
Alterations in Leg Muscle Glucose Uptake and Inter-Limb Asymmetry after a Single Session of tDCS in Four People with Multiple Sclerosis


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
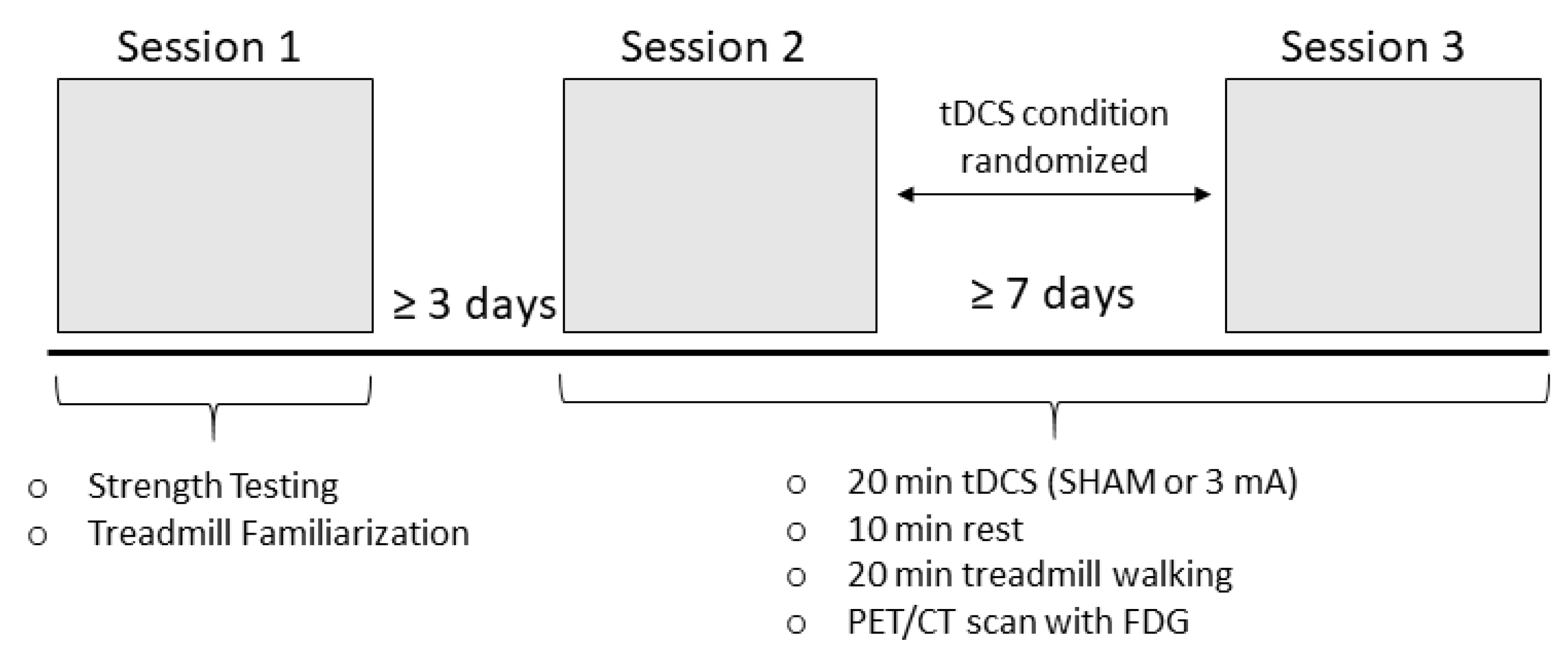
2.2. Experimental Protocol
2.3. Strength Testing
2.4. Transcranial Direct Current Stimulation
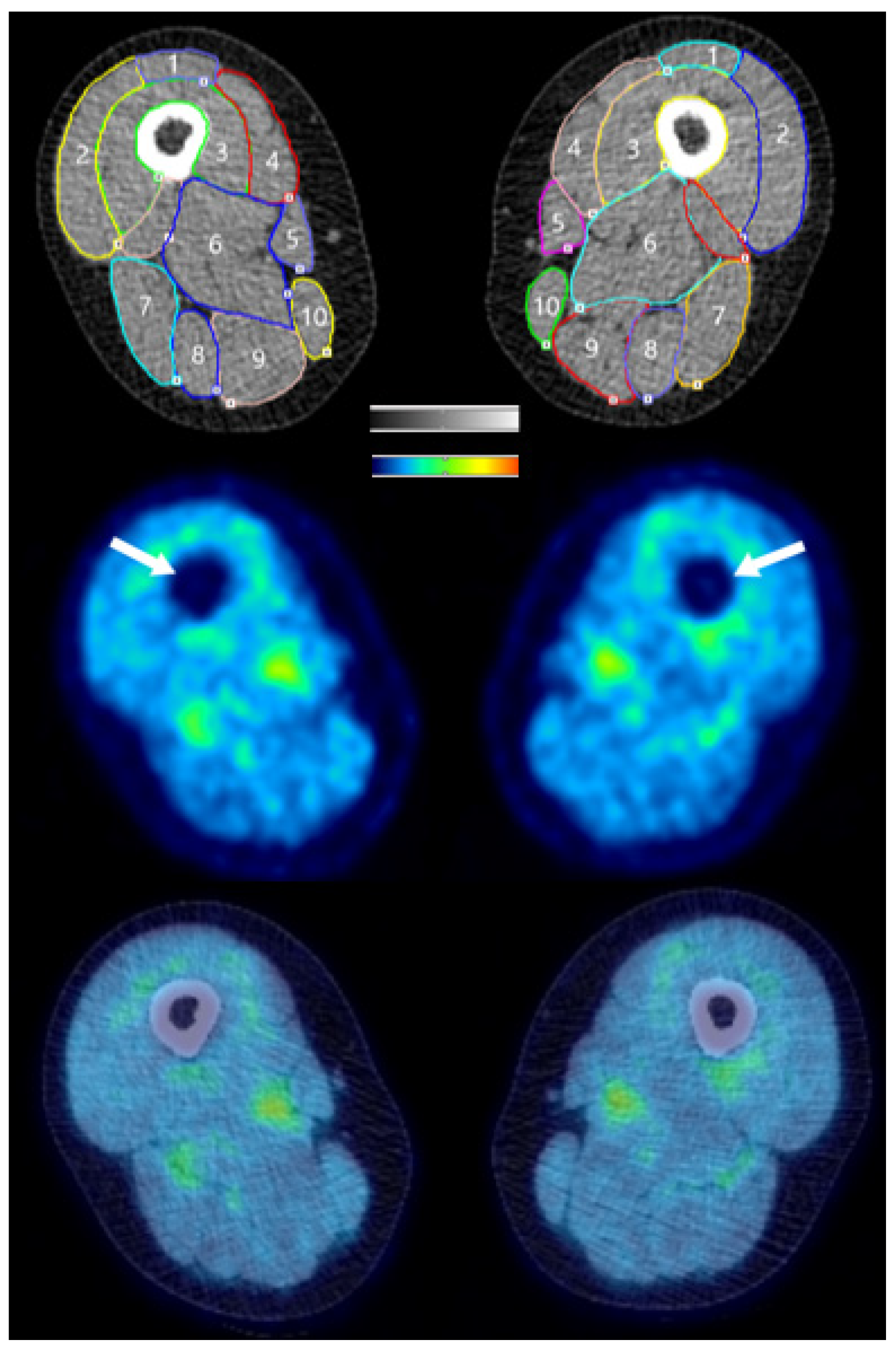
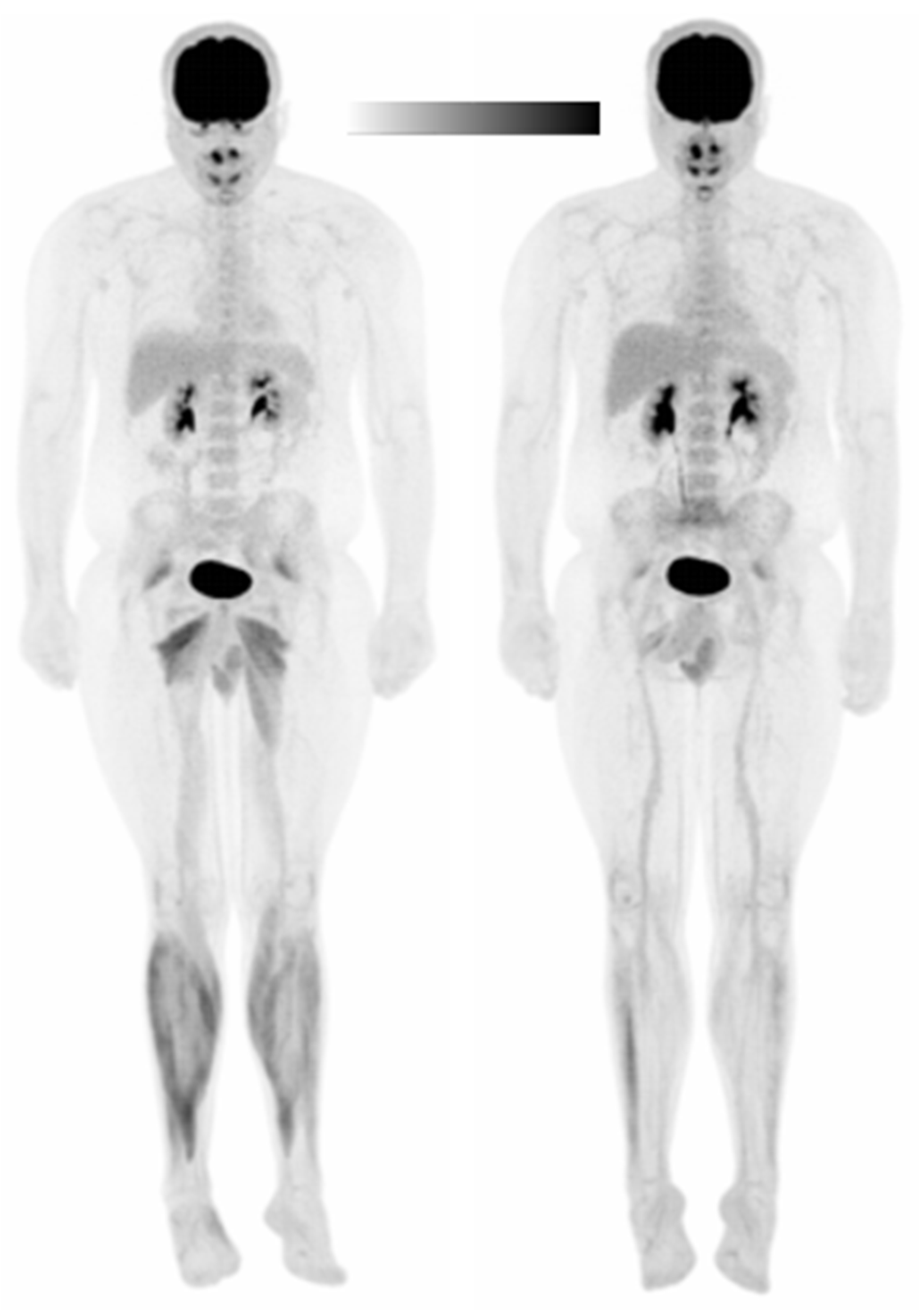
2.5. PET/CT Imaging
2.6. Data Analysis
2.7. Statistical Analysis
3. Results
3.1. Subject 1
3.1.1. Standardized Uptake Values (SUVs)
3.1.2. Asymmetry Indices (AIs)
3.1.3. Glucose Uptake Heterogeneity (GUh)
3.2. Subject 2
3.2.1. Standardized Uptake Values (SUVs)
3.2.2. Asymmetry Indices (AIs)
3.2.3. Glucose Uptake Heterogeneity (GUh)
3.3. Subject 3
3.3.1. Standardized Uptake Values (SUVs)
3.3.2. Asymmetry Indices (AIs)
3.3.3. Glucose Uptake Heterogeneity (GUh)
3.4. Subject 4
3.4.1. Standardized Uptake Values (SUVs)
3.4.2. Asymmetry Indices (AIs)
3.4.3. Glucose Uptake Heterogeneity (GUh)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Noseworthy, J.H.; Lucchinetti, C.; Rodriguez, M.; Weinshenker, B.G. Multiple Sclerosis. N. Engl. J. Med. 2000, 343, 938–952. [Google Scholar] [CrossRef]
- Chung, L.H.; Remelius, J.G.; VAN Emmerik, R.E.A.; Kent-Braun, J.A. Leg Power Asymmetry and Postural Control in Women with Multiple Sclerosis. Med. Sci. Sports Exerc. 2008, 40, 1717–1724. [Google Scholar] [CrossRef]
- Frzovic, D.; Morris, M.E.; Vowels, L. Clinical tests of standing balance: Performance of persons with multiple sclerosis. Arch. Phys. Med. Rehabil. 2000, 81, 215–221. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Paulus, W. Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. J. Physiol. 2000, 527 Pt 3, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Workman, C.; Kamholz, J.; Rudroff, T. The Tolerability and Efficacy of 4 mA Transcranial Direct Current Stimulation on Leg Muscle Fatigability. Brain Sci. 2019, 10, 12. [Google Scholar] [CrossRef] [Green Version]
- Workman, C.D.; Fietsam, A.C.; Rudroff, T. Tolerability and Blinding of Transcranial Direct Current Stimulation in People with Parkinson’s Disease: A Critical Review. Brain Sci. 2020, 10, 467. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Paulus, W. Sustained excitability elevations induced by transcranial DC motor cortex stimulation in humans. Neurology 2001, 57, 1899–1901. [Google Scholar] [CrossRef] [PubMed]
- Nitsche, M.A.; Nitsche, M.S.; Klein, C.C.; Tergau, F.; Rothwell, J.; Paulus, W. Level of action of cathodal DC polarisation induced inhibition of the human motor cortex. Clin. Neurophysiol. 2003, 114, 600–604. [Google Scholar] [CrossRef]
- van Asseldonk, E.H.; Boonstra, T.A. Transcranial Direct Current Stimulation of the Leg Motor Cortex Enhances Coordinated Motor Output During Walking With a Large Inter-Individual Variability. Brain Stimul. 2016, 9, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Hummel, F.C.; Heise, K.-F.; Celnik, P.; Floel, A.; Gerloff, C.; Cohen, L.G. Facilitating skilled right hand motor function in older subjects by anodal polarization over the left primary motor cortex. Neurobiol. Aging 2010, 31, 2160–2168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zandvliet, S.B.; Meskers, C.; Kwakkel, G.; Van Wegen, E.E.H. Short-Term Effects of Cerebellar tDCS on Standing Balance Performance in Patients with Chronic Stroke and Healthy Age-Matched Elderly. Cerebellum 2018, 17, 575–589. [Google Scholar] [CrossRef] [Green Version]
- Workman, C.D.; Fietsam, A.C.; Uc, E.Y.; Rudroff, T. Cerebellar Transcranial Direct Current Stimulation in People with Parkinson’s Disease: A Pilot Study. Brain Sci. 2020, 10, 96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Workman, C.; Kamholz, J.; Rudroff, T. Transcranial Direct Current Stimulation (tDCS) to Improve Gait in Multiple Sclerosis: A Timing Window Comparison. Front. Hum. Neurosci. 2019, 13, 420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilloni, G.; Choi, C.; Shaw, M.T.; Coghe, G.; Krupp, L.; Moffat, M.; Cocco, E.; Pau, M.; Charvet, L. Walking in multiple sclerosis improves with tDCS: A randomized, double-blind, sham-controlled study. Ann. Clin. Transl. Neurol. 2020, 7, 2310–2319. [Google Scholar] [CrossRef] [PubMed]
- Pilloni, G.; Choi, C.; Coghe, G.; Cocco, E.; Krupp, L.; Pau, M.; Charvet, L. Gait and Functional Mobility in Multiple Sclerosis: Immediate Effects of Transcranial Direct Current Stimulation (tDCS) Paired With Aerobic Exercise. Front. Neurol. 2020, 11, 310. [Google Scholar] [CrossRef]
- Sivaramakrishnan, A.; Hombali, A.S.; Shankar, R.; Fregni, F.; Thibaut, A. Transcranial direct current stimulation (tDCS) for improving fatigue, motor function, and pain in people with multiple sclerosis. Cochrane Database Syst. Rev. 2019. [Google Scholar] [CrossRef]
- Leray, E.; Moreau, T.; Fromont, A.; Edan, G. Epidemiology of multiple sclerosis. Rev. Neurol. 2016, 172, 3–13. [Google Scholar] [CrossRef]
- Rudroff, T.; Workman, C.; Fietsam, A.; Ponto, L. Imaging Transcranial Direct Current Stimulation (tDCS) with Positron Emission Tomography (PET). Brain Sci. 2020, 10, 236. [Google Scholar] [CrossRef] [Green Version]
- Farina, D.; Merletti, R.; Enoka, R.M. The extraction of neural strategies from the surface EMG. J. Appl. Physiol. 2004, 96, 1486–1495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rudroff, T.; Ketelhut, N.B.; Kindred, J.H. Metabolic imaging in exercise physiology. J. Appl. Physiol. 2018, 124, 497–503. [Google Scholar] [CrossRef] [Green Version]
- Olgiati, R.; Burgunder, J.M.; Mumenthaler, M. Increased energy cost of walking in multiple sclerosis: Effect of spasticity, ataxia, and weakness. Arch. Phys. Med. Rehabil. 1988, 69, 846–849. [Google Scholar]
- Olgiati, R.; Jacquet, J.; Di Prampero, P.E. Energy Cost of Walking and Exertional Dyspnea in Multiple Sclerosis1–3. Am. Rev. Respir. Dis. 1986, 134, 1005–1010. [Google Scholar] [CrossRef]
- Agiovlasitis, S.; Motl, R.; Fernhall, B. Prediction of oxygen uptake during level treadmill walking in people with multiple sclerosis. J. Rehabil. Med. 2010, 42, 650–655. [Google Scholar] [CrossRef] [Green Version]
- Wens, I.; Dalgas, U.; Vandenabeele, F.; Krekels, M.; Grevendonk, L.; Eijnde, B.O. Multiple Sclerosis Affects Skeletal Muscle Characteristics. PLoS ONE 2014, 9, e108158. [Google Scholar] [CrossRef] [PubMed]
- Kent-Braun, J.A.; Ng, A.V.; Castro, M.; Weiner, M.W.; Gelinas, D.; Dudley, G.A.; Miller, R.G. Strength, skeletal muscle composition, and enzyme activity in multiple sclerosis. J. Appl. Physiol. 1997, 83, 1998–2004. [Google Scholar] [CrossRef]
- Heinonen, I.; Nesterov, S.V.; Kemppainen, J.; Fujimoto, T.; Knuuti, J.; Kalliokoski, K.K. Increasing Exercise Intensity Reduces Heterogeneity of Glucose Uptake in Human Skeletal Muscles. PLoS ONE 2012, 7, e52191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kindred, J.H.; Ketelhut, N.B.; Rudroff, T. Glucose uptake heterogeneity of the leg muscles is similar between patients with multiple sclerosis and healthy controls during walking. Clin. Biomech. 2015, 30, 159–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rudroff, T.; Kindred, J.H.; Benson, J.-M.; Tracy, B.L.; Kalliokoski, K.K. Greater glucose uptake heterogeneity in knee muscles of old compared to young men during isometric contractions detected by [18F]-FDG PET/CT. Front. Physiol. 2014, 5, 198. [Google Scholar] [CrossRef] [Green Version]
- Abu-Zidan, F.M.; Abbas, A.K.; Hefny, A.F. Clinical "case series": A concept analysis. Afr. Health Sci. 2012, 12, 557–562. [Google Scholar] [CrossRef] [Green Version]
- Ng, A.V.; Miller, R.G.; Gelinas, D.; Kent-Braun, J.A. Functional relationships of central and peripheral muscle alterations in multiple sclerosis. Muscle Nerve 2004, 29, 843–852. [Google Scholar] [CrossRef] [PubMed]
- Garner, D.J.; Widrick, J.J. Cross-bridge mechanisms of muscle weakness in multiple sclerosis. Muscle Nerve 2003, 27, 456–464. [Google Scholar] [CrossRef]
- Fietsam, A.; Workman, C.; Ponto, L.; Kamholz, J.; Rudroff, T. Different Effects of Transcranial Direct Current Stimulation on Leg Muscle Glucose Uptake Asymmetry in Two Women with Multiple Sclerosis. Brain Sci. 2020, 10, 549. [Google Scholar] [CrossRef]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Thompson, P.D.; Arena, R.; Riebe, D.; Pescatello, L.S. ACSM’s New Preparticipation Health Screening Recommendations from ACSM’s Guidelines for Exercise Testing and Prescription, Ninth Edition. Curr. Sports Med. Rep. 2013, 12, 215–217. [Google Scholar] [CrossRef] [PubMed]
- Giesser, B.S. Exercise in the management of persons with multiple sclerosis. Ther. Adv. Neurol. Disord. 2015, 8, 123–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halabchi, F.; Ali, S.M.; Sahraian, M.A.; Abolhasani, M. Exercise prescription for patients with multiple sclerosis; potential benefits and practical recommendations. BMC Neurol. 2017, 17, 1–11. [Google Scholar] [CrossRef]
- Batsikadze, G.; Moliadze, V.; Paulus, W.; Kuo, M.-F.; Nitsche, M.A. Partially non-linear stimulation intensity-dependent effects of direct current stimulation on motor cortex excitability in humans. J. Physiol. 2013, 591, 1987–2000. [Google Scholar] [CrossRef] [PubMed]
- Learmonth, Y.C.; Motl, R.W.; Sandroff, B.M.; Pula, J.H.; Cadavid, D. Validation of patient determined disease steps (PDDS) scale scores in persons with multiple sclerosis. BMC Neurol. 2013, 13, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.G.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 328–354. [Google Scholar] [CrossRef]
- Delbeke, D.; Coleman, R.E.; Guiberteau, M.J.; Brown, M.L.; Royal, H.D.; Siegel, B.A.; Townsend, D.W.; Berland, L.L.; Parker, J.A.; Hubner, K.; et al. Procedure guideline for tumor imaging with 18F-FDG PET/CT 1.0. J. Nucl. Med. 2006, 47, 885–895. [Google Scholar]
- Jeffery, D.T.; Norton, J.A.; Roy, F.D.; Gorassini, M.A. Effects of transcranial direct current stimulation on the excitability of the leg motor cortex. Exp. Brain Res. 2007, 182, 281–287. [Google Scholar] [CrossRef]
- Esantarnecchi, E.; Feurra, M.; Ebarneschi, F.; Acampa, M.; Ebianco, G.; Ecioncoloni, D.; Erossi, A.; Rossi, S. Time Course of Corticospinal Excitability and Autonomic Function Interplay during and Following Monopolar tDCS. Front. Psychiatry 2014, 5, 86. [Google Scholar] [CrossRef] [Green Version]
- Klem, G.H.; Lüders, H.O.; Jasper, H.H.; Elger, C. The ten-twenty electrode system of the International Federation. The International Federation of Clinical Neurophysiology. Electroencephalogr. Clin. Neurophysiol. Suppl. 1999, 52, 3–6. [Google Scholar]
- Foerster, Á.; Yavari, F.; Farnad, L.; Jamil, A.; Paulus, W.; Nitsche, M.A.; Kuo, M.-F. Effects of electrode angle-orientation on the impact of transcranial direct current stimulation on motor cortex excitability. Brain Stimul. 2019, 12, 263–266. [Google Scholar] [CrossRef] [PubMed]
- Schambra, H.M.; Abe, M.; Luckenbaugh, D.A.; Reis, J.; Krakauer, J.W.; Cohen, L.G. Probing for hemispheric specialization for motor skill learning: A transcranial direct current stimulation study. J. Neurophysiol. 2011, 106, 652–661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foerster, Á.S.; Rezaee, Z.; Paulus, W.; Nitsche, M.A.; Dutta, A. Effects of Cathode Location and the Size of Anode on Anodal Transcranial Direct Current Stimulation Over the Leg Motor Area in Healthy Humans. Front. Neurosci. 2018, 12, 443. [Google Scholar] [CrossRef]
- Jayaram, G.; Stinear, J.W. The Effects of Transcranial Stimulation on Paretic Lower Limb Motor Excitability During Walking. J. Clin. Neurophysiol. 2009, 26, 272–279. [Google Scholar] [CrossRef]
- Agboada, D.; Samani, M.M.; Jamil, A.; Kuo, M.-F.; Nitsche, M.A. Expanding the parameter space of anodal transcranial direct current stimulation of the primary motor cortex. Sci. Rep. 2019, 9, 1–11. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Bikson, M. Extending the parameter range for tDCS: Safety and tolerability of 4 mA stimulation. Brain Stimul. 2017, 10, 541–542. [Google Scholar] [CrossRef]
- Workman, C.; Kamholz, J.; Rudroff, T. Increased leg muscle fatigability during 2 mA and 4 mA transcranial direct current stimulation over the left motor cortex. Exp. Brain Res. 2020, 238, 333–343. [Google Scholar] [CrossRef] [PubMed]
- Khadka, N.; Borges, H.; Paneri, B.; Kaufman, T.; Nassis, E.; Zannou, A.L.; Shin, Y.; Choi, H.; Kim, S.; Lee, K.; et al. Adaptive current tDCS up to 4 mA. Brain Stimul. 2020, 13, 69–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bikson, M.; Grossman, P.; Thomas, C.; Zannou, A.L.; Jiang, J.; Adnan, T.; Mourdoukoutas, A.P.; Kronberg, G.; Truong, D.; Boggio, P.; et al. Safety of Transcranial Direct Current Stimulation: Evidence Based Update 2016. Brain Stimul. 2016, 9, 641–661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rudroff, T.; Kindred, J.H.; Kalliokoski, K. [18F]-FDG positron emission tomography—An established clinical tool opening a new window into exercise physiology. J. Appl. Physiol. 2015, 118, 1181–1190. [Google Scholar] [CrossRef]
- Zasadny, K.R.; Wahl, R.L. Standardized uptake values of normal tissues at PET with 2-[fluorine-18]-fluoro-2-deoxy-D-glucose: Variations with body weight and a method for correction. Radiology 1993, 189, 847–850. [Google Scholar] [CrossRef] [PubMed]
- Paquet, N.; Albert, A.; Foidart, J.; Hustinx, R. Within-patient variability of (18)F-FDG: Standardized uptake values in normal tissues. J. Nucl. Med. 2004, 45, 784–788. [Google Scholar]
- Ramos, C.D.; Erdi, Y.E.; Gonen, M.; Riedel, E.; Yeung, H.W.D.; Macapinlac, H.A.; Chisin, R.; Larson, S.M. FDG-PET standardized uptake values in normal anatomical structures using iterative reconstruction segmented attenuation correction and filtered back-projection. Eur. J. Nucl. Med. Mol. Imaging 2001, 28, 155–164. [Google Scholar] [CrossRef]
- Proessl, F.; Ketelhut, N.B.; Rudroff, T. No association of leg strength asymmetry with walking ability, fatigability, and fatigue in multiple sclerosis. Int. J. Rehabil. Res. 2018, 41, 267–269. [Google Scholar] [CrossRef]
- Ithurburn, M.; Paterno, M.V.; Ford, K.; Hewett, T.E.; Schmitt, L.C. Young Athletes With Quadriceps Femoris Strength Asymmetry at Return to Sport After Anterior Cruciate Ligament Reconstruction Demonstrate Asymmetric Single-Leg Drop-Landing Mechanics. Am. J. Sports Med. 2015, 43, 2727–2737. [Google Scholar] [CrossRef]
- Takakusaki, K. Neurophysiology of gait: From the spinal cord to the frontal lobe. Mov. Disord. 2013, 28, 1483–1491. [Google Scholar] [CrossRef]
- Van de Crommert, H.W.; Mulder, T.; Duysens, J. Neural control of locomotion: Sensory control of the central pattern generator and its relation to treadmill training. Gait Posture 1998, 7, 251–263. [Google Scholar] [CrossRef]
- Duysens, J.; Pearson, K. From cat to man: Basic aspects of locomotion relevant to motor rehabilitation of SCI. NeuroRehabilitation 1998, 10, 107–118. [Google Scholar] [CrossRef] [PubMed]
- Filli, L.; Sutter, T.; Easthope, C.S.; Killeen, T.; Meyer, C.; Reuter, K.; Lörincz, L.; Bolliger, M.; Weller, M.; Curt, A.; et al. Profiling walking dysfunction in multiple sclerosis: Characterisation, classification and progression over time. Sci. Rep. 2018, 8, 4984. [Google Scholar] [CrossRef]
- Barthélemy, D.; Grey, M.J.; Nielsen, J.B.; Bouyer, L. Involvement of the corticospinal tract in the control of human gait. Adv. Vasopressin Oxytocin Genes Behav. Dis. 2011, 192, 181–197. [Google Scholar] [CrossRef]
- Meinders, A.G.M. The role of ankle plantar flexor muscle work during walking. Scand. J. Rehabil. Med. 1998, 30, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Workman, C.D.; Fietsam, A.C.; Rudroff, T. Associations of lower limb joint asymmetry with fatigue and disability in people with multiple sclerosis. Clin. Biomech. 2020, 75, 104989. [Google Scholar] [CrossRef]
- Andreasen, A.; Jakobsen, J.; Soerensen, L.; Andersen, H.; Petersen, T.; Bjarkam, C.; Ahdidan, J. Regional brain atrophy in primary fatigued patients with multiple sclerosis. NeuroImage 2010, 50, 608–615. [Google Scholar] [CrossRef]
- Lambert, C.P.; Archer, R.L.; Evans, W.J. Muscle strength and fatigue during isokinetic exercise in individuals with multiple sclerosis. Med. Sci. Sports Exerc. 2001, 33, 1613–1619. [Google Scholar] [CrossRef]
- Wagner, J.M.; Kremer, T.; Van Dillen, L.R.; Naismith, R.T. Plantarflexor Weakness Negatively Impacts Walking in Persons With Multiple Sclerosis More Than Plantarflexor Spasticity. Arch. Phys. Med. Rehabil. 2014, 95, 1358–1365. [Google Scholar] [CrossRef] [Green Version]
- Vogt, J.; Paul, F.; Aktas, O.; Müller-Wielsch, K.; Dörr, J.; Dörr, S.; Bharathi, B.S.; Glumm, R.; Schmitz, C.; Steinbusch, H.; et al. Lower motor neuron loss in multiple sclerosis and experimental autoimmune encephalomyelitis. Ann. Neurol. 2009, 66, 310–322. [Google Scholar] [CrossRef]
- Ahmed, Z. Modulation of gamma and alpha spinal motor neurons activity by trans-spinal direct current stimulation: Effects on reflexive actions and locomotor activity. Physiol. Rep. 2016, 4, e12696. [Google Scholar] [CrossRef]
- Workman, C.; Fietsam, A.; Rudroff, T. Transcranial Direct Current Stimulation at 4 mA Induces Greater Leg Muscle Fatigability in Women Compared to Men. Brain Sci. 2020, 10, 244. [Google Scholar] [CrossRef] [Green Version]
- Vaghefi, E.; Cai, P.; Fang, F.; Byblow, W.; Stinear, C.; Thompson, B. MRI Guided Brain Stimulation without the Use of a Neuronavigation System. BioMed Res. Int. 2015, 2015, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Datta, A.; Bansal, V.; Diaz, J.; Patel, J.; Reato, D.; Bikson, M. Gyri-precise head model of transcranial direct current stimulation: Improved spatial focality using a ring electrode versus conventional rectangular pad. Brain Stimul. 2009, 2, 201–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mondini, V.; Mangia, A.L.; Cappello, A. Single-session tDCS over the dominant hemisphere affects contralateral spectral EEG power, but does not enhance neurofeedback-guided event-related desynchronization of the non-dominant hemisphere’s sensorimotor rhythm. PLoS ONE 2018, 13, e0193004. [Google Scholar] [CrossRef] [Green Version]
- Park, C.-H.; Chang, W.H.; Park, J.-Y.; Shin, Y.-I.; Kim, S.T.; Kim, Y.-H. Transcranial direct current stimulation increases resting state interhemispheric connectivity. Neurosci. Lett. 2013, 539, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Waters, S.; Wiestler, T.; Diedrichsen, J. Cooperation Not Competition: Bihemispheric tDCS and fMRI Show Role for Ipsilateral Hemisphere in Motor Learning. J. Neurosci. 2017, 37, 7500–7512. [Google Scholar] [CrossRef] [Green Version]
- Turi, Z.; Csifcsák, G.; Boayue, N.M.; Aslaksen, P.; Antal, A.; Paulus, W.; Groot, J.; Hawkins, G.E.; Forstmann, B.; Opitz, A.; et al. Blinding is compromised for transcranial direct current stimulation at 1 mA for 20 min in young healthy adults. Eur. J. Neurosci. 2019, 50, 3261–3268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Connell, N.E.; Cossar, J.; Marston, L.; Wand, B.M.; Bunce, D.; Moseley, L.; De Souza, L.H. Rethinking Clinical Trials of Transcranial Direct Current Stimulation: Participant and Assessor Blinding Is Inadequate at Intensities of 2mA. PLoS ONE 2012, 7, e47514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fonteneau, C.; Mondino, M.; Arns, M.; Baeken, C.; Bikson, M.; Brunoni, A.R.; Burke, M.J.; Neuvonen, T.; Padberg, F.; Pascual-Leone, A.; et al. Sham tDCS: A hidden source of variability? Reflections for further blinded, controlled trials. Brain Stimul. 2019, 12, 668–673. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Subject | Sex | Age (years) | Height (cm) | Weight (kg) | BMI | PDDS | Time Since Diagnosis | Physically Active * |
|---|---|---|---|---|---|---|---|---|
| Subject 1 | M | 27 | 168 | 81 | 28.7 | 0.0 | 12 years | No |
| Subject 2 | M | 44 | 183 | 95 | 28.4 | 0.0 | 2 years | No |
| Subject 3 | M | 52 | 191 | 111 | 30.4 | 3.0 | 10 years | No |
| Subject 4 | F | 57 | 165 | 51 | 18.7 | 3.0 | 32 years | Yes |
| NN MA Leg | NN LA Leg | NL MA Leg | NL LA Leg | |||||
|---|---|---|---|---|---|---|---|---|
| SHAM | tDCS | SHAM | tDCS | SHAM | tDCS | SHAM | tDCS | |
| Knee Extensors | ||||||||
| Subject 1 | 0.48 ± 0.09 | 0.52 ± 0.08 | 0.50 ± 0.07 | 0.54 ± 0.07 ± | 0.25 ± 0.05 | 0.26 ± 0.04 | 0.25 ± 0.04 | 0.27 ± 0.03 ± |
| Subject 2 | 0.59 ± 0.07 | 0.59 ± 0.06 | 0.60 ± 0.07 | 0.59 ± 0.06 | 0.25 ± 0.03 | 0.24 ± 0.02 | 0.25 ± 0.03 | 0.24 ± 0.02 |
| Subject 3 | 0.72 ± 0.13 | 0.61 ± 0.07 | 0.61 ± 0.05 | 0.55 ± 0.05 | 0.30 ± 0.05 | 0.26 ± 0.03 | 0.25 ± 0.02 | 0.24 ± 0.02 |
| Subject 4 | 0.69 ± 0.06 | 0.67 ± 0.05 | 0.69 ± 0.06 | 0.66 ± 0.04 | 0.40 ± 0.03 | 0.39 ± 0.03 | 0.40 ± 0.03 | 0.38 ± 0.03 |
| Knee Flexors | ||||||||
| Subject 1 | 0.66 ± 0.28 | 0.56 ± 0.04 | 0.63 ± 0.20 | 0.57 ± 0.03 | 0.33 ± 0.14 | 0.28 ± 0.02 | 0.32 ± 0.10 | 0.28 ± 0.02 |
| Subject 2 | 0.64 ± 0.05 | 0.66 ± 0.05 ± | 0.61 ± 0.05 | 0.62 ± 0.04 | 0.27 ± 0.02 | 0.27 ± 0.02 | 0.26 ± 0.02 | 0.26 ± 0.02 |
| Subject 3 | 0.69 ± 0.08 | 0.70 ± 0.08 | 0.62 ± 0.10 | 0.68 ± 0.21 | 0.29 ± 0.03 | 0.30 ± 0.04 | 0.26 ± 0.04 | 0.29 ± 0.09 |
| Subject 4 | 0.66 ± 0.06 | 0.65 ± 0.06 | 0.65 ± 0.05 | 0.63 ± 0.05 * | 0.38 ± 0.04 | 0.38 ± 0.03 | 0.38 ± 0.03 | 0.36 ± 0.03 * |
| Plantar Flexors | ||||||||
| Subject 1 | 2.17 ± 0.60 | 0.99 ± 0.09 * | 1.81 ± 0.60 | 1.03 ± 0.14 * | 1.10 ± 0.30 | 0.49 ± 0.05 * | 0.92 ± 0.30 | 0.51 ± 0.07 * |
| Subject 2 | 1.39 ± 0.82 | 1.01 ± 0.20 | 1.12 ± 0.54 | 0.95 ± 0.19 | 0.59 ± 0.35 | 0.42 ± 0.08 | 0.48 ± 0.23 | 0.39 ± 0.08 |
| Subject 3 | 0.96 ± 0.10 | 0.96 ± 0.07 | 0.81 ± 0.09 | 0.93 ± 0.12 ± | 0.40 ± 0.04 | 0.41 ± 0.03 | 0.34 ± 0.04 | 0.40 ± 0.05 ± |
| Subject 4 | 1.00 ± 0.14 | 1.01 ± 0.14 | 1.01 ± 0.13 | 1.09 ± 0.19 ± | 0.58 ± 0.08 | 0.58 ± 0.08 | 0.58 ± 0.08 | 0.63 ± 0.11 ± |
| Dorsiflexors | ||||||||
| Subject 1 | 2.39 ± 0.20 | 1.78 ± 0.21 * | 2.25 ± 0.06 | 1.45 ± 0.14 * | 1.21 ± 0.10 | 0.88 ± 0.10 * | 1.14 ± 0.03 | 0.72 ± 0.07 * |
| Subject 2 | 1.01 ± 0.15 | 1.06 ± 0.13 | 1.54 ± 0.34 | 1.05 ± 0.15 * | 0.43 ± 0.06 | 0.44 ± 0.05 | 0.66 ± 0.15 | 0.43 ± 0.06 * |
| Subject 3 | 1.36 ± 0.08 | 1.32 ± 0.10 | 1.06 ± 0.14 | 1.24 ± 0.26 | 0.56 ± 0.03 | 0.57 ± 0.04 | 0.44 ± 0.06 | 0.53 ± 0.11 |
| Subject 4 | 1.10 ± 0.11 | 1.12 ± 0.14 | 1.07 ± 0.07 | 1.08 ± 0.10 | 0.63 ± 0.06 | 0.65 ± 0.08 | 0.62 ± 0.04 | 0.62 ± 0.06 |
| Knee Extensors | Knee Flexors | Plantar Flexors | Dorsiflexors | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Subject | SHAM | tDCS | ΔAI | SHAM | tDCS | ΔAI | SHAM | tDCS | ΔAI | SHAM | tDCS | ΔAI |
| Subject 1 | 3.23 | 3.47 | −0.24 | −4.28 | 2.21 | −6.50 | −17.88 | 3.58 | −21.46 | −6.02 | −20.39 | 14.37 |
| Subject 2 | 1.08 | 0.10 | 0.99 | −4.17 | −6.45 | 2.28 | −21.22 | −7.00 | −14.22 | 41.94 | −1.03 | 42.97 |
| Subject 3 | −16.90 | −10.71 | −6.19 | −10.29 | −3.45 | −6.84 | −15.86 | −3.12 | −12.73 | −25.21 | −6.76 | −18.45 |
| Subject 4 | 0.02 | −1.11 | 1.13 | −1.00 | −3.67 | 2.66 | 1.12 | 7.52 | −6.40 | −1.99 | 1.38 | −3.37 |
| MA Leg | LA Leg | |||||||
|---|---|---|---|---|---|---|---|---|
| SHAM | tDCS | ΔGUh | % GUh Change | SHAM | tDCS | ΔGUh | % GUh Change | |
| Knee Extensors | ||||||||
| Subject 1 | 22.54 ± 6.21 | 21.27 ± 3.41 | −1.27 ± 5.91 | −1.5 ± 27.46 | 21.16 ± 6.10 | 22.37 ± 6.52 | 1.21 ± 6.33 | 7.86 ± 28.99 |
| Subject 2 | 25.81 ± 15.43 | 22.75 ± 2.47 | −3.06 ± 14.00 | 4.12 ± 35.77 | 24.86 ± 16.43 | 23.36 ± 5.74 | −1.50 ± 11.33 | 9.98 ± 33.14 |
| Subject 3 | 26.02 ± 8.64 | 21.77 ± 5.61 | −4.25 ± 5.96 | −14.03 ± 18.01 | 29.44 ± 14.81 | 25.35 ± 11.31 | −4.09 ± 5.61 | −10.39 ± 17.49 |
| Subject 4 | 19.50 ± 4.65 | 20.37 ± 4.88 | 0.87 ± 0.83 | 4.61 ± 4.97 | 18.71 ± 4.62 | 19.01 ± 4.53 | 0.31 ± 0.77 | 1.96 ± 4.95 |
| Knee Flexors | ||||||||
| Subject 1 | 23.59 ± 4.59 | 22.67 ± 7.61 | −0.92 ± 8.50 | −1.3 ± 33.32 | 27.40 ± 7.80 | 22.43 ± 7.88 | −4.96 ± 9.53 | −13.98 ± 30.54 |
| Subject 2 | 19.17 ± 2.87 | 20.22 ± 3.26 | 1.05 ± 2.66 | 6.42 ± 16.43 | 20.25 ± 2.77 | 21.19 ± 4.53 | 0.94 ± 2.36 | 4.04 ± 10.25 |
| Subject 3 | 22.37 ± 5.75 | 19.42 ± 3.66 * | −2.95 ± 2.43 | −10.43 ± 7.49 | 24.92 ± 4.21 | 21.89 ± 4.57 * | −3.02 ± 2.10 | −12.32 ± 5.84 |
| Subject 4 | 17.34 ± 4.72 | 15.63 ± 3.56 | −1.71 ± 2.15 | −8.55 ± 13.02 | 16.97 ± 3.04 | 15.56 ± 3.12 * | −1.41 ± 0.78 | −8.52 ± 6.00 |
| Plantar Flexors | ||||||||
| Subject 1 | 43.32 ± 21.42 | 28.69 ± 12.63 | −14.63 ± 18.85 | −25.4 ± 33.22 | 31.35 ± 6.17 | 24.34 ± 4.82 * | −7.01 ± 6.71 | −20.51 ± 17.47 |
| Subject 2 | 42.05 ± 15.45 | 30.72 ± 12.60 * | −11.33 ± 11.21 | −26.72 ± 22.81 | 38.47 ± 9.61 | 30.19 ± 14.91 | −8.28 ± 12.60 | −22.58 ± 33.19 |
| Subject 3 | 35.77 ± 8.41 | 20.74 ± 4.35 * | −15.03 ± 8.14 | −40.16 ± 15.40 | 34.28 ± 8.74 | 23.29 ± 5.05 * | −10.99 ± 9.83 | −28.63 ± 22.16 |
| Subject 4 | 21.08 ± 2.66 | 21.10 ± 3.33 | 0.02 ± 3.03 | 0.75 ± 15.07 | 20.74 ± 3.27 | 23.08 ± 3.96 | 2.33 ± 2.62 | 11.74 ± 12.07 |
| Dorsiflexors | ||||||||
| Subject 1 | 30.78 ± 12.71 | 33.41 ± 11.06 | 2.63 ± 6.13 | 11.30 ± 19.14 | 27.08 ± 8.46 | 22.99 ± 7.94 * | −4.09 ± 0.71 | −15.72 ± 3.75 |
| Subject 2 | 23.78 ± 3.08 | 19.93 ± 3.21 | −3.85 ± 4.24 | −15.43 ± 17.13 | 40.29 ± 4.21 | 18.98 ± 0.93 * | −21.30 ± 4.57 | −52.48 ± 6.01 |
| Subject 3 | 41.63 ± 11.95 | 24.07 ± 4.74 | −17.56 ± 9.97 | −40.55 ± 12.16 | 40.11 ± 18.96 | 24.87 ± 6.00 | −15.24 ± 14.54 | −33.32 ± 16.99 |
| Subject 4 | 19.39 ± 4.30 | 22.34 ± 8.43 | 2.95 ± 4.57 | 13.15 ± 20.94 | 17.01 ± 2.55 | 17.15 ± 3.91 | 0.14 ± 1.74 | 0.24 ± 9.41 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fietsam, A.C.; Deters, J.R.; Workman, C.D.; Ponto, L.L.B.; Rudroff, T. Alterations in Leg Muscle Glucose Uptake and Inter-Limb Asymmetry after a Single Session of tDCS in Four People with Multiple Sclerosis. Brain Sci. 2021, 11, 1363. https://doi.org/10.3390/brainsci11101363
Fietsam AC, Deters JR, Workman CD, Ponto LLB, Rudroff T. Alterations in Leg Muscle Glucose Uptake and Inter-Limb Asymmetry after a Single Session of tDCS in Four People with Multiple Sclerosis. Brain Sciences. 2021; 11(10):1363. https://doi.org/10.3390/brainsci11101363
Chicago/Turabian StyleFietsam, Alexandra C., Justin R. Deters, Craig D. Workman, Laura L. Boles Ponto, and Thorsten Rudroff. 2021. "Alterations in Leg Muscle Glucose Uptake and Inter-Limb Asymmetry after a Single Session of tDCS in Four People with Multiple Sclerosis" Brain Sciences 11, no. 10: 1363. https://doi.org/10.3390/brainsci11101363