Effect of Brain Lesions on Voluntary Cough in Patients with Supratentorial Stroke: An Observational Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Clinical Assessment
2.3. Lesion Analysis
2.4. Respiratory Pressure Parameters
2.5. Swallowing Assessment
2.6. Statistical Analysis
3. Results
3.1. Clinical Assessment
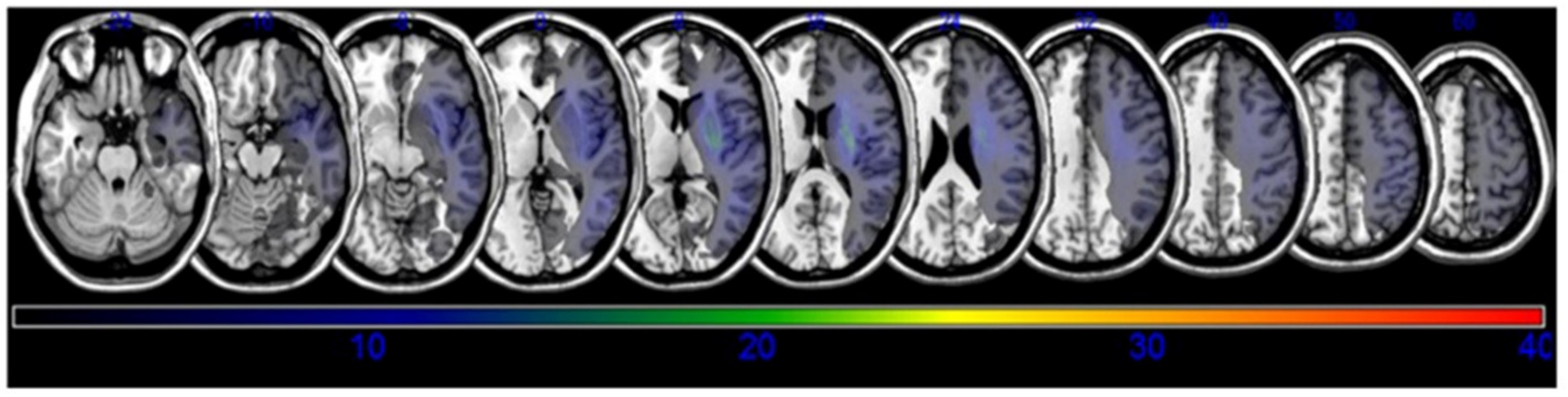
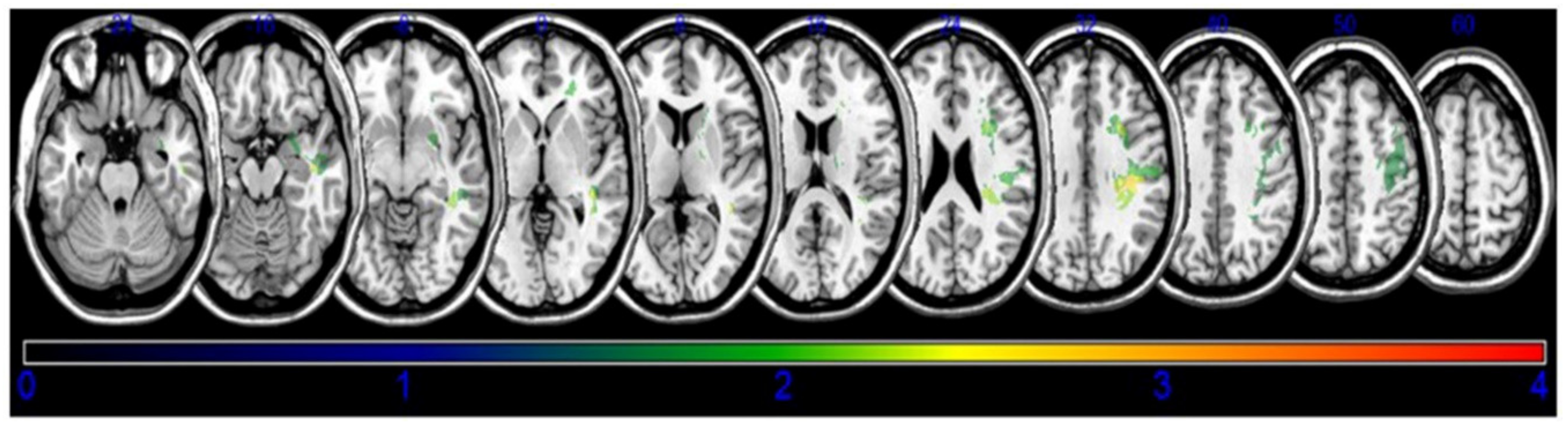
3.2. Lesion Analysis
3.3. Respiratory Pressure Parameters
3.4. Swallowing Parameters
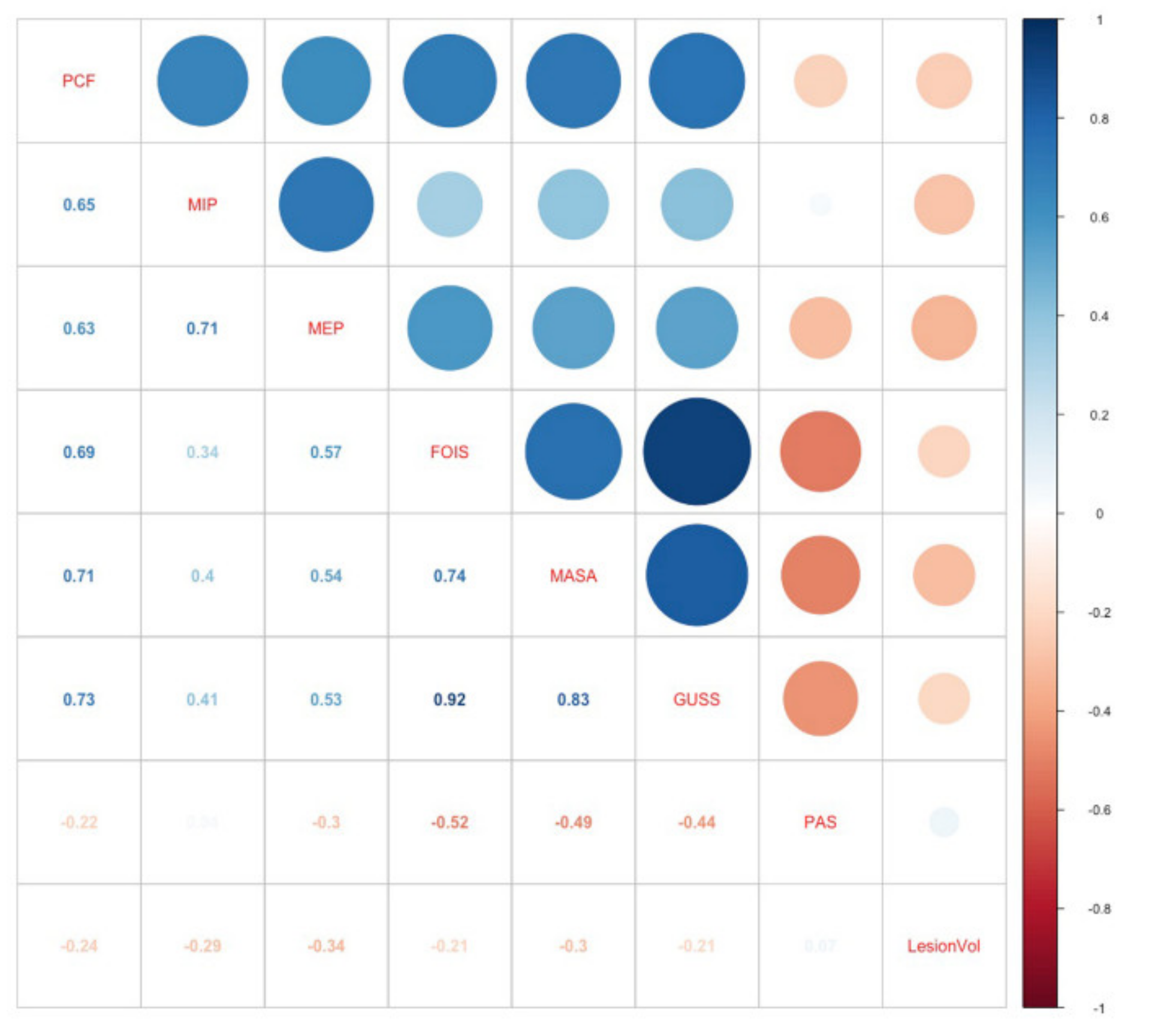
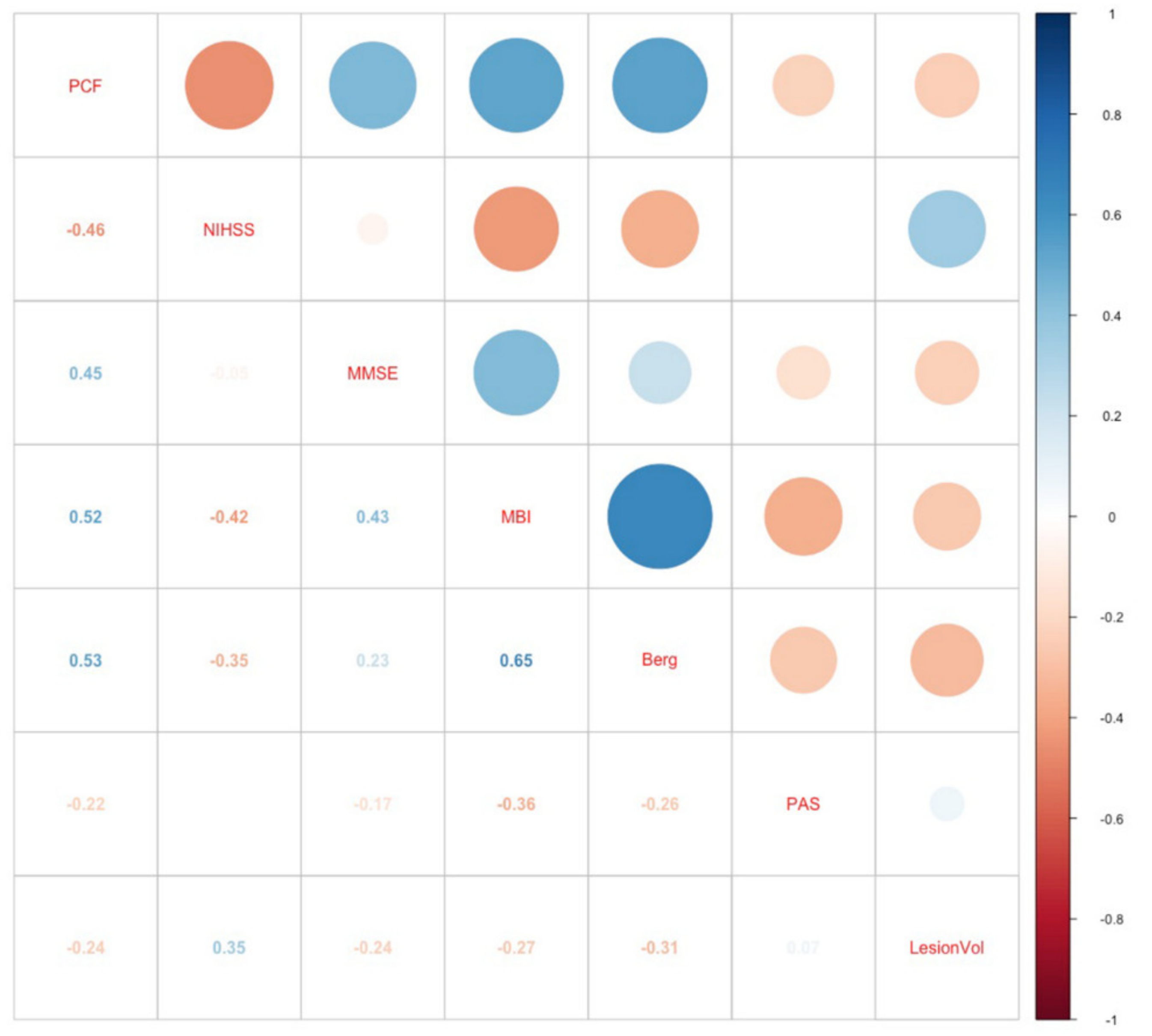
3.5. Correlation Analysis of PCF
3.6. Correlation Analysis of Lesion Volume
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Weimar, C.; Roth, M.P.; Zillessen, G.; Glahn, J.; Wimmer, M.L.; Busse, O.; Haberl, R.L.; Diener, H.C. Complications following acute ischemic stroke. Eur. Neurol. 2002, 48, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Troche, M.S.; Brandimore, A.E.; Godoy, J.; Hegland, K.W. A framework for understanding shared substrates of airway protection. J. Appl. Oral Sci. 2014, 22, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Park, G.Y.; Kim, S.R.; Kim, Y.W.; Jo, K.W.; Lee, E.J.; Kim, Y.M.; Im, S. Decreased diaphragm excursion in stroke patients with dysphagia as assessed by M-mode sonography. Arch. Phys. Med. Rehabil. 2015, 96, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Voyvoda, N.; Yucel, C.; Karatas, G.; Oguzulgen, I.; Oktar, S. An evaluation of diaphragmatic movements in hemiplegic patients. Br. J. Radiol. 2012, 85, 411–414. [Google Scholar] [CrossRef] [Green Version]
- Khedr, E.M.; Trakhan, M.N. Localization of diaphragm motor cortical representation and determination of corticodiaphragmatic latencies by using magnetic stimulation in normal adult human subjects. Eur. J. Appl. Physiol. 2001, 85, 560–566. [Google Scholar] [CrossRef]
- Khedr, E.M.; El Shinawy, O.; Khedr, T.; Aziz Ali, Y.A.; Awad, E.M. Assessment of corticodiaphragmatic pathway and pulmonary function in acute ischemic stroke patients. Eur. J. Neurol. 2000, 7, 323–330. [Google Scholar] [CrossRef] [Green Version]
- Similowski, T.; Catala, M.; Rancurel, G.; Derenne, J.P. Impairment of central motor conduction to the diaphragm in stroke. Am. J. Respir. Crit. Care Med. 1996, 154, 436–441. [Google Scholar] [CrossRef]
- Kasé, Y.; Kito, G.; Miyata, T.; Takahama, K. Influence of cerebral cortex stimulation upon cough-like spasmodic expiratory response (SER) and cough in the cat. Brain Res. 1984, 306, 293–298. [Google Scholar] [CrossRef]
- Fong, J.; Sandhu, G.; Ellaway, P.; Davey, N.; Strutton, P.; Murphy, K.; Guz, A. What do we know about how humans cough? Pulm. Pharmacol. Ther. 2004, 17, 431–434. [Google Scholar] [CrossRef]
- Daniels, S.K.; Foundas, A.L. Lesion localization in acute stroke patients with risk of aspiration. J. Neuroimaging 1999, 9, 91–98. [Google Scholar] [CrossRef]
- Wu, M.N.; Chen, P.N.; Lai, C.L.; Liou, L.M. Contralateral diaphragmatic palsy after subcortical middle cerebral artery infarction without capsular involvement. Neurol. Sci. 2011, 32, 487–490. [Google Scholar] [CrossRef] [PubMed]
- Urban, P.P.; Morgenstern, M.; Brause, K.; Wicht, S.; Vukurevic, G.; Kessler, S.; Stoeter, P. Distribution and course of cortico-respiratory projections for voluntary activation in man. A transcranial magnetic stimulation study in healthy subjects and patients with cerebral ischemia. J. Neurol. 2002, 249, 735–744. [Google Scholar] [CrossRef] [PubMed]
- Simonyan, K.; Saad, Z.S.; Loucks, T.M.; Poletto, C.J.; Ludlow, C.L. Functional neuroanatomy of human voluntary cough and sniff production. Neuroimage 2007, 37, 401–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martino, R.; Foley, N.; Bhogal, S.; Diamant, N.; Speechley, M.; Teasell, R. Dysphagia after stroke: Incidence, diagnosis, and pulmonary complications. Stroke 2005, 36, 2756–2763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guillen-Sola, A.; Messagi Sartor, M.; Bofill Soler, N.; Duarte, E.; Barrera, M.C.; Marco, E. Respiratory muscle strength training and neuromuscular electrical stimulation in subacute dysphagic stroke patients: A randomized controlled trial. Clin. Rehabil. 2017, 31, 761–771. [Google Scholar] [CrossRef]
- Bates, E.; Wilson, S.M.; Saygin, A.P.; Dick, F.; Sereno, M.I.; Knight, R.T.; Dronkers, N.F. Voxel-based lesion-symptom mapping. Nat. Neurosci. 2003, 6, 448–450. [Google Scholar] [CrossRef]
- Lee, K.B.; Kim, J.S.; Hong, B.Y.; Sul, B.; Song, S.; Sung, W.J.; Hwang, B.Y.; Lim, S.H. Brain lesions affecting gait recovery in stroke patients. Brain Behav. 2017, 7, e00868. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.B.; Hong, B.Y.; Kim, J.S.; Sul, B.; Yoon, S.C.; Ji, E.K.; Son, D.B.; Hwang, B.Y.; Lim, S.H. Which brain lesions produce spasticity? An observational study on 45 stroke patients. PLoS ONE 2019, 14, e0210038. [Google Scholar] [CrossRef]
- Suntrup-Krueger, S.; Kemmling, A.; Warnecke, T.; Hamacher, C.; Oelenberg, S.; Niederstadt, T.; Heindel, W.; Wiendl, H.; Dziewas, R. The impact of lesion location on dysphagia incidence, pattern and complications in acute stroke. Part 2: Oropharyngeal residue, swallow and cough response, and pneumonia. Eur. J. Neurol. 2017, 24, 867–874. [Google Scholar] [CrossRef]
- Stephens, R.E.; Addington, W.R.; Widdicombe, J.G. Effect of acute unilateral middle cerebral artery infarcts on voluntary cough and the laryngeal cough reflex. Am. J. Phys. Med. Rehabil. 2003, 82, 379–383. [Google Scholar] [CrossRef]
- Galovic, M.; Leisi, N.; Pastore-Wapp, M.; Zbinden, M.; Vos, S.B.; Mueller, M.; Weber, J.; Brugger, F.; Kagi, G.; Weder, B.J. Diverging lesion and connectivity patterns influence early and late swallowing recovery after hemispheric stroke. Hum. Brain Mapp. 2017, 38, 2165–2176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, A.B.; Widdicombe, J.G. Cough throughout life: Children, adults and the senile. Pulm. Pharmacol. Ther. 2007, 20, 371–382. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.P., Jr.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E., 3rd. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The Barthel Index. MD State Med. J. 1965, 14, 61–65. [Google Scholar] [PubMed]
- Rorden, C.; Karnath, H.O.; Bonilha, L. Improving lesion-symptom mapping. J. Cogn. Neurosci. 2007, 19, 1081–1088. [Google Scholar] [CrossRef]
- Lancaster, J.L.; Woldorff, M.G.; Parsons, L.M.; Liotti, M.; Freitas, C.S.; Rainey, L.; Kochunov, P.V.; Nickerson, D.; Mikiten, S.A.; Fox, P.T. Automated Talairach atlas labels for functional brain mapping. Hum. Brain Mapp. 2000, 10, 120–131. [Google Scholar] [CrossRef]
- American Thoracic Society/European Respiratory Society. ATS/ERS Statement on respiratory muscle testing. Am. J. Respir. Crit. Care Med. 2002, 166, 518–624. [Google Scholar] [CrossRef]
- Sohn, D.; Park, G.Y.; Koo, H.; Jang, Y.; Han, Y.; Im, S. Determining peak cough flow cutoff values to predict aspiration pneumonia among patients with dysphagia using the citric acid reflexive cough test. Arch. Phys. Med. Rehabil. 2018, 99, 2532–2539. [Google Scholar] [CrossRef]
- Minnerup, J.; Wersching, H.; Brokinkel, B.; Dziewas, R.; Heuschmann, P.U.; Nabavi, D.G.; Ringelstein, E.B.; Schabitz, W.R.; Ritter, M.A. The impact of lesion location and lesion size on poststroke infection frequency. J. Neurol. Neurosurg. Psychiatry 2010, 81, 198–202. [Google Scholar] [CrossRef] [Green Version]
- Warnecke, T.; Im, S.; Kaiser, C.; Hamacher, C.; Oelenberg, S.; Dziewas, R. Aspiration and dysphagia screening in acute stroke—The Gugging Swallowing Screen revisited. Eur. J. Neurol. 2017, 24, 594–601. [Google Scholar] [CrossRef]
- Trapl, M.; Enderle, P.; Nowotny, M.; Teuschl, Y.; Matz, K.; Dachenhausen, A.; Brainin, M. Dysphagia bedside screening for acute-stroke patients: The Gugging Swallowing Screen. Stroke 2007, 38, 2948–2952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzalez-Fernandez, M.; Sein, M.T.; Palmer, J.B. Clinical experience using the Mann assessment of swallowing ability for identification of patients at risk for aspiration in a mixed-disease population. Am. J. Speech Lang. Pathol. 2011, 20, 331–336. [Google Scholar] [CrossRef]
- Crary, M.A.; Mann, G.D.; Groher, M.E. Initial psychometric assessment of a functional oral intake scale for dysphagia in stroke patients. Arch. Phys. Med. Rehabil. 2005, 86, 1516–1520. [Google Scholar] [CrossRef] [PubMed]
- Rosenbek, J.C.; Robbins, J.A.; Roecker, E.B.; Coyle, J.L.; Wood, J.L. A penetration-aspiration scale. Dysphagia 1996, 11, 93–98. [Google Scholar] [CrossRef]
- Logemann, J.A. Manual for the Videofluorographic Study of Swallowing, 2nd ed.; Pro Ed: Austin, TX, USA, 1993. [Google Scholar]
- Borders, J.C.; Brates, D. Use of the Penetration-Aspiration Scale in Dysphagia Research: A Systematic Review. Dysphagia 2020, 35, 583–597. [Google Scholar] [CrossRef]
- Mann, G. MASA: The Mann Assessment of Swallowing Ability; Singular Clifton Park: Clifton Park, NY, USA, 2002. [Google Scholar]
- Widdicombe, J.G.; Addington, W.R. Cough in patients after stroke. Eur. Respir. J. 2011, 37, 218. [Google Scholar] [CrossRef]
- Magni, C.; Chellini, E.; Lavorini, F.; Fontana, G.A.; Widdicombe, J. Voluntary and reflex cough: Similarities and differences. Pulm. Pharmacol. Ther. 2011, 24, 308–311. [Google Scholar] [CrossRef] [Green Version]
- Murphy, K.; Mier, A.; Adams, L.; Guz, A. Putative cerebral cortical involvement in the ventilatory response to inhaled CO2 in conscious man. J. Physiol. 1990, 420, 1–18. [Google Scholar] [CrossRef]
- Sapsford, R.R.; Hodges, P.W.; Richardson, C.A.; Cooper, D.H.; Markwell, S.J.; Jull, G.A. Co-activation of the abdominal and pelvic floor muscles during voluntary exercises. Neurourol. Urodyn. 2001, 20, 31–42. [Google Scholar] [CrossRef]
- Petrides, M.; Pandya, D.N. Projections to the frontal cortex from the posterior parietal region in the rhesus monkey. J. Comp. Neurol. 1984, 228, 105–116. [Google Scholar] [CrossRef]
- Corbetta, M.; Shulman, G.L. Control of goal-directed and stimulus-driven attention in the brain. Nat. Rev. Neurosci. 2002, 3, 201–215. [Google Scholar] [CrossRef] [PubMed]
- Pitts, T.; Morris, K.; Lindsey, B.; Davenport, P.; Poliacek, I.; Bolser, D. Co-ordination of cough and swallow in vivo and in silico. Exp. Physiol. 2012, 97, 469–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimura, Y.; Takahashi, M.; Wada, F.; Hachisuka, K. Differences in the peak cough flow among stroke patients with and without dysphagia. J. UOEH 2013, 35, 9–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kulnik, S.T.; Birring, S.S.; Hodsoll, J.; Moxham, J.; Rafferty, G.F.; Kalra, L. Higher cough flow is associated with lower risk of pneumonia in acute stroke. Thorax 2016, 71, 474–475. [Google Scholar] [CrossRef] [Green Version]
- Laciuga, H.; Brandimore, A.E.; Troche, M.S.; Hegland, K.W. Analysis of Clinicians’ Perceptual Cough Evaluation. Dysphagia 2016, 31, 521–530. [Google Scholar] [CrossRef]
- Miles, A.; Huckabee, M.L. Intra- and inter-rater reliability for judgement of cough following citric acid inhalation. Int. J. Speech Lang. Pathol. 2013, 15, 209–215. [Google Scholar] [CrossRef]
- Vilardell, N.; Rofes, L.; Nascimento, W.V.; Muriana, D.; Palomeras, E.; Clave, P. Cough reflex attenuation and swallowing dysfunction in sub-acute post-stroke patients: Prevalence, risk factors, and clinical outcome. Neurogastroenterol. Motil. 2017, 29, e12910. [Google Scholar] [CrossRef]
- Colebatch, J.G.; Adams, L.; Murphy, K.; Martin, A.J.; Lammertsma, A.A.; Tochon-Danguy, H.J.; Clark, J.C.; Friston, K.J.; Guz, A. Regional cerebral blood flow during volitional breathing in man. J. Physiol. 1991, 443, 91–103. [Google Scholar] [CrossRef]
- Ward, K.; Seymour, J.; Steier, J.; Jolley, C.J.; Polkey, M.I.; Kalra, L.; Moxham, J. Acute ischaemic hemispheric stroke is associated with impairment of reflex in addition to voluntary cough. Eur. Respir. J. 2010, 36, 1383–1390. [Google Scholar] [CrossRef]
- Bahat, G.; Tufan, A.; Ozkaya, H.; Tufan, F.; Akpinar, T.S.; Akin, S.; Bahat, Z.; Kaya, Z.; Kiyan, E.; Erten, N.; et al. Relation between hand grip strength, respiratory muscle strength and spirometric measures in male nursing home residents. Aging Male 2014, 17, 136–140. [Google Scholar] [CrossRef]
- Harraf, F.; Ward, K.; Man, W.; Rafferty, G.; Mills, K.; Polkey, M.; Moxham, J.; Kalra, L. Transcranial magnetic stimulation study of expiratory muscle weakness in acute ischemic stroke. Neurology 2008, 71, 2000–2007. [Google Scholar] [CrossRef] [PubMed]
- Messaggi-Sartor, M.; Guillen-Sola, A.; Depolo, M.; Duarte, E.; Rodriguez, D.A.; Barrera, M.C.; Barreiro, E.; Escalada, F.; Orozco-Levi, M.; Marco, E. Inspiratory and expiratory muscle training in subacute stroke: A randomized clinical trial. Neurology 2015, 85, 564–572. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total (n = 39) | Cough <80 L/min (n = 19) | Cough ≥80 L/min (n = 20) | p-Value |
|---|---|---|---|---|
| Basic demographics | ||||
| Age | 72.6 ± 12.5 | 76.6 ± 10.3 | 68.8 ± 13.5 | 0.0051 |
| Gender | 0.584 | |||
| Male | 25 (64.1) | 13 (68.4) | 12 (60.0) | |
| Female | 14 (35.9) | 6 (31.6) | 8 (40.0) | |
| Body mass index (kg/m2) | 22.9 ± 2.9 | 23.4 ± 2.6 | 22.4 ± 3.1 | 0.300 |
| Brain lesion classification | ||||
| Total lesion volume (voxels) | 55,985.1 ± 91,883.6 | 60,558.8 ± 92,950.9 | 51,640 ± 93,055.1 | 0.989 |
| Laterality | 0.648 | |||
| Right | 24 (61.5) | 11 (57.9) | 13 (65.0) | |
| Left | 15 (38.5) | 8 (42.1) | 7 (35.0) | |
| TOAST | 0.465 | |||
| Large artery atherosclerosis | 18 (46.1) | 8 (42.1) | 10 (50.0) | |
| Cardio embolism | 9 (23.1) | 6 (31.6) | 3 (15.0) | |
| Small-vessel occlusion | 12 (30.8) | 5 (26.3) | 7 (35.0) | |
| Medical comorbidities | ||||
| Diabetes mellitus | 12 (30.8) | 7 (36.8) | 5 (25.0) | 0.650 |
| Hypertension | 24 (61.5) | 15 (78.9) | 9 (45.0) | 0.064 |
| Atrial fibrillation | 9 (23.1) | 6 (31.6) | 3 (15.0) | 0.396 |
| Hyperlipidemia | 1 (2.6) | 0 (0.0) | 1 (5.0) | 1.000 |
| Neurological function | ||||
| NIHSS | 6.4 ± 4.2 | 7.6 ± 4.2 | 5.3 ± 3.9 | 0.095 |
| MBI | 38.7 ± 27.7 | 26.5 ± 25.5 | 50.3 ± 25.0 1 | 0.006 |
| MMSE | 19.6 ± 6.4 | 17.3 ± 6.6 | 21.8 ± 5.4 1 | 0.0024 |
| Berg | 17.7 ± 20.6 | 9.7 ± 14.7 | 25.2 ± 22.8 1 | 0.017 |
| Respiratory pressure measurements | ||||
| Peak cough flow (L/min) | 98.4 ± 58.4 | 53.0 ± 20.6 | 141.5 ± 48.9 1 | <0.001 |
| MIP (cmH2O) | 26.6 ± 25.4 | 14.5 ± 8.8 | 38.2 ± 30.5 1 | 0.003 |
| MEP (cmH2O) | 40.2 ± 32.4 | 23.2 ± 16.6 | 56.4 ± 35.7 1 | 0.001 |
| Swallowing parameters | ||||
| FOIS | 2 (1–4) | 1 (1–2) | 4 (2–4) 1 | 0.007 |
| MASA | 155.1 ± 17.1 | 142.9 ± 14.9 | 166.7 ± 9.3 1 | <0.001 |
| GUSS | 7.6 ± 4.3 | 4.7 ± 2.6 | 10.3 ± 3.7 1 | <0.001 |
| PAS | 8 (7–8) | 8 (7.5–8) | 7 (5–8) | 0.137 |
| MNI Coordinates (X, Y, Z) | BM Z max | n Voxels | Anatomical Brain Lesion |
|---|---|---|---|
| 34, −38, 35 | 2.90267 | 114 | Parietal lobe, Sub-Gyral |
| 29, −26, 32 | 3.38958 | 111 | Frontal lobe, Superior longitudinal |
| 29, 13, 28 | 2.85527 | 116 | Frontal lobe, Sub-Gyral |
| 29, −27, 30 | 3.17468 | 114 | Posterior corona radiata |
| 38, −35, 15 | 2.65207 | 106 | Temporal lobe, STG |
| 42, −41, −7 | 2.55235 | 115 | Temporal lobe, MTG |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.B.; Lim, S.H.; Park, G.-Y.; Im, S. Effect of Brain Lesions on Voluntary Cough in Patients with Supratentorial Stroke: An Observational Study. Brain Sci. 2020, 10, 627. https://doi.org/10.3390/brainsci10090627
Lee KB, Lim SH, Park G-Y, Im S. Effect of Brain Lesions on Voluntary Cough in Patients with Supratentorial Stroke: An Observational Study. Brain Sciences. 2020; 10(9):627. https://doi.org/10.3390/brainsci10090627
Chicago/Turabian StyleLee, Kyoung Bo, Seong Hoon Lim, Geun-Young Park, and Sun Im. 2020. "Effect of Brain Lesions on Voluntary Cough in Patients with Supratentorial Stroke: An Observational Study" Brain Sciences 10, no. 9: 627. https://doi.org/10.3390/brainsci10090627