
Breakdowns in Informativeness of Naturalistic Speech Production in Primary Progressive Aphasia

 ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Speech Sample Collection
2.3. Speech Sample Transcription and Basic Coding
2.4. Content Unit (CUs) Coding
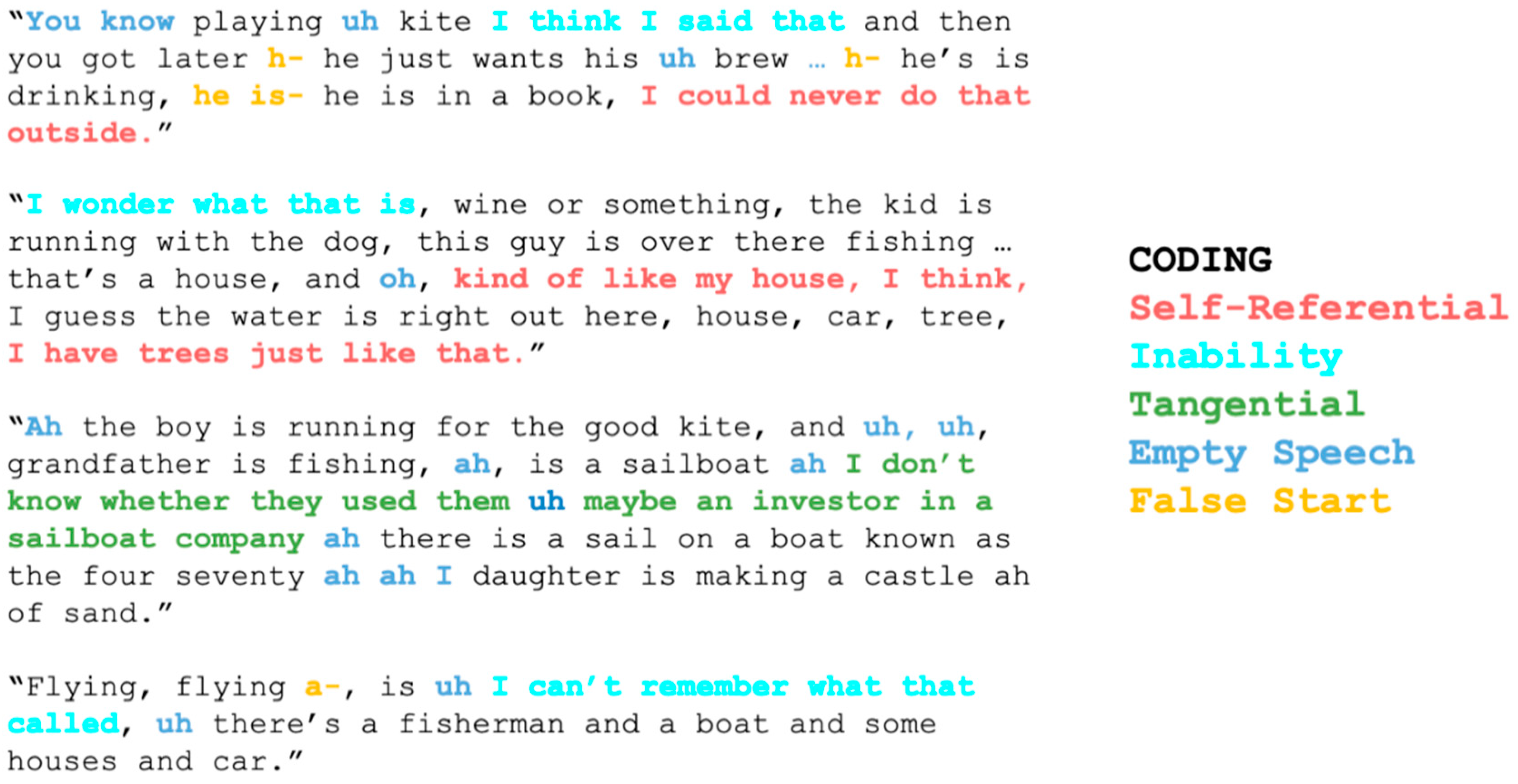
2.5. Self-Referential, Empty, or Other Atypical Speech
2.6. Statistical Analysis
3. Results
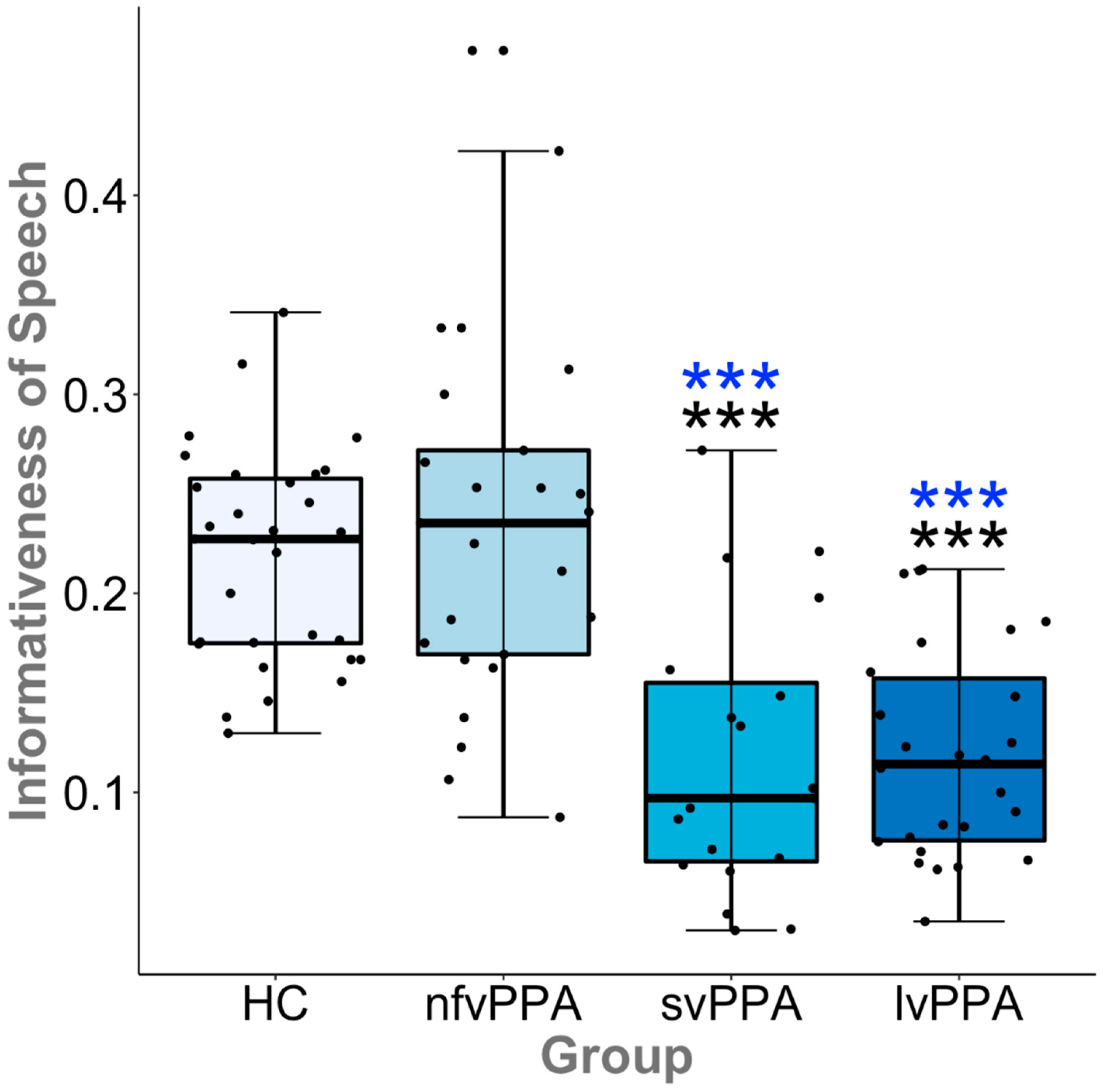
3.1. CUs and Informativeness
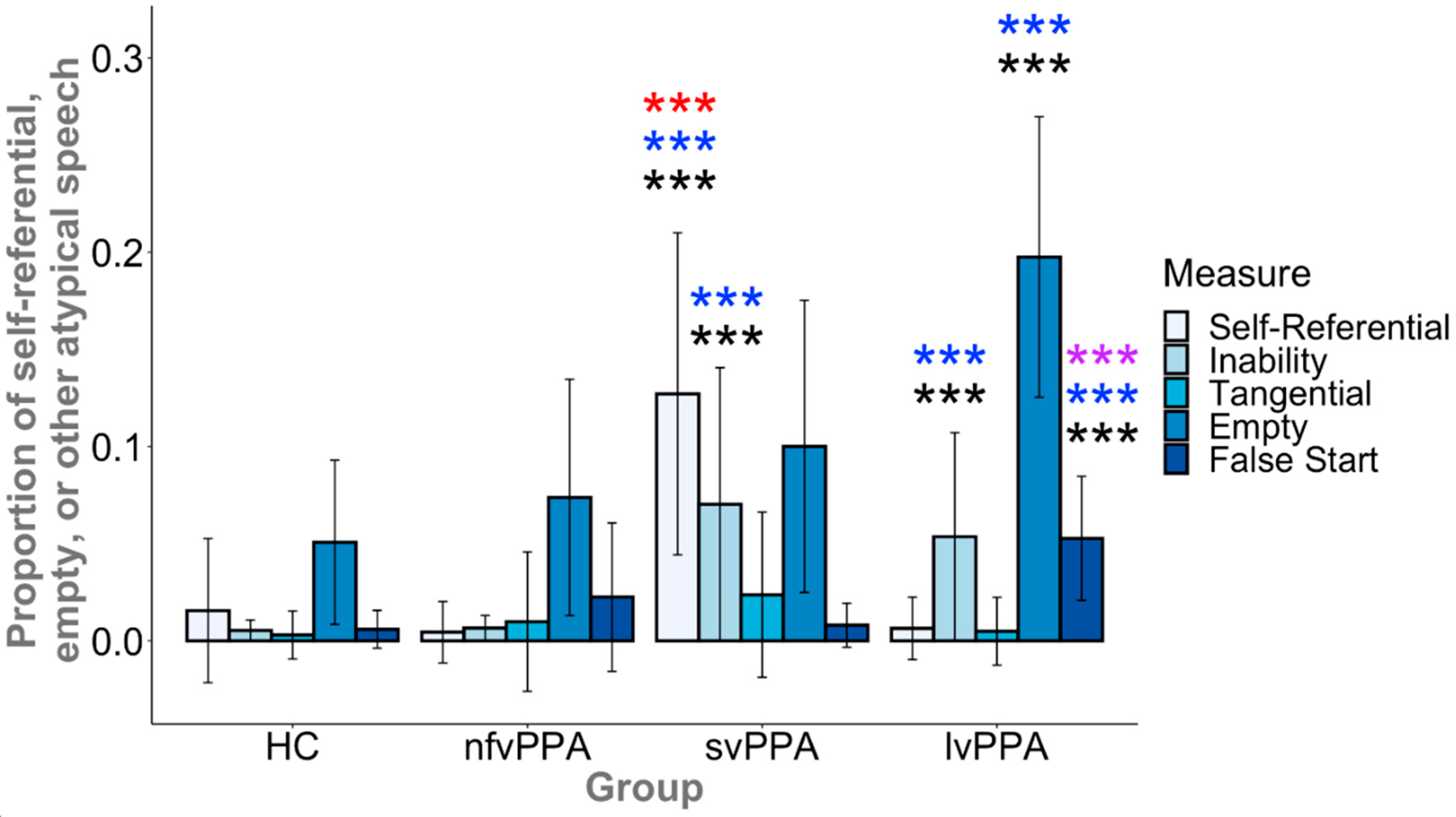
3.2. Self-Referential, Empty, or Other Atypical Speech
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Participant | Sex | Age | Highest Educational Degree | CDR: Language | PASS Sum of Boxes |
|---|---|---|---|---|---|---|
| Semantic variant PPA | svPPA 1 | F | 68 | Master’s | 1 | 6 |
| svPPA 2 | F | 62 | Bachelor’s | 1 | 3 | |
| svPPA 3 | F | 53 | Bachelor’s | 0.5 | 3 | |
| svPPA 4 | F | 64 | High School | 0.5 | 3.5 | |
| svPPA 5 | M | 54 | Master’s | 0.5 | 1.5 | |
| svPPA 6 | M | 59 | Bachelor’s | 0.5 | 3 | |
| svPPA 7 | M | 83 | Bachelor’s | 0.5 | 5 | |
| svPPA 8 | F | 63 | Bachelor’s | 1 | 4.5 | |
| svPPA 9 | M | 80 | Bachelor’s | 0.5 | 2 | |
| svPPA 10 | F | 63 | High School | 0.5 | 4 | |
| svPPA 11 | F | 70 | Master’s | 0.5 | 4.5 | |
| svPPA 12 | M | 65 | Bachelor’s | 1 | 5 | |
| svPPA 13 | M | 81 | Bachelor’s | 0.5 | 3 | |
| svPPA 14 | M | 64 | Doctorate | 1 | 5 | |
| svPPA 15 | F | 54 | Doctorate | 1 | 3 | |
| svPPA 16 | F | 74 | Bachelor’s | 0.5 | 2.5 | |
| svPPA 17 | F | 72 | High School | 0.5 | 4 | |
| svPPA 18 | F | 65 | Bachelor’s | 1 | 3 | |
| svPPA 19 | M | 68 | Master’s | 1 | 1 | |
| Logopenic variant PPA | lvPPA 1 | M | 68 | Bachelor’s | 1 | 5 |
| lvPPA 2 | F | 68 | High School | 0.5 | 3.5 | |
| lvPPA 3 | M | 79 | High School | 0.5 | 3 | |
| lvPPA 4 | M | 71 | Master’s | 0.5 | 0.5 | |
| lvPPA 5 | M | 71 | Master’s | 0.5 | 3.5 | |
| lvPPA 6 | M | 79 | Master’s | 1 | 3.5 | |
| lvPPA 7 | F | 59 | Bachelor’s | 1 | 6 | |
| lvPPA 8 | F | 70 | Associate’s | 1 | 5 | |
| lvPPA 9 | F | 59 | Master’s | 1 | 6 | |
| lvPPA 10 | F | 64 | Bachelor’s | 0.5 | 5 | |
| lvPPA 11 | M | 71 | Master’s | 1 | 3.5 | |
| lvPPA 12 | M | 72 | High School | 1 | 5 | |
| lvPPA 13 | F | 53 | Bachelor’s | 0.5 | 4.5 | |
| lvPPA 14 | F | 68 | High School | 1 | 3 | |
| lvPPA 15 | F | 75 | High School | 0.5 | 5 | |
| lvPPA 16 | M | 79 | Bachelor’s | 0.5 | 4 | |
| lvPPA 17 | F | 70 | Bachelor’s | 0.5 | 3.5 | |
| lvPPA 18 | F | 69 | Bachelor’s | 0.5 | 3 | |
| lvPPA 19 | M | 75 | Bachelor’s | 1 | 5 | |
| lvPPA 20 | M | 76 | Master’s | 0.5 | 3.5 | |
| lvPPA 21 | F | 78 | Master’s | 0.5 | 5 | |
| lvPPA 22 | F | 55 | High School | 0.5 | 5 | |
| lvPPA 23 | M | 69 | Doctorate | 0.5 | 3 | |
| lvPPA 24 | M | 72 | Master’s | 1 | 4 | |
| lvPPA 25 | M | 73 | Bachelor’s | 1 | 5 | |
| lvPPA 26 | M | 69 | Bachelor’s | 0.5 | 2 | |
| Non-fluent variant PPA | nfvPPA 1 | F | 72 | Bachelor’s | 0.5 | 3.5 |
| nfvPPA 2 | M | 64 | Bachelor’s | 0.5 | 5.5 | |
| nfvPPA 3 | F | 69 | Master’s | 1 | 3 | |
| nfvPPA 4 | F | 74 | Bachelor’s | 0.5 | 5 | |
| nfvPPA 5 | M | 60 | Bachelor’s | 1 | 5 | |
| nfvPPA 6 | M | 63 | Bachelor’s | 0.5 | 4 | |
| nfvPPA 7 | M | 70 | Doctorate | 0.5 | 2 | |
| nfvPPA 8 | F | 69 | Master’s | 1 | 3 | |
| nfvPPA 9 | F | 63 | High School | 0.5 | 4 | |
| nfvPPA 10 | M | 68 | Bachelor’s | 1 | 4 | |
| nfvPPA 11 | F | 75 | Doctorate | 0.5 | 2 | |
| nfvPPA 12 | M | 67 | Bachelor’s | 0.5 | 3.5 | |
| nfvPPA 13 | F | 65 | Bachelor’s | 0.5 | 5.5 | |
| nfvPPA 14 | F | 79 | High School | 0.5 | 5.5 | |
| nfvPPA 15 | M | 55 | Master’s | 0.5 | 3 | |
| nfvPPA 16 | M | 80 | Master’s | 0.5 | 3 | |
| nfvPPA 17 | F | 71 | Master’s | 0.5 | 1 | |
| nfvPPA 18 | F | 78 | High School | 0.5 | 3.5 | |
| nfvPPA 19 | M | 69 | Bachelor’s | 1 | 5 | |
| nfvPPA 20 | F | 75 | High School | 0.5 | 3.5 | |
| nfvPPA 21 | F | 79 | High School | 0.5 | 5 | |
| nfvPPA 22 | F | 82 | High School | 1 | 6 | |
| nfvPPA 23 | M | 77 | High School | 0.5 | 3 | |
| nfvPPA 24 | F | 74 | High School | 1 | 4 | |
| nfvPPA 25 | F | 62 | Master’s | 1 | 3 | |
| Healthy Controls | HC 1 | F | 61 | Bachelor’s | ||
| HC 2 | F | 61 | High School | |||
| HC 3 | M | 53 | Bachelor’s | |||
| HC 4 | F | 50 | High School | |||
| HC 5 | M | 52 | Bachelor’s | |||
| HC 6 | M | 51 | Bachelor’s | |||
| HC 7 | M | 68 | Bachelor’s | |||
| HC 8 | F | 71 | Bachelor’s | |||
| HC 9 | F | 71 | Bachelor’s | |||
| HC 10 | M | 62 | High School | |||
| HC 11 | F | 71 | Bachelor’s | |||
| HC 12 | F | 68 | Bachelor’s | |||
| HC 13 | M | 69 | Bachelor’s | |||
| HC 14 | M | 53 | Bachelor’s | |||
| HC 15 | F | 55 | Bachelor’s | |||
| HC 16 | M | 68 | Bachelor’s | |||
| HC 17 | F | 66 | High School | |||
| HC 18 | M | 65 | Bachelor’s | |||
| HC 19 | F | 62 | Bachelor’s | |||
| HC 20 | F | 66 | Bachelor’s | |||
| HC 21 | M | 59 | Bachelor’s | |||
| HC 22 | F | 57 | High School | |||
| HC 23 | M | 54 | Bachelor’s | |||
| HC 24 | F | 60 | Bachelor’s | |||
| HC 25 | F | 72 | High School | |||
| HC 26 | M | 73 | Bachelor’s | |||
| HC 27 | F | 55 | High School | |||
| HC 28 | F | 65 | Bachelor’s | |||
| HC 29 | F | 63 | Bachelor’s | |||
| HC 30 | M | 76 | High School | |||
| HC 31 | M | 83 | Bachelor’s |
Appendix B
| Group | 0 pt. | 1 pt. | 2 pt. | 3 pt. | 4 pt. | No. Participants Changed |
|---|---|---|---|---|---|---|
| HC | 7 | 9 | 11 | 2 | 2 | 24 |
| lvPPA | 18 | 7 | 0 | 1 | 0 | 8 |
| nfvPPA | 17 | 4 | 4 | 0 | 0 | 8 |
| svPPA | 10 | 6 | 2 | 1 | 0 | 9 |
Appendix C
| Group | Self-Referential Statements | SD | Ability Statements | SD | Tangential Statements | SD | Empty Speech | SD | False Starts | SD |
|---|---|---|---|---|---|---|---|---|---|---|
| HC | 0.016 | 0.037 | 0.005 | 0.013 | 0.003 | 0.012 | 0.051 | 0.042 | 0.006 | 0.009 |
| lvPPA | 0.006 | 0.016 | 0.053 | 0.056 | 0.005 | 0.017 | 0.198 | 0.072 | 0.053 | 0.032 |
| nfvPPA | 0.004 | 0.016 | 0.007 | 0.019 | 0.009 | 0.036 | 0.074 | 0.061 | 0.023 | 0.038 |
| svPPA | 0.127 | 0.183 | 0.070 | 0.067 | 0.024 | 0.043 | 0.100 | 0.075 | 0.008 | 0.011 |
References
- Mesulam, M.-M. Primary Progressive Aphasia—A Language-Based Dementia. N. Engl. J. Med. 2003, 349, 1535–1542. [Google Scholar] [CrossRef] [PubMed]
- Neary, D.; Snowden, J.S.; Gustafson, L.; Passant, U.; Stuss, D.; Black, S.; Freedman, M.; Kertesz, A.; Robert, P.H.; Albert, M.; et al. Frontotemporal lobar degeneration: A consensus on clinical diagnostic criteria. Neurology 1998, 51, 1546–1554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mesulam, M.-M. Primary progressive aphasia. Ann. Neurol. 2001, 49, 425–432. [Google Scholar] [CrossRef]
- Gorno-Tempini, M.L.; Dronkers, N.F.; Rankin, K.P.; Ms, J.M.O.; Ba, L.P.; Rosen, H.J.; Johnson, J.K.; Weiner, M.W.; Miller, B.L. Cognition and anatomy in three variants of primary progressive aphasia. Ann. Neurol. 2004, 55, 335–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorno-Tempini, M.L.; Brambati, S.M.; Ginex, V.; Ogar, J.; Dronkers, N.F.; Marcone, A.; Perani, D.; Garibotto, V.; Cappa, S.F.; Miller, B.L. The logopenic/phonological variant of primary progressive aphasia. Neurology 2008, 71, 1227–1234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorno-Tempini, M.L.; Hillis, A.E.; Weintraub, S.; Kertesz, A.; Mendez, M.; Cappa, S.F.; Ogar, J.M.; Rohrer, J.D.; Black, S.; Boeve, B.F.; et al. Classification of primary progressive aphasia and its variants. Neurology 2011, 76, 1006–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sapolsky, D.; Domoto-Reilly, K.; Negreira, A.; Brickhouse, M.; McGinnis, S.; Dickerson, B.C. Monitoring progression of primary progressive aphasia: Current approaches and future directions. Neurodegener. Dis. Manag. 2011, 1, 43–55. [Google Scholar] [CrossRef] [Green Version]
- Grossman, M. Linguistic Aspects of Primary Progressive Aphasia. Annu. Rev. Linguist. 2018, 4, 377–403. [Google Scholar] [CrossRef]
- Beales, A.; Whitworth, A.; Cartwright, J.; Panegyres, P.K.; Kane, R.T. Determining stability in connected speech in primary progressive aphasia and Alzheimer’s disease. Int. J. Speech Lang. Pathol. 2018, 20, 361–370. [Google Scholar] [CrossRef]
- Sapolsky, D.; Domoto-Reilly, K.; Dickerson, B.C. Use of the Progressive Aphasia Severity Scale (PASS) in monitoring speech and language status in PPA. Aphasiology 2014, 28, 993–1003. [Google Scholar] [CrossRef]
- Grasso, S.M.; Henry, M.L. Assessment of Individuals with Primary Progressive Aphasia. Semin. Speech Lang. 2018, 39, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, E.; Ferguson, A. Language, meaning, context, and functional communication. Aphasiology 2010, 24, 480–496. [Google Scholar] [CrossRef]
- Linnik, A.; Bastiaanse, R.; Höhle, B. Discourse production in aphasia: A current review of theoretical and methodological challenges. Aphasiology 2016, 30, 765–800. [Google Scholar] [CrossRef]
- Doedens, W.J.; Meteyard, L. Measures of functional, real-world communication for aphasia: A critical review. Aphasiology 2019, 34, 492–514. [Google Scholar] [CrossRef]
- Volkmer, A.; Spector, A.; Meitanis, V.; Warren, J.D.; Beeke, S. Effects of functional communication interventions for people with primary progressive aphasia and their caregivers: A systematic review. Aging Ment. Health 2020, 24, 1381–1393. [Google Scholar] [CrossRef]
- Pritchard, M.; Hilari, K.; Cocks, N.; Dipper, L. Reviewing the quality of discourse information measures in aphasia. Int. J. Lang. Commun. Disord. 2017, 52, 689–732. [Google Scholar] [CrossRef]
- Wilson, S.M.; Henry, M.L.; Besbris, M.; Ogar, J.M.; Dronkers, N.F.; Jarrold, W.; Miller, B.L.; Gorno-Tempini, M.L. Connected speech production in three variants of primary progressive aphasia. Brain 2010, 133, 2069–2088. [Google Scholar] [CrossRef] [Green Version]
- Ash, S.; Evans, E.; O’Shea, J.; Powers, J.; Boller, A.; Weinberg, D.; Haley, J.; McMillan, C.; Irwin, D.J.; Rascovsky, K.; et al. Differentiating primary progressive aphasias in a brief sample of connected speech. Neurology 2013, 81, 329–336. [Google Scholar] [CrossRef] [Green Version]
- Bryant, L.; Ferguson, A.; Spencer, E. Linguistic analysis of discourse in aphasia: A review of the literature. Clin. Linguist. Phon. 2016, 30, 489–518. [Google Scholar] [CrossRef]
- Boschi, V.; Catricalà, E.; Consonni, M.; Chesi, C.; Moro, A.; Cappa, S.F. Connected Speech in Neurodegenerative Language Disorders: A Review. Front. Psychol. 2017, 8, 269. [Google Scholar] [CrossRef] [Green Version]
- Berube, S.; Nonnemacher, J.; Demsky, C.; Glenn, S.; Saxena, S.; Wright, A.; Tippett, D.C.; Hillis, A. Stealing Cookies in the Twenty-First Century: Measures of Spoken Narrative in Healthy Versus Speakers With Aphasia. Am. J. Speech Lang. Pathol. 2019, 28, 321–329. [Google Scholar] [CrossRef]
- Yorkston, K.M.; Beukelman, D.R. An Analysis of Connected Speech Samples of Aphasic and Normal Speakers. J. Speech Hear. Disord. 1980, 45, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Fraser, K.C.; Meltzer, J.A.; Graham, N.L.; Leonard, C.; Hirst, G.; Black, S.E.; Rochon, E. Automated classification of primary progressive aphasia subtypes from narrative speech transcripts. Cortex 2014, 55, 43–60. [Google Scholar] [CrossRef]
- Ash, S.; Grossman, M. Why study connected speech production? In Cognitive Neuroscience of Natural Language Use; Willems, R.M., Ed.; Cambridge University Press: Cambridge, UK, 2015; pp. 29–58. [Google Scholar]
- Meteyard, L.; Patterson, K.E. The relation between content and structure in language production: An analysis of speech errors in semantic dementia. Brain Lang. 2009, 110, 121–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sajjadi, S.A.; Patterson, K.; Tomek, M.; Nestor, P.J. Abnormalities of connected speech in the non-semantic variants of primary progressive aphasia. Aphasiology 2012, 26, 1219–1237. [Google Scholar] [CrossRef]
- Ash, S.; Moore, P.; Antani, S.; McCawley, G.; Work, M.; Grossman, M. Trying to tell a tale: Discourse impairments in progressive aphasia and frontotemporal dementia. Neurology 2006, 66, 1405–1413. [Google Scholar] [CrossRef] [PubMed]
- Graham, N.L.; Patterson, K.; Hodges, J.R. When More Yields Less: Speaking and Writing Deficits in Nonfluent Progressive Aphasia. Neurocase 2004, 10, 141–155. [Google Scholar] [CrossRef]
- Rogalski, E.; Cobia, D.; Harrison, T.M.; Wieneke, C.; Thompson, C.K.; Weintraub, S.; Mesulam, M.-M. Anatomy of Language Impairments in Primary Progressive Aphasia. J. Neurosci. 2011, 31, 3344–3350. [Google Scholar] [CrossRef] [Green Version]
- Cordella, C.; Dickerson, B.C.; Quimby, M.; Yunusova, Y.; Green, J.R. Slowed articulation rate is a sensitive diagnostic marker for identifying non-fluent primary progressive aphasia. Aphasiology 2017, 31, 241–260. [Google Scholar] [CrossRef]
- Cordella, C.; Quimby, M.; Touroutoglou, A.; Brickhouse, M.; Dickerson, B.C.; Green, J.R. Quantification of motor speech impairment and its anatomic basis in primary progressive aphasia. Neurology 2019, 92, e1992–e2004. [Google Scholar] [CrossRef] [Green Version]
- Knibb, J.A.; Woollams, A.M.; Hodges, J.R.; Patterson, K. Making sense of progressive non-fluent aphasia: An analysis of conversational speech. Brain 2009, 132, 2734–2746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knopman, D.S.; Weintraub, S.; Pankratz, V.S. Language and behavior domains enhance the value of the clinical dementia rating scale. Alzheimer’s Dement. 2011, 7, 293–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kertesz, A. WAB-R: Western Aphasia Battery-Revised; PsychCorp: Toronto, ON, Canada, 2007. [Google Scholar]
- Audacity Team. Audacity(R): Free Audio Editor and Recorder, Version 2.4.1. 2014. Available online: http://audacity.sourceforge.net/ (accessed on 21 April 2020).
- Agis, D.; Goggins, M.B.; Oishi, K.; Oishi, K.; Davis, C.; Wright, A.; Kim, E.H.; Sebastian, R.; Tippett, D.C.; Faria, A.; et al. Picturing the Size and Site of Stroke With an Expanded National Institutes of Health Stroke Scale. Stroke 2016, 47, 1459–1465. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2014; Available online: http://www.R-project.org/ (accessed on 21 April 2020).
- Sajjadi, S.A.; Patterson, K.; Tomek, M.; Nestor, P.J. Abnormalities of connected speech in semantic dementia vs Alzheimer’s disease. Aphasiology 2012, 26, 847–866. [Google Scholar] [CrossRef]




| PPA (N = 70) | Healthy Controls | |||
|---|---|---|---|---|
| svPPA (N = 19) | lvPPA (N = 26) | nfvPPA (N = 25) | (HC) (N = 31) | |
| Age at testing, years (SD) | 69.7 (8.35) | 70.2 (7.17) | 68.2 (8.28) | 63.4 (8.20) |
| Female, n (%) | 11.0 (57.8) | 12.0 (46.2) | 15.0 (60.0) | 17.0 (54.8) |
| Education, years (SD) | 16.2 (2.30) | 15.7 (2.38) | 15.5 (2.73) | 14.9 (1.83) |
| CDR language (SD), n = 0.5 | 0.71 (0.25), 11 | 0.71 (0.25), 15 | 0.66 (0.24), 17 | -- |
| PASS sum of boxes (SD) | 3.50 (1.30) | 4.04 (1.25) | 3.82 (1.26) | -- |
| Category | CU # | Referent CU# | Count | CU |
|---|---|---|---|---|
| Unambiguous entities/objects/events | 1 | 31 | Kite | |
| 2 | 31 | House, home, rental, cottage, cabin | ||
| 3 | 31 | Wine, drink, liquid, drinks, beverage, soda, juice, champagne | ||
| 4 | 30 | Dog, puppy | ||
| 5 | 29 | Beach, sand | ||
| 6 | 28 | Sailboat, boat | ||
| 7 | 28 | Picnic, picnicking | ||
| 8 | 27 | Woman, mother, mom, wife, lady | ||
| 9 | 26 | Sandcastle(s), pile, castle | ||
| 10 | 26 | Water, lake, ocean, river, sea | ||
| 11 | 26 | Boy, son | ||
| 12 | 24 | Girl, daughter | ||
| 13 | 21 | Pier, dock | ||
| 14 | 18 | Book | ||
| 15 | 18 | Tree | ||
| 16 | 16 | Car | ||
| 17 | 16 | Driveway, path, road, street | ||
| 18 | 15 | Garage, parked (car) | ||
| 19 | 15 | Shoes, sandals, sneakers | ||
| 20 | 13 | Fish (noun) | ||
| 21 | 13 | Couple, two (people), parents | ||
| 22 | 13 | Radio, boombox | ||
| 23 | 11 | Flag, flagpole | ||
| 24 | 11 | Glass, cup, glasses | ||
| 25 | 10 | Blanket, carpet | ||
| 26 | 8 | Shovel | ||
| 27 | 7 | Pail, bucket | ||
| 28 | 7 | Sky, clouds | ||
| 29 | 6 | Fisherman | ||
| 30 | 4 | Nasket | ||
| 31 | 3 | (Man’s) glasses | ||
| 32 | 3 | Bottle, thermos | ||
| Unambiguous actions | 33 | 31 | Fishing, caught (a fish), catching (a fish) | |
| 34 | 31 | Flying (a kite), pulling (a kite) | ||
| 35 | 31 | Building (a sandcastle), making (a sandcastle), playing (in the sand), built a sandcastle | ||
| 36 | 26 | Reading | ||
| 37 | 21 | Pouring | ||
| 38 | 18 | Enjoying, relaxing, happy, having a good time, relaxed, (having) fun | ||
| 39 | 17 | (Dog is) chasing, (dog is) following, chased | ||
| 40 | 8 | Sailing, cruising | ||
| Unambiguous properties | 41 | 17 | Beautiful, idyllic, nice, lovely, pleasant, calm | |
| 42 | 10 | Big, large | ||
| Ambiguous-referent entities | 43 | 31 | Man, father, dad, gentleman, grandpa, husband, hubby, pops | |
| 43a | 42 | 18 | ||
| 43b | 29 | 15 | ||
| 44 | No Pattern | 31 | Grass, yard, shrubbery, park, enclave, grassy, place, bushes, environment, foliage, gable, hill, mountains, scenery, spot, trees, forest | |
| 45 | 30 | Someone, guy, fellow, somebody, person, jabroni, adult | ||
| 45a | 11 | |||
| 45b | 12 | |||
| 45c | 42 | |||
| 45d | 29 | |||
| 46 | 24 | Family, people, everyone, families, occupants | ||
| 46a | 11, 12, 8, 42 | |||
| 46b | 11, 12, 8, 42, 29 | |||
| 46c | No Pattern | |||
| 47 | 12 | Inlet, lakeside, seashore, seaside, bay, oceanside, shore, wharf | ||
| 47a | 58 | |||
| 47b | 12 | |||
| 47c | 29 | |||
| 48 | 8 | Kid, kids, children | ||
| 48a | 11 | |||
| 48b | 12 | |||
| 49 | 5 | Shorts | ||
| 49a | 11 | |||
| 49b | 8 + 42 | |||
| 49c | 42 | |||
| 50 | 3 | T-shirt | ||
| 50a | 11 | |||
| 50b | 8 | |||
| Ambiguous-referent actions | 51 | 12 | Running | |
| 51a | 11 | |||
| 51b | 4 | |||
| 51c | 11 + 4 | |||
| 52 | 6 | Sitting | ||
| 52a | 8 | |||
| 52b | 42 | |||
| 52c | 8 + 42 | |||
| 53 | 5 | Wearing | ||
| 53a | 11 | |||
| 53b | 8 + 42 | |||
| 53c | 42 | |||
| 53d | 29 | |||
| 54 | 15 | 4 | Bloom, blossomed, blooming | |
| Ambiguous-referent properties | 55 | 27 | Little, young, younger | |
| 55a | 11 | |||
| 55b | 12 | |||
| 55c | 4 | |||
| 55d | 2 | |||
| 55e | 43 | |||
| Unambiguous but inferred (not physically present/abstract) | 56 | 20 | Summer, sun, sunny, summertime, weather, season, spring, warm | |
| 57 | 16 | Music, listening to (music), (playing) music | ||
| 58 | 16 | Day, afternoon, vacation, retreat | ||
| 59 | 9 | Scene, picture | ||
| 60 | 9 | Activities, recreational, sport | ||
| 61 | 8 | Outside | ||
| 62 | 4 | Breeze, windy | ||
| 63 | 4 | Sandwich(es), food | ||
| Ambiguous-referent spatial relations | 64 | 31 | Across, around, background, behind, beside, close, distance, distant, far, foreground, front, left, nearby, next to, right, side | |
| 64a | 2 | |||
| 64b | 6 | |||
| 64c | 11 | |||
| 64d | 15 | |||
| 64e | 23 | |||
| 64f | 4 | |||
| 64g | 21 | |||
| 64h | 29 | |||
| 64i | 43 | |||
| 64j | 16 | |||
| 64k | 22 | |||
| 64l | 17 |
| Method | Group | CUs (SD) | CU Effect Size vs. HCs (Hedge’s g) | Informativeness (SD) | Informativeness Effect Size vs. HCs (Hedge’s g) |
|---|---|---|---|---|---|
| Original Berube et al. (2019) [21] | HC | 28.5 (6.46) | - | 20.9% (5.67) | - |
| lvPPA | 14.5 (5.81) ***♦ | 2.25 | 11.7% (5.18) ***♦ | 1.75 | |
| nfvPPA | 20.3 (6.07) *** | 1.28 | 23.1% (9.45) | −0.29 | |
| svPPA | 13.0 (5.67) ***♦ | 2.47 | 11.1% (6.46) ***♦ | 1.69 | |
| CU-uniqueref | HC | 30.0 (7.99) | - | 21.9% (5.87) | - |
| lvPPA | 14.8 (6.07) ***♦ | 2.23 | 11.9% (5.26) ***♦ | 1.86 | |
| nfvPPA | 20.8 (6.19) *** | 1.33 | 23.5% (9.31) | >−0.22 | |
| svPPA | 13.7 (6.24) ***♦ | 2.34 | 11.7% (7.02) ***♦ | 1.65 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gallée, J.; Cordella, C.; Fedorenko, E.; Hochberg, D.; Touroutoglou, A.; Quimby, M.; Dickerson, B.C. Breakdowns in Informativeness of Naturalistic Speech Production in Primary Progressive Aphasia. Brain Sci. 2021, 11, 130. https://doi.org/10.3390/brainsci11020130
Gallée J, Cordella C, Fedorenko E, Hochberg D, Touroutoglou A, Quimby M, Dickerson BC. Breakdowns in Informativeness of Naturalistic Speech Production in Primary Progressive Aphasia. Brain Sciences. 2021; 11(2):130. https://doi.org/10.3390/brainsci11020130
Chicago/Turabian StyleGallée, Jeanne, Claire Cordella, Evelina Fedorenko, Daisy Hochberg, Alexandra Touroutoglou, Megan Quimby, and Bradford C. Dickerson. 2021. "Breakdowns in Informativeness of Naturalistic Speech Production in Primary Progressive Aphasia" Brain Sciences 11, no. 2: 130. https://doi.org/10.3390/brainsci11020130