The Supplementary Motor Area Responsible for Word Retrieval Decline After Acute Thalamic Stroke Revealed by Coupled SPECT and Near-Infrared Spectroscopy


Abstract
:1. Introduction
2. Materials and Methods
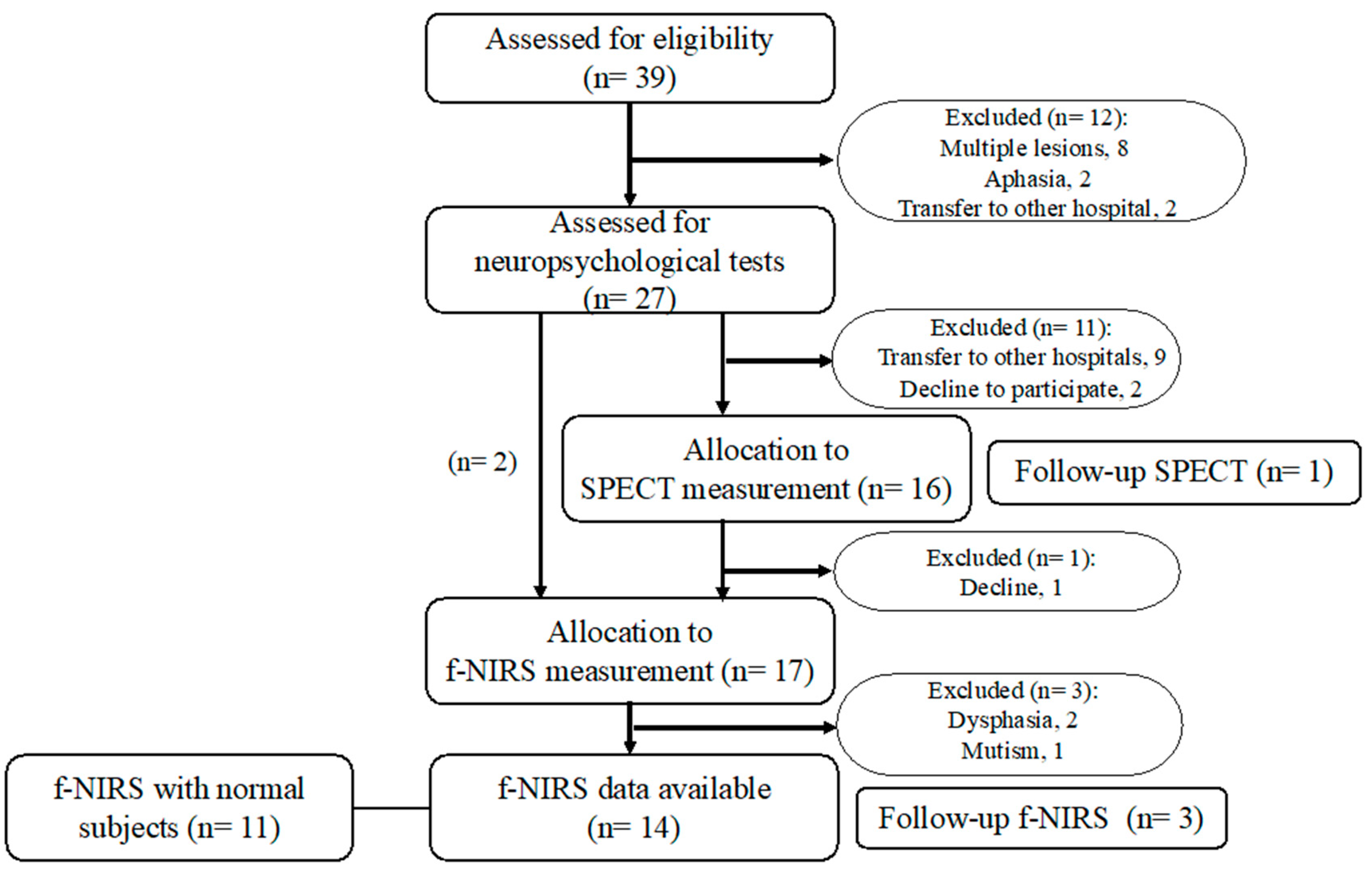
2.1. Participant Recruitment and Inclusion Criteria
2.2. Neuropsychological Estimation
2.3. NIRS Studies: Image Acquisition and Analysis
2.3.1. Image Acquisition
2.3.2. Definition of Regions of Interest
2.3.3. Task Procedure of f-NIRS Study
2.3.4. NIRS Data Acquisition and Analysis
2.4. SPECT Image Acquisition and Analysis
2.5. Statistical Analysis
3. Results
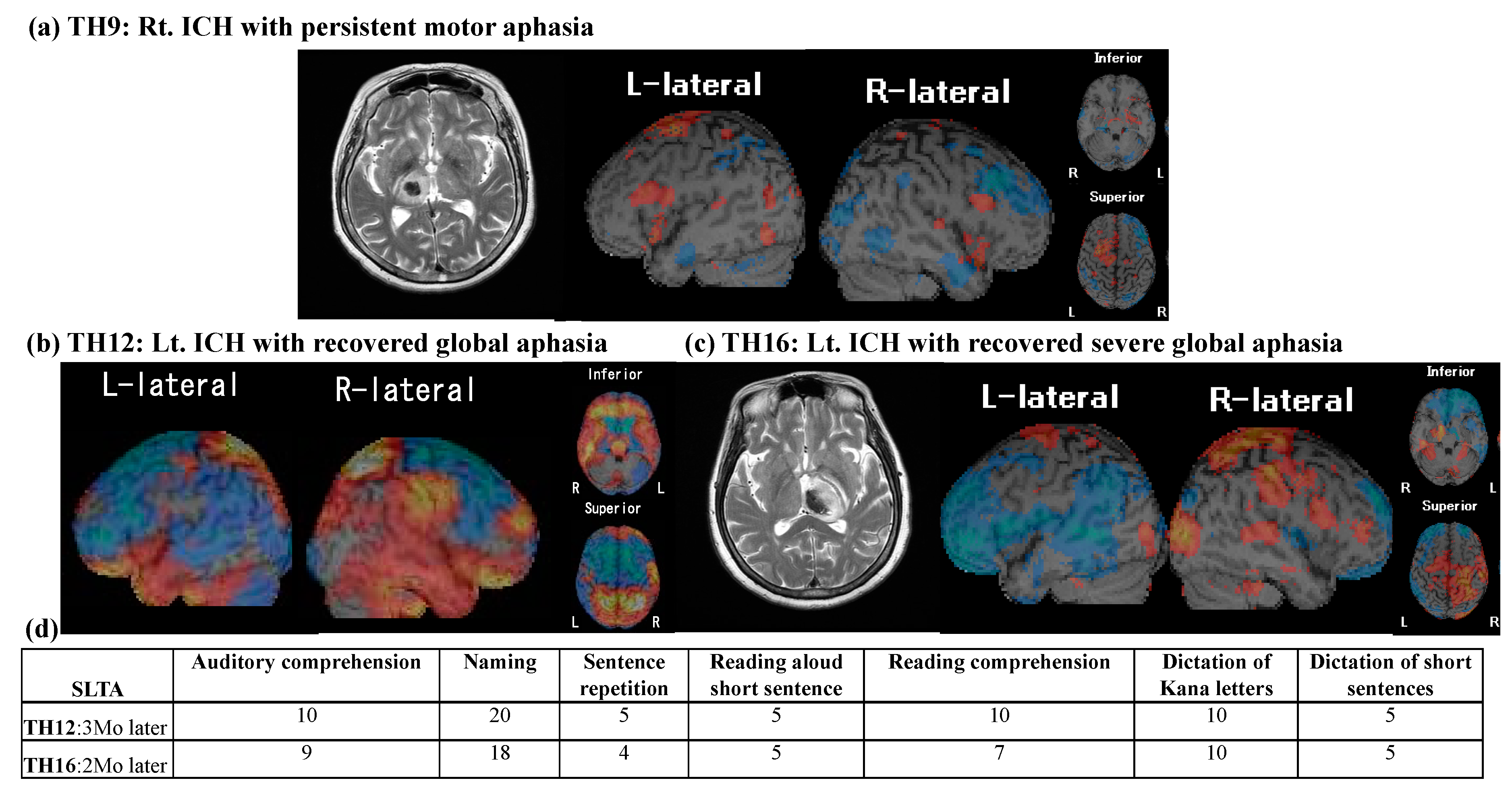
3.1. Neuropsychological Findings
3.2. SPECT Results
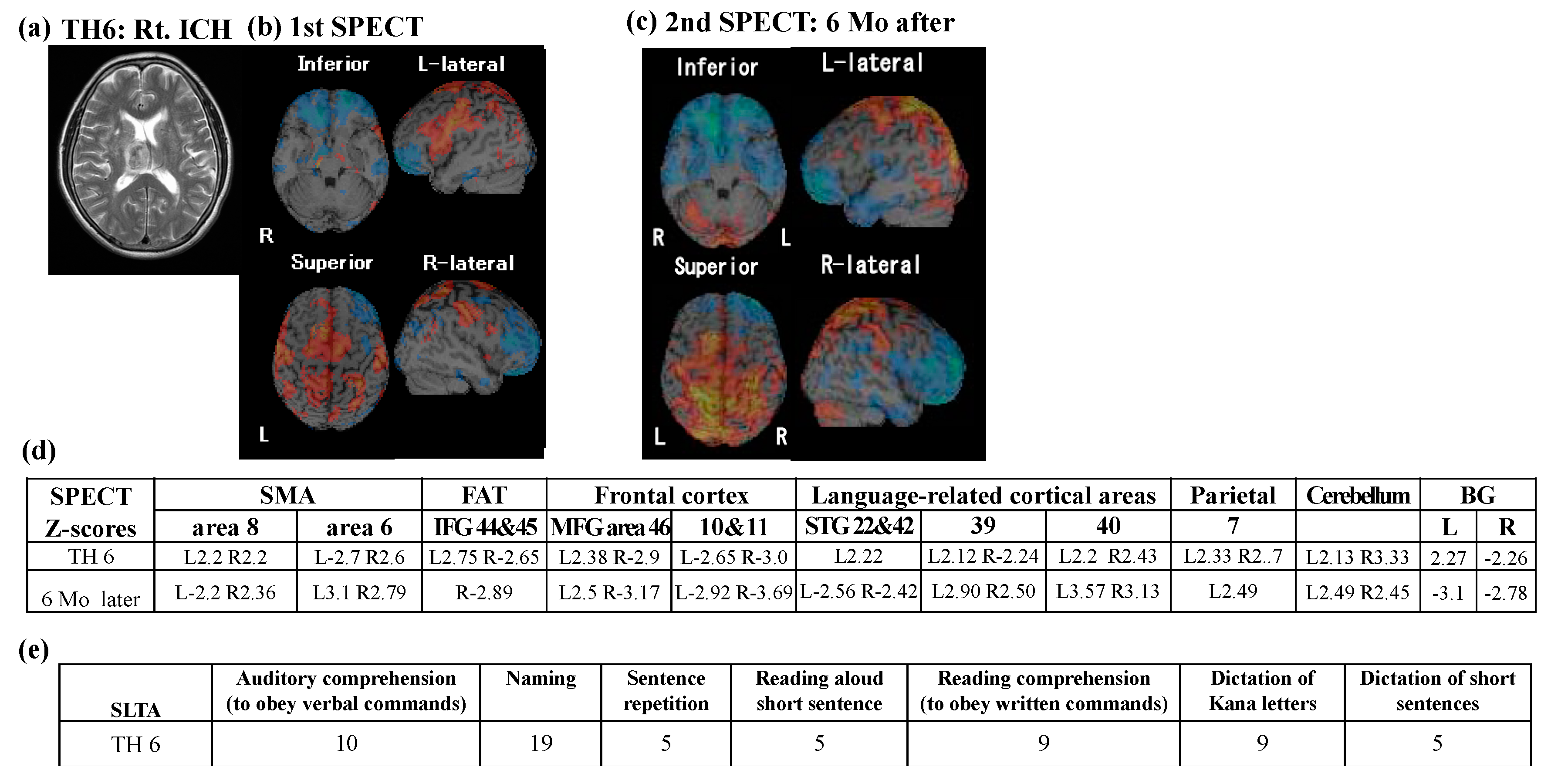
3.2.1. SPECT Z-Score Mapping
3.2.2. Follow-Up SPECT
3.3. NIRS Results
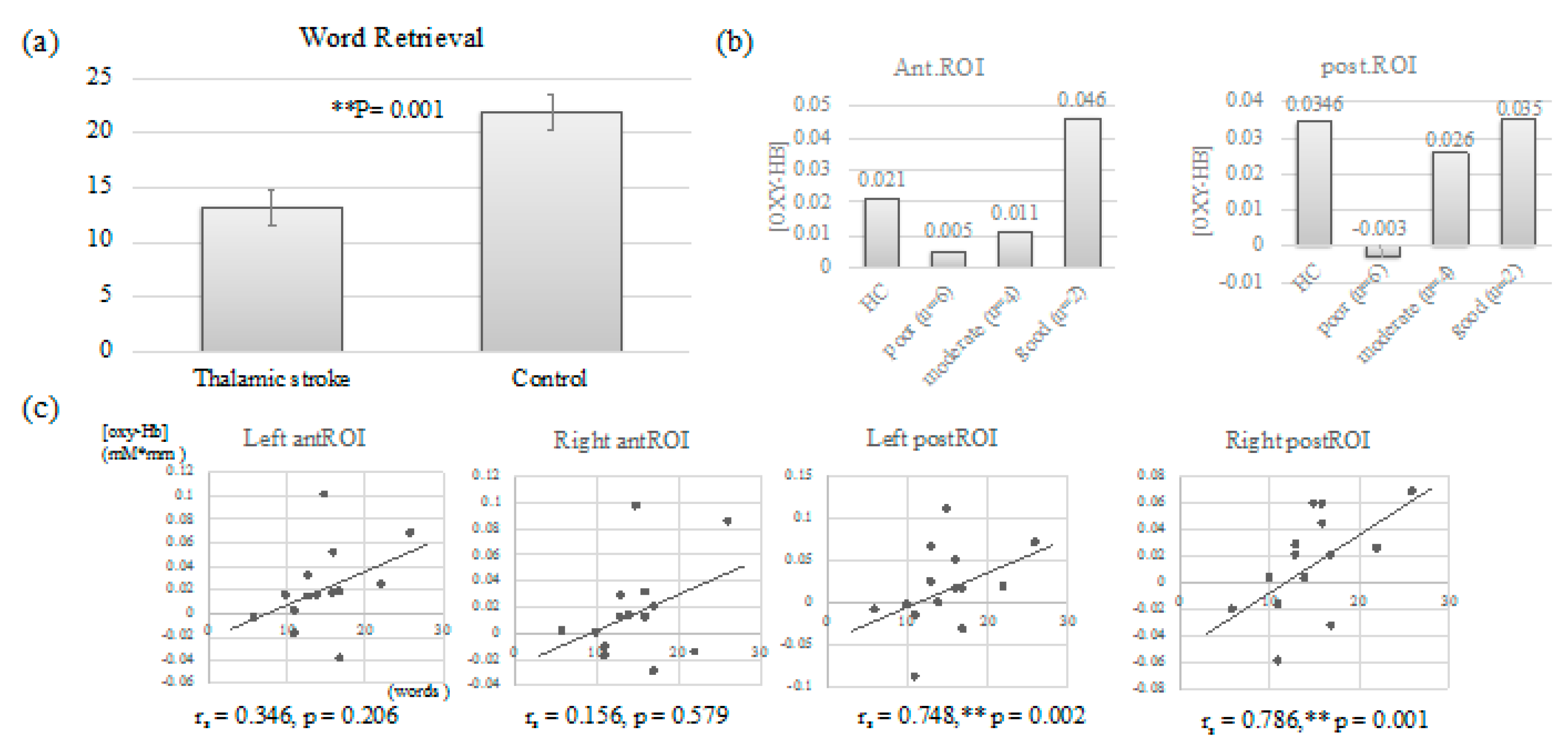
3.3.1. Word Retrieval: Comparison between Thalamic Stroke Survivors and Control
3.3.2. NIRS Results: The Comparison with the Control and the Correlation
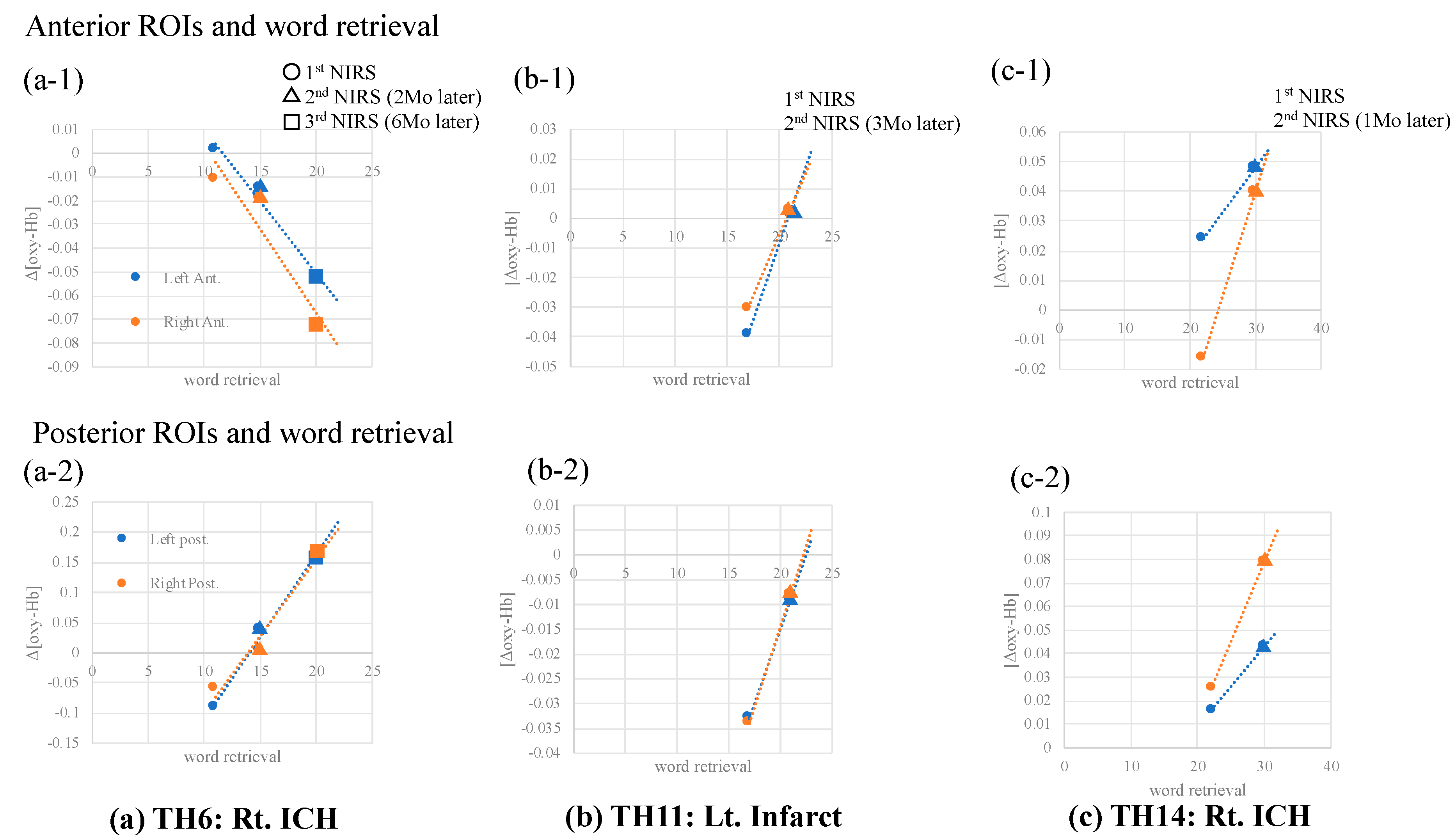
3.3.3. Follow-Up NIRS Tests
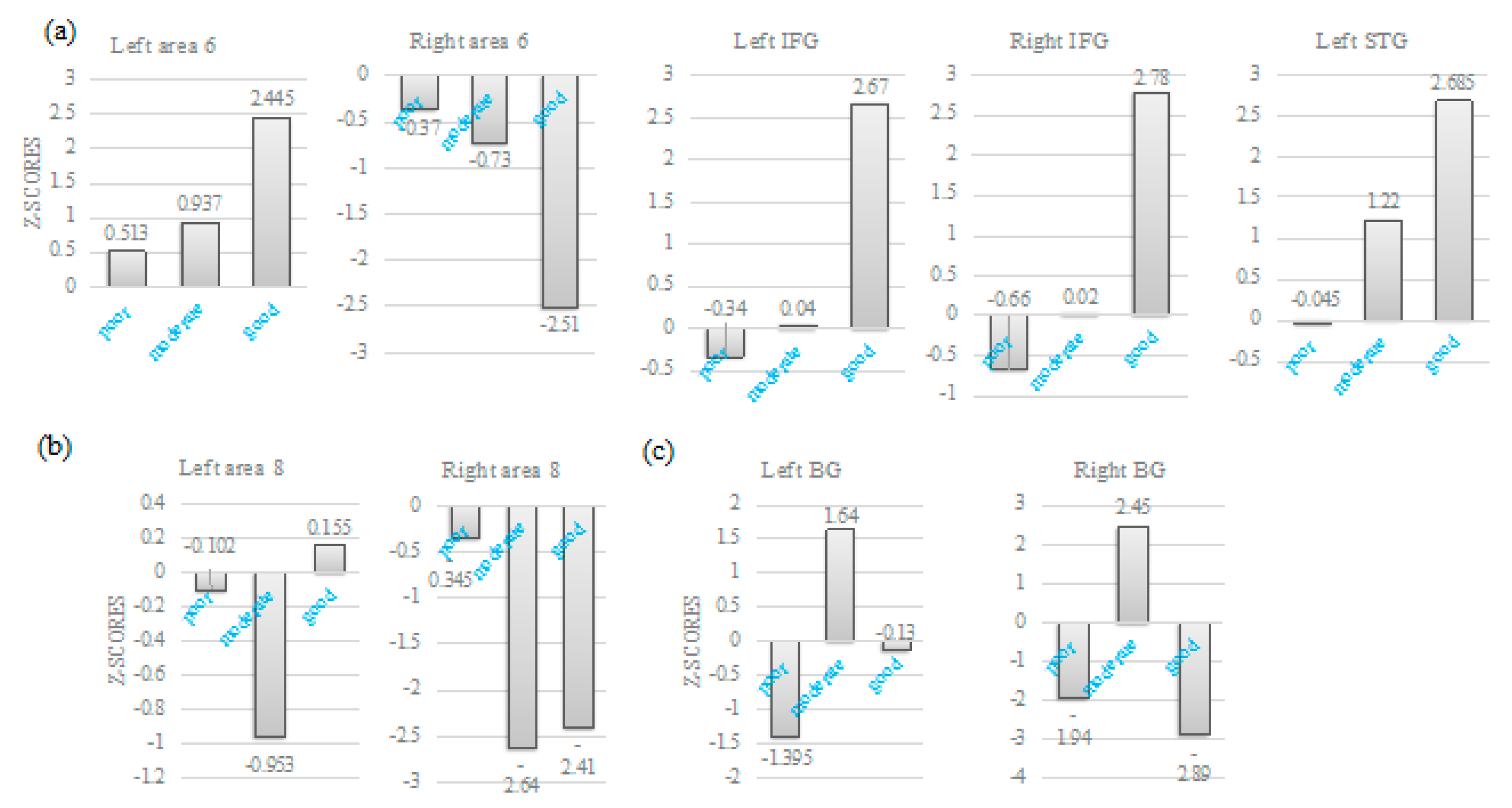
3.3.4. NIRS Data and SPECT Z-Scores
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wolff, M.; Vann, S.D. The Cognitive Thalamus as a Gateway to Mental Representations. J. Neurosci. 2019, 39, 3–14. [Google Scholar] [CrossRef]
- Raymer, A.M.; Moberg, P.; Crosson, B.; Nadeau, S.; Rothi, L.J. Lexical-semantic deficits in two patients with dominant thalamic infarction. Neuropsychologia 1997, 35, 211–219. [Google Scholar] [CrossRef]
- Fontaine, D.; Capelle, L.; Duffau, H. Somatotopy of the supplementary motor area: Evidence from correlation of the extent of surgical resection with the clinical patterns of deficit. Neurosurgery 2002, 50, 297–303. [Google Scholar]
- Tremblay, P.; Gracco, V.L. Contribution of the pre-SMA to the production of words and non-speech oral motor gestures, as revealed by repetitive transcranial magnetic stimulation (rTMS). Brain Res. 2009, 1268, 112–124. [Google Scholar] [CrossRef]
- Alario, F.X.; Chainay, H.; Lehericy, S.; Cohen, L. The role of the supplementary motor area (SMA) in word production. Brain Res. 2006, 1076, 129–143. [Google Scholar] [CrossRef]
- Shima, K.; Mushiake, H.; Saito, N.; Tanji, J. Role for cells in the presupplementary motor area in updating motor plans. Proc. Natl. Acad. Sci. USA 1996, 93, 8694–8698. [Google Scholar] [CrossRef] [Green Version]
- Catani, M.; Dell’acqua, F.; Vergani, F.; Malik, F.; Hodge, H.; Roy, P.; Valabregue, R.; Thiebaut de Schotten, M. Short frontal lobe connections of the human brain. Cortex 2012, 48, 273–291. [Google Scholar] [CrossRef]
- Thiebaut de Schotten, M.; Dell’Acqua, F.; Valabregue, R.; Catani, M. Monkey to human comparative anatomy of the frontal lobe association tracts. Cortex 2012, 48, 82–96. [Google Scholar] [CrossRef]
- Laplane, D.; Talairach, J.; Meininger, V.; Bancaud, J.; Orgogozo, J.M. Clinical consequences of corticectomies involving the supplementary motor area in man. J. Neurol. Sci. 1977, 34, 301–314. [Google Scholar] [CrossRef]
- Potgieser, A.R.; de Jong, B.M.; Wagemakers, M.; Hoving, E.W.; Groen, R.J. Insights from the supplementary motor area syndrome in balancing movement initiation and inhibition. Front. Hum. Neurosci. 2014, 8, 960. [Google Scholar] [CrossRef] [Green Version]
- Saur, D.; Lange, R.; Baumgaertner, A.; Schraknepper, V.; Willmes, K.; Rijntjes, M.; Weiller, C. Dynamics of language reorganization after stroke. Brain 2006, 129, 1371–1384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obayashi, S.; Hara, Y. Hypofrontal activity during word retrieval in older adults: A near-infrared spectroscopy study. Neuropsychologia 2013, 51, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Carrera, E.; Tononi, G. Diaschisis: Past, present, future. Brain 2014, 137, 2408–2422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Aes, T.; Marien, P. Cognitive and affective disturbances following focal brainstem lesions: A review and report of three cases. Cerebellum 2015, 14, 317–340. [Google Scholar] [CrossRef] [PubMed]
- Garrard, P.; Bradshaw, D.; Jäger, H.R.; Thompson, A.J.; Losseff, N.; Playford, D. Cognitive dysfunction after isolated brain stem insult. An underdiagnosed cause of long term morbidity. J. Neurol. Neurosurg. Psychiat. 2002, 73, 191–194. [Google Scholar] [CrossRef] [PubMed]
- Fazekas, F.; Payer, F.; Valetitsch, H.; Schmidt, R.; Flooh, E. Brain stem infarction and diaschisis. A SPECT cerebral perfusion study. Stroke 1993, 24, 1162–1166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obayashi, S. Frontal dynamic activity as a predictor of cognitive dysfunction after pontine ischemia. NeuroRehabilitation 2019, 44, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Toyokura, M.; Tanaka, H.; Furukawa, T.; Yamanouchi, Y.; Murakami, K. Normal aging effect on cognitive task performance of information-processing speed: Analysis of paced auditory serial addition task and trail making test. Brain Sci. Ment. Disord. 1996, 7, 401–409. [Google Scholar]
- Obrig, H.; Villringer, A. Beyond the visible—Imaging the human brain with light. J. Cereb. Blood Flow Metab. 2003, 23, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Okamoto, M.; Dan, H.; Sakamoto, K.; Takeo, K.; Shimizu, K.; Kohno, S.; Oda, I.; Isobe, S.; Suzuki, T.; Kohyama, K.; et al. Three-dimensional probabilistic anatomical cranio-cerebral correlation via the international 10–20 system oriented for transcranial functional brain mapping. Neuroimage 2004, 21, 99–111. [Google Scholar] [CrossRef] [PubMed]
- Yokoi, T.; Soma, T.; Shinohara, H.; Matsuda, H. Accuracy and reproducibility of co-registration techniques based on mutual information and normalized mutual information for MRI and SPECT brain images. Ann. Nucl. Med. 2004, 18, 659–667. [Google Scholar] [CrossRef] [PubMed]
- Mizumura, S.; Kumita, S.; Cho, K.; Ishihara, M.; Nakajo, H.; Toba, M.; Kumazaki, T. Development of quantitative analysis method for stereotactic brain image: Assessment of reduced accumulation in extent and severity using anatomical segmentation. Ann. Nucl. Med. 2003, 17, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Costafreda, S.G.; Fu, C.H.; Lee, L.; Everitt, B.; Brammer, M.J.; David, A.S. A systematic review and quantitative appraisal of fMRI studies of verbal fluency: Role of the left inferior frontal gyrus. Hum. Brain Mapp. 2006, 27, 799–810. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, W.; Kilian, B.; Deger, K. The role of the left mesial frontal cortex in fluent speech: Evidence from a case of left supplementary motor area hemorrhage. Neuropsychologia 1997, 35, 1197–1208. [Google Scholar] [CrossRef]
- Dick, A.S.; Garic, D.; Graziano, P.; Tremblay, P. The frontal aslant tract (FAT) and its role in speech, language and executive function. Cortex 2019, 111, 148–163. [Google Scholar] [CrossRef]
- Demeurisse, G.; Derouck, M.; Coekaerts, M.J.; Deltenre, P.; Van Nechel, C.; Demol, O.; Capon, A. Study of two cases of aphasia by infarction of the left thalamus, without cortical lesion. Acta Neurol. Belg. 1979, 79, 450–459. [Google Scholar]
- Jonas, S. The thalamus and aphasia, including transcortical aphasia: A review. J. Comm. Disord. 1982, 15, 31–41. [Google Scholar] [CrossRef]
- Llano, D.A. Functional imaging of the thalamus in language. Brain Lang. 2013, 126, 62–72. [Google Scholar] [CrossRef] [Green Version]
- Bell, D.S. Speech functions of the thalamus inferred from the effects of thalamotomy. Brain 1968, 91, 619–638. [Google Scholar] [CrossRef]
- Karussis, D.; Leker, R.R.; Abramsky, O. Cognitive dysfunction following thalamic stroke: A study of 16 cases and review of the literature. J. Neurol. Sci. 2000, 172, 25–29. [Google Scholar] [CrossRef]
- Anglade, C.; Thiel, A.; Ansaldo, A.I. The complementary role of the cerebral hemispheres in recovery from aphasia after stroke: A critical review of literature. Brain Inj. 2014, 28, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Sebastian, R.; Long, C.; Purcell, J.J.; Faria, A.V.; Lindquist, M.; Jarso, S.; Race, D.; Davis, C.; Posner, J.; Wright, A.; et al. Imaging network level language recovery after left PCA stroke. Restor. Neurol. Neurosci. 2016, 34, 473–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akkal, D.; Dum, R.P.; Strick, P.L. Supplementary motor area and presupplementary motor area: Targets of basal ganglia and cerebellar output. J. Neurosci. 2007, 27, 10659–10673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Boissezon, X.; Marie, N.; Castel-Lacanal, E.; Marque, P.; Bezy, C.; Gros, H.; Lotterie, J.A.; Cardebat, D.; Puel, M.; Demonet, J.F. Good recovery from aphasia is also supported by right basal ganglia: A longitudinal controlled pet study. Ejprm-esprm 2008 award winner. Eur. J. Phys. Rehabi. Med. 2009, 45, 547–558. [Google Scholar]
- Naeser, M.A.; Palumbo, C.L.; Helm-Estabrooks, N.; Stiassny-Eder, D.; Albert, M.L. Severe nonfluency in aphasia. Role of the medial subcallosal fasciculus and other white matter pathways in recovery of spontaneous speech. Brain 1989, 112, 1–38. [Google Scholar] [CrossRef] [PubMed]
- Smielewski, P.; Czosnyka, M.; Pickard, J.D.; Kirkpatrick, P. Clinical evaluation of near-infrared spectroscopy for testing cerebrovascular reactivity in patients with carotid artery disease. Stroke 1997, 28, 331–338. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Thalamic Stroke Patients | Normal Control for f-NIRS | |
|---|---|---|
| n | 27 | 11 |
| Age, mean (SD) | 63.3 (6.17) | 63.3 (7.39) |
| Sex (Female) | 7 | 8 |
| Stroke type | ||
| Infarct | 12 | |
| Hemorrhage | 15 | |
| Laterality | Right 18 Left 7 Bilateral 1 | |
| Cognitive impairments | ||
| None | 2 | |
| One domain | 9 | |
| Two domains | 12 | |
| Three domains | 4 | |
| Details: | ||
| Inattention | 18 | |
| Memory disturbance | 15 | |
| Executive dysfunction | 11 | |
| Social behavioral disorders | 1 |
| Thalamic Patients | Auditory Comprehension (to Obey Verbal Commands) | Naming | Sentence Repetition | Reading Aloud Short Sentence | Reading Comprehension (to Obey Written Commands) | Dictation of Kana Letters | Dictation of Short Sentences |
|---|---|---|---|---|---|---|---|
| TH 1 | 10/10 | 20/20 | 5/5 | 5/5 | 10/10 | 10/10 | 5/5 |
| TH 2 | 10 | 20 | 5 | 5 | 10 | 10 | 5 |
| TH 3 | 10 | 20 | 5 | 5 | 10 | 10 | 5 |
| TH 4 | 10 | 20 | 5 | 5 | 10 | 10 | 5 |
| TH 5 | 10 | 20 | 5 | 5 | 10 | 10 | 5 |
| TH 6 | 10 | 19 | 5 | 5 | 9 | 9 | 5 |
| TH 7 | 10 | 20 | 5 | 5 | 9 | - | - |
| TH 8 | 10 | 20 | 5 | 5 | 10 | 10 | 5 |
| TH 9 | 10 | 17 | 4 | 4 | 5 | 10 | 2 |
| TH 10 | - | - | - | - | - | - | - |
| TH 11 | 10 | 19 | 5 | 5 | 10 | 10 | 4 |
| TH 12 | 6 | 15 | 5 | 5 | 6 | 10 | 5 |
| TH 13 | 9 | 20 | 5 | 5 | 10 | 10 | 5 |
| TH 14 | - | - | - | - | - | - | - |
| TH 15 | 10 | 20 | 4 | 5 | 10 | 10 | 5 |
| TH 16 | 0 | 6 | 3 | 4 | 0 | 8 | 0 |
| SPECT Z-Scores | SMA | FAT | Frontal Cortex | Language-Related Cortical Areas | Parietal | Cerebellum | BG | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Area 8 | Area 6 | IFG 44&45 | MFG 46 | 10&11 | STG 22&42 | 39 | 40 | 7 | L | R | ||
| TH 1 | L −2.66 | L −2.5 | L 2.6 | L 2.44 | L 2.55 | L 2.22 | L −2.16 | L −2.82 | L −2.56 | L 2.35 | 2.35 | 2.47 |
| R −2.36 | R −2.2 | R 2.94 | R 2.22 | R 2.17 | R 2.44 | R 2.06 | R −2.44 | R 2.33 | R 2.59 | |||
| TH 2 | L 2.46 | L 2.8 | L −2.5 | L 2.33 | L −2.29 | L −2.37 | L 2.94 | L 3.15 | L 2.57 | L −2.28 | −2.9 | −2.39 |
| R 2.63 | R 2.61 | R −2.62 | R −2.16 | R −2.55 | R 2.64 | R 2.1 | R −2.40 | R 2.48 | R 2.32 | |||
| TH 3 | L 2.36 | L 2.81 | L 3.72 | L 4.0 | L 2.35 | L 2.35 | L 2.3 | L 2.63 | L 2.99 | R −2.55 | 3.12 | 2.16 |
| R −2.27 | R 2.3 | R 2.35 | R2.2 | R 2.39 | R 2.18 | R 2.48 | R 2.72 | |||||
| TH 4 | L −2.2 | L 2.36 | L 2.06 | normal | L -2.2 | L 2.1 | L 2.47 | L 2.05 | L -2.33 | L 2.32 | −2.9 | −2.53 |
| R −2.3 | R −2.38 | R 2.23 | R 2.12 | R −2.5 | R 2.17 | R 2.57 | ||||||
| TH 5 | L −2.4 | L −2.44 | L 2.15 | L 2.66 | L −2.15 | L 2.64 | L 2.74 | L 2.47 | R 2.45 | L 2.29 | −2.7 | −2.41 |
| R −2.15 | R −2.34 | R 2.73 | R 2.73 | R −2.0 | R 2.23 | R −2.22 | R −2.67 | |||||
| TH 6 | L 2.2 | L 2.7 | L 2.78 | L 2.38 | L −2.65 | L 2.22 | L 2.12 | L 2.2 | L 2.33 | L 2.13 | 2.27 | −2.26 |
| R 2.2 | R 2.6 | R −2.66 | R −2.9 | R −3 | R −2.24 | R 2.43 | R 2.7 | R 3.33 | ||||
| TH 7 | R −2.36 | L 2.82 | L 3.1 | L 3.28 | L 2.52 | L 2.2 | L 2.5 | L −2.79 | L 2.34 | L 2.31 | 2.84 | 2.4 |
| R −2.45 | R 2.68 | R 2.34 | R 2.32 | R 2.41 | R −2.41 | R 2.97 | R -2.7 | R −2.35 | ||||
| TH 8 | L −2.22 | L 2.64 | L −3.4 | L −2.28 | L −2.89 | L 2.90 | L 4.39 | L 2.43 | L 3.05 | L −2.58 | 4.27 | 2.48 |
| R −2.11 | R 2.53 | R −2.54 | R −2.34 | R −2.37 | R 2.88 | R 3.14 | R 2.61 | R 3.22 | R −2.63 | |||
| TH 9 | L 2.18 | L 2.64 | L 2.42 | R −2.27 | R −2.28 | L 2.04 | L 2.33 | L −2.1 | L −2.36 | L −2.38 | −2.58 | |
| R 2.36 | R −2.42 | R 2.46 | R −2.55 | |||||||||
| TH 10 | L 2.21 | L 3.7 | L −5.0 | L −2.97 | L −2.87 | L −2.44 | L −2.36 | L −2.87 | L 2.93 | L −2.42 | −2.6 | −2.56 |
| R 2.32 | R 2.93 | R −3.5 | R −2.89 | R −2.38 | R −3.28 | R -2.39 | R −2.28 | R 2.91 | R −2.42 | |||
| TH 11 | L −3.0 | L −2.64 | L −2.76 | L −2.5 | L −2.64 | L −2.59 | L −2.41 | L −2.60 | L −2.34 | L 3.73 | −3.2 | 2.71 |
| R −3.18 | R −2.44 | R −2.62 | R 2.19 | R 2.2 | R 2.5 | R −2.58 | R 2.81 | R 2.52 | R 3.25 | |||
| TH 12 | L −5.22 | L −5.31 | L −4.87 | L −4.63 | L 5.47 | L −2.65 | L −2.66 | L −3.07 | L 4.38 | L −3.57 | −5.3 | −4.83 |
| R −4.91 | R −5.22 | R −3.44 | R −3.32 | R 6.41 | R 3.79 | R 2.56 | R 3.67 | R 5.17 | R 3.1 | |||
| TH 13 | L 2.51 | L 2.45 | L −4.23 | L −2.92 | L −2.2 | L −3.0 | R 2.48 | L −2.94 | L 2.47 | L 2.32 | −2.9 | −2.58 |
| R 2.53 | R 2.45 | R −2.48 | R −2.65 | R −2.21 | R −2.50 | R −2.25 | R 2.09 | R 2.77 | ||||
| TH 14 | L 2.51 | L 2.53 | L 3.28 | L 2.55 | L 2.80 | L 3.27 | L 3.63 | L 2.81 | L 2.81 | L 3.01 | 2.59 | −3.25 |
| R −2.52 | R −2.65 | R 2.78 | R 2.78 | R 2.36 | R −3.14 | R −2.68 | R -2.59 | R −2.47 | R 2.79 | |||
| TH 15 | L −2.12 | L 2.51 | L −2.71 | L −2.36 | L −2.3 | L −2.31 | L 2.26 | L 2.8 | L 2.38 | L 2.36 | −2.6 | −2.15 |
| R 2.51 | R 2.58 | R 2.19 | R −2.42 | R 2.74 | R 2.0 | R 2.38 | R 2.24 | R 2.83 | ||||
| TH 16 | L −2.26 | L 2.36 | L −3.25 | L −2.4 | L −2.99 | L −2.97 | L −2.38 | L −2.59 | L −2.35 | L 2.48 | −2.4 | 2.68 |
| R 2.33 | R 2.35 | R 2.38 | R 2.36 | R −3.12 | R 2.56 | R −2.56 | R 2.53 | R 2.82 | R 2.41 | |||
| Patients | Word Retrieval during NIRS | HC | Word Retrieval |
|---|---|---|---|
| TH 1 | 16 | HC 1 | 22 |
| TH 2 | 6 | HC 2 | 25 |
| TH 3 | 17 | HC 3 | 27 |
| TH 4 | 26 | HC 4 | 18 |
| TH 5 | 11 | HC 5 | 29 |
| TH 6 | 11 | HC 6 | 29 |
| TH 7 | 13 | HC 7 | 13 |
| TH 8 | 16 | HC 8 | 23 |
| TH 9 | 3 | HC 9 | 19 |
| TH 10 | 1 | HC 10 | 15 |
| TH 11 | 17 | HC 11 | 21 |
| TH 12 | 13 | average | 21.91 |
| TH 13 | declined | SD | 5.375 |
| TH 14 | 22 | ||
| TH 15 | 10 | ||
| TH 16 | 0 | ||
| average | 13.18 | ||
| SD | 6.4 |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Obayashi, S. The Supplementary Motor Area Responsible for Word Retrieval Decline After Acute Thalamic Stroke Revealed by Coupled SPECT and Near-Infrared Spectroscopy. Brain Sci. 2020, 10, 247. https://doi.org/10.3390/brainsci10040247
Obayashi S. The Supplementary Motor Area Responsible for Word Retrieval Decline After Acute Thalamic Stroke Revealed by Coupled SPECT and Near-Infrared Spectroscopy. Brain Sciences. 2020; 10(4):247. https://doi.org/10.3390/brainsci10040247
Chicago/Turabian StyleObayashi, Shigeru. 2020. "The Supplementary Motor Area Responsible for Word Retrieval Decline After Acute Thalamic Stroke Revealed by Coupled SPECT and Near-Infrared Spectroscopy" Brain Sciences 10, no. 4: 247. https://doi.org/10.3390/brainsci10040247