Maternal Depression Affects Infants’ Lexical Processing Abilities in the Second Year of Life

 , , ,
, , ,
Abstract
:1. Introduction
1.1. Maternal Depression and Anxiety and Links with Language Development
1.2. Language Learning and Social–Environmental Influences
1.3. The Present Study
2. Materials and Methods
2.1. Participants
2.2. Maternal Measures
2.3. Infant Measures
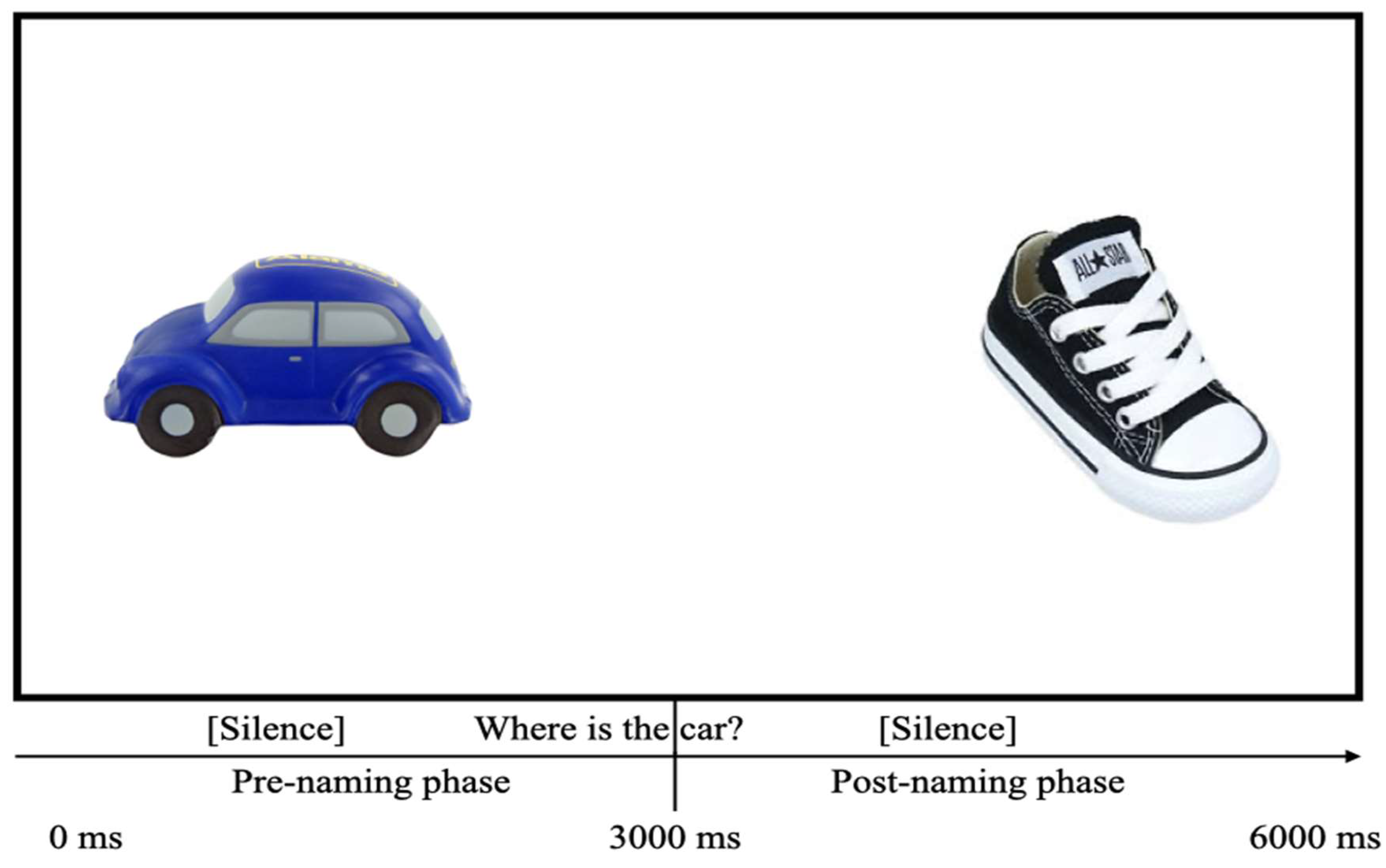
2.3.1. Lexical Processing
2.3.2. Expressive Vocabulary Checklist
3. Results
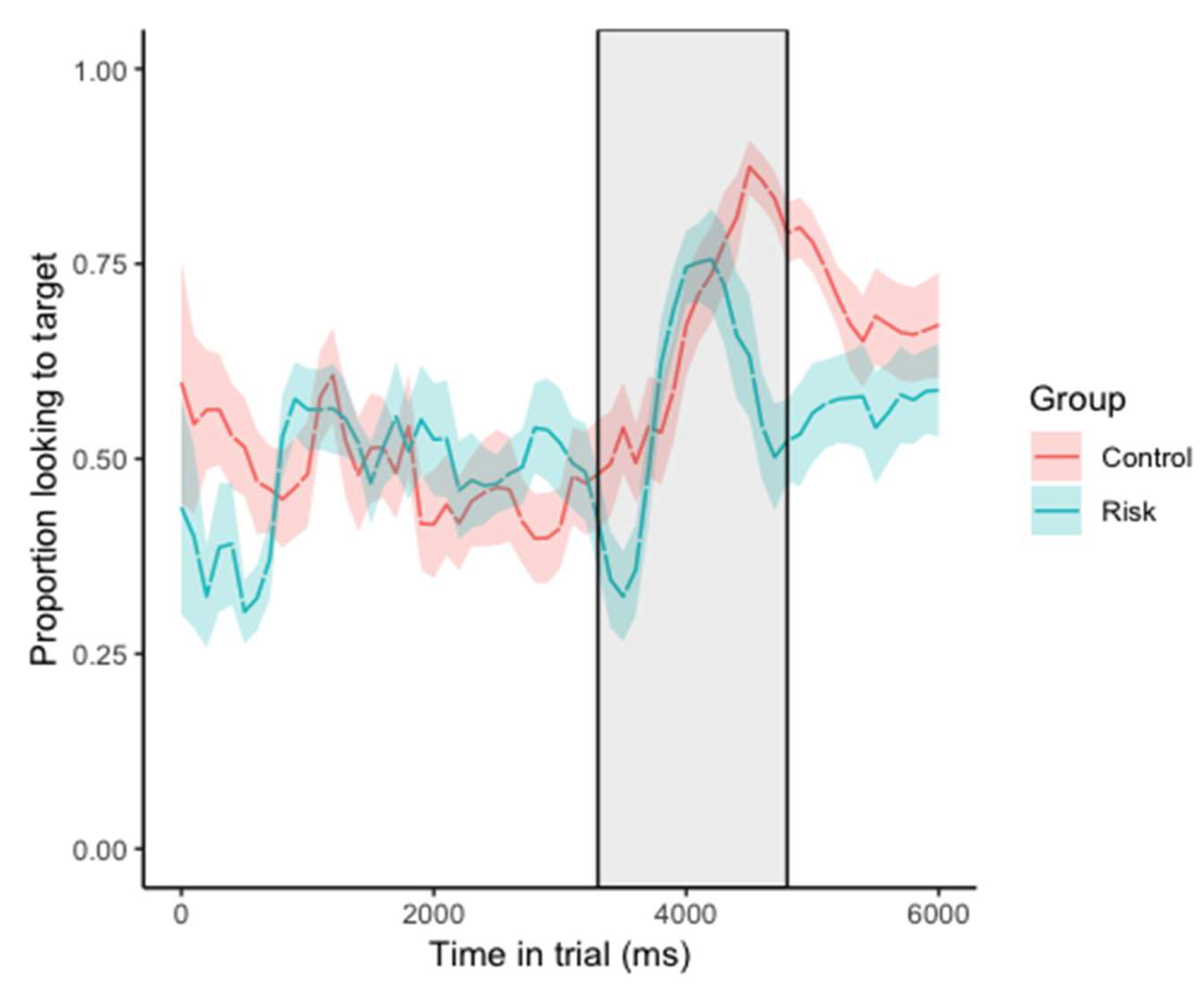
3.1. Lexical Processing
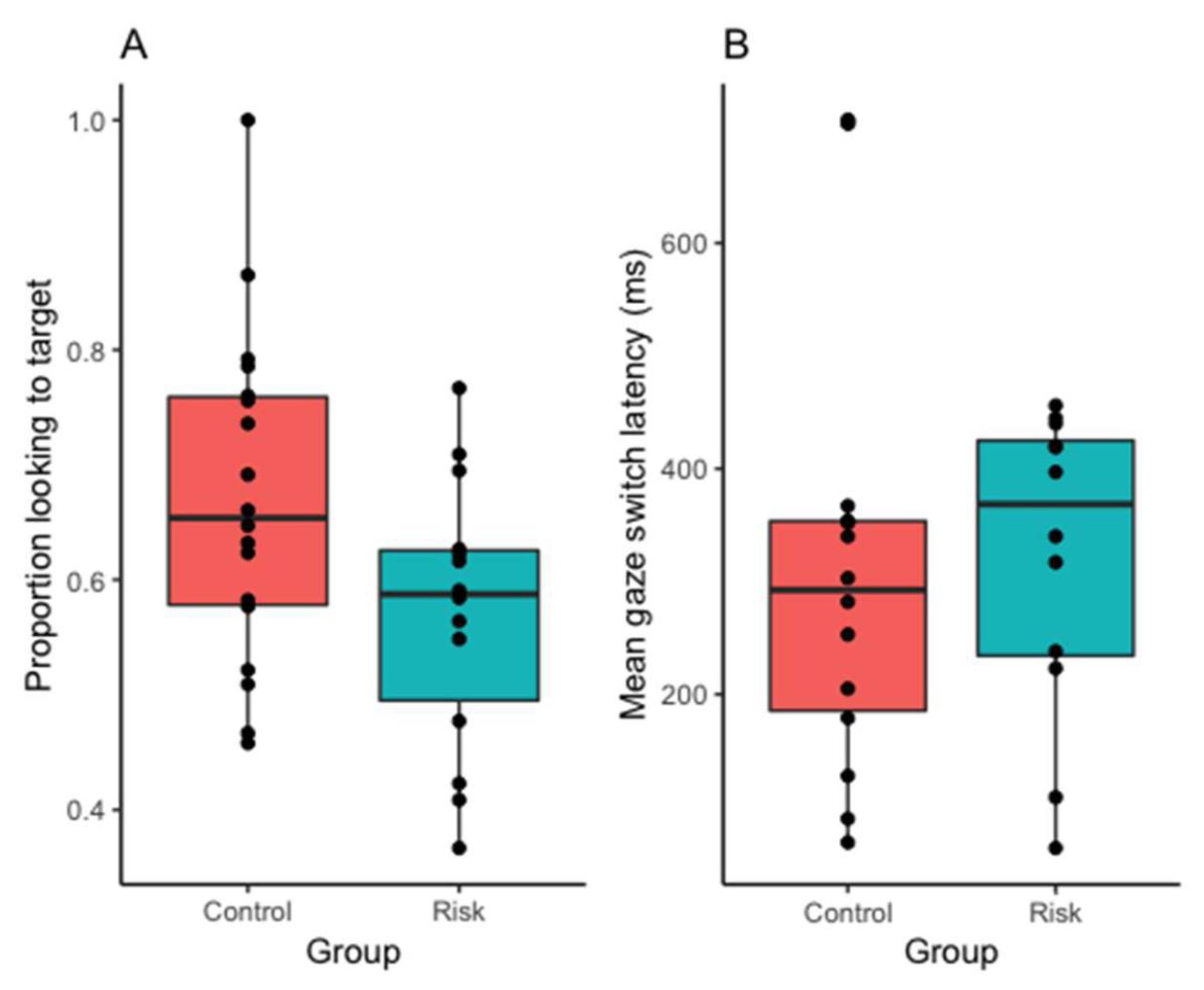
3.1.1. Accuracy
3.1.2. Latency
3.2. Expressive Vocabulary Size
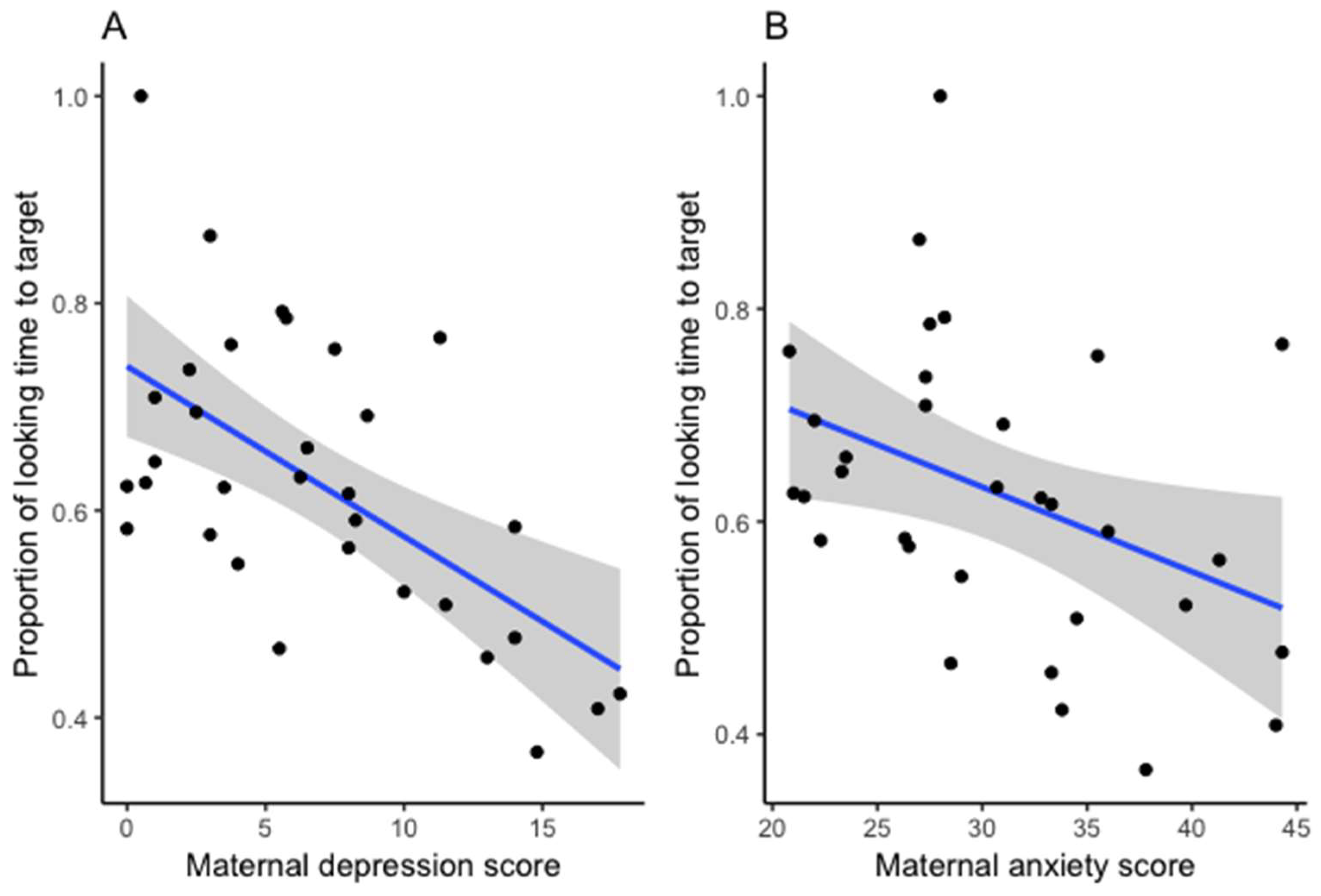
3.3. Links between Infants’ Lexical Abilities and Maternal Depression and Anxiety Measures
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Nature and Design; Harvard University Press: Cambridge, MA, USA, 1979. [Google Scholar]
- Papoušek, M. Communication in early infancy: An arena of intersubjective learning. Infant Behav. Dev. 2007, 30, 258–266. [Google Scholar] [CrossRef]
- Tamis-LeMonda, C.S.; Bornstein, M.H.; Baumwell, L. Maternal responsiveness and children’s achievement of language milestones. Child Dev. 2001, 72, 748–767. [Google Scholar] [CrossRef] [PubMed]
- Matthey, S.; Barnett, B.; Howie, P.; Kavanagh, D.J. Diagnosing postpartum depression in mothers and fathers: Whatever happened to anxiety? J. Affect. Disord. 2003, 74, 139–147. [Google Scholar] [CrossRef]
- Reck, C.; Noe, D.; Gerstenlauer, J.; Stehle, E. Effects of postpartum anxiety disorders and depression on maternal self-confidence. Infant Behav. Dev. 2012, 35, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Beebe, B.; Lachmann, F.; Jaffe, J.; Markese, S.; Buck, K.A.; Chen, H.; Andrews, H. Maternal postpartum depressive symptoms and 4-month mother–infant interaction. Psychoanal. Psychol. 2012, 29, 383–407. [Google Scholar] [CrossRef]
- Field, T. Infants of depressed mothers. Infant Behav. Dev. 1995, 18, 1–13. [Google Scholar] [CrossRef]
- Brookman, R.; Kalashnikova, M.; Conti, J.; Xu Rattanasone, N.; Grant, K.-A.; Demuth, K.; Burnham, D. Depression and Anxiety in the Postnatal Period: An Examination of Infants’ Home Language Environment, Vocalizations, and Expressive Language Abilities. Child Dev. 2020, 91, e1211–e1230. [Google Scholar] [CrossRef]
- Reck, C.; Van Den Bergh, B.; Tietz, A.; Müller, M.; Ropeter, A.; Zipser, B.; Pauen, S. Maternal avoidance, anxiety cognitions and interactive behaviour predicts infant development at 12 months in the context of anxiety disorders in the postpartum period. Infant Behav. Dev. 2018, 50, 116–131. [Google Scholar] [CrossRef]
- Kaplan, P.S.; Danko, C.M.; Everhart, K.D.; Diaz, A.; Asherin, R.M.; Vogeli, J.M.; Fekri, S.M. Maternal depression and expressive communication in one-year-old infants. Infant Behav. Dev. 2014, 37, 398–405. [Google Scholar] [CrossRef] [Green Version]
- Sohr-Preston, S.L.; Scaramella, L.V. Implications of timing of maternal depressive symptoms for early cognitive and language development. Clin. Child Fam. Psychol. Rev. 2006, 9, 65–83. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Pub.: Philadelphia, PA, USA, 2013. [Google Scholar]
- Leach, L.S.; Poyser, C.; Fairweather-Schmidt, K. Maternal perinatal anxiety: A review of prevalence and correlates. Clin. Psychol. 2007, 21, 4–19. [Google Scholar] [CrossRef]
- Barlow, D.H. Anxiety and Its Disorders: The Nature and Treatment of Anxiety and Panic; Guilford Press: New York, NY, USA, 2004. [Google Scholar]
- Farr, S.L.; Dietz, P.M.; O’Hara, M.W.; Burley, K.; Ko, J.Y. Postpartum anxiety and comorbid depression in a population-based sample of women. J. Women’s Health 2014, 23, 120–128. [Google Scholar] [CrossRef] [PubMed]
- NICHD Early Child Care Research Network. Chronicity of maternal depressive symptoms, maternal sensitivity, and child functioning at 36 months. Dev. Psychol. 1999, 35, 1297–1310. [Google Scholar] [CrossRef]
- Bayley, N. Bayley Scales of Infant and Toddler Development; PsychCorp, Pearson: San Antonio, TX, USA, 2006. [Google Scholar]
- Grant, K.-A.; McMahon, C.; Austin, M.-P. Maternal anxiety during the transition to parenthood: A prospective study. J. Affect. Disord. 2008, 108, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Kaitz, M.; Maytal, H.R.; Devor, N.; Bergman, L.; Mankuta, D. Maternal anxiety, mother–infant interactions, and infants’ response to challenge. Infant Behav. Dev. 2010, 33, 136–148. [Google Scholar] [CrossRef]
- Kuhl, P.K. Is speech learning “gated” by the social brain? Dev. Sci. 2007, 10, 110–120. [Google Scholar] [CrossRef]
- Rowe, M.L.; Snow, C.E. Analyzing input quality along three dimensions: Interactive, linguistic, and conceptual. J. Child Lang. 2019, 1, 17. [Google Scholar] [CrossRef] [Green Version]
- Kuhl, P.K. Early language acquisition: Cracking the speech code. Nat. Rev. Neurosci. 2004, 5, 831–843. [Google Scholar] [CrossRef]
- Huang, Z.J.; Lewin, A.; Mitchell, S.J.; Zhang, J. Variations in the relationship between maternal depression, maternal sensitivity, and child attachment by race/ethnicity and nativity: Findings from a nationally representative cohort study. Matern. Child Health J. 2012, 16, 40–50. [Google Scholar] [CrossRef]
- Gilkerson, J.; Richards, J.A.; Warren, S.F.; Oller, D.K.; Russo, R.; Vohr, B. Language Experience in the Second Year of Life and Language Outcomes in Late Childhood. Pediatrics 2018, 142, e20174276. [Google Scholar] [CrossRef] [Green Version]
- Romeo, R.R.; Leonard, J.A.; Robinson, S.T.; West, M.R.; Mackey, A.P.; Rowe, M.L.; Gabrieli, J.D.E. Beyond the 30-Million-Word Gap: Children’s Conversational Exposure Is Associated With Language-Related Brain Function. Psychol. Sci. 2018, 29, 700–710. [Google Scholar] [CrossRef] [PubMed]
- Weisleder, A.; Fernald, A. Talking to children matters: Early language experience strengthens processing and builds vocabulary. Psychol. Sci. 2013, 24, 2143–2152. [Google Scholar] [CrossRef] [PubMed]
- Fernald, A.; Pinto, J.P.; Swingley, D.; Weinberg, A.; McRoberts, G.W. Rapid Gains in Speed of Verbal Processing by infants in the 2nd year. Psychol. Sci. 1998, 9, 228–231. [Google Scholar] [CrossRef]
- Fernald, A. Speech to infants as hyperspeech: Knowledge-driven processes in early word recognition. Phonetica 2000, 57, 242–254. [Google Scholar] [CrossRef]
- Fernald, A.; Perfors, A.; Marchman, V.A. Picking up speed in understanding: Speech processing efficiency and vocabulary growth across the 2nd year. Dev. Psychol. 2006, 42, 98. [Google Scholar] [CrossRef] [Green Version]
- Marchman, V.A.; Fernald, A. Speed of word recognition and vocabulary knowledge in infancy predict cognitive and language outcomes in later childhood. Dev. Sci. 2008, 11, F9–F16. [Google Scholar] [CrossRef]
- Marchman, V.A.; Adams, K.A.; Loi, E.C.; Fernald, A.; Feldman, H.M. Early language processing efficiency predicts later receptive vocabulary outcomes in children born preterm. Child Neuropsychol. 2016, 22, 649–665. [Google Scholar] [CrossRef] [Green Version]
- Marchman, V.A.; Loi, E.C.; Adams, K.A.; Ashland, M.; Fernald, A.; Feldman, H.M. Speed of language comprehension at 18 months old predicts school-relevant outcomes at 54 months old in children born Preterm. J. Dev. Behav. Pediatr. 2018, 39, 246–253. [Google Scholar] [CrossRef]
- Morgan, P.L.; Farkas, G.; Hillemeier, M.M.; Hammer, C.S.; Maczuga, S. 24-Month-Old Children With Larger Oral Vocabularies Display Greater Academic and Behavioral Functioning at Kindergarten Entry. Child Dev. 2016, 86, 1351–1370. [Google Scholar] [CrossRef] [Green Version]
- Donnelly, S.; Kidd, E. Individual differences in lexical processing efficiency and vocabulary in toddlers: A longitudinal investigation. J. Exp. Child Psychol. 2020, 192, 104781. [Google Scholar] [CrossRef]
- Fenson, L.; Marchman, V.A.; Thal, D.J.; Dale, P.S.; Reznick, J.S. MacArthur-Bates Communicative Development Inventories; Paul H. Brookes Publishing Co.: Baltimore, MD, USA, 2007. [Google Scholar]
- Feldman, H.M.; Dollaghan, C.A.; Campbell, T.F.; Kurs-Lasky, M.; Janosky, J.E.; Paradise, J.L. Measurement properties of the MacArthur Communicative Development Inventories at ages one and two years. Child Dev. 2000, 71, 310–322. [Google Scholar] [CrossRef] [PubMed]
- Fernald, A.; Zangl, R.; Portillo, A.L.; Marchman, V.A. Looking while listening: Using eye movements to monitor spoken language. In Developmental Psycholinguistics: On-Line Methods in Children’s Language Processing; John Benjamins Publishing: Amsterdam, The Netherlands, 2008; Volume 44, p. 97. [Google Scholar]
- Eaton, W.W.; Smith, C.; Ybarra, M.; Muntaner, C.; Tien, A. Center for Epidemiologic Studies Depression Scale: Review and revision (CESD and CESD-R). In The Use of Psychological Testing for Treatment Planning and Outcomes Assessment: Instruments for Adults; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2004. [Google Scholar]
- Engle, P.L. Maternal mental health: Program and policy implications. Am. J. Clin. Nutr. 2009, 89, 963S–966S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Dam, N.T.; Earleywine, M. Validation of the Center for Epidemiologic Studies Depression Scale—Revised (CESD-R): Pragmatic depression assessment in the general population. Psychiatry Res. 2011, 186, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.; Vagg, P.R.; Jacobs, G.A. Manual for the State-Trait Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Glasheen, C.; Richardson, G.A.; Fabio, A. A systematic review of the effects of postnatal maternal anxiety on children. Arch. Women’s Ment. Health 2010, 13, 61–74. [Google Scholar] [CrossRef]
- Murray, L.; Halligan, S.; Cooper, P. Effects of postnatal depression on mother–infant interactions and child development. In Handbook of Infant Development, 2nd ed.; Bremner, G., Wachs, T., Eds.; Wiley-Blackwell: Chichester, UK, 2010; Volume 2, pp. 192–220. [Google Scholar]
- Song, J.Y.; Demuth, K.; Morgan, J. Effects of the acoustic properties of infant-directed speech on infant word recognition. J. Acoust. Soc. Am. 2010, 128, 389–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boersma, P.; Weenink, D. Praat, a system for doing phonetics by computer, version 3.4. Inst. Phon. Sci. Univ. Amst. Rep. 1996, 132, 182. [Google Scholar]
- Fernald, A.; Taeschner, T.; Dunn, J.; Papousek, M.; de Boysson-Bardies, B.; Fukui, I. A cross-language study of prosodic modifications in mothers’ and fathers’ speech to preverbal infants. J. Child Lang. 1989, 16, 477–501. [Google Scholar] [CrossRef]
- Ma, W.; Golinkoff, R.M.; Houston, D.M.; Hirsh-Pasek, K. Word Learning in Infant- and Adult-Directed Speech. Lang. Learn. Dev. 2011, 7, 185–201. [Google Scholar] [CrossRef] [Green Version]
- Thiessen, E.D.; Hill, E.A.; Saffran, J.R. Infant-directed speech facilitates word segmentation. Infancy 2005, 7, 53–71. [Google Scholar] [CrossRef]
- Swingley, D.; Aslin, R.N. Spoken word recognition and lexical representation in very young children. Cognition 2000, 76, 147–166. [Google Scholar] [CrossRef] [Green Version]
- Dink, J.W.; Ferguson, B. eyetrackingR: An R Library for Eye-Tracking Data Analysis. 2015. Available online: www.eyetracking-r.com (accessed on 1 April 2019).
- Kalashnikova, M.; Schwarz, I.C.; Burnham, D. OZI: Australian English Communicative Development Inventory. First Lang. 2016, 36, 407–427. [Google Scholar] [CrossRef]
- Fenson Larry Dale, P.S.; Reznick, J.S.; Bates, E.; Thal, D.J.; Pethick, S.J.; Stiles, J. Variability in early communicative development. Monogr. Soc. Res. Child Dev. 1994. [Google Scholar] [CrossRef]
- Hurtado, N.; Marchman, V.A.; Fernald, A. Does input influence uptake? Links between maternal talk, processing speed and vocabulary size in Spanish-learning children. Dev. Sci. 2008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egger, J.; Rowland, C.F.; Bergmann, C. Improving the robustness of infant lexical processing speed measures. Behav. Res. Methods 2020, 52, 2188–2201. [Google Scholar] [CrossRef]
- Milgrom, J.; Westley, D.T.; Gemmill, A.W. The mediating role of maternal responsiveness in some longer term effects of postnatal depression on infant development. Infant Behav. Dev. 2004, 27, 443–454. [Google Scholar] [CrossRef]
- Masi, G.; Millepiedi, S.; Mucci, M.; Poli, P.; Bertini, N.; Milantoni, L. Generalized anxiety disorder in referred children and adolescents. J. Am. Acad. Child Adolesc. Psychiatry 2004, 43, 752–760. [Google Scholar] [CrossRef]
- Golinkoff, R.M.; Can, D.D.; Soderstrom, M.; Hirsh-Pasek, K. (Baby) Talk to Me: The Social Context of Infant-Directed Speech and Its Effects on Early Language Acquisition. Curr. Dir. Psychol. Sci. 2015, 24, 339–344. [Google Scholar] [CrossRef]
- Bettes, B.A. Maternal Depression and Motherese: Temporal and Intonational Features. Child Dev. 1988, 59, 1089–1096. [Google Scholar] [CrossRef]
- Lam-Cassettari, C.; Kohlhoff, J. Effect of maternal depression on infant-directed speech to prelinguistic infants: Implications for language development. PLoS ONE 2020, 15, e0236787. [Google Scholar] [CrossRef]
- Porritt, L.; Zinser, M.; Bachorowski, J.; Kaplan, P. Depression diagnoses and fundamental frequency-based acoustic cues in maternal infant-directed speech. Lang. Learn. Dev. 2015, 10, 51–67. [Google Scholar] [CrossRef]
- Kaplan, P.; Jung, P.; Ryther, J.; Zarlengo-Strouse, P.; Zar, P.; We, F.; Scheuneman, D. Infant-Directed Versus Adult-Directed Speech as Signals for Faces. Dev. Psychol. 1996, 32, 880–891. [Google Scholar] [CrossRef]
- Kaplan, P.S.; Bachorowski, J.; Zarlengo-Strouse, P. Child-directed speech produced by mothers with symptoms of depression fails to promote associative learning in 4-month-old infants. Child Dev. 1999, 70, 560–570. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, P.S.; Dungan, J.K.; Zinser, M.C. Infants of chronically depressed mothers learn in response to male, but not female, infant-directed speech. Dev. Psychol. 2004, 40, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Austin, M.P.; Priest, S.R. Clinical issues in perinatal mental health: New developments in the detection and treatment of perinatal mood and anxiety disorders. Acta Psychiatr. Scand. 2005, 112, 97–104. [Google Scholar] [CrossRef]
- Dennis, C.L.; Stewart, D.E. Treatment of postpartum depression, part 1: A critical review of biological interventions. J. Clin. Psychiatry 2004, 65, 1242–1251. [Google Scholar] [CrossRef]
- Field, T. Maternal Depression Effects on Infants and Early Interventions 1. Prev. Med. 1998, 203, 200–203. [Google Scholar] [CrossRef]
- Murray, L.; Cooper, P. Intergenerational transmission of affective and cognitive processes associated with depression: Infancy and the pre-school years. In Unipolar Depression: A Lifespan Perspective; Oxford University Press: Oxford, UK, 2003; pp. 17–46. [Google Scholar]
- Nielsen, D.; Videbech, P.; Hedegaard, M.; Dalby, J.; Secher, N.J. Postpartum depression: Identification of women at risk. BJOG Int. J. Obstet. Gynaecol. 2000, 107, 1210–1217. [Google Scholar] [CrossRef]
- Roberts, M.Y.; Curtis, P.R.; Sone, B.J.; Hampton, L.H. Association of parent training with child language development: A systematic review and meta-analysis. JAMA Pediatr. 2019, 173, 671–680. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mother and Infant Characteristics | Total Sample (n = 36) | Control Group (n = 19) | Risk Group (n = 17) |
|---|---|---|---|
| Infant Gender: n (%) | |||
| Male Female | 19 (53) 17 (47) | 12 (63) 7 (37) | 7 (41) 10 (59) |
| Birth weight (kg) | |||
| Range M (SD) | 2.38–4.89 3.49 (0.52) | 2.38–4.74 3.38 (0.53) | 3.01–4.89 3.61 (0.51) |
| Birth order: n (%) | |||
| First-born | 26 (72) | 13 (68) | 13 (77) |
| Maternal Age | |||
| Range M (SD) | 26–41 32.69 (4.05) | 26–40 32.74 (3.57) | 26–41 32.65 (4.64) |
| Maternal education | |||
| Mean rank | 15.42 | 21.94 | |
| Household income | |||
| Mean rank | 15.58 | 21.76 |
| Variable | Accuracy | Latency | Mean Depression | Mean Anxiety |
|---|---|---|---|---|
| OZI | 0.594 *** | −0.609 ** | −0.455 * | −0.351 |
| Accuracy | 1/1 | −0.491 * | −0.538 ** | −0.434 * |
| Latency | 1/1 | 0.334 | 0.318 | |
| Depression | 1/1 | 0.758 ** |
| Model 1: Proportion of Looking Time to Target | ||||||||
|---|---|---|---|---|---|---|---|---|
| Removed covariate | R2 = 0.389, F(2, 28) = 8.930, p = 0.001 | |||||||
| β | SE | T | P | |||||
| Vocabulary size | 0.327 | 2.035 | 0.052 | |||||
| Entered predictor variables | ||||||||
| Mean postnatal depression | −0.677 | 0.006 | −3.180 | 0.004 *** | ||||
| Mean postnatal anxiety | 0.076 | 0.004 | 0.358 | 0.723 | ||||
| Model 2: Latency of Gaze Switch to Target | ||||||||
| Removed covariate | R2 = 0.286, F(2, 18) = 3.609, p = 0.048 | |||||||
| β | SE | T | P | |||||
| Vocabulary size | −0.383 | 0.328 | −1.798 | 0.090 | ||||
| Entered predictor variables | ||||||||
| Mean postnatal depression | 0.399 | 5.584 | 1.429 | 0.170 | ||||
| Mean postnatal anxiety | 0.173 | 4.234 | 0.618 | 0.544 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brookman, R.; Kalashnikova, M.; Conti, J.; Xu Rattanasone, N.; Grant, K.-A.; Demuth, K.; Burnham, D. Maternal Depression Affects Infants’ Lexical Processing Abilities in the Second Year of Life. Brain Sci. 2020, 10, 977. https://doi.org/10.3390/brainsci10120977
Brookman R, Kalashnikova M, Conti J, Xu Rattanasone N, Grant K-A, Demuth K, Burnham D. Maternal Depression Affects Infants’ Lexical Processing Abilities in the Second Year of Life. Brain Sciences. 2020; 10(12):977. https://doi.org/10.3390/brainsci10120977
Chicago/Turabian StyleBrookman, Ruth, Marina Kalashnikova, Janet Conti, Nan Xu Rattanasone, Kerry-Ann Grant, Katherine Demuth, and Denis Burnham. 2020. "Maternal Depression Affects Infants’ Lexical Processing Abilities in the Second Year of Life" Brain Sciences 10, no. 12: 977. https://doi.org/10.3390/brainsci10120977