | - | - | 9.6 | - | - | 7.1 | - | - | 33.9 | - | - |
| Max. | 20.9 | - | - | 14.8 | - | - | 15.1 | - | - | 96.2 | - | - |
| Mean | 16.1 | 16.22 | 16.4 | 11.9 | 11.37 | 11.3 | 10.4 | 7.25 | 9.6 | 60.7 | 41.79 | 45.9 |
| Median | 15.6 | - | - | 11.8 | - | - | 10.2 | - | - | 60.6 | - | - |
| SD | 2.2 | 0.36 | 3.4 | 1.1 | 0.54 | 3.4 | 2 | 1.03 | 3.6 | 15.5 | 6.45 | 25 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wysiadecki, G.; Radek, M.; Tubbs, R.S.; Iwanaga, J.; Walocha, J.; Brzeziński, P.; Polguj, M. Microsurgical Anatomy of the Inferomedial Paraclival Triangle: Contents, Topographical Relationships and Anatomical Variations. Brain Sci. 2021, 11, 596. https://doi.org/10.3390/brainsci11050596
Wysiadecki G, Radek M, Tubbs RS, Iwanaga J, Walocha J, Brzeziński P, Polguj M. Microsurgical Anatomy of the Inferomedial Paraclival Triangle: Contents, Topographical Relationships and Anatomical Variations. Brain Sciences. 2021; 11(5):596. https://doi.org/10.3390/brainsci11050596
Chicago/Turabian StyleWysiadecki, Grzegorz, Maciej Radek, R. Shane Tubbs, Joe Iwanaga, Jerzy Walocha, Piotr Brzeziński, and Michał Polguj. 2021. "Microsurgical Anatomy of the Inferomedial Paraclival Triangle: Contents, Topographical Relationships and Anatomical Variations" Brain Sciences 11, no. 5: 596. https://doi.org/10.3390/brainsci11050596