
Gait and Balance Changes with Investigational Peripheral Nerve Cell Therapy during Deep Brain Stimulation in People with Parkinson’s Disease

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Surgical implantation
2.2. Clinical Testing
2.3. Gait Data Collection
2.4. Outcome Variables
3. Results
3.1. Changes in Clinical Scales 6 and 24 Months after APNG Implantation
3.2. Gait Measures for the Cohort
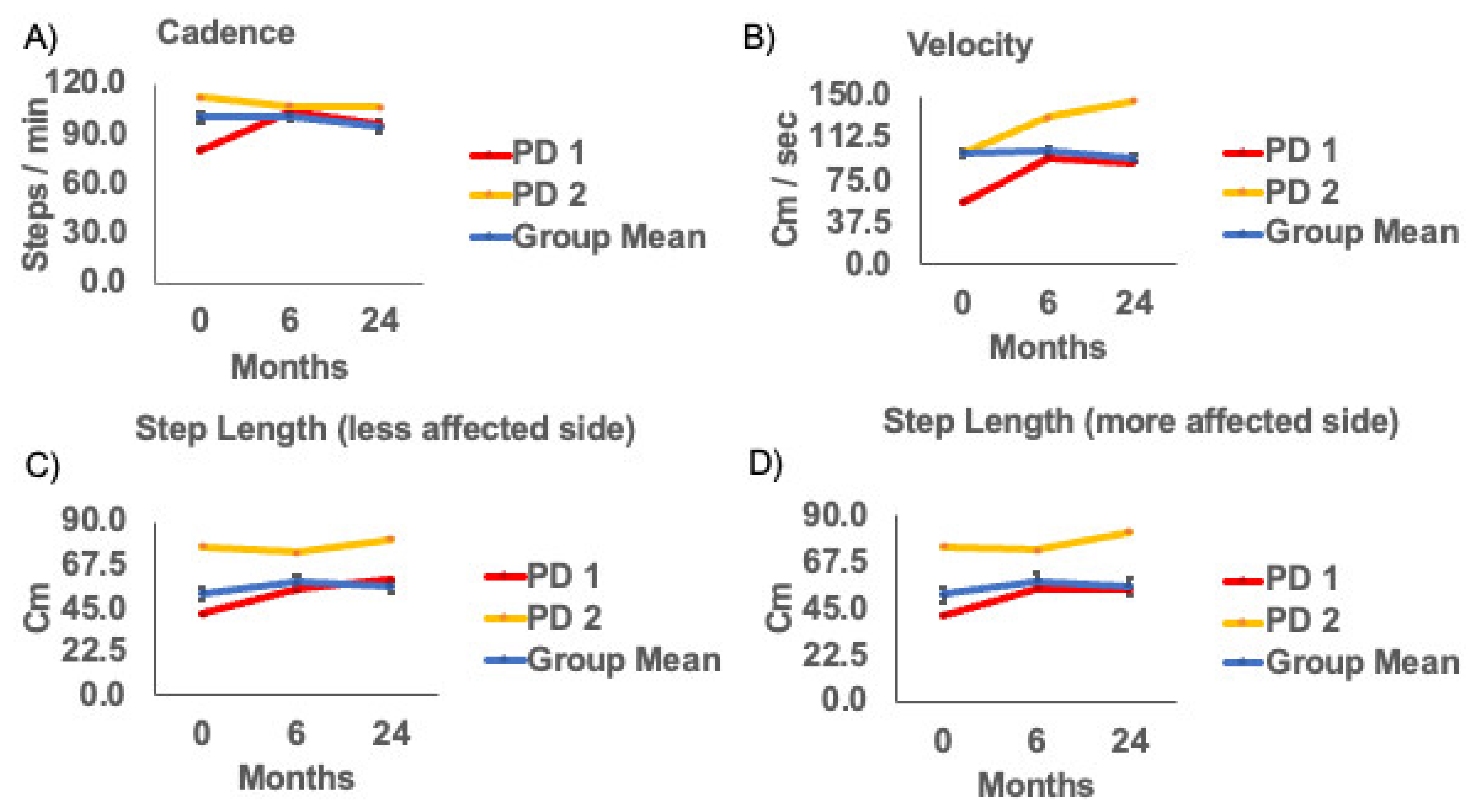
3.3. Gait Measures for Subjects with Deficits in Gait and Overall Disease Severity
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethical Compliance Statement
References
- Delamarre, A.; Meissner, W.G. Epidemiology, environmental risk factors and genetics of Parkinson’s disease. Presse Med. 2017, 46, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Georgem, J.L.; Mok, S.; Moses, D.; Wilkins, S.; Bush, A.I.; Cherny, R.A.; Finkelstein, D.I. Targeting the progression of Parkinson’s disease. Curr. Neuropharmacol. 2009, 7, 9–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morrish, P.K.; Rakshi, J.S.; Bailey, D.L.; Sawle, G.V.; Brooks, D.J. Measuring the rate of progression and estimating the preclinical period of Parkinson’s disease with [18F]dopa PET. J. Neurol. Neurosurg. Psychiatry 1998, 64, 314–319. [Google Scholar] [CrossRef] [PubMed]
- George, R.J.S.; Nutt, J.G.; Burchiel, K.J.; Horak, F.B. A meta-regression of the long-term effects of deep brain stimulation on balance and gait in PD. Neurology 2010, 75, 1292–1299. [Google Scholar] [CrossRef] [Green Version]
- Mirelman, A.; Bonato, P.; Camicioli, R.; Ellis, T.D.; Giladi, N.; Hamilton, J.L.; Hass, C.J.; Hausdorff, J.M.; Pelosin, E.; Almeida, Q.J. Gait impairments in Parkinson’s disease. Lancet Neurol. 2019, 18, 697–708. [Google Scholar] [CrossRef]
- Collomb-Clerc, A.; Welter, M.L. Effects of deep brain stimulation on balance and gait in patients with Parkinson’s disease: A systematic neurophysiological review. Neurophysiol. Clin. 2015, 45, 371–388. [Google Scholar] [CrossRef] [Green Version]
- Krack, P.; Batir, A.; Van Blercom, N.; Chabardes, S.; Fraix, V.; Ardouin, C.; Koudsie, A.; Limousin, P.D.; Benazzouz, A.; LeBas, J.F.; et al. Five-year follow-up of bilateral stimulation of the subthalamic nucleus in advanced Parkinson’s disease. N. Engl. J. Med. 2003, 349, 1925–1934. [Google Scholar] [CrossRef] [Green Version]
- van Horne, C.G.; Quintero, J.E.; Gurwell, J.A.; Wagner, R.P.; Slevin, J.T.; Gerhardt, G.A. Implantation of autologous peripheral nerve grafts into the substantia nigra of subjects with idiopathic Parkinson’s disease treated with bilateral STN DBS: A report of safety and feasibility. J. Neurosurg. 2017, 126, 1140–1147. [Google Scholar] [CrossRef] [Green Version]
- van Horne, C.G.; Quintero, J.E.; Slevin, J.T.; Anderson-Mooney, A.; Gurwell, J.A.; Welleford, A.S.; Lamm, J.R.; Wagner, R.P.; Gerhardt, G.A. Peripheral nerve grafts implanted into the substantia nigra in patients with Parkinson’s disease during deep brain stimulation surgery: 1-year follow-up study of safety, feasibility, and clinical outcome. J. Neurosurg. 2018, 129, 1550–1561. [Google Scholar] [CrossRef]
- Jessen, K.R.; Arthur-Farraj, P. Repair Schwann cell update: Adaptive reprogramming, EMT, and stemness in regenerating nerves. Glia 2019, 67, 421–437. [Google Scholar] [CrossRef]
- Jessen, K.R.; Mirsky, R. The repair Schwann cell and its function in regenerating nerves. J. Physiol. 2016, 594, 3521–3531. [Google Scholar] [CrossRef] [Green Version]
- Jessen, K.R.; Mirsky, R. The Success and Failure of the Schwann Cell Response to Nerve Injury. Front Cell Neurosci. 2019, 13, 33. [Google Scholar] [CrossRef] [PubMed]
- Jessen, K.R.; Mirsky, R.; Lloyd, A.C. Schwann Cells: Development and Role in Nerve Repair. Cold Spring Harb. Perspect. Biol. 2015, 7, a020487. [Google Scholar] [CrossRef] [PubMed]
- Fontana, X.; Hristova, M.; Da Costa, C.; Patodia, S.; Thei, L.; Makwana, M.; Spencer-Dene, B.; Latouche, M.; Mirsky, R.; Jessen, K.R.; et al. c-Jun in Schwann cells promotes axonal regeneration and motoneuron survival via paracrine signaling. J. Cell Biol. 2012, 198, 127–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naveilhan, P.; ElShamy, W.M.; Ernfors, P. Differential regulation of mRNAs for GDNF and its receptors Ret and GDNFR alpha after sciatic nerve lesion in the mouse. Eur. J. Neurosci. 1997, 9, 1450–1460. [Google Scholar] [CrossRef]
- Heumann, R.; Korsching, S.; Bandtlow, C.; Thoenen, H. Changes of nerve growth factor synthesis in nonneuronal cells in response to sciatic nerve transection. J. Cell Biol. 1987, 104, 1623–1631. [Google Scholar] [CrossRef] [Green Version]
- Brushart, T.M.; Aspalter, M.; Griffin, J.W.; Redett, R.; Hameed, H.; Zhou, C.; Wright, M.; Vyas, A.; Höke, A. Schwann cell phenotype is regulated by axon modality and central–peripheral location, and persists in vitro. Exp. Neurol. 2013, 247, 272–281. [Google Scholar] [CrossRef] [Green Version]
- Meyer, M.; Matsuoka, I.; Wetmore, C.; Olson, L.; Thoenen, H. Enhanced synthesis of brain-derived neurotrophic factor in the lesioned peripheral nerve: Different mechanisms are responsible for the regulation of BDNF and NGF mRNA. J. Cell Biol. 1992, 119, 45–54. [Google Scholar] [CrossRef] [Green Version]
- Welleford, A.S.; Quintero, J.E.; El Seblani, N.; Blalock, E.; Gunewardena, S.; Shapiro, S.M.; Riordan, S.M.; Huettl, P.; Guduru, Z.; Stanford, J.A.; et al. RNA Sequencing of Human Peripheral Nerve in Response to Injury: Distinctive Analysis of the Nerve Repair Pathways. Cell Transplant. 2020, 29, 963689720926157. [Google Scholar] [CrossRef] [PubMed]
- Allert, N.; Volkmann, J.; Dotse, S.; Hefter, H.; Sturm, V.; Freund, H.J. Effects of bilateral pallidal or subthalamic stimulation on gait in advanced Parkinson’s disease. Mov. Disord. 2001, 16, 1076–1085. [Google Scholar] [CrossRef]
- Faist, M.; Xie, J.; Kurz, D.; Berger, W.; Maurer, C.; Pollak, P.; Lücking, C.H. Effect of bilateral subthalamic nucleus stimulation on gait in Parkinson’s disease. Brain 2001, 124, 1590–1600. [Google Scholar] [CrossRef]
- Ferrarin, M.; Lopiano, L.; Rizzone, M.; Lanotte, M.; Bergamasco, B.; Recalcati, M.; Pedotti, A. Quantitative analysis of gait in Parkinson’s disease: A pilot study on the effects of bilateral sub-thalamic stimulation. Gait Posture 2002, 16, 135–148. [Google Scholar] [CrossRef]
- Ferrarin, M.; Rizzone, M.; Bergamasco, B.; Lanotte, M.; Recalcati, M.; Pedotti, A.; Lopiano, L. Effects of bilateral subthalamic stimulation on gait kinematics and kinetics in Parkinson’s disease. Exp. Brain Res. 2004, 160, 517–527. [Google Scholar] [CrossRef]
- Liu, W.; McIntire, K.; Kim, S.H.; Zhang, J.; Dascalos, S.; Lyons, K.E.; Pahwa, R. Quantitative assessments of the effect of bilateral subthalamic stimulation on multiple aspects of sensorimotor function for patients with Parkinson’s disease. Parkinsonism. Relat. Disord. 2005, 11, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Stolze, H.; Klebe, S.; Poepping, M.; Lorenz, D.; Herzog, J.; Hamel, W.; Schrader, B.; Raethjen, J.; Wenzelburger, R.; Mehdorn, H.M.; et al. Effects of bilateral subthalamic nucleus stimulation on parkinsonian gait. Neurology 2001, 57, 144–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, J.; Krack, P.; Benabid, A.-L.; Pollak, P. Effect of bilateral subthalamic nucleus stimulation on parkinsonian gait. J. Neurol. 2001, 248, 1068–1072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hausdorff, J.M.; Gruendlinger, L.; Scollins, L.; O’Herron, S.; Tarsy, D. Deep brain stimulation effects on gait variability in Parkinson’s disease. Mov. Disord. 2009, 24, 1688–1692. [Google Scholar] [CrossRef]
- Johnsen, E.L.; Mogensen, P.H.; Sunde, N.A.; Østergaard, K. Improved asymmetry of gait in Parkinson’s disease with DBS: Gait and postural instability in Parkinson’s disease treated with bilateral deep brain stimulation in the subthalamic nucleus. Mov. Disord. 2009, 24, 590–597. [Google Scholar] [CrossRef] [PubMed]
- Johnsen, E.L.; Sunde, N.; Mogensen, P.H.; Østergaard, K. MRI verified STN stimulation site-gait improvement and clinical outcome. Eur. J. Neurol. 2010, 17, 746–753. [Google Scholar] [CrossRef] [PubMed]
- Lubik, S.; Fogel, W.; Tronnier, V.; Krause, M.; König, J.; Jost, W.H. Gait analysis in patients with advanced Parkinson disease: Different or additive effects on gait induced by levodopa and chronic STN stimulation. J. Neural Transm. 2005, 113, 163–173. [Google Scholar] [CrossRef]
- Vallabhajosula, S.; Haq, I.U.; Hwynn, N.; Oyama, G.; Okun, M.; Tillman, M.D.; Hass, C.J. Low-frequency versus high-frequency subthalamic nucleus deep brain stimulation on postural control and gait in Parkinson’s disease: A quantitative study. Brain Stimul. 2015, 8, 64–75. [Google Scholar] [CrossRef] [PubMed]
- Defebvre, L.J.; Krystkowiak, P.; Blatt, J.L.; Duhamel, A.; Bourriez, J.L.; Périna, M.; Blond, S.; Guieu, J.D.; Destée, A. Influence of pallidal stimulation and levodopa on gait and preparatory postural adjustments in Parkinson’s disease. Mov. Disord. 2002, 17, 76–83. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| 0 months | 6 months | 24 months | F-Score, P, ηp2 | |
|---|---|---|---|---|
| UPDRS III | 37.6 (30.8−44.5) | 29.1 (23.4−34.7) a | 27.4 (21.3−33.6) b | F2, 26 = 9.43, p < 0.05, 0.42 |
| UPDRS III (Gait) | 1.3 (0.7−1.9) | 0.6 (0.32−1.0) | 0.9 (0.4−1.3) | F2, 26 = 3.34, p = 0.051, 0.21 |
| Hoehn and Yahr | 3.0 (2.6−3.4) | 2.6 (2.4−2.8) | 2.4 (2.1−2.6) b | F2, 26 = 4.59, p < 0.05, 0.26 |
| UPDRS III (Postural Stability) | 1.0 (0.5−1.5) | 0.8 (0.3−1.2) | 0.6 (0.2−1.1) | F2, 26 = 0.815, p = 0.45, 0.06 |
| 0 months | 6 months | 24 months | F-Score, P, ηp2 | |
|---|---|---|---|---|
| Cadence | 97.71 (90.84−104.59) | 101.19 (94.82−107.55) | 94.04 (85.22−102.86) | F2, 26= 2.05, p = 0.15, ηp2= 0.14 |
| Velocity | 82.58 (66.91−98.25) | 99.14 (84.32−113.96) | 89.72 (71.65−107.79) | F2, 26= 2.92, p = 0.07, ηp2 = 0.18 |
| Step Length(less affected side) | 52.55 (43.20−61.90) | 59.03 (52.11−65.95) | 56.55 (48.54−64.55) | F2, 26= 2.54, p = 0.1, ηp2 = 0.16 |
| Step Length(more affected side) | 51.43 (41.97−60.89) | 58.19 (50.72−65.66) | 55.86 (46.80−64.91) | F2, 26= 2.83, p = 0.08, ηp2 = 0.18 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gera, G.; Guduru, Z.; Yamasaki, T.; Gurwell, J.A.; Chau, M.J.; Krotinger, A.; Schmitt, F.A.; Slevin, J.T.; Gerhardt, G.A.; van Horne, C.; et al. Gait and Balance Changes with Investigational Peripheral Nerve Cell Therapy during Deep Brain Stimulation in People with Parkinson’s Disease. Brain Sci. 2021, 11, 500. https://doi.org/10.3390/brainsci11040500
Gera G, Guduru Z, Yamasaki T, Gurwell JA, Chau MJ, Krotinger A, Schmitt FA, Slevin JT, Gerhardt GA, van Horne C, et al. Gait and Balance Changes with Investigational Peripheral Nerve Cell Therapy during Deep Brain Stimulation in People with Parkinson’s Disease. Brain Sciences. 2021; 11(4):500. https://doi.org/10.3390/brainsci11040500
Chicago/Turabian StyleGera, Geetanjali, Zain Guduru, Tritia Yamasaki, Julie A. Gurwell, Monica J. Chau, Anna Krotinger, Frederick A. Schmitt, John T. Slevin, Greg A. Gerhardt, Craig van Horne, and et al. 2021. "Gait and Balance Changes with Investigational Peripheral Nerve Cell Therapy during Deep Brain Stimulation in People with Parkinson’s Disease" Brain Sciences 11, no. 4: 500. https://doi.org/10.3390/brainsci11040500