
Health Economic Impact of Software-Assisted Brain MRI on Therapeutic Decision-Making and Outcomes of Relapsing-Remitting Multiple Sclerosis Patients—A Microsimulation Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
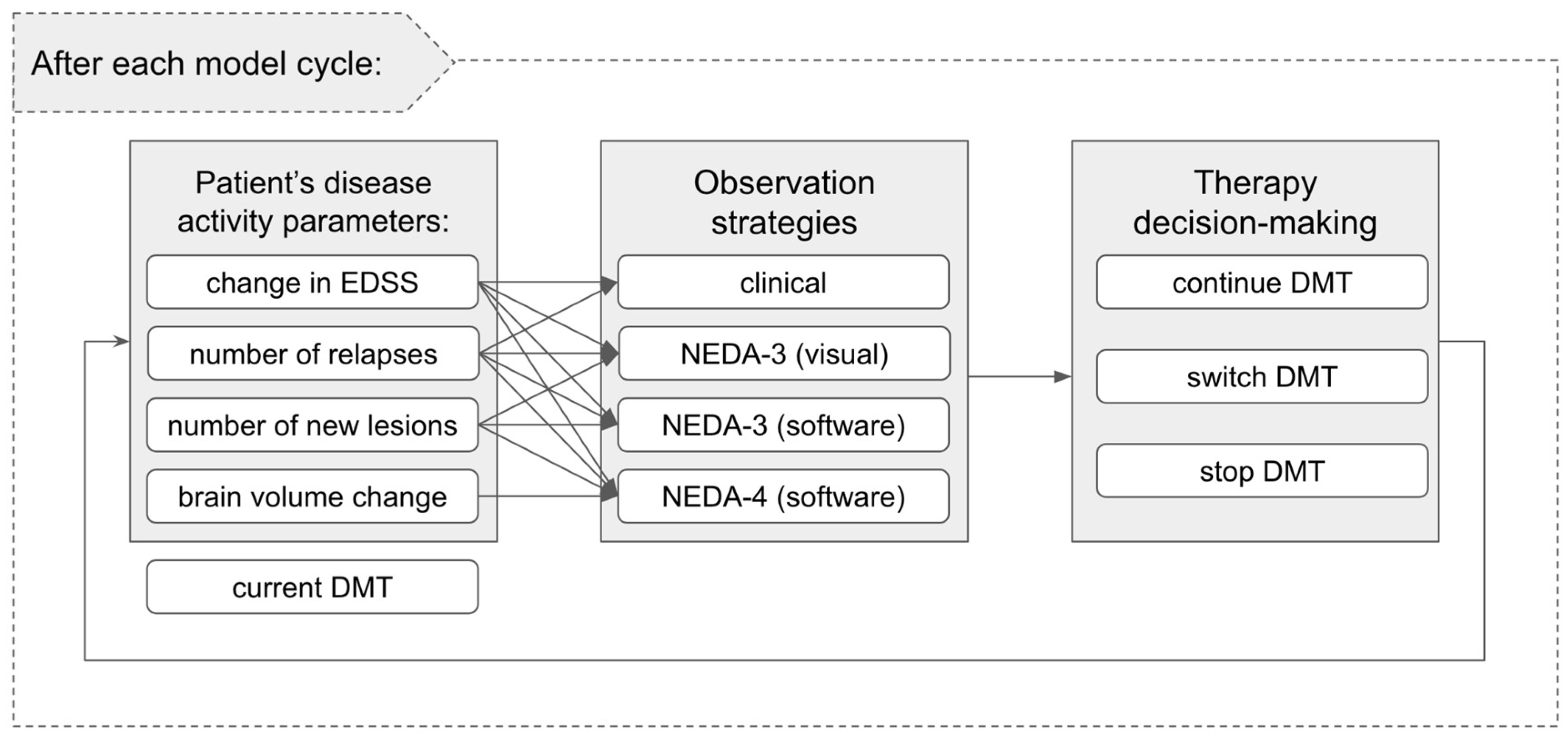
2.1. Model Structure
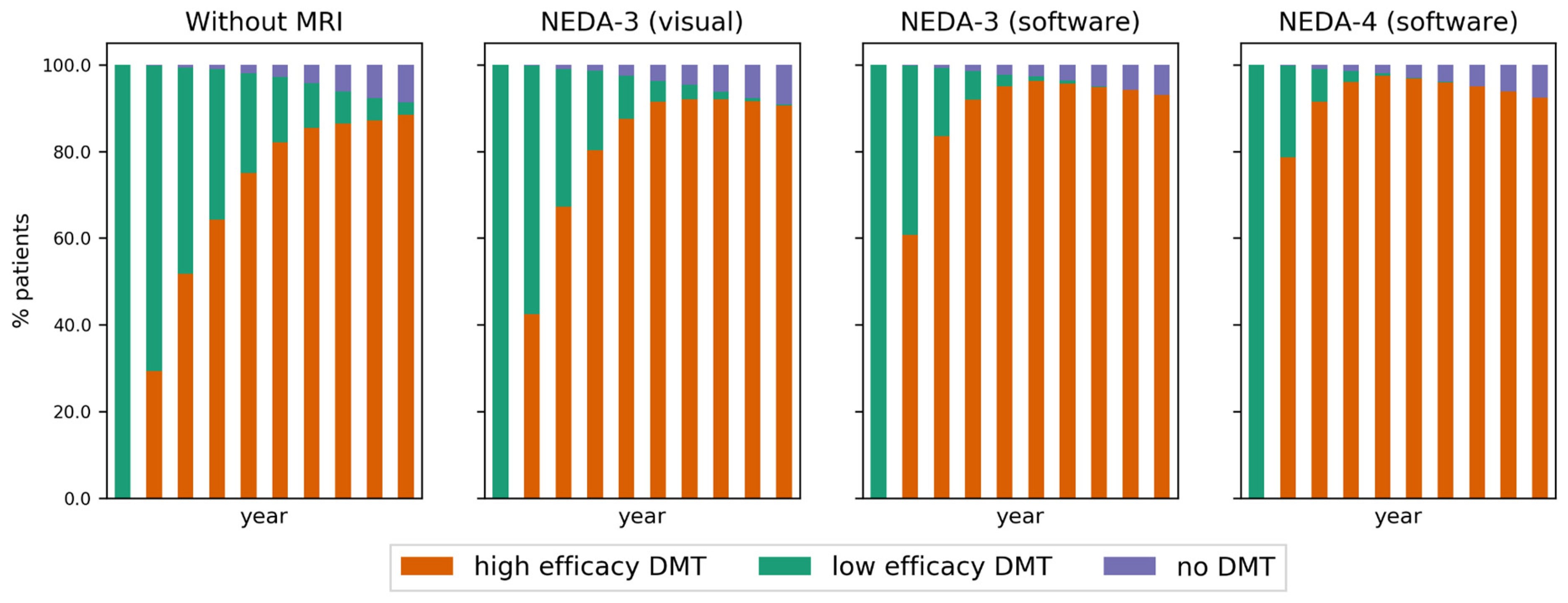
- clinical examination without MRI: disease activity or progression is established solely on clinical relapses and/or EDSS progression;
- NEDA-3 (visual): clinical criteria (as above) are complemented by visually inspected MRI to detect lesion evolution;
- NEDA-3 (software): NEDA-3 (visual) criteria as above are complemented by software-assisted lesion detection;
- NEDA-4 (software): NEDA-3 (software) criteria as above are complemented by software-assisted brain volume loss computation.
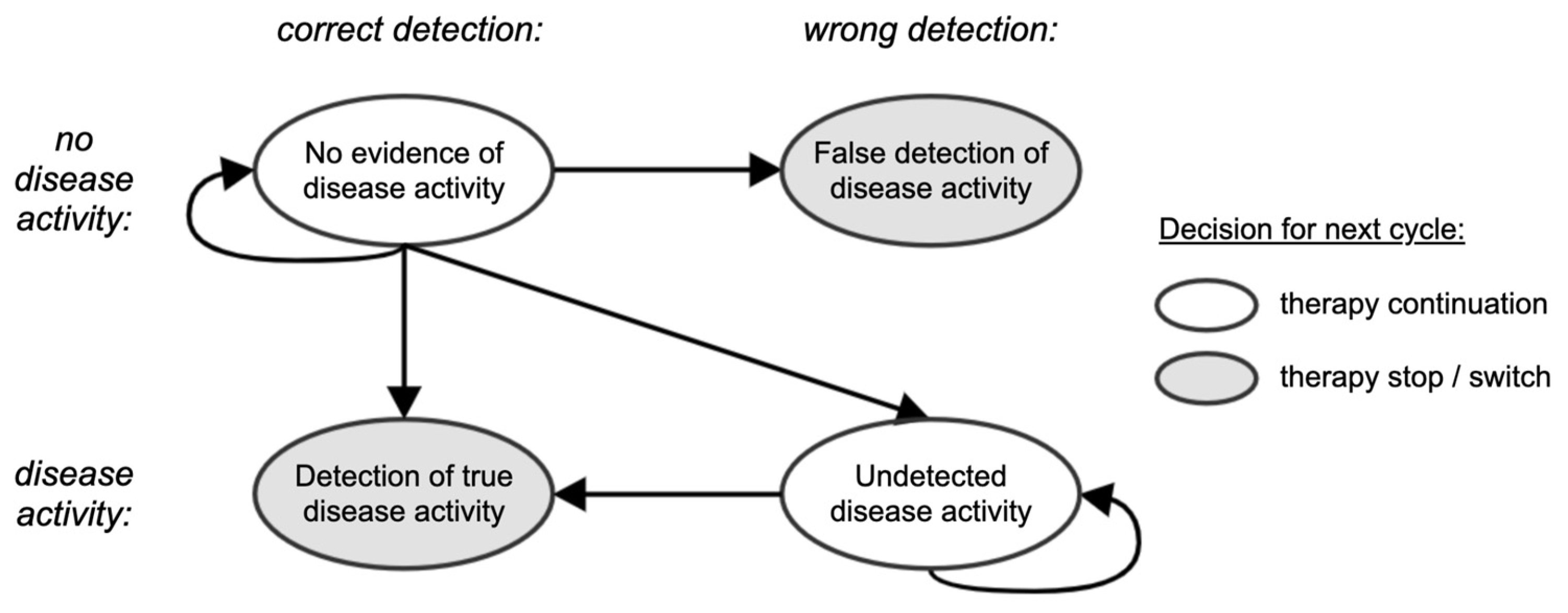
2.2. Simulation of Observation and Therapy Decision Strategies
2.3. Model Inputs—Simulation Details
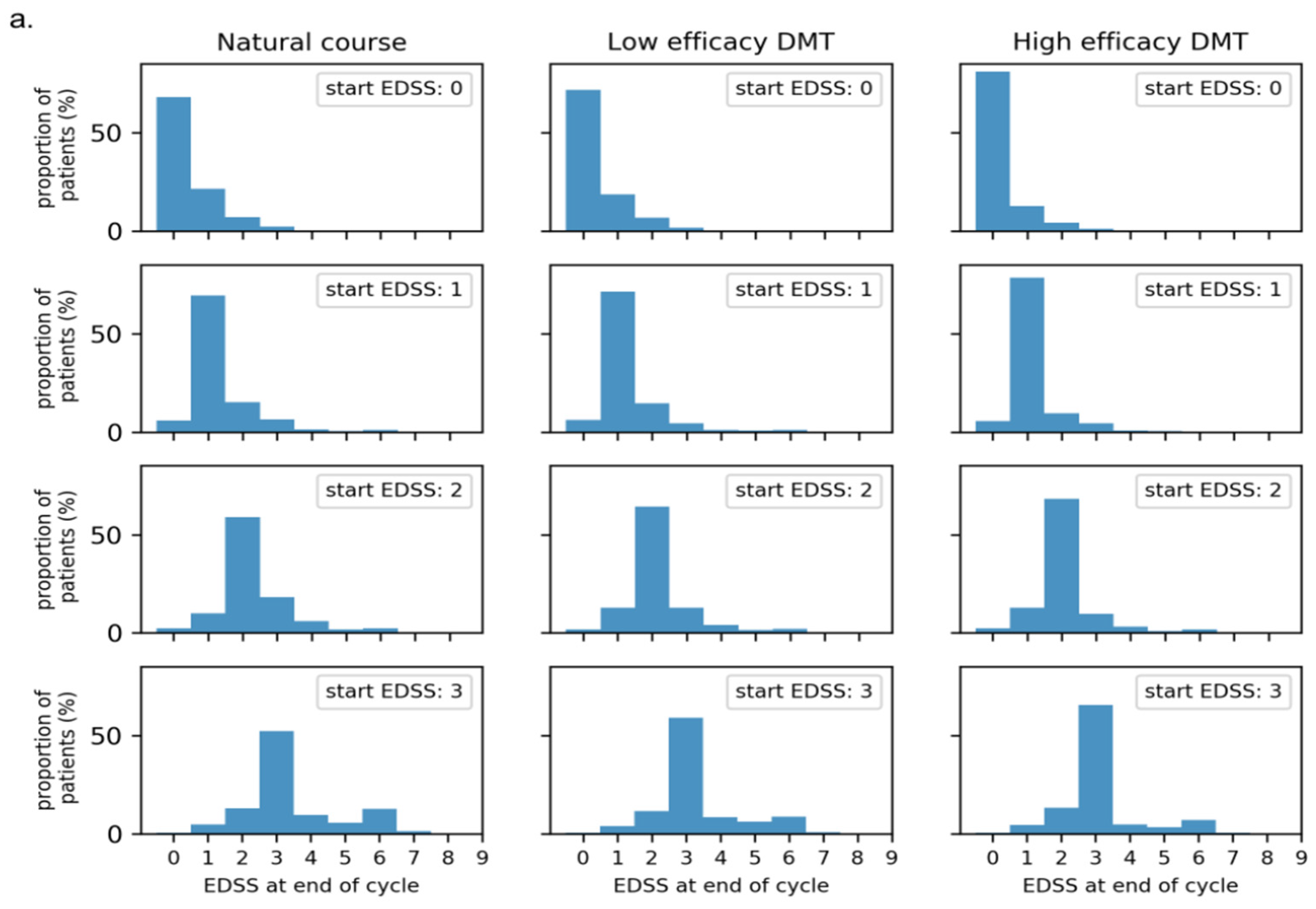
2.3.1. MS Disease Progression Parameters
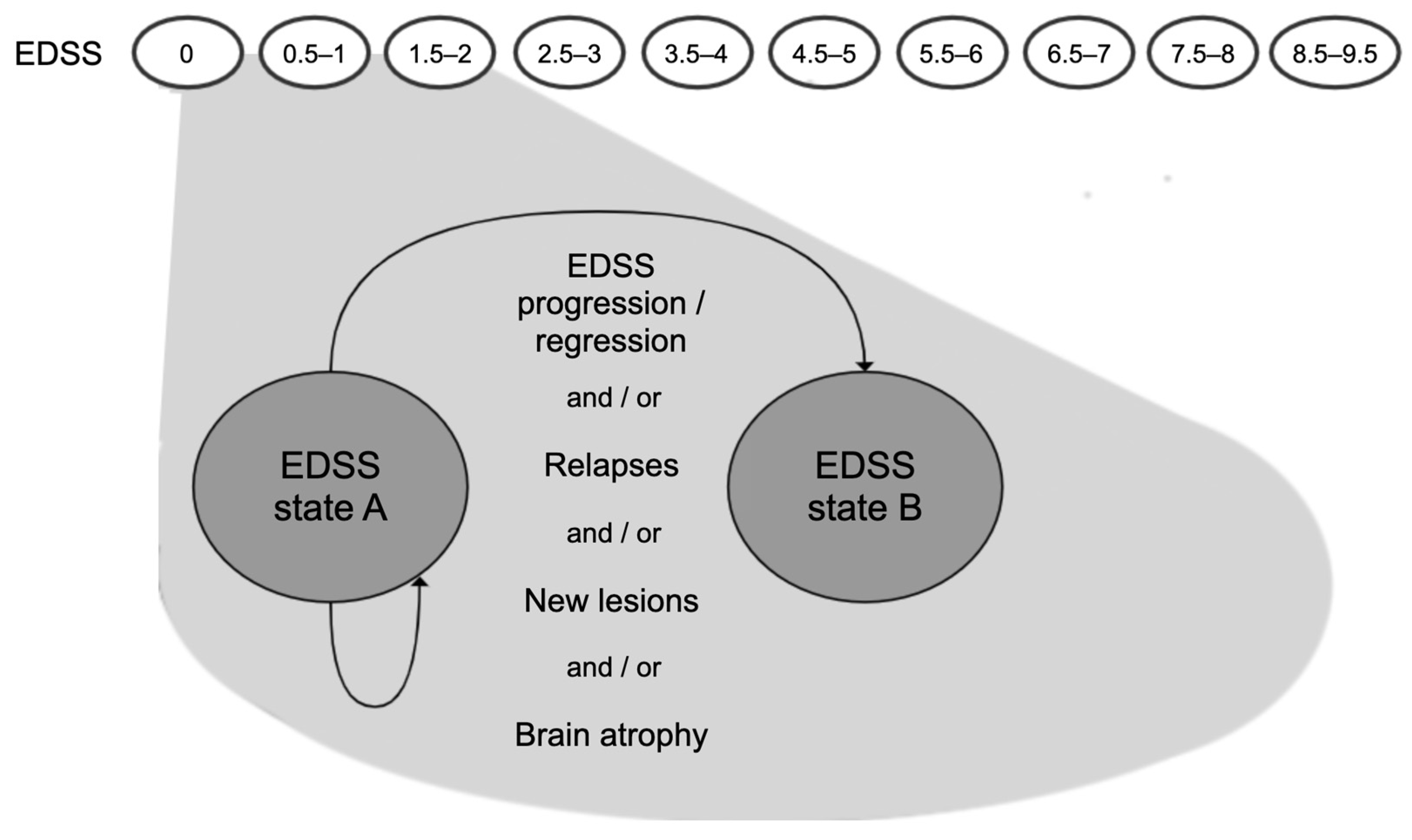
2.3.2. EDSS
- first, the relative risk factor is obtained from the interval corresponding to the patient’s DMT family (see Table 2, second column) assuming a uniform distribution and using the patient’s fixed percentile score;
- secondly, a new EDSS transition matrix is constructed by multiplying all transitions going from the patient’s current EDSS state towards states higher than the current EDSS state by f. For f < 1, this leads to less chance of EDSS progression. The remaining transition probabilities corresponding to EDSS states lower than or equal to the current state are scaled proportionally in order to ensure that all probabilities sum to 1 in each row.
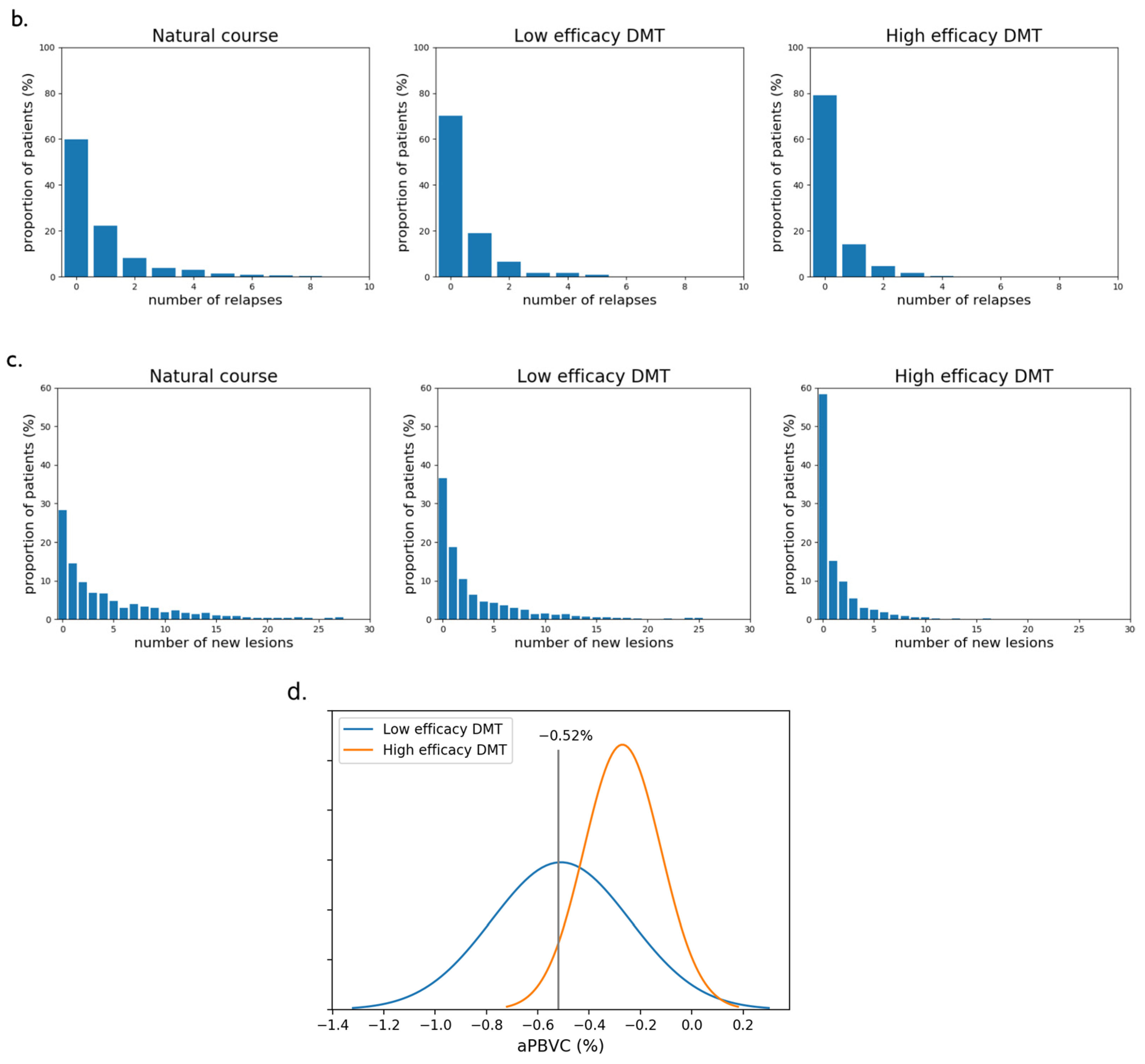
2.3.3. Relapses and New Lesions
2.3.4. Brain Atrophy
2.4. Outcome Measures, Utilities, and Costs
3. Results
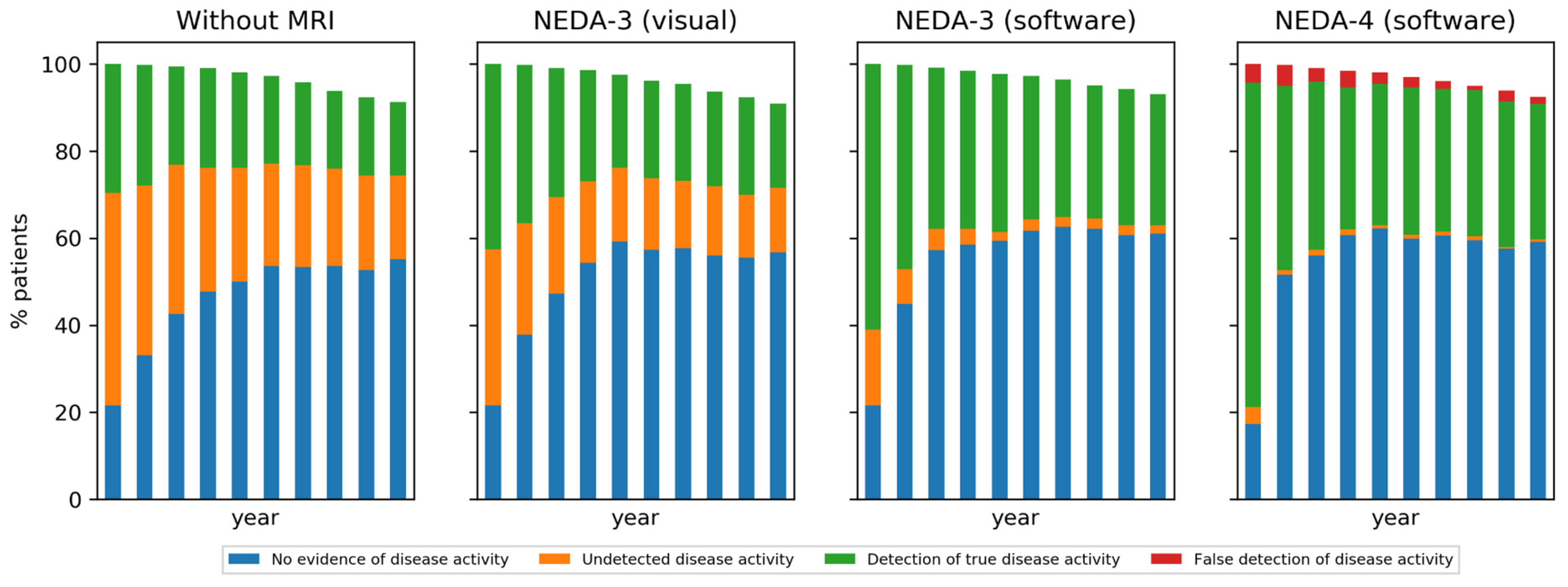
3.1. Effect of Decision-Making Strategy on Detecting Disease Progression
3.2. Health Outcomes
- 3.2 ± 2.4 years for the clinical strategy without MRI,
- 2.3 ± 1.6 years for the NEDA-3 (visual) strategy,
- 1.7 ± 1.1 years for the NEDA-3 (software) strategy,
- 1.3 ± 0.7 years for the NEDA-4 (software) strategy.
- 2.8 ± 2.3 years for the clinical strategy without MRI,
- 1.9 ± 1.4 years for the NEDA-3 (visual) strategy,
- 1.3 ± 0.8 years for the NEDA-3 (software) strategy,
- 1.0 ± 0.2 years for the NEDA-4 (software) strategy.
3.3. Utilities and Costs
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Model Inputs

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| EDSS 0 | EDSS 1 | EDSS 2 | EDSS 3 | EDSS 4 | EDSS 5 | EDSS 6 | EDSS 7 | EDSS 8 | EDSS 9 | |
|---|---|---|---|---|---|---|---|---|---|---|
| Proportion | 25 | 25 | 25 | 25 | 0 | 0 | 0 | 0 | 0 | 0 |
| Age ≥ 28 y | EDSS State at End of Year | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | ||
| EDSS State at Start of Year | 0 | 0.6954 | 0.2029 | 0.0725 | 0.0217 | 0.0042 | 0.0014 | 0.0018 | 0.0001 | 0.00003 | 0.00000 |
| 1 | 0.0583 | 0.6950 | 0.1578 | 0.0609 | 0.0164 | 0.0046 | 0.0064 | 0.0005 | 0.0001 | 0.00001 | |
| 2 | 0.0159 | 0.1213 | 0.6079 | 0.1680 | 0.0446 | 0.0185 | 0.0216 | 0.0017 | 0.0005 | 0.0000 | |
| 3 | 0.0059 | 0.0496 | 0.1201 | 0.5442 | 0.0911 | 0.0584 | 0.1165 | 0.0103 | 0.0035 | 0.0003 | |
| 4 | 0.0016 | 0.0221 | 0.0666 | 0.1152 | 0.4893 | 0.1039 | 0.1681 | 0.0258 | 0.0067 | 0.0006 | |
| 5 | 0.0005 | 0.0053 | 0.0294 | 0.0587 | 0.0874 | 0.4869 | 0.2731 | 0.0388 | 0.0188 | 0.0010 | |
| 6 | 0.0001 | 0.0013 | 0.0044 | 0.0250 | 0.0307 | 0.0408 | 0.7407 | 0.1090 | 0.0438 | 0.0042 | |
| 7 | 0.00001 | 0.0002 | 0.0005 | 0.0025 | 0.0073 | 0.0039 | 0.1168 | 0.6927 | 0.1606 | 0.0156 | |
| 8 | 0.0000 | 0.00001 | 0.0000 | 0.0003 | 0.0005 | 0.0005 | 0.0188 | 0.0557 | 0.9034 | 0.0207 | |
| 9 | 0.0000 | 0.0000 | 0.0000 | 0.00002 | 0.00004 | 0.00003 | 0.0018 | 0.0057 | 0.1741 | 0.8183 | |
| EDSS 0 | EDSS 1 | EDSS 2 | EDSS 3 | EDSS 4 | EDSS 5 | EDSS 6 | EDSS 7 | EDSS 8 | EDSS 9 | |
|---|---|---|---|---|---|---|---|---|---|---|
| Relapse rate * | 0.71 | 0.73 | 0.68 | 0.72 | 0.71 | 0.59 | 0.49 | 0.51 | 0.51 | 0.51 |
| Treatment | Relative Risk EDSS Progression (Range) | Rate Ratio for Relapse Rate (Range) |
|---|---|---|
| Alemtuzumab | 0.25–0.68 | 0.22–0.35 |
| Dimethyl Fumarate | 0.46–0.84 | 0.43–0.63 |
| Fingolimod | 0.51–0.90 | 0.39–0.55 |
| Glatiramer acetate 20 mg | 0.58–0.94 | 0.55–0.71 |
| Interferon β-1a 30 mcg | 0.63–1.00 | 0.74–0.94 |
| Interferon β-1a 22 mcg | 0.52–1.23 | 0.55–0.85 |
| Interferon β-1a 44 mcg | 0.52–0.99 | 0.54–0.73 |
| Interferon β-1b 250 mcg | 0.46–0.89 | 0.55–0.77 |
| Natalizumab | 0.37–0.84 | 0.25–0.40 |
| Ocrelizumab | 0.28–0.76 | 0.27–0.44 |
| Peginterferon β-1a | 0.37–1.02 | 0.47–0.86 |
| Teriflunomide 7 mg | 0.63–1.14 | 0.67–0.93 |
| Teriflunomide 14 mg | 0.52–0.97 | 0.56–0.79 |
Appendix B. Utilities and Costs
| EDSS 0 | EDSS 1 | EDSS 2 | EDSS 3 | EDSS 4 | EDSS 5 | EDSS 6 | EDSS 7 | EDSS 8 | EDSS 9 | |
|---|---|---|---|---|---|---|---|---|---|---|
| Utility | 0.9248 | 0.7614 | 0.6741 | 0.5643 | 0.5643 | 0.4906 | 0.4453 | 0.2686 | 0.0076 | −0.2304 |
| Annual Costs | EDSS 0 | EDSS 1 | EDSS 2 | EDSS 3 | EDSS 4 | EDSS 5 | EDSS 6 | EDSS 7 | EDSS 8 | EDSS 9 |
|---|---|---|---|---|---|---|---|---|---|---|
| Direct | $3221 | $5536 | $7851 | $10,165 | $12,481 | $14,796 | $17,111 | $19,427 | $21,741 | $24,056 |
| Indirect | $12,211 | $16,704 | $21,198 | $25,692 | $30,187 | $34,681 | $39,175 | $43,669 | $48,164 | $52,658 |
Appendix C. Model Parameter Distributions


| EDSS Progression | Relapse Progression Using nrelapse Threshold of | Lesion Progression Using nlesion Threshold of | PBVC Progression Using α Threshold of | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| - | 1 * | 2 | 3 | 1 | 2 | 3 * | 4 | −0.40 | −0.52 * | −0.72 | |
| natural course | 22% | 35% | 17% | 8% | 64% | 56% | 48% | 43% | 66% | 49% | 21% |
| low efficacy DMT | 19% | 30% | 12% | 5% | 64% | 43% | 38% | 28% | 66% | 49% | 21% |
| high efficacy DMT | 12% | 20% | 6% | 2% | 48% | 28% | 15% | 11% | 19% | 5% | 0% |
References
- Costello, K.; Halper, J.; Kalb, R.; Skutnik, L.; Rapp, R. The Use of Disease-Modifying Therapies in Multiple Sclerosis, Principles and Current Evidence—A Consensus Paper by the Multiple Sclerosis Coalition; The Multiple Sclerosis Coalition: Hackensack, NJ, USA, 2019; Available online: https://ms-coalition.org/the-use-of-disease-modifying-therapies-in-multiple-sclerosis-updated/ (accessed on 10 October 2021).
- Giovannoni, G.; Butzkueven, H.; Dhib-Jalbut, S.; Hobart, J.; Kobelt, G.; Pepper, G.; Sormani, M.P.; Thalheim, C.; Traboulsee, A.; Vollmer, T. Brain Health: Time Matters in Multiple Sclerosis. Mult. Scler. Relat. Disord. 2016, 9 (Suppl. 1), S5–S48. [Google Scholar] [CrossRef] [Green Version]
- University of California, San Francisco MS-EPIC Team; Cree, B.A.C.; Hollenbach, J.A.; Bove, R.; Kirkish, G.; Sacco, S.; Caverzasi, E.; Bischof, A.; Gundel, T.; Zhu, A.H.; et al. Silent Progression in Disease Activity-Free Relapsing Multiple Sclerosis. Ann. Neurol. 2019, 85, 653–666. [Google Scholar] [CrossRef] [PubMed]
- Rosenkrantz, A.B.; Duszak, R.; Babb, J.S.; Glover, M.; Kang, S.K. Discrepancy Rates and Clinical Impact of Imaging Secondary Interpretations: A Systematic Review and Meta-Analysis. J. Am. Coll. Radiol. 2018, 15. [Google Scholar] [CrossRef] [PubMed]
- Van Hecke, W.; Costers, L.; Descamps, A.; Ribbens, A.; Nagels, G.; Smeets, D.; Sima, D.M. A Novel Digital Care Management Platform to Monitor Clinical and Subclinical Disease Activity in Multiple Sclerosis. Brain Sci. 2021, 11, 1171. [Google Scholar] [CrossRef] [PubMed]
- Erbayat Altay, E.; Fisher, E.; Jones, S.E.; Hara-Cleaver, C.; Lee, J.-C.; Rudick, R.A. Reliability of Classifying Multiple Sclerosis Disease Activity Using Magnetic Resonance Imaging in a Multiple Sclerosis Clinic. JAMA Neurol. 2013, 70, 338–344. [Google Scholar] [CrossRef]
- Wang, W.; van Heerden, J.; Tacey, M.A.; Gaillard, F. Neuroradiologists Compared with Non-Neuroradiologists in the Detection of New Multiple Sclerosis Plaques. AJNR Am. J. Neuroradiol. 2017, 38, 1323–1327. [Google Scholar] [CrossRef] [Green Version]
- Adelman, G.; Rane, S.G.; Villa, K.F. The Cost Burden of Multiple Sclerosis in the United States: A Systematic Review of the Literature. J. Med. Econ. 2013, 16, 639–647. [Google Scholar] [CrossRef]
- Chen, A.Y.; Chonghasawat, A.O.; Leadholm, K.L. Multiple Sclerosis: Frequency, Cost, and Economic Burden in the United States. J. Clin. Neurosci. 2017, 45, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Owens, G.M.; Olvey, E.L.; Skrepnek, G.H.; Pill, M.W. Perspectives for Managed Care Organizations on the Burden of Multiple Sclerosis and the Cost-Benefits of Disease-Modifying Therapies. J. Manag. Care Pharm. 2013, 19, S41–S53. [Google Scholar] [CrossRef] [PubMed]
- Hult, K.J. Measuring the Potential Health Impact of Personalized Medicine: Evidence from MS Treatments. In Economic Dimensions of Personalized and Precision Medicine; Berndt, E.R., Goldman, D.P., Rowe, J.W., Eds.; National Bureau of Economic Research; University of Chicago Press: Chicago, IL, USA, 2019. [Google Scholar]
- Furneri, G.; Santoni, L.; Ricella, C.; Prosperini, L. Cost-Effectiveness Analysis of Escalating to Natalizumab or Switching among Immunomodulators in Relapsing-Remitting Multiple Sclerosis in Italy. BMC Health Serv. Res. 2019, 19, 436. [Google Scholar] [CrossRef]
- Chirikov, V.; Ma, I.; Joshi, N.; Patel, D.; Smith, A.; Giambrone, C.; Cornelio, N.; Hashemi, L. Cost-Effectiveness of Alemtuzumab in the Treatment of Relapsing Forms of Multiple Sclerosis In The United States and Societal Spillover Effects. Value Health 2017, 20, A722. [Google Scholar] [CrossRef]
- Gani, R.; Giovannoni, G.; Bates, D.; Kemball, B.; Hughes, S.; Kerrigan, J. Cost-Effectiveness Analyses of Natalizumab (Tysabri) Compared with Other Disease-Modifying Therapies for People with Highly Active Relapsing-Remitting Multiple Sclerosis in the UK. Pharmacoeconomics 2008, 26, 617–627. [Google Scholar] [CrossRef] [PubMed]
- Kaunzner, U.W.; Gauthier, S.A. MRI in the Assessment and Monitoring of Multiple Sclerosis: An Update on Best Practice. Ther. Adv. Neurol. Disord. 2017, 10, 247–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tremlett, H.; Zhao, Y.; Rieckmann, P.; Hutchinson, M. New Perspectives in the Natural History of Multiple Sclerosis. Neurology 2010, 74, 2004–2015. [Google Scholar] [CrossRef] [PubMed]
- Institute for Clinical and Economic Review and California Technology Assessment Forum. Disease-Modifying Therapies for Relapsing-Remitting and Primary-Progressive Multiple Sclerosis: Effectiveness and Value: Final Evidence Report; Institute for Clinical and Economic Review: Boston, MA, USA, 2017. Available online: http://resource.nlm.nih.gov/101704699 (accessed on 10 October 2021).
- Dahan, A.; Wang, W.; Gaillard, F. Computer-Aided Detection Can Bridge the Skill Gap in Multiple Sclerosis Monitoring. J. Am. Coll. Radiol. 2018, 15, 93–96. [Google Scholar] [CrossRef]
- Galletto Pregliasco, A.; Collin, A.; Guéguen, A.; Metten, M.A.; Aboab, J.; Deschamps, R.; Gout, O.; Duron, L.; Sadik, J.C.; Savatovsky, J.; et al. Improved Detection of New MS Lesions during Follow-Up Using an Automated MR Coregistration-Fusion Method. AJNR Am. J. Neuroradiol. 2018, 39, 1226–1232. [Google Scholar] [CrossRef] [PubMed]
- van Heerden, J.; Rawlinson, D.; Zhang, A.M.; Chakravorty, R.; Tacey, M.A.; Desmond, P.M.; Gaillard, F. Improving Multiple Sclerosis Plaque Detection Using a Semiautomated Assistive Approach. AJNR Am. J. Neuroradiol. 2015, 36, 1465–1471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zopfs, D.; Laukamp, K.R.; Paquet, S.; Lennartz, S.; Pinto Dos Santos, D.; Kabbasch, C.; Bunck, A.; Schlamann, M.; Borggrefe, J. Follow-up MRI in Multiple Sclerosis Patients: Automated Co-Registration and Lesion Color-Coding Improves Diagnostic Accuracy and Reduces Reading Time. Eur. Radiol. 2019, 29, 7047–7054. [Google Scholar] [CrossRef] [PubMed]
- De Stefano, N.; Stromillo, M.L.; Giorgio, A.; Bartolozzi, M.L.; Battaglini, M.; Baldini, M.; Portaccio, E.; Amato, M.P.; Sormani, M.P. Establishing Pathological Cut-Offs of Brain Atrophy Rates in Multiple Sclerosis. J. Neurol. Neurosurg. Psychiatry 2016, 87, 93–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smeets, D.; Ribbens, A.; Sima, D.M.; Cambron, M.; Horakova, D.; Jain, S.; Maertens, A.; Van Vlierberghe, E.; Terzopoulos, V.; Van Binst, A.-M.; et al. Reliable Measurements of Brain Atrophy in Individual Patients with Multiple Sclerosis. Brain Behav. 2016, 6, e00518. [Google Scholar] [CrossRef]
- Hettle, R.; Harty, G.; Wong, S.L. Cost-Effectiveness of Cladribine Tablets, Alemtuzumab, and Natalizumab in the Treatment of Relapsing-Remitting Multiple Sclerosis with High Disease Activity in England. J. Med. Econ. 2018, 21, 676–686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palace, J.; Duddy, M.; Bregenzer, T.; Lawton, M.; Zhu, F.; Boggild, M.; Piske, B.; Robertson, N.P.; Oger, J.; Tremlett, H.; et al. Effectiveness and Cost-Effectiveness of Interferon Beta and Glatiramer Acetate in the UK Multiple Sclerosis Risk Sharing Scheme at 6 Years: A Clinical Cohort Study with Natural History Comparator. Lancet Neurol. 2015, 14, 497–505. [Google Scholar] [CrossRef]
- Ribbons, K.A.; McElduff, P.; Boz, C.; Trojano, M.; Izquierdo, G.; Duquette, P.; Girard, M.; Grand’Maison, F.; Hupperts, R.; Grammond, P.; et al. Male Sex Is Independently Associated with Faster Disability Accumulation in Relapse-Onset MS but Not in Primary Progressive MS. PLoS ONE 2015, 10, e0122686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sormani, M.P.; Bruzzi, P.; Miller, D.H.; Gasperini, C.; Barkhof, F.; Filippi, M. Modelling MRI Enhancing Lesion Counts in Multiple Sclerosis Using a Negative Binomial Model: Implications for Clinical Trials. J. Neurol. Sci. 1999, 163, 74–80. [Google Scholar] [CrossRef]
- van den Elskamp, I.; Knol, D.; Uitdehaag, B.; Barkhof, F. The Distribution of New Enhancing Lesion Counts in Multiple Sclerosis: Further Explorations. Mult. Scler. 2009, 15, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Aban, I.B.; Cutter, G.R.; Mavinga, N. Inferences and Power Analysis Concerning Two Negative Binomial Distributions with an Application to MRI Lesion Counts Data. Comput. Stat. Data Anal. 2008, 53, 820–833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalincik, T.; Vivek, V.; Jokubaitis, V.; Lechner-Scott, J.; Trojano, M.; Izquierdo, G.; Lugaresi, A.; Grand’maison, F.; Hupperts, R.; Oreja-Guevara, C.; et al. Sex as a Determinant of Relapse Incidence and Progressive Course of Multiple Sclerosis. Brain 2013, 136, 3609–3617. [Google Scholar] [CrossRef] [PubMed]
- Sormani, M.P.; Bruzzi, P. MRI Lesions as a Surrogate for Relapses in Multiple Sclerosis: A Meta-Analysis of Randomised Trials. Lancet Neurol. 2013, 12, 669–676. [Google Scholar] [CrossRef]
- Azevedo, C.J.; Cen, S.Y.; Jaberzadeh, A.; Zheng, L.; Hauser, S.L.; Pelletier, D. Contribution of Normal Aging to Brain Atrophy in MS. Neurol. Neuroimmunol. Neuroinflamm. 2019, 6. [Google Scholar] [CrossRef] [Green Version]
- Favaretto, A.; Lazzarotto, A.; Margoni, M.; Poggiali, D.; Gallo, P. Effects of Disease Modifying Therapies on Brain and Grey Matter Atrophy in Relapsing Remitting Multiple Sclerosis. Mult. Scler. Demyelinating Disord. 2018, 3, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Ontaneda, D.; Tallantyre, E.C.; Raza, P.C.; Planchon, S.M.; Nakamura, K.; Miller, D.; Hersh, C.; Craner, M.; Bale, C.; Chaudhry, B.; et al. Determining the Effectiveness of Early Intensive versus Escalation Approaches for the Treatment of Relapsing-Remitting Multiple Sclerosis: The DELIVER-MS Study Protocol. Contemp. Clin. Trials 2020, 95, 106009. [Google Scholar] [CrossRef] [PubMed]
- Chirikov, V.; Ma, I.; Joshi, N.; Patel, D.; Smith, A.; Giambrone, C.; Cornelio, N.; Hashemi, L. Cost-Effectiveness of Alemtuzumab in the Treatment of Relapsing Forms of Multiple Sclerosis in the United States. Value Health 2019, 22, 168–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmermann, M.; Brouwer, E.; Tice, J.A.; Seidner, M.; Loos, A.M.; Liu, S.; Chapman, R.H.; Kumar, V.; Carlson, J.J. Disease-Modifying Therapies for Relapsing-Remitting and Primary Progressive Multiple Sclerosis: A Cost-Utility Analysis. CNS Drugs 2018, 32, 1145–1157. [Google Scholar] [CrossRef] [PubMed]
- Andorra, M.; Nakamura, K.; Lampert, E.J.; Pulido-Valdeolivas, I.; Zubizarreta, I.; Llufriu, S.; Martinez-Heras, E.; Sola-Valls, N.; Sepulveda, M.; Tercero-Uribe, A.; et al. Assessing Biological and Methodological Aspects of Brain Volume Loss in Multiple Sclerosis. JAMA Neurol. 2018, 75, 1246–1255. [Google Scholar] [CrossRef] [PubMed]
- Confavreux, C.; Vukusic, S. Age at Disability Milestones in Multiple Sclerosis. Brain 2006, 129, 595–605. [Google Scholar] [CrossRef] [Green Version]





| Strategy | Criteria for Detecting Disease Activity | Parameter Choices * |
|---|---|---|
| without MRI | at least nrelapse clinical relapses or EDSS disability progression ** | nrelapse: {1, 2, 3} |
| NEDA-3 (visual) | same as “without MRI” or at least nlesion new lesions, but only a proportion plesion of true lesions are caught | nlesion: {1, 2, 3, 4} plesion: 33%, 66% |
| NEDA-3 (software) | same as “NEDA-3 (visual)” | nlesion: {1, 2, 3, 4} plesion: 90%, 100% |
| NEDA-4 (software) | same as “NEDA-3 (software)” or annualized whole brain volume loss > α% measurement error between two consecutive scans: ±ε% | α: {0.4, 0.52, 0.72} ε: {0.1, 0.2, 0.3} |
| Therapy Family | Relative Risk of Disability Progression c | Rate Ratio for Relapse Rate c | Rate Ratio for New Lesions d | aPBVC e |
|---|---|---|---|---|
| low efficacy a | 0.52–1.23 | 0.55–0.94 | 0.32–0.89 | −0.51% ± 0.27% |
| high efficacy b | 0.25–0.90 | 0.22–0.63 | 0.06–0.42 | −0.27% ± 0.15% |
| Year | Decision | Clinical without MRI | NEDA-3 (Visual) | NEDA-3 (Software) | NEDA-4 (Software) |
|---|---|---|---|---|---|
| 1 | stable | 72% | 58% | 40% | 22% |
| - truly stable | 22% | 22% | 22% | 18% | |
| - undetected disease activity | 50% | 36% | 18% | 4% | |
| active | 28% | 42% | 60% | 78% | |
| - true disease activity | 28% | 42% | 60% | 74% | |
| - false detection of disease activity | - | - | - | 4% | |
| reached EDSS 7 | 0% | 0% | 0% | 0% | |
| 5 | stable | 74% | 71% | 60% | 59% |
| - truly stable | 38% | 50% | 55% | 58% | |
| - undetected disease activity | 36% | 21% | 5% | 1% | |
| active | 24% | 28% | 39% | 41% | |
| - true disease activity | 24% | 28% | 39% | 37% | |
| - false detection of disease activity | - | - | - | 4% | |
| reached EDSS 7 | 2% | 1% | 1% | 0% | |
| 10 | stable | 75% | 72% | 62% | 60% |
| - truly stable | 46% | 54% | 59% | 59% | |
| - undetected disease activity | 29% | 18% | 3% | 1% | |
| active | 20% | 25% | 35% | 38% | |
| - true disease activity | 20% | 25% | 35% | 35% | |
| - false detection of disease activity | - | - | - | 3% | |
| reached EDSS 7 | 5% | 3% | 3% | 2% |
| Strategy | Utility | Incremental Utility Compared to | ||
|---|---|---|---|---|
| Clinical without MRI | NEDA-3 (Visual) | NEDA-3 (Software) | ||
| over a 10-year horizon | ||||
| Clinical without MRI | 6.48 ± 4.49 | - | - | - |
| NEDA-3 (visual) | 6.50 ± 4.63 | 0.03 ± 2.81 | - | - |
| NEDA-3 (software) | 6.67 ± 4.53 | 0.19 ± 2.80 | 0.16 ± 2.83 | - |
| NEDA-4 (software) | 6.71 ± 4.42 | 0.23 ± 2.79 | 0.20 ± 2.80 | 0.04 ± 2.81 |
| over a 15-year horizon | ||||
| Clinical without MRI | 9.45 ± 4.83 | - | - | - |
| NEDA-3 (visual) | 9.48 ± 4.97 | 0.03 ± 4.71 | - | - |
| NEDA-3 (software) | 9.78 ± 4.85 | 0.32 ± 4.68 | 0.29 ± 4.75 | - |
| NEDA-4 (software) | 9.83 ± 4.78 | 0.37 ± 4.63 | 0.34 ± 4.69 | 0.05 ± 4.67 |
| Strategy | Cost | Incremental Cost Compared to | ||
|---|---|---|---|---|
| Clinical without MRI | NEDA-3 (Visual) | NEDA-3 (Software) | ||
| in a 10-years horizon | ||||
| Clinical without MRI | $33,809 ± $15,918 | - | - | - |
| NEDA-3 (visual) | $33,176 ± $16,056 | −$633 ± $18,606 | - | - |
| NEDA-3 (software) | $32,272 ± $15,470 | −$1538 ± $18,759 | −$905 ± $18,686 | - |
| NEDA-4 (software) | $31,655 ± $15,104 | −$2155 ± $18,764 | −$1521 ± $18,661 | −$617 ± $18,384 |
| in a 15-years horizon | ||||
| Clinical without MRI | $35,142 ± $17,304 | - | - | - |
| NEDA-3 (visual) | $34,567 ± $17,437 | −$576 ± $21,718 | - | - |
| NEDA-3 (software) | $33,341 ± $16,565 | −$1800 ± $21,366 | −$1225 ± $21,348 | - |
| NEDA-4 (software) | $32,875 ± $16,567 | −$2267 ± $21,380 | −$1691 ± $21,467 | −$466 ± $20,831 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sima, D.M.; Esposito, G.; Van Hecke, W.; Ribbens, A.; Nagels, G.; Smeets, D. Health Economic Impact of Software-Assisted Brain MRI on Therapeutic Decision-Making and Outcomes of Relapsing-Remitting Multiple Sclerosis Patients—A Microsimulation Study. Brain Sci. 2021, 11, 1570. https://doi.org/10.3390/brainsci11121570
Sima DM, Esposito G, Van Hecke W, Ribbens A, Nagels G, Smeets D. Health Economic Impact of Software-Assisted Brain MRI on Therapeutic Decision-Making and Outcomes of Relapsing-Remitting Multiple Sclerosis Patients—A Microsimulation Study. Brain Sciences. 2021; 11(12):1570. https://doi.org/10.3390/brainsci11121570
Chicago/Turabian StyleSima, Diana M., Giovanni Esposito, Wim Van Hecke, Annemie Ribbens, Guy Nagels, and Dirk Smeets. 2021. "Health Economic Impact of Software-Assisted Brain MRI on Therapeutic Decision-Making and Outcomes of Relapsing-Remitting Multiple Sclerosis Patients—A Microsimulation Study" Brain Sciences 11, no. 12: 1570. https://doi.org/10.3390/brainsci11121570