
Cerebral Autoregulation in Ischemic Stroke: From Pathophysiology to Clinical Concepts

{kind=link}
{kind=link}
Abstract
:1. Introduction
- discuss the role of CA in the ischemic process
- the methodology used to evaluate CA in IS
- CA in IS patients
- the evolution in different phases of IS (acute, sub-acute and chronic)
- the relationship with stroke subtypes
- the association with clinical outcomes
- potential non-reperfusion therapies for IS patients based on CA concept
- the impact of common IS-associated comorbidities and phenotype on CA status.
2. The Potential Role of CA in the Ischemic Process in the Acute Phase of IS
3. Methods Used to Assess CA in AIS
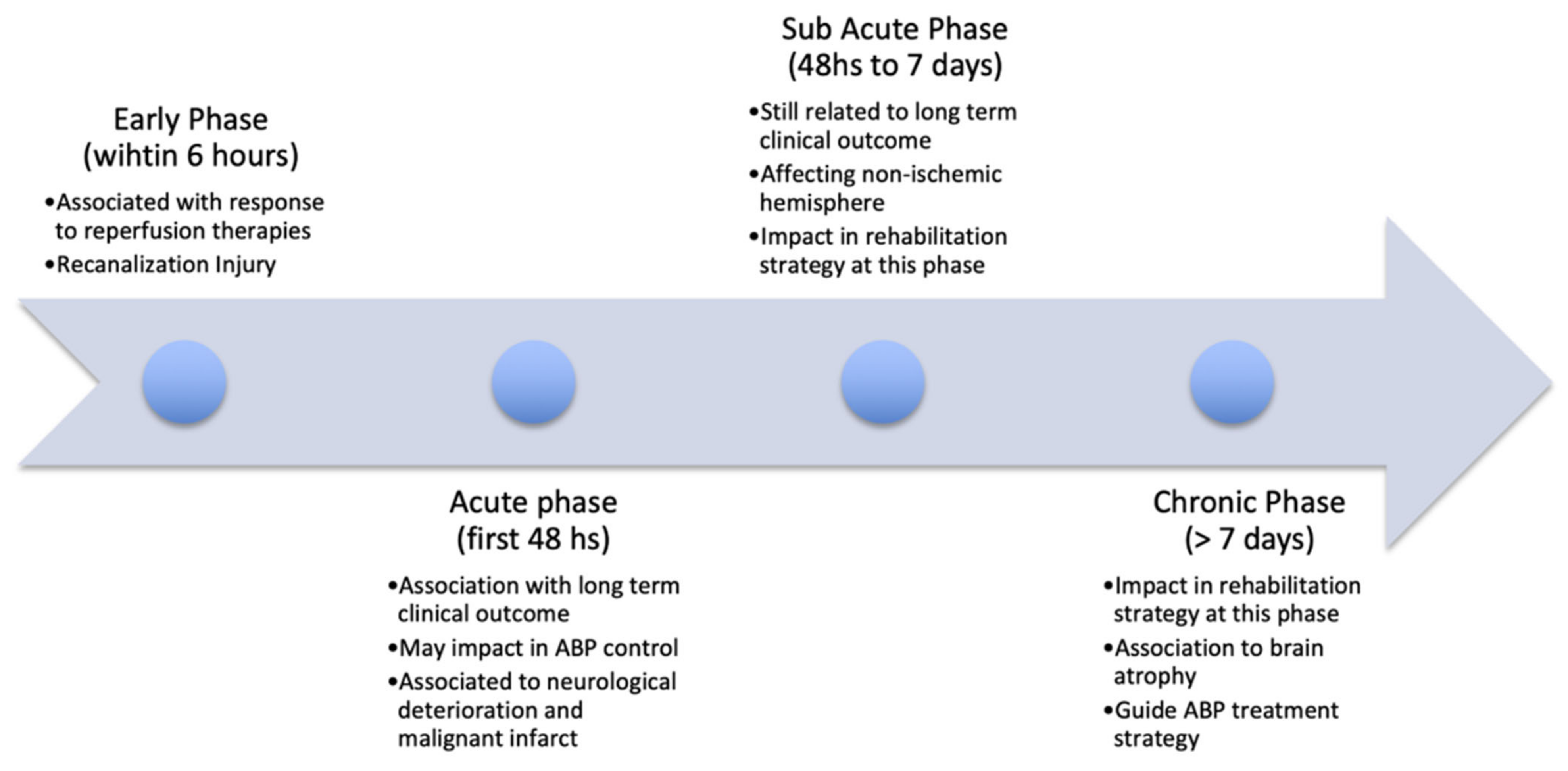
4. CA Evolution in Different Phases of IS (Acute, Sub-Acute and Chronic)
4.1. Acute Phase (<48 h)
4.2. Sub-Acute Phase (48 h to 7 Days)
4.3. Chronic Phase (>7 Days)
4.4. Summary
5. CA in Different Stroke Subtypes
5.1. Large and Small Vessel Artery Stroke
5.2. Intra- and Extracranial Stenosis
5.3. Anterior and Posterior Circulation
5.4. Summary
6. CA and Outcome in IS
Summary
7. Potential Non-Reperfusion Therapies for IS Patients Based on CA Concept
7.1. Blood Pressure Management
7.2. Head-of-Bed Positioning
7.3. Summary
8. The Impact of Comorbidities and Phenotype in CA and Stroke
8.1. Hypertension
8.2. Diabetes
8.3. Chronic Kidney Disease
8.4. Heart Failure
8.5. Phenotype: Age & Sex
8.6. Summary
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Campbell, B.C.V.; De Silva, D.A.; Macleod, M.R.; Coutts, S.B.; Schwamm, L.H.; Davis, S.M.; Donnan, G.A. Ischaemic stroke. Nat. Rev. Dis. Prim. 2019, 5, 70. [Google Scholar] [CrossRef] [PubMed]
- Prabhakaran, S.; Ruff, I.; Bernstein, R.A. Acute stroke intervention: A systematic review. JAMA 2015, 313, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Goyal, M.; Menon, B.K.; van Zwam, W.H.; Dippel, D.W.; Mitchell, P.J.; Demchuk, A.M.; Dávalos, A.; Majoie, C.B.; van der Lugt, A.; de Miquel, M.A.; et al. Endovascular thrombectomy after large-vessel ischaemic stroke: A meta-analysis of individual patient data from five randomised trials. Lancet 2016, 387, 1723–1731. [Google Scholar] [CrossRef]
- Smith, E.E.; Saver, J.L.; Cox, M.; Liang, L.; Matsouaka, R.; Xian, Y.; Bhatt, D.L.; Fonarow, G.C.; Schwamm, L.H. Increase in Endovascular Therapy in Get With The Guidelines-Stroke After the Publication of Pivotal Trials. Circulation 2017, 136, 2303–2310. [Google Scholar] [CrossRef]
- Craig, L.E.; Middleton, S.; Hamilton, H.; Cudlip, F.; Swatzell, V.; Alexandrov, A.V.; Lightbody, E.; Watkins, D.C.; Philip, S.; Cadilhac, D.A.; et al. Does the Addition of Non-Approved Inclusion and Exclusion Criteria for rtPA Impact Treatment Rates? Findings in Australia, the UK, and the USA. Interv. Neurol. 2020, 8, 1–12. [Google Scholar] [CrossRef]
- Goyal, M.; Ospel, J. Challenges to stroke care 5 years after endovascular therapy became the standard. Lancet Neurol. 2020, 19, 210–211. [Google Scholar] [CrossRef]
- Martins, S.O.; Mont’Alverne, F.; Rebello, L.C.; Abud, D.G.; Silva, G.S.; Lima, F.O.; Parente, B.S.M.; Nakiri, G.S.; Faria, M.B.; Frudit, M.E.; et al. Thrombectomy for Stroke in the Public Health Care System of Brazil. N. Engl. J. Med. 2020, 382, 2316–2326. [Google Scholar] [CrossRef]
- Bustamante, A.; Ning, M.; García-Berrocoso, T.; Penalba, A.; Boada, C.; Simats, A.; Pagola, J.; Ribó, M.; Molina, C.; Lo, E.; et al. Usefulness of ADAMTS13 to predict response to recanalization therapies in acute ischemic stroke. Neurology 2018, 90, e995–e1004. [Google Scholar] [CrossRef]
- Nogueira, R.C.; Lam, M.Y.; Llwyd, O.; Salinet, A.S.M.; Bor-Seng-Shu, E.; Panerai, R.B.; Robinson, T.G. Cerebral autoregulation and response to intravenous thrombolysis for acute ischemic stroke. Sci. Rep. 2020, 10, 10554. [Google Scholar] [CrossRef]
- Anderson, C.S.; Huang, Y.; Lindley, R.I.; Chen, X.; Arima, H.; Chen, G.; Li, Q.; Billot, L.; Delcourt, C.; Bath, P.M.; et al. Intensive blood pressure reduction with intravenous thrombolysis therapy for acute ischaemic stroke (ENCHANTED): An international, randomised, open-label, blinded-endpoint, phase 3 trial. Lancet 2019, 393, 877–888. [Google Scholar] [CrossRef] [Green Version]
- Iadecola, C. Neurovascular regulation in the normal brain and in Alzheimer’s disease. Nat. Rev. Neurosci. 2004, 5, 347–360. [Google Scholar] [CrossRef]
- Markus, H.S. Cerebral perfusion and stroke. J. Neurol. Neurosurg. Psychiatry 2004, 75, 353–361. [Google Scholar] [CrossRef]
- Panerai, R.B. Assessment of cerebral pressure autoregulation in humans—A review of measurement methods. Physiol. Meas. 1998, 19, 305–338. [Google Scholar] [CrossRef]
- Panerai, R.B. Cerebral autoregulation: From models to clinical applications. Cardiovasc. Eng. 2008, 8, 42–59. [Google Scholar] [CrossRef]
- Czosnyka, M.; Brady, K.; Reinhard, M.; Smielewski, P.; Steiner, L.A. Monitoring of cerebrovascular autoregulation: Facts, myths, and missing links. Neurocrit. Care 2009, 10, 373–386. [Google Scholar] [CrossRef]
- Nogueira, R.C.; Bor-Seng-Shu, E.; Santos, M.R.; Negrão, C.E.; Teixeira, M.J.; Panerai, R.B. Dynamic cerebral autoregulation changes during sub-maximal handgrip maneuver. PLoS ONE 2013, 8, e70821. [Google Scholar] [CrossRef] [Green Version]
- Aaslid, R. Cerebral autoregulation and vasomotor reactivity. Front. Neurol. Neurosci. 2006, 21, 216–228. [Google Scholar] [CrossRef]
- Willie, C.K.; Tzeng, Y.-C.; Fisher, J.A.; Ainslie, P.N. Integrative regulation of human brain blood flow. J. Physiol. 2014, 592, 841–859. [Google Scholar] [CrossRef]
- Heistad, D.D.; Kontos, H.A. Cerebral circulation. In Handbook of Physiology, The Cardiovascular System, Peripheral Circulation and Organ Blood Flow; Abboud: Bethesda, MD, USA, 1983; Volume 3, pp. 137–182. [Google Scholar]
- Paulson, O.B.; Strandgaard, S.; Edvinsson, L. Cerebral autoregulation. Cerebrovasc. Brain Metab. Rev. 1990, 2, 161–192. [Google Scholar]
- Liebeskind, D.S. Collaterals in acute stroke: Beyond the clot. Neuroimaging Clin. N. Am. 2005, 15, 553–573. [Google Scholar] [CrossRef]
- Siesjö, B.K. Pathophysiology and treatment of focal cerebral ischemia. Part I: Pathophysiology. J. Neurosurg. 1992, 77, 169–184. [Google Scholar] [CrossRef]
- Hossmann, K.A. Viability thresholds and the penumbra of focal ischemia. Ann. Neurol. 1994, 36, 557–565. [Google Scholar] [CrossRef]
- Young, A.R.; Touzani, O.; Derlon, J.M.; Sette, G.; MacKenzie, E.T.; Baron, J.C. Early reperfusion in the anesthetized baboon reduces brain damage following middle cerebral artery occlusion: A quantitative analysis of infarction volume. Stroke 1997, 28, 632–637. [Google Scholar] [CrossRef]
- Heiss, W.D.; Graf, R.; Wienhard, K.; Löttgen, J.; Saito, R.; Fujita, T.; Rosner, G.; Wagner, R. Dynamic penumbra demonstrated by sequential multitracer PET after middle cerebral artery occlusion in cats. J. Cereb. Blood Flow Metab. 1994, 14, 892–902. [Google Scholar] [CrossRef] [Green Version]
- Yang, M.; Yang, Z.; Yuan, T.; Feng, W.; Wang, P. A Systemic Review of Functional Near-Infrared Spectroscopy for Stroke: Current Application and Future Directions. Front. Neurol. 2019, 10, 58. [Google Scholar] [CrossRef]
- Martins, E.; Inamura, K.; Themner, K.; Malmqvist, K.G.; Siesjo, B.K. Accumulation of calcium and loss of potassium in the hippocampus following transient cerebral ischemia: A proton microprobe study. J. Cereb. Blood Flow Metab. 1988, 8, 531–538. [Google Scholar] [CrossRef] [Green Version]
- Wexler, B.C. Metabolic changes in response to acute cerebral ischemia following bilateral carotid artery ligation in arteriosclerotic versus nonarteriosclerotic rats. Stroke 1970, 1, 112–121. [Google Scholar] [CrossRef] [Green Version]
- Choi, D.W. Calcium-Mediated neurotoxicity: Relationship to specific channel types and role in ischemic damage. Trends Neurosci. 1988, 11, 465–469. [Google Scholar] [CrossRef]
- Panickar, K.S.; Norenberg, M.D. Astrocytes in cerebral ischemic injury: Morphological and general considerations. Glia 2005, 50, 287–298. [Google Scholar] [CrossRef]
- Panerai, R.B. Transcranial Doppler for evaluation of cerebral autoregulation. Clin. Auton. Res. Off. J. Clin. Auton. Res. Soc. 2009, 19, 197–211. [Google Scholar] [CrossRef] [PubMed]
- Tiecks, F.P.; Lam, A.M.; Aaslid, R.; Newell, D.W. Comparison of static and dynamic cerebral autoregulation measurements. Stroke 1995, 26, 1014–1019. [Google Scholar] [CrossRef] [PubMed]
- Aaslid, R.; Lindegaard, K.F.; Sorteberg, W.; Nornes, H. Cerebral autoregulation dynamics in humans. Stroke 1989, 20, 45–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minhas, J.S.; Panerai, R.B.; Robinson, T.G. Modelling the cerebral haemodynamic response in the physiological range of PaCO2. Physiol. Meas. 2018, 39, 065001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salinet, A.S.; Robinson, T.G.; Panerai, R.B. Effects of cerebral ischemia on human neurovascular coupling, CO2 reactivity, and dynamic cerebral autoregulation. J. Appl. Physiol. (1985) 2015, 118, 170–177. [Google Scholar] [CrossRef] [Green Version]
- Castro, P.; Azevedo, E.; Sorond, F. Cerebral Autoregulation in Stroke. Curr. Atheroscler. Rep. 2018, 20, 37. [Google Scholar] [CrossRef]
- Intharakham, K.; Beishon, L.; Panerai, R.B.; Haunton, V.J.; Robinson, T.G. Assessment of cerebral autoregulation in stroke: A systematic review and meta-analysis of studies at rest. J. Cereb. Blood Flow Metab. 2019, 39, 2105–2116. [Google Scholar] [CrossRef] [Green Version]
- Aries, M.J.; Elting, J.W.; De Keyser, J.; Kremer, B.P.; Vroomen, P.C. Cerebral autoregulation in stroke: A review of transcranial Doppler studies. Stroke 2010, 41, 2697–2704. [Google Scholar] [CrossRef]
- Lindegaard, K.F.; Lundar, T.; Wiberg, J.; Sjøberg, D.; Aaslid, R.; Nornes, H. Variations in middle cerebral artery blood flow investigated with noninvasive transcranial blood velocity measurements. Stroke 1987, 18, 1025–1030. [Google Scholar] [CrossRef] [Green Version]
- Newell, D.W.; Aaslid, R.; Lam, A.; Mayberg, T.S.; Winn, H.R. Comparison of flow and velocity during dynamic autoregulation testing in humans. Stroke 1994, 25, 793–797. [Google Scholar] [CrossRef] [Green Version]
- Petersen, N.H.; Silverman, A.; Strander, S.M.; Kodali, S.; Wang, A.; Sansing, L.H.; Schindler, J.L.; Falcone, G.J.; Gilmore, E.J.; Jasne, A.S.; et al. Fixed Compared With Autoregulation-Oriented Blood Pressure Thresholds After Mechanical Thrombectomy for Ischemic Stroke. Stroke 2020, 51, 914–921. [Google Scholar] [CrossRef]
- Ghosh, A.; Elwell, C.; Smith, M. Review article: Cerebral near-infrared spectroscopy in adults: A work in progress. Anesth. Analg. 2012, 115, 1373–1383. [Google Scholar] [CrossRef]
- Nguyen, H.D.; Hong, K.S. Bundled-optode implementation for 3D imaging in functional near-infrared spectroscopy. Biomed. Opt. Express 2016, 7, 3491–3507. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, H.D.; Hong, K.S.; Shin, Y.I. Bundled-Optode Method in Functional Near-Infrared Spectroscopy. PLoS ONE 2016, 11, e0165146. [Google Scholar] [CrossRef]
- Powers, W.J.; Videen, T.O.; Diringer, M.N.; Aiyagari, V.; Zazulia, A.R. Autoregulation after ischaemic stroke. J. Hypertens. 2009, 27, 2218–2222. [Google Scholar] [CrossRef] [Green Version]
- Dohmen, C.; Bosche, B.; Graf, R.; Reithmeier, T.; Ernestus, R.I.; Brinker, G.; Sobesky, J.; Heiss, W.D. Identification and clinical impact of impaired cerebrovascular autoregulation in patients with malignant middle cerebral artery infarction. Stroke 2007, 38, 56–61. [Google Scholar] [CrossRef] [Green Version]
- Panerai, R.B.; Jara, J.L.; Saeed, N.P.; Horsfield, M.A.; Robinson, T.G. Dynamic cerebral autoregulation following acute ischaemic stroke: Comparison of transcranial Doppler and magnetic resonance imaging techniques. J. Cereb. Blood Flow Metab. 2016, 36, 2194–2202. [Google Scholar] [CrossRef] [Green Version]
- Panerai, R.B.; Sammons, E.L.; Smith, S.M.; Rathbone, W.E.; Bentley, S.; Potter, J.F.; Samani, N.J. Continuous estimates of dynamic cerebral autoregulation: Influence of non-invasive arterial blood pressure measurements. Physiol. Meas. 2008, 29, 497–513. [Google Scholar] [CrossRef] [Green Version]
- Lassen, N.A. Control of cerebral circulation in health and disease. Circ. Res. 1974, 34, 749–760. [Google Scholar] [CrossRef] [Green Version]
- Rosenblum, W.I. Autoregulatory plateau: Does it exist? J. Cereb. Blood Flow Metab. 1995, 15, 174–177. [Google Scholar] [CrossRef]
- Strandgaard, S. Autoregulation of cerebral blood flow in hypertensive patients. The modifying influence of prolonged antihypertensive treatment on the tolerance to acute, drug-induced hypotension. Circulation 1976, 53, 720–727. [Google Scholar] [CrossRef] [Green Version]
- Georgiadis, D.; Schwarz, S.; Evans, D.H.; Schwab, S.; Baumgartner, R.W. Cerebral autoregulation under moderate hypothermia in patients with acute stroke. Stroke 2002, 33, 3026–3029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Novak, V.; Chowdhary, A.; Farrar, B.; Nagaraja, H.; Braun, J.; Kanard, R.; Novak, P.; Slivka, A. Altered cerebral vasoregulation in hypertension and stroke. Neurology 2003, 60, 1657–1663. [Google Scholar] [CrossRef] [PubMed]
- Dawson, S.L.; Blake, M.J.; Panerai, R.B.; Potter, J.F. Dynamic but not static cerebral autoregulation is impaired in acute ischaemic stroke. Cerebrovasc. Dis. 2000, 10, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Dawson, S.L.; Panerai, R.B.; Potter, J.F. Serial changes in static and dynamic cerebral autoregulation after acute ischaemic stroke. Cerebrovasc. Dis. 2003, 16, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Panerai, R.B.; Kelsall, A.W.; Rennie, J.M.; Evans, D.H. Cerebral autoregulation dynamics in premature newborns. Stroke 1995, 26, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Claassen, J.A.; Meel-van den Abeelen, A.S.; Simpson, D.M.; Panerai, R.B. Transfer function analysis of dynamic cerebral autoregulation: A white paper from the International Cerebral Autoregulation Research Network. J. Cereb. Blood Flow Metab. 2016, 36, 665–680. [Google Scholar] [CrossRef] [Green Version]
- Simpson, D.; Claassen, J. CrossTalk opposing view: Dynamic cerebral autoregulation should be quantified using induced (rather than spontaneous) blood pressure fluctuations. J. Physiol. 2018, 596, 7–9. [Google Scholar] [CrossRef]
- Salinet, A.S.; Silva, N.C.; Caldas, J.; de Azevedo, D.S.; de-Lima-Oliveira, M.; Nogueira, R.C.; Conforto, A.B.; Texeira, M.J.; Robinson, T.G.; Panerai, R.B.; et al. Impaired cerebral autoregulation and neurovascular coupling in middle cerebral artery stroke: Influence of severity? J. Cereb. Blood Flow Metab. 2019, 39, 2277–2285. [Google Scholar] [CrossRef]
- Panerai, R.B.; White, R.P.; Markus, H.S.; Evans, D.H. Grading of cerebral dynamic autoregulation from spontaneous fluctuations in arterial blood pressure. Stroke 1998, 29, 2341–2346. [Google Scholar] [CrossRef] [Green Version]
- Reinhard, M.; Wihler, C.; Roth, M.; Harloff, A.; Niesen, W.D.; Timmer, J.; Weiller, C.; Hetzel, A. Cerebral autoregulation dynamics in acute ischemic stroke after rtPA thrombolysis. Cerebrovasc. Dis. 2008, 26, 147–155. [Google Scholar] [CrossRef]
- Reinhard, M.; Rutsch, S.; Lambeck, J.; Wihler, C.; Czosnyka, M.; Weiller, C.; Hetzel, A. Dynamic cerebral autoregulation associates with infarct size and outcome after ischemic stroke. Acta Neurol. Scand. 2012, 125, 156–162. [Google Scholar] [CrossRef]
- Reinhard, M.; Roth, M.; Guschlbauer, B.; Harloff, A.; Timmer, J.; Czosnyka, M.; Hetzel, A. Dynamic cerebral autoregulation in acute ischemic stroke assessed from spontaneous blood pressure fluctuations. Stroke 2005, 36, 1684–1689. [Google Scholar] [CrossRef] [Green Version]
- Meyer, M.; Juenemann, M.; Braun, T.; Schirotzek, I.; Tanislav, C.; Engelhard, K.; Schramm, P. Impaired Cerebrovascular Autoregulation in Large Vessel Occlusive Stroke after Successful Mechanical Thrombectomy: A Prospective Cohort Study. J. Stroke Cerebrovasc. Dis. Off. J. Natl. Stroke Assoc. 2020, 29, 104596. [Google Scholar] [CrossRef]
- Novak, V.; Yang, A.C.; Lepicovsky, L.; Goldberger, A.L.; Lipsitz, L.A.; Peng, C.K. Multimodal pressure-flow method to assess dynamics of cerebral autoregulation in stroke and hypertension. Biomed. Eng. Online 2004, 3, 39. [Google Scholar] [CrossRef] [Green Version]
- Aoi, M.C.; Hu, K.; Lo, M.T.; Selim, M.; Olufsen, M.S.; Novak, V. Impaired cerebral autoregulation is associated with brain atrophy and worse functional status in chronic ischemic stroke. PLoS ONE 2012, 7, e46794. [Google Scholar] [CrossRef]
- Lam, M.Y.; Haunton, V.J.; Robinson, T.G.; Panerai, R.B. Dynamic cerebral autoregulation measurement using rapid changes in head positioning: Experiences in acute ischemic stroke and healthy control populations. Am. J. Physiol. Heart Circ. Physiol. 2019, 316, H673–H683. [Google Scholar] [CrossRef] [Green Version]
- Petersen, N.H.; Ortega-Gutierrez, S.; Reccius, A.; Masurkar, A.; Huang, A.; Marshall, R.S. Dynamic cerebral autoregulation is transiently impaired for one week after large-vessel acute ischemic stroke. Cerebrovasc. Dis. 2015, 39, 144–150. [Google Scholar] [CrossRef] [Green Version]
- Atkins, E.R.; Brodie, F.G.; Rafelt, S.E.; Panerai, R.B.; Robinson, T.G. Dynamic cerebral autoregulation is compromised acutely following mild ischaemic stroke but not transient ischaemic attack. Cerebrovasc. Dis. 2010, 29, 228–235. [Google Scholar] [CrossRef]
- Llwyd, O.; Salinet, A.S.M.; Panerai, R.B.; Lam, M.Y.; Saeed, N.P.; Brodie, F.; Bor-Seng-Shu, E.; Robinson, T.G.; Nogueira, R.C. Cerebral Haemodynamics following Acute Ischaemic Stroke: Effects of Stroke Severity and Stroke Subtype. Cerebrovasc. Dis. Extra 2018, 8, 80–89. [Google Scholar] [CrossRef]
- Saeed, N.P.; Panerai, R.B.; Horsfield, M.A.; Robinson, T.G. Does stroke subtype and measurement technique influence estimation of cerebral autoregulation in acute ischaemic stroke? Cerebrovasc. Dis. 2013, 35, 257–261. [Google Scholar] [CrossRef]
- Ma, H.; Guo, Z.N.; Jin, H.; Yan, X.; Liu, J.; Lv, S.; Zhang, P.; Sun, X.; Yang, Y. Preliminary Study of Dynamic Cerebral Autoregulation in Acute Ischemic Stroke: Association With Clinical Factors. Front. Neurol. 2018, 9, 1006. [Google Scholar] [CrossRef] [Green Version]
- Eames, P.J.; Blake, M.J.; Dawson, S.L.; Panerai, R.B.; Potter, J.F. Dynamic cerebral autoregulation and beat to beat blood pressure control are impaired in acute ischaemic stroke. J. Neurol. Neurosurg. Psychiatry 2002, 72, 467–472. [Google Scholar] [CrossRef]
- Tutaj, M.; Miller, M.; Krakowska-Stasiak, M.; Piątek, A.; Hebda, J.; Lątka, M.; Strojny, J.; Szczudlik, A.; Słowik, A. Dynamic cerebral autoregulation is compromised in ischaemic stroke of undetermined aetiology only in the non-affected hemisphere. Neurobiol. Neurochir. Pol. 2014, 48, 91–97. [Google Scholar] [CrossRef] [Green Version]
- Immink, R.V.; van Montfrans, G.A.; Stam, J.; Karemaker, J.M.; Diamant, M.; van Lieshout, J.J. Dynamic cerebral autoregulation in acute lacunar and middle cerebral artery territory ischemic stroke. Stroke 2005, 36, 2595–2600. [Google Scholar] [CrossRef]
- Guo, Z.N.; Liu, J.; Xing, Y.; Yan, S.; Lv, C.; Jin, H.; Yang, Y. Dynamic cerebral autoregulation is heterogeneous in different subtypes of acute ischemic stroke. PLoS ONE 2014, 9, e93213. [Google Scholar] [CrossRef]
- Salinet, A.S.; Panerai, R.B.; Robinson, T.G. The longitudinal evolution of cerebral blood flow regulation after acute ischaemic stroke. Cerebrovasc. Dis. Extra 2014, 4, 186–197. [Google Scholar] [CrossRef]
- Kwan, J.; Lunt, M.; Jenkinson, D. Assessing dynamic cerebral autoregulation after stroke using a novel technique of combining transcranial Doppler ultrasonography and rhythmic handgrip. Blood Press. Monit. 2004, 9, 3–8. [Google Scholar] [CrossRef]
- Guo, Z.-N.; Xing, Y.; Wang, S.; Ma, H.; Liu, J.; Yang, Y. Characteristics of dynamic cerebral autoregulation in cerebral small vessel disease: Diffuse and sustained. Sci. Rep. 2015, 5, 15269. [Google Scholar] [CrossRef] [Green Version]
- Xiong, L.; Tian, G.; Lin, W.; Wang, W.; Wang, L.; Leung, T.; Mok, V.; Liu, J.; Chen, X.; Wong, K.S. Is Dynamic Cerebral Autoregulation Bilaterally Impaired after Unilateral Acute Ischemic Stroke? J. Stroke Cerebrovasc. Dis. 2017, 26, 1081–1087. [Google Scholar] [CrossRef] [PubMed]
- Nomura, Y.; Faegle, R.; Hori, D.; Al-Qamari, A.; Nemeth, A.J.; Gottesman, R.; Yenokyan, G.; Brown, C.; Hogue, C.W. Cerebral Small Vessel, But Not Large Vessel Disease, Is Associated With Impaired Cerebral Autoregulation During Cardiopulmonary Bypass: A Retrospective Cohort Study. Anesth. Analg. 2018, 127, 1314–1322. [Google Scholar] [CrossRef] [PubMed]
- Reinhard, M.; Roth, M.; Müller, T.; Czosnyka, M.; Timmer, J.; Hetzel, A. Cerebral Autoregulation in Carotid Artery Occlusive Disease Assessed From Spontaneous Blood Pressure Fluctuations by the Correlation Coefficient Index. Stroke 2003, 34, 2138–2144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reinhard, M.; Roth, M.; Müller, T.; Guschlbauer, B.; Timmer, J.; Czosnyka, M.; Hetzel, A. Effect of Carotid Endarterectomy or Stenting on Impairment of Dynamic Cerebral Autoregulation. Stroke 2004, 35, 1381–1387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, H.-H.; Kuo, T.B.-J.; Wong, W.-J.; Luk, Y.-O.; Chern, C.-M.; Hsu, L.-C.; Sheng, W.-Y. Transfer Function Analysis of Cerebral Hemodynamics in Patients with Carotid Stenosis. J. Cereb. Blood Flow Metab. 1999, 19, 460–465. [Google Scholar] [CrossRef] [Green Version]
- White, R.P.; Markus, H.S. Impaired dynamic cerebral autoregulation in carotid artery stenosis. Stroke 1997, 28, 1340–1344. [Google Scholar] [CrossRef]
- Reinhard, M.; Müller, T.; Guschlbauer, B.; Timmer, J.; Hetzel, A. Dynamic cerebral autoregulation and collateral flow patterns in patients with severe carotid stenosis or occlusion. Ultrasound Med. Biol. 2003, 29, 1105–1113. [Google Scholar] [CrossRef]
- Guo, Z.-N.; Sun, X.; Liu, J.; Sun, H.; Zhao, Y.; Ma, H.; Xu, B.; Wang, Z.; Li, C.; Yan, X.; et al. The Impact of Variational Primary Collaterals on Cerebral Autoregulation. Front. Physiol. 2018, 9. [Google Scholar] [CrossRef]
- Reinhard, M.; Gerds, T.A.; Grabiak, D.; Zimmermann, P.R.; Roth, M.; Guschlbauer, B.; Timmer, J.; Czosnyka, M.; Weiller, C.; Hetzel, A. Cerebral dysautoregulation and the risk of ischemic events in occlusive carotid artery disease. J. Neurol. 2008, 255, 1182–1189. [Google Scholar] [CrossRef]
- Gong, X.; Liu, J.; Dong, P.; Zhang, P.; Li, N.; Zhao, X.; Wang, Y. Assessment of dynamic cerebral autoregulation in patients with basilar artery stenosis. PLoS ONE 2013, 8, e77802. [Google Scholar] [CrossRef] [Green Version]
- Gong, X.P.; Li, Y.; Jiang, W.J.; Wang, Y. Impaired dynamic cerebral autoregulation in middle cerebral artery stenosis. Neurol. Res. 2006, 28, 76–81. [Google Scholar] [CrossRef]
- Wang, S.; Guo, Z.N.; Xing, Y.; Ma, H.; Jin, H.; Liu, J.; Yang, Y. Dynamic Cerebral Autoregulation in Asymptomatic Patients with Unilateral Middle Cerebral Artery Stenosis. Medicine 2015, 94, e2234. [Google Scholar] [CrossRef]
- Chen, J.; Liu, J.; Xu, W.H.; Xu, R.; Hou, B.; Cui, L.Y.; Gao, S. Impaired dynamic cerebral autoregulation and cerebrovascular reactivity in middle cerebral artery stenosis. PLoS ONE 2014, 9, e88232. [Google Scholar] [CrossRef]
- Castro, P.; Serrador, J.M.; Rocha, I.; Sorond, F.; Azevedo, E. Efficacy of Cerebral Autoregulation in Early Ischemic Stroke Predicts Smaller Infarcts and Better Outcome. Front. Neurol. 2017, 8, 113. [Google Scholar] [CrossRef] [Green Version]
- Martins, A.I.; Sargento-Freitas, J.; Silva, F.; Jesus-Ribeiro, J.; Correia, I.; Gomes, J.P.; Aguiar-Gonçalves, M.; Cardoso, L.; Machado, C.; Rodrigues, B.; et al. Recanalization Modulates Association Between Blood Pressure and Functional Outcome in Acute Ischemic Stroke. Stroke 2016, 47, 1571–1576. [Google Scholar] [CrossRef] [Green Version]
- Tikhonoff, V.; Zhang, H.; Richart, T.; Staessen, J.A. Blood pressure as a prognostic factor after acute stroke. Lancet Neurol. 2009, 8, 938–948. [Google Scholar] [CrossRef]
- Tian, G.; Ji, Z.; Huang, K.; Lin, Z.; Pan, S.; Wu, Y. Dynamic cerebral autoregulation is an independent outcome predictor of acute ischemic stroke after endovascular therapy. BMC Neurol. 2020, 20, 189. [Google Scholar] [CrossRef]
- Castro, P.; Azevedo, E.; Rocha, I.; Sorond, F.; Serrador, J.M. Chronic kidney disease and poor outcomes in ischemic stroke: Is impaired cerebral autoregulation the missing link? BMC Neurol. 2018, 18, 21. [Google Scholar] [CrossRef] [Green Version]
- Castro, P.; Azevedo, E.; Serrador, J.; Rocha, I.; Sorond, F. Hemorrhagic transformation and cerebral edema in acute ischemic stroke: Link to cerebral autoregulation. J. Neurol. Sci. 2017, 372, 256–261. [Google Scholar] [CrossRef] [Green Version]
- Ito, T.; Yamakawa, H.; Bregonzio, C.; Terrón, J.A.; Falcón-Neri, A.; Saavedra, J.M. Protection against ischemia and improvement of cerebral blood flow in genetically hypertensive rats by chronic pretreatment with an angiotensin II AT1 antagonist. Stroke 2002, 33, 2297–2303. [Google Scholar] [CrossRef] [Green Version]
- Gur, A.Y.; Gücüyener, D.; Korczyn, A.D.; Üzüner, N.; Gilutz, Y.; Özdemir, G.; Bornstein, N.M. Cerebral vasomotor reactivity and dementia after ischemic stroke. Acta Neurol. Scand. 2010, 122, 383–388. [Google Scholar] [CrossRef]
- De Heus, R.A.A.; de Jong, D.L.K.; Sanders, M.L.; van Spijker, G.J.; Oudegeest-Sander, M.H.; Hopman, M.T.; Lawlor, B.A.; Olde Rikkert, M.G.M.; Claassen, J. Dynamic Regulation of Cerebral Blood Flow in Patients With Alzheimer Disease. Hypertension 2018, 72, 139–150. [Google Scholar] [CrossRef]
- Zhou, G.; Zhao, X.; Lou, Z.; Zhou, S.; Shan, P.; Zheng, N.; Yu, X.; Ma, L. Impaired Cerebral Autoregulation in Alzheimer’s Disease: A Transcranial Doppler Study. J. Alzheimer Dis. JAD 2019, 72, 623–631. [Google Scholar] [CrossRef] [PubMed]
- Beishon, L.C.; Williams, C.A.L.; Panerai, R.B.; Robinson, T.G.; Haunton, V.J. The assessment of neurovascular coupling with the Addenbrooke’s Cognitive Examination: A functional transcranial Doppler ultrasonographic study. J. Neurophysiol. 2018, 119, 1084–1094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moody, M.; Panerai, R.B.; Eames, P.J.; Potter, J.F. Cerebral and systemic hemodynamic changes during cognitive and motor activation paradigms. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2005, 288, R1581–R1588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chi, N.F.; Hu, H.H.; Chan, L.; Wang, C.Y.; Chao, S.P.; Huang, L.K.; Ku, H.L.; Hu, C.J. Impaired cerebral autoregulation is associated with poststroke cognitive impairment. Ann. Clin. Transl. Neurol. 2020, 7, 1092–1102. [Google Scholar] [CrossRef]
- ENOS Trial Investigators. Efficacy of nitric oxide, with or without continuing antihypertensive treatment, for management of high blood pressure in acute stroke (ENOS): A partial-factorial randomised controlled trial. Lancet 2015, 385, 617–628. [Google Scholar] [CrossRef] [Green Version]
- Sandset, E.C.; Bath, P.M.W.; Boysen, G.; Jatuzis, D.; Kõrv, J.; Lüders, S.; Murray, G.D.; Richter, P.S.; Roine, R.O.; Terént, A.; et al. The angiotensin-receptor blocker candesartan for treatment of acute stroke (SCAST): A randomised, placebo-controlled, double-blind trial. Lancet 2011, 377, 741–750. [Google Scholar] [CrossRef]
- Gorelick, P.B.; Qureshi, S.; Farooq, M.U. Management of blood pressure in stroke. Int. J. Cardiol. Hypertens. 2019, 3, 100021. [Google Scholar] [CrossRef]
- Wang, H.; Tang, Y.; Rong, X.; Li, H.; Pan, R.; Wang, Y.; Peng, Y. Effects of early blood pressure lowering on early and long-term outcomes after acute stroke: An updated meta-analysis. PLoS ONE 2014, 9, e97917. [Google Scholar] [CrossRef] [Green Version]
- Qureshi Adnan, I. Acute Hypertensive Response in Patients with Stroke. Circulation 2008, 118, 176–187. [Google Scholar] [CrossRef] [Green Version]
- Rothwell, P.M. Blood pressure in acute stroke: Which questions remain? Lancet 2015, 385, 582–585. [Google Scholar] [CrossRef] [Green Version]
- Willmot, M.; Leonardi-Bee, J.; Bath, P.M. High blood pressure in acute stroke and subsequent outcome: A systematic review. Hypertension 2004, 43, 18–24. [Google Scholar] [CrossRef]
- Minhas, J.S.; Wang, X.; Lindley, R.I.; Delcourt, C.; Song, L.; Woodward, M.; Lee, T.H.; Broderick, J.P.; Pontes-Neto, O.M.; Kim, J.S.; et al. Comparative effects of intensive-blood pressure versus standard-blood pressure-lowering treatment in patients with severe ischemic stroke in the ENCHANTED trial. J. Hypertens. 2020, 39. [Google Scholar] [CrossRef]
- Anderson, C.S.; Olavarría, V.V. Head Positioning in Acute Stroke. Stroke 2019, 50, 224–228. [Google Scholar] [CrossRef]
- Anderson, C.S.; Arima, H.; Lavados, P.; Billot, L.; Hackett, M.L.; Olavarría, V.V.; Muñoz Venturelli, P.; Brunser, A.; Peng, B.; Cui, L.; et al. Cluster-Randomized, Crossover Trial of Head Positioning in Acute Stroke. N. Engl. J. Med. 2017, 376, 2437–2447. [Google Scholar] [CrossRef]
- Efficacy and safety of very early mobilisation within 24 h of stroke onset (AVERT): A randomised controlled trial. Lancet 2015, 386, 46–55. [CrossRef] [Green Version]
- National Guideline Centre. National Institute for Health and Care Excellence: Clinical Guidelines. In Stroke and Transient Ischaemic Attack in Over 16s: Diagnosis and Initial Management; National Institute for Health and Care Excellence: London, UK, 2019. [Google Scholar]
- Truijen, J.; Rasmussen, L.S.; Kim, Y.S.; Stam, J.; Stok, W.J.; Pott, F.C.; van Lieshout, J.J. Cerebral autoregulatory performance and the cerebrovascular response to head-of-bed positioning in acute ischaemic stroke. Eur. J. Neurol. 2018, 25, 1365-e1117. [Google Scholar] [CrossRef] [Green Version]
- Lam, M.Y.; Haunton, V.J.; Nath, M.; Panerai, R.B.; Robinson, T.G. The effect of head positioning on cerebral hemodynamics: Experiences in mild ischemic stroke. J. Neurol. Sci. 2020, 419, 117201. [Google Scholar] [CrossRef]
- Wajngarten, M.; Silva, G.S. Hypertension and Stroke: Update on Treatment. Eur. Cardiol. 2019, 14, 111–115. [Google Scholar] [CrossRef] [Green Version]
- Hong, K.S. Blood Pressure Management for Stroke Prevention and in Acute Stroke. J. Stroke 2017, 19, 152–165. [Google Scholar] [CrossRef]
- Traon, A.P.-L.; Costes-Salon, M.-C.; Galinier, M.; Fourcade, J.; Larrue, V. Dynamics of cerebral blood flow autoregulation in hypertensive patients. J. Neurol. Sci. 2002, 195, 139–144. [Google Scholar] [CrossRef]
- Eames, P.; Eames, P.J.; Blake, M.J.; Panerai, R.B.; Potter, J.F. Cerebral autoregulation indices are unimpaired by hypertension in middle aged and older people*. Am. J. Hypertens. 2003, 16, 746–753. [Google Scholar] [CrossRef] [Green Version]
- Lipsitz, L.A.; Mukai, S.; Hamner, J.; Gagnon, M.; Babikian, V. Dynamic regulation of middle cerebral artery blood flow velocity in aging and hypertension. Stroke 2000, 31, 1897–1903. [Google Scholar] [CrossRef] [Green Version]
- Serrador, J.M.; Sorond, F.A.; Vyas, M.; Gagnon, M.; Iloputaife, I.D.; Lipsitz, L.A. Cerebral pressure-flow relations in hypertensive elderly humans: Transfer gain in different frequency domains. J. Appl. Physiol. 2005, 98, 151–159. [Google Scholar] [CrossRef] [Green Version]
- van Beek, A.H.; Claassen, J.A.; Rikkert, M.G.; Jansen, R.W. Cerebral autoregulation: An overview of current concepts and methodology with special focus on the elderly. J. Cereb. Blood Flow Metab. 2008, 28, 1071–1085. [Google Scholar] [CrossRef]
- Kitagawa, K.; Oku, N.; Kimura, Y.; Yagita, Y.; Sakaguchi, M.; Hatazawa, J.; Sakoda, S. Relationship between cerebral blood flow and later cognitive decline in hypertensive patients with cerebral small vessel disease. Hypertens. Res. Off. J. Jpn. Soc. Hypertens. 2009, 32, 816–820. [Google Scholar] [CrossRef] [Green Version]
- Mankovsky, B.N.; Ziegler, D. Stroke in patients with diabetes mellitus. Diabetes Metab. Res. Rev. 2004, 20, 268–287. [Google Scholar] [CrossRef]
- Tziomalos, K.; Spanou, M.; Bouziana, S.D.; Papadopoulou, M.; Giampatzis, V.; Kostaki, S.; Dourliou, V.; Tsopozidi, M.; Savopoulos, C.; Hatzitolios, A.I. Type 2 diabetes is associated with a worse functional outcome of ischemic stroke. World J. Diabetes 2014, 5, 939–944. [Google Scholar] [CrossRef]
- Bellolio, M.F.; Gilmore, R.M.; Ganti, L. Insulin for glycaemic control in acute ischaemic stroke. Cochrane Database Syst. Rev. 2014, CD005346. [Google Scholar] [CrossRef]
- Fuentes, B.; Ntaios, G.; Putaala, J.; Thomas, B.; Turc, G.; Díez-Tejedor, E. European Stroke Organisation (ESO) guidelines on glycaemia management in acute stroke. Eur. Stroke J. 2018, 3, 5–21. [Google Scholar] [CrossRef]
- Kim, Y.-S.; Immink, R.V.; Stok, W.J.; Karemaker, J.M.; Secher, N.H.; van Lieshout, J.J. Dynamic cerebral autoregulatory capacity is affected early in Type 2 diabetes. Clin. Sci. 2008, 115, 255–262. [Google Scholar] [CrossRef] [Green Version]
- Hu, K.; Peng, C.K.; Huang, N.E.; Wu, Z.; Lipsitz, L.A.; Cavallerano, J.; Novak, V. Altered phase interactions between spontaneous blood pressure and flow fluctuations in type 2 diabetes mellitus: Nonlinear assessment of cerebral autoregulation. Phys. A Stat. Mech. Appl. 2008, 387, 2279–2292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vianna, L.C.; Deo, S.H.; Jensen, A.K.; Holwerda, S.W.; Zimmerman, M.C.; Fadel, P.J. Impaired dynamic cerebral autoregulation at rest and during isometric exercise in type 2 diabetes patients. Am. J. Physiol. Heart Circ. Physiol. 2015, 308, H681–H687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mankovsky, B.N.; Piolot, R.; Mankovsky, O.L.; Ziegler, D. Impairment of cerebral autoregulation in diabetic patients with cardiovascular autonomic neuropathy and orthostatic hypotension. Diabet. Med. 2003, 20, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Huq, R.; Philbey, C.E.; Mistri, A.K.; Panerai, R.B.; Robinson, T.G. Dynamic cerebral autoregulation assessed by respiratory manoeuvres in non-insulin-treated Type 2 diabetes mellitus. Diabet. Med. 2012, 29, 609–613. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-S.; Davis, S.C.A.T.; Truijen, J.; Stok, W.J.; Secher, N.H.; Lieshout, J.J.V. Intensive Blood Pressure Control Affects Cerebral Blood Flow in Type 2 Diabetes Mellitus Patients. Hypertension 2011, 57, 738–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pendlebury, S.T.; Rothwell, P.M. Prevalence, incidence, and factors associated with pre-stroke and post-stroke dementia: A systematic review and meta-analysis. Lancet Neurol. 2009, 8, 1006–1018. [Google Scholar] [CrossRef]
- Dad, T.; Weiner, D.E. Stroke and Chronic Kidney Disease: Epidemiology, Pathogenesis, and Management Across Kidney Disease Stages. Semin. Nephrol. 2015, 35, 311–322. [Google Scholar] [CrossRef] [Green Version]
- Ghoshal, S.; Freedman, B.I. Mechanisms of Stroke in Patients with Chronic Kidney Disease. Am. J. Nephrol. 2019, 50, 229–239. [Google Scholar] [CrossRef]
- Sedaghat, S.; Vernooij, M.W.; Loehrer, E.; Mattace-Raso, F.U.; Hofman, A.; van der Lugt, A.; Franco, O.H.; Dehghan, A.; Ikram, M.A. Kidney Function and Cerebral Blood Flow: The Rotterdam Study. J. Am. Soc. Nephrol. 2016, 27, 715–721. [Google Scholar] [CrossRef] [Green Version]
- Schiller, A.; Covic, A. Kidney and brain—A renal perspective of ‘Les Liaisons Dangereuses’. Nephrol. Dial. Transplant. 2010, 25, 1370–1373. [Google Scholar] [CrossRef] [Green Version]
- Caldas, J.R.; Panerai, R.B.; Haunton, V.J.; Almeida, J.P.; Ferreira, G.S.R.; Camara, L.; Nogueira, R.C.; Bor-Seng-Shu, E.; Oliveira, M.L.; Groehs, R.R.V.; et al. Cerebral blood flow autoregulation in ischemic heart failure. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2017, 312, R108–R113. [Google Scholar] [CrossRef] [Green Version]
- Adelborg, K.; Szépligeti, S.; Sundbøll, J.; Horváth-Puhó, E.; Henderson, V.W.; Ording, A.; Pedersen, L.; Sørensen, H.T. Risk of Stroke in Patients with Heart Failure. Stroke 2017, 48, 1161–1168. [Google Scholar] [CrossRef]
- Witt, B.J.; Brown, R.D.; Jacobsen, S.J.; Weston, S.A.; Ballman, K.V.; Meverden, R.A.; Roger, V.L. Ischemic stroke after heart failure: A community-based study. Am. Heart J. 2006, 152, 102–109. [Google Scholar] [CrossRef]
- Castro, P.; Serrador, J.; Rocha, I.; Chaves, P.C.; Sorond, F.; Azevedo, E. Heart failure patients have enhanced cerebral autoregulation response in acute ischemic stroke. J. Thromb. Thrombolysis 2020, 50. [Google Scholar] [CrossRef]
- Georgiadis, D.; Sievert, M.; Cencetti, S.; Uhlmann, F.; Krivokuca, M.; Zierz, S.; Werdan, K. Cerebrovascular reactivity is impaired in patients with cardiac failure. Eur. Heart J. 2000, 21, 407–413. [Google Scholar] [CrossRef] [Green Version]
- Caldas, J.R.; Panerai, R.B.; Salinet, A.M.; Seng-Shu, E.; Ferreira, G.S.R.; Camara, L.; Passos, R.H.; Galas, F.R.B.G.; Almeida, J.P.; Nogueira, R.C.; et al. Dynamic cerebral autoregulation is impaired during submaximal isometric handgrip in patients with heart failure. Am. J. Physiol. Heart Circ. Physiol. 2018, 315, H254–H261. [Google Scholar] [CrossRef]
- Liljehult, J.; Christensen, T.; Christensen, K.B. Early Prediction of One-Year Mortality in Ischemic and Haemorrhagic Stroke. J. Stroke Cerebrovasc. Dis. Off. J. Natl. Stroke Assoc. 2020, 29, 104667. [Google Scholar] [CrossRef]
- Andersen, K.K.; Andersen, Z.J.; Olsen, T.S. Predictors of early and late case-fatality in a nationwide Danish study of 26,818 patients with first-ever ischemic stroke. Stroke 2011, 42, 2806–2812. [Google Scholar] [CrossRef] [Green Version]
- Yang, D.; Cabral, D.; Gaspard, E.N.; Lipton, R.B.; Rundek, T.; Derby, C.A. Cerebral Hemodynamics in the Elderly: A Transcranial Doppler Study in the Einstein Aging Study Cohort. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2016, 35, 1907–1914. [Google Scholar] [CrossRef] [Green Version]
- De Vis, J.B.; Hendrikse, J.; Bhogal, A.; Adams, A.; Kappelle, L.J.; Petersen, E.T. Age-Related changes in brain hemodynamics: A calibrated MRI study. Hum. Brain Mapp. 2015, 36, 3973–3987. [Google Scholar] [CrossRef]
- Smirl, J.D.; Hoffman, K.; Tzeng, Y.C.; Hansen, A.; Ainslie, P.N. Relationship between blood pressure and cerebral blood flow during supine cycling: Influence of aging. J. Appl. Physiol. 2016, 120, 552–563. [Google Scholar] [CrossRef] [Green Version]
- Patel, N.; Panerai, R.B.; Haunton, V.; Katsogridakis, E.; Saeed, N.P.; Salinet, A.; Brodie, F.; Syed, N.; D’Sa, S.; Robinson, T.G. The Leicester cerebral haemodynamics database: Normative values and the influence of age and sex. Physiol. Meas. 2016, 37, 1485–1498. [Google Scholar] [CrossRef] [Green Version]
- Sandset, E.C.; Ferretti, M.T. Sex and gender differences in stroke-The need for individualised follow-up. Eur. J. Neurol. 2021, 28, 365–366. [Google Scholar] [CrossRef]
- Di Carlo, A.; Lamassa, M.; Baldereschi, M.; Pracucci, G.; Basile, A.M.; Wolfe, C.D.; Giroud, M.; Rudd, A.; Ghetti, A.; Inzitari, D. Sex differences in the clinical presentation, resource use, and 3-month outcome of acute stroke in Europe: Data from a multicenter multinational hospital-based registry. Stroke 2003, 34, 1114–1119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deegan, B.M.; Sorond, F.A.; Galica, A.; Lipsitz, L.A.; O’Laighin, G.; Serrador, J.M. Elderly women regulate brain blood flow better than men do. Stroke 2011, 42, 1988–1993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madureira, J.; Castro, P.; Azevedo, E. Demographic and Systemic Hemodynamic Influences in Mechanisms of Cerebrovascular Regulation in Healthy Adults. J. Stroke Cerebrovasc. Dis. Off. J. Natl. Stroke Assoc. 2017, 26, 500–508. [Google Scholar] [CrossRef] [PubMed]
- Beishon, L.; Minhas, J.S.; Nogueira, R.; Castro, P.; Budgeon, C.; Aries, M.; Payne, S.; Robinson, T.G.; Panerai, R.B. INFOMATAS multi-center systematic review and meta-analysis individual patient data of dynamic cerebral autoregulation in ischemic stroke. Int. J. Stroke 2020, 15, 807–812. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nogueira, R.C.; Beishon, L.; Bor-Seng-Shu, E.; Panerai, R.B.; Robinson, T.G. Cerebral Autoregulation in Ischemic Stroke: From Pathophysiology to Clinical Concepts. Brain Sci. 2021, 11, 511. https://doi.org/10.3390/brainsci11040511
Nogueira RC, Beishon L, Bor-Seng-Shu E, Panerai RB, Robinson TG. Cerebral Autoregulation in Ischemic Stroke: From Pathophysiology to Clinical Concepts. Brain Sciences. 2021; 11(4):511. https://doi.org/10.3390/brainsci11040511
Chicago/Turabian StyleNogueira, Ricardo C., Lucy Beishon, Edson Bor-Seng-Shu, Ronney B. Panerai, and Thompson G. Robinson. 2021. "Cerebral Autoregulation in Ischemic Stroke: From Pathophysiology to Clinical Concepts" Brain Sciences 11, no. 4: 511. https://doi.org/10.3390/brainsci11040511