
Accelerated Early Progression of Amyotrophic Lateral Sclerosis over the COVID-19 Pandemic

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
- (1)
- Group 2020 (G20): in the pandemic year, we diagnosed ALS in 38 patients and followed during the disease course (or censored date, 30 April 2021); 34 were included in the study, four excluded for missing data.
- (2)
- Group 2018 (G18): in 2018, we diagnosed ALS in 82 patients and followed during the disease course (or censored date, 30 April 2021): 31 were included in the study, 51 excluded for missing data (of these 51 patients, 27 were excluded as patients led to our center only for a second-opinion visit and/or for diagnosis confirmation from other Italian regions but not followed for whole disease course in our center).
2.2. Data Collection
2.3. Statistical Analyses
2.4. Data Availability
3. Results
3.1. Patient Characteristics
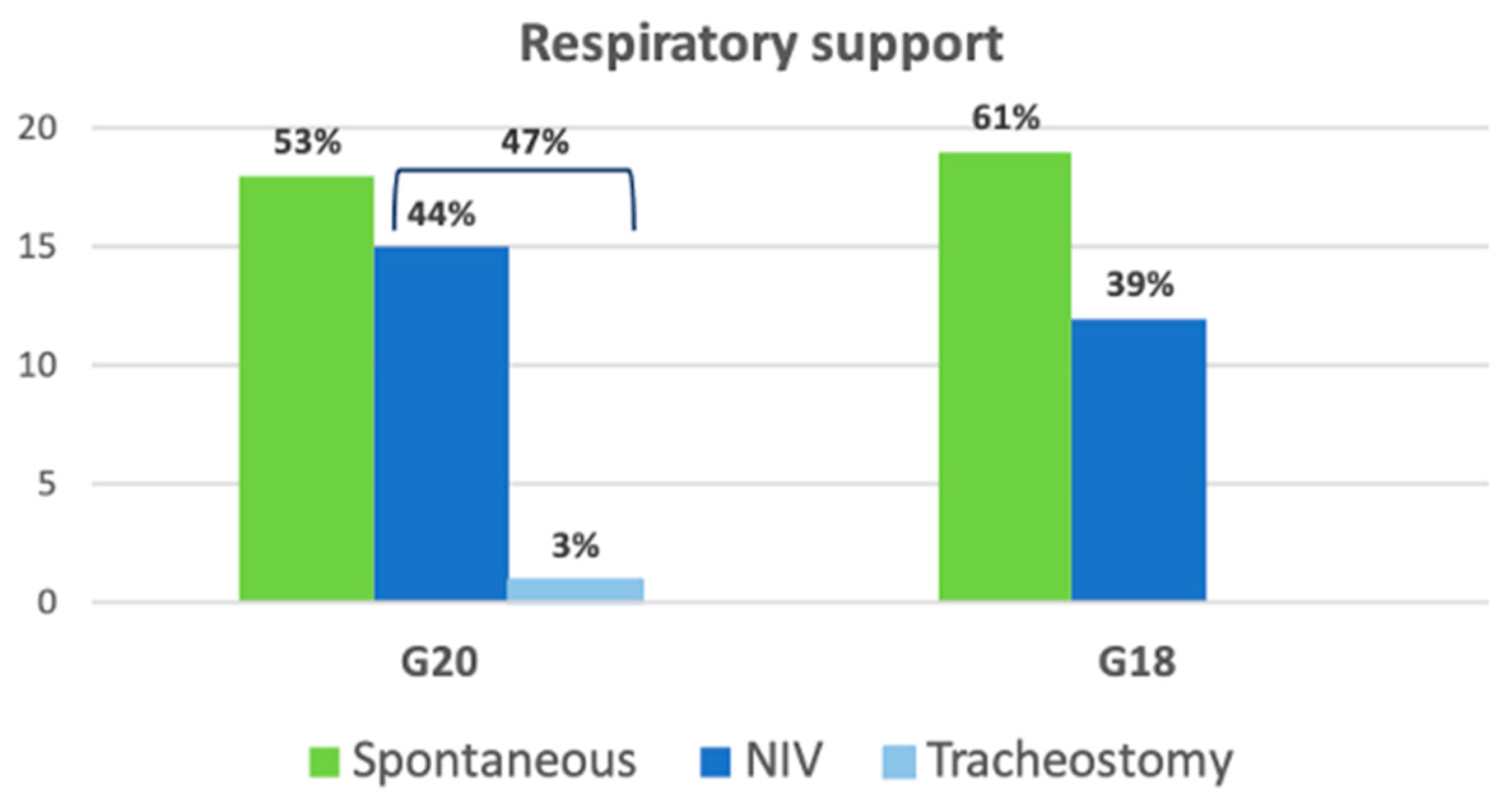
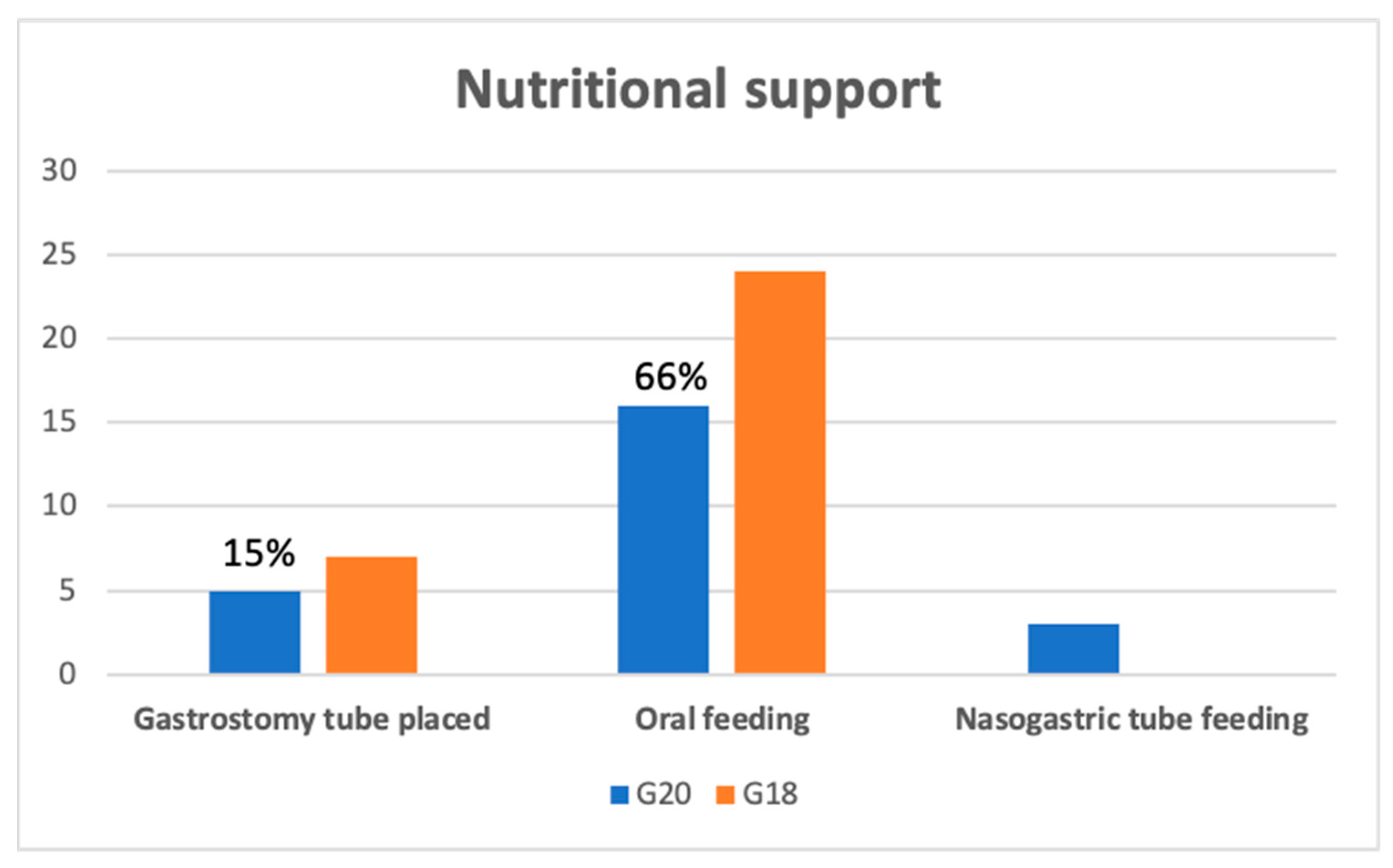
3.2. ALS Disease Progression in the First Year of the Disease
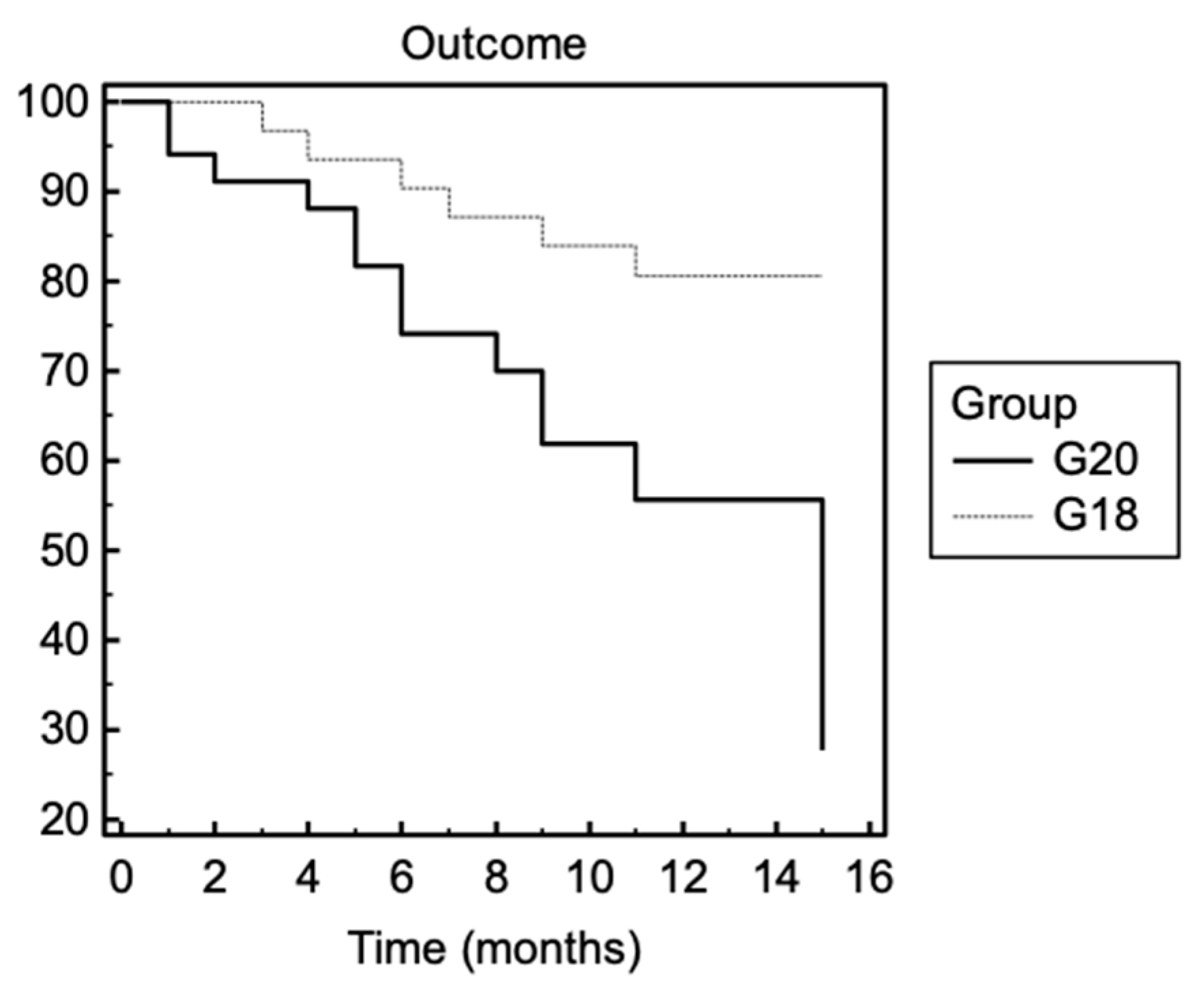
3.3. Survival
3.4. Psychological Assessment and Medication Use
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, X.; Bedlack, R. COVID-19-accelerated disease progression in two patients with amyotrophic lateral sclerosis. Muscle Nerve 2021, 64, E13–E15. [Google Scholar] [CrossRef] [PubMed]
- Digala, L.P.; Prasanna, S.; Rao, P.; Govindarajan, R.; Qureshi, A.I. Impact of COVID-19 Infection Among Hospitalized Amyotrophic Lateral Sclerosis Patients. J. Clin. Neuromuscul. Dis. 2021, 22, 180–181. [Google Scholar] [CrossRef] [PubMed]
- Galea, M.D.; Galea, V.P.; Eberhart, A.C.; Patwa, H.S.; Howard, I.; Fournier, C.N.; Bedlack, R. Infection rate, mortality and characteristics of veterans with amyotrophic lateral sclerosis with COVID-19. Muscle Nerve 2021, 64, E18–E20. [Google Scholar] [CrossRef] [PubMed]
- Helmich, R.C.; Bloem, B.R. The Impact of the COVID-19 Pandemic on Parkinson’s Disease: Hidden Sorrows and Emerging Opportunities. J. Parkinsons Dis. 2020, 10, 351–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boutoleau-Bretonnière, C.; Pouclet-Courtemanche, H.; Gillet, A.; Bernard, A.; Deruet, A.L.; Gouraud, I.; Mazoue, A.; Lamy, E.; Rocher, L.; Kapogiannis, D.; et al. The Effects of Confinement on Neuropsychiatric Symptoms in Alzheimer’s Disease During the COVID-19 Crisis. J. Alzheimers Dis. 2020, 76, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Pelicioni, P.H.S.; Schulz-Moore, J.S.; Hale, L.; Canning, C.G.; Lord, S.R. Lockdown During COVID-19 and the Increase of Frailty in People With Neurological Conditions. Front. Neurol. 2020, 11, 604299. [Google Scholar] [CrossRef] [PubMed]
- De Marchi, F.; Cantello, R.; Ambrosini, S.; Mazzini, L.; CANPALS Study Group. Telemedicine and technological devices for amyotrophic lateral sclerosis in the era of COVID-19. Neurol. Sci. 2020, 41, 1365–1367. [Google Scholar] [CrossRef] [PubMed]
- Esselin, F.; De La Cruz, E.; Pageot, N.; Juntas-Moralès, R.; Alphandéry, S.; Camu, W. Increased worsening of amyotrophic lateral sclerosis patients during COVID-19-related lockdown in France. Amyotroph. Lateral Scler. Front. Degener. 2021, 12, 1–3. [Google Scholar] [CrossRef]
- Ellis, T.; Motl, R.W. Physical activity behavior change in persons with neurologic disorders: Overview and examples from Parkinson disease and multiple sclerosis. J. Neurol. Phys. Ther. 2013, 37, 85–90. [Google Scholar] [CrossRef]
- De Lucia, N.; Ausiello, F.P.; Spisto, M.; Manganelli, F.; Salvatore, E.; Dubbioso, R. The emotional impact of COVID-19 outbreak in amyotrophic lateral sclerosis patients: Evaluation of depression, anxiety and interoceptive awareness. Neurol. Sci. 2020, 41, 2339–2341. [Google Scholar] [CrossRef]
- Consonni, M.; Telesca, A.; Dalla Bella, E.; Bersano, E.; Lauria, G. Amyotrophic lateral sclerosis patients’ and caregivers’ distress and loneliness during COVID-19 lockdown. J. Neurol. 2021, 268, 420–423. [Google Scholar] [CrossRef]
- Kurt, A.; Nijboer, F.; Matuz, T.; Kübler, A. Depression and anxiety in individuals with amyotrophic lateral sclerosis: Epidemiology and management. CNS Drugs 2007, 21, 279–291. [Google Scholar] [CrossRef]
- Oh, J.; Kim, J.A. Supportive care needs of patients with amyotrophic lateral sclerosis/motor neuron disease and their caregivers: A scoping review. J. Clin. Nurs. 2017, 26, 4129–4152. [Google Scholar] [CrossRef]
- EFNS Task Force on Diagnosis and Management of Amyotrophic Lateral Sclerosis; Andersen, P.M.; Abrahams, S.; Borasio, G.D.; de Carvalho, M.; Chio, A. EFNS guidelines on the clinical management of amyotrophic lateral sclerosis (MALS)—Revised report of an EFNS task force. Eur. J. Neurol. 2012, 19, 360–375. [Google Scholar] [CrossRef] [PubMed]
- Vasta, R.; D’ovidio, F.; Canosa, A.; Manera, U.; Torrieri, M.C.; Grassano, M. Plateaus in amyotrophic lateral sclerosis progression: Results from a population-based cohort. Eur. J. Neurol. 2020, 27, 1397–1404. [Google Scholar] [CrossRef] [PubMed]
- Cabona, C.; Ferraro, P.M.; Meo, G.; Roccatagliata, L.; Schenone, A.; Inglese, M.; Villani, F.; Caponnetto, C. Predictors of self-perceived health worsening over COVID-19 emergency in ALS. Neurol. Sci. 2021, 42, 1231–1236. [Google Scholar] [CrossRef] [PubMed]
- Giusiano, S.; Peotta, L.; Iazzolino, B.; Mastro, E.; Arcari, M.; Palumbo, F. Amyotrophic lateral sclerosis caregiver burden and patients’ quality of life during COVID-19 pandemic. Amyotroph. Lateral Scler. Front. Degener. 2021, 16, 1–3. [Google Scholar] [CrossRef]
- Gonçalves, F.; Magalhães, B. Effects of prolonged interruption of rehabilitation routines in amyotrophic lateral sclerosis patients. Palliat Support. Care 2021, 4, 1–6. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| G20 (n = 34) | G18 (n = 31) | p-Value | |
|---|---|---|---|
| Age (years) at onset (SD) | 66.23 (9.90) | 62.83 (13.43) | >0.05 |
| Male/Female (%) | 19 (56%)/ 15 (44%) | 15 (48%)/ 16 (52%) | >0.05 |
| Months from onset to diagnosis (IQR) | 9.00 (6.24–12.76) | 10.50 (6.00–12.00) | >0.05 |
| Phenotype (%): - spinal - bulbar | 24 (71%) 10 (29%) | 19 (61%) 12 (39%) | >0.05 |
| Cognition (%): - normal - impaired | 21 (62%) 13 (38%) | 23 (74%) 8 (26%) | >0.05 |
| Gene mutations (%): - negative - C9Orf72 | 31 (91%) 3 (9%) | 29 (94%) 2 (6%) | >0.05 |
| ALSFRS-R at baseline (SD) | 38.51 (5.34) | 39.03 (5.35) | >0.05 |
| FVC% at baseline (SD) | 75.41 (22.27) | 84.00 (16.63) | >0.05 |
| BMI at baseline (SD) | 23.90 (4.48) | 25.35 (5.36) | >0.05 |
| Outcome | G20 | G18 | p-Value |
|---|---|---|---|
| ΔALSFRS-R | 1.52 (2.69) | 0.76 (0.56) | 0.005 |
| ΔFVC% | 1.97 (1.50) | 1.74 (2.35) | >0.05 |
| ΔBMI | 0.25 (0.62) | 0.05 (0.20) | >0.05 |
| Scale | Score | Meaning |
|---|---|---|
| HADS–depression (mean, SD) | 6.86 (5.74) | Absence |
| HADS–anxiety (mean, SD) | 7.2 (5.95) | Mild level |
| ALSAQ-40–physical mobility (mean, SD) | 40.13 (29.66) | Problems sometimes |
| ALSAQ-40–independence (mean, SD) | 37.63 (27.48) | Problems rarely |
| ALSAQ-40–eating (mean, SD) | 39.00 (44.01) | Problems rarely |
| ALSAQ-40–communication (mean, SD) | 31.84 (41.65) | Problems rarely |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Marchi, F.; Gallo, C.; Sarnelli, M.F.; De Marchi, I.; Saraceno, M.; Cantello, R.; Mazzini, L. Accelerated Early Progression of Amyotrophic Lateral Sclerosis over the COVID-19 Pandemic. Brain Sci. 2021, 11, 1291. https://doi.org/10.3390/brainsci11101291
De Marchi F, Gallo C, Sarnelli MF, De Marchi I, Saraceno M, Cantello R, Mazzini L. Accelerated Early Progression of Amyotrophic Lateral Sclerosis over the COVID-19 Pandemic. Brain Sciences. 2021; 11(10):1291. https://doi.org/10.3390/brainsci11101291
Chicago/Turabian StyleDe Marchi, Fabiola, Chiara Gallo, Maria Francesca Sarnelli, Ilaria De Marchi, Massimo Saraceno, Roberto Cantello, and Letizia Mazzini. 2021. "Accelerated Early Progression of Amyotrophic Lateral Sclerosis over the COVID-19 Pandemic" Brain Sciences 11, no. 10: 1291. https://doi.org/10.3390/brainsci11101291