Effects of Social Isolation and Loneliness in Children with Neurodevelopmental Disabilities: A Scoping Review

Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy:
2.3. Study Selection/Screening:
2.4. Data Collection and Synthesis:
2.5. Methodological Quality Appraisal:
3. Results
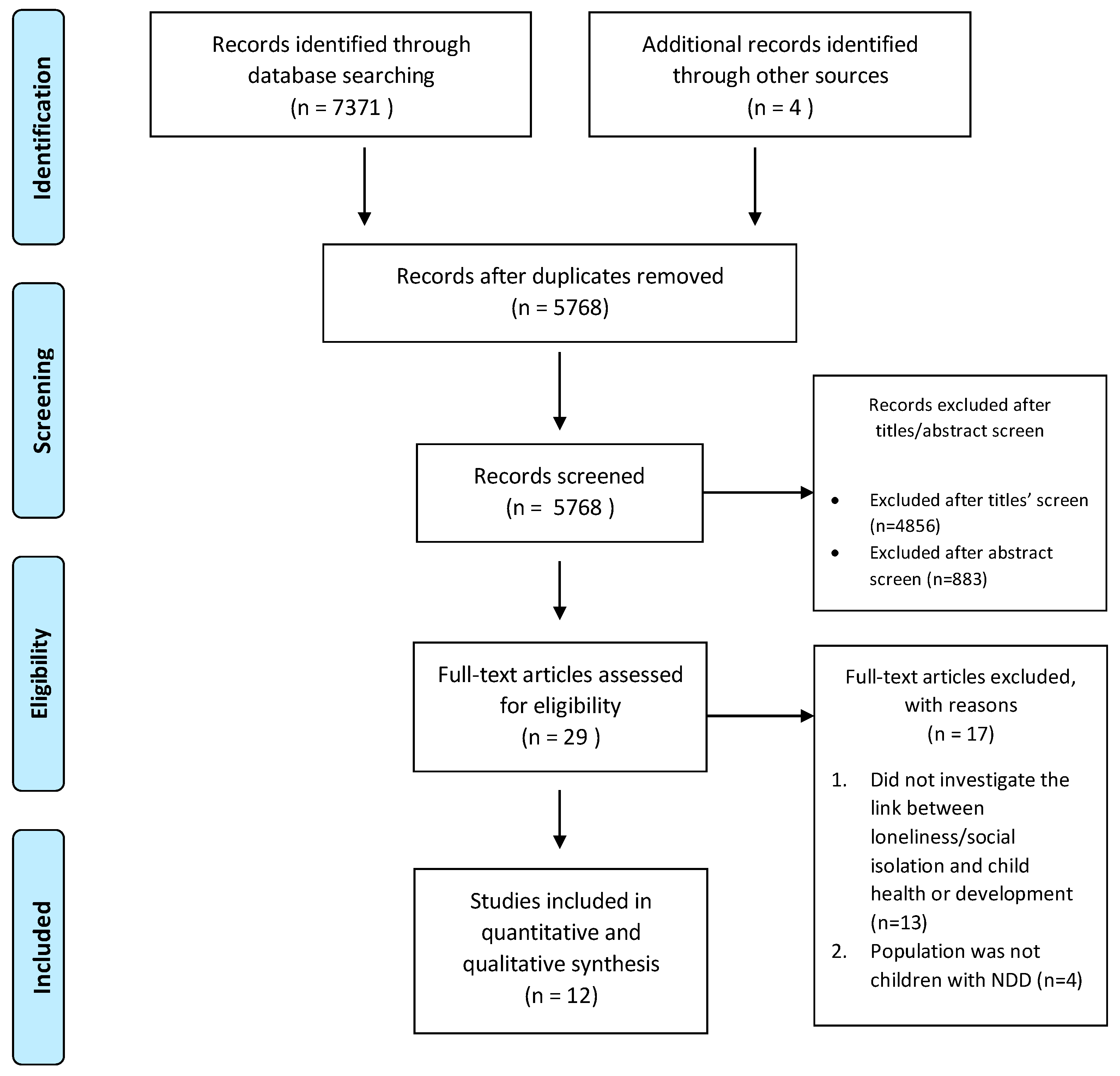
3.1. Identified Studies
3.2. Study Characteristics
3.3. Study Participants
3.4. Measurement of Loneliness and Social Isolation
3.5. Study Outcomes
3.6. Quality Appraisal
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Complete Search Strategy for Each Database
| S44 | S9 AND S43 | Limiters-Age Groups: Childhood (birth-12 yrs), Adolescence (13–17 yrs) | Interface-EBSCOhost Research Databases |
| Search modes-Boolean/Phrase | Search Screen -Advanced Search | ||
| Database - PsycINFO | |||
| S43 | (S1 OR S2 OR S10 OR S11 OR S12 OR S13 OR S14 OR S15 OR S16 OR S17 OR S18 OR S19 OR S20 OR S21 OR S22 OR S23 OR S24 OR S25 OR S26 OR S27 OR S28 OR S29 OR S30 OR S31 OR S32 OR S33 OR S34 OR S35 OR S36 OR S37 OR S38 OR S39 OR S40 OR S41 OR S42) | Search modes-Boolean/Phrase | Interface - EBSCOhost Research Databases |
| Search Screen -Advanced Search | |||
| Database-PsycINFO | |||
| S42 | DE “Cerebral Palsy” | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen -Advanced Search | |||
| Database-PsycINFO | |||
| S41 | cerebral palsy | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S40 | down syndrome or trisomy 21 | Search modes - Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S39 | DE “Down’s Syndrome” | Search modes - Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S38 | movement dis* | Search modes - Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S37 | DE “Movement Disorders” | Search modes - Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S36 | Schizophrenia | Search modes - Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S35 | DE “Schizophrenia” | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S34 | Mutism | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S33 | DE “Mutism” | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S32 | Tourette OR Tic dis* | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S31 | DE “Tourette Syndrome” OR DE “Tics” | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S30 | reactive attachment dis* | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S29 | motor skills dis* | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S28 | DE “Motor Skills” OR DE “Movement Disorders” | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen -Advanced Search | |||
| Database-PsycINFO | |||
| S27 | dyslexia OR acalculia OR agraphia | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen -Advanced Search | |||
| Database-PsycINFO | |||
| S26 | learning dis* | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S25 | DE “Learning Disabilities” OR DE “Learning Disorders” OR DE “Dyslexia” OR DE “Acalculia” OR DE “Agraphia” | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S24 | development* dis* | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S23 | intellectual dis* | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S22 | communication dis* | Search modes - Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S21 | DE “Communication Disorders” OR DE “Language Disorders” OR DE “Developmental Disabilities” | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S20 | autism | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S19 | DE “Autism Spectrum Disorders” | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S18 | child development dis* | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S17 | DE “Intellectual Development Disorder” | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S16 | conduct dis* | Search modes - Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S15 | DE “Conduct Disorder” | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S14 | child behavio* dis* | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S13 | attention deficit | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S12 | DE “Attention Deficit Disorder with Hyperactivity” OR DE “Attention Deficit Disorder” | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S11 | anxiety | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S10 | DE “Anxiety” OR DE “Anxiety Disorders” | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S9 | (S3 OR S4 OR S5 OR S6 OR S7 OR S8) | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S8 | social* participat* | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S7 | DE “Social Isolation” OR DE “Social Deprivation” | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S6 | DE “Patient Seclusion” | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S5 | social* isolat* | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S4 | lonel* | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S3 | DE “Loneliness” | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S2 | Neurodevelopmental Disorders” OR Neurodevelopmental dis* | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen-Advanced Search | |||
| Database-PsycINFO | |||
| S1 | DE “Neurodevelopmental Disorders” | Search modes-Boolean/Phrase | Interface-EBSCOhost Research Databases |
| Search Screen -Advanced Search | |||
| Database-PsycINFO | |||
| Note: * search function. | |||
References
- Frey, L.M.; Wilhite, K. Our Five Basic Needs: Application for Understanding the Function of Behavior. Interv. Sch. Clin. 2005, 40, 156–160. [Google Scholar]
- Pyszczynski, T.; Greenberg, J.; Solomon, S. Why Do We Need What We Need? A Terror Management Perspective on the Roots of Human Social Motivation. Psychol. Inq. 1997, 8, 1–20. [Google Scholar] [CrossRef]
- Bolmsjö, I.; Tengland, P.A.; Rämgård, M. Existential loneliness: An attempt at an analysis of the concept and the phenomenon. Nurs. Ethics 2019, 26, 1310–1325. [Google Scholar] [CrossRef]
- Weiss, R.S. Loneliness: The Experience of Emotional and Social Isolation; MIT Press: Cambridge, MA, USA, 1973. [Google Scholar]
- Hawkley, L.C.; Cacioppo, J.T. Loneliness matters: A theoretical and empirical review of consequences and mechanisms. Ann. Behav. Med. A Publ. Soc. Behav. Med. 2010, 40, 218–227. [Google Scholar] [CrossRef] [Green Version]
- Lyyra, N.; Valimaa, R.; Tynjala, J. Loneliness and subjective health complaints among school-aged children. Scand. J. Public Health 2018, 46, 87–93. [Google Scholar] [CrossRef] [Green Version]
- Fried, L.; Prohaska, T.; Burholt, V.; Burns, A.; Golden, J.; Hawkley, L.; Lawlor, B.; Leavey, G.; Lubben, J.; O’Sullivan, R.; et al. A unified approach to loneliness. Lancet 2020, 395, 114. [Google Scholar] [CrossRef] [Green Version]
- Heinrich, L.M.; Gullone, E. The clinical significance of loneliness: A literature review. Clin. Psychol. Rev. 2006, 26, 695–718. [Google Scholar]
- Peplau, L.A.; Perlman, D.; Perlman, D. Loneliness: A Sourcebook of Current Theory, Research and Therapy; Wiley: Hoboken, NJ, USA, 1982. [Google Scholar]
- Stickley, A.; Koyanagi, A.; Koposov, R.; Blatný, M.; Hrdlička, M.; Schwab-Stone, M.; Ruchkin, V. Loneliness and its association with psychological and somatic health problems among Czech, Russian and U.S. adolescents. BMC Psychiatry 2016, 16, 128. [Google Scholar] [CrossRef]
- Petitte, T.; Mallow, J.; Barnes, E.; Petrone, A.; Barr, T.; Theeke, L. A Systematic Review of Loneliness and Common Chronic Physical Conditions in Adults. Open Psychol. J. 2015, 8, 113–132. [Google Scholar] [CrossRef]
- Caspi, A.; Harrington, H.; Moffitt, T.E.; Milne, B.J.; Poulton, R. Socially isolated children 20 years later: Risk of cardiovascular disease. Arch. Pediatrics Adolesc. Med. 2006, 160, 805–811. [Google Scholar] [CrossRef] [Green Version]
- Wilson, R.S.; Krueger, K.R.; Arnold, S.E.; Schneider, J.A.; Kelly, J.F.; Barnes, L.L.; Tang, Y.; Bennett, D.A. Loneliness and risk of Alzheimer disease. Arch. Gen. Psychiatry 2007, 64, 234–240. [Google Scholar] [CrossRef] [Green Version]
- Currie, G.; Szabo, J. Social isolation and exclusion: The parents’ experience of caring for children with rare neurodevelopmental disorders. Int. J. Qual. Stud. Health Well-Being 2020, 15, 1725362. [Google Scholar] [CrossRef] [Green Version]
- Neurodevelopmental Disorders. In Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association: Washington, DC, USA, 2013.
- Deckers, A.; Muris, P.; Roelofs, J. Being on your own or feeling lonely? Loneliness and other social variables in youths with autism spectrum disorders. Child Psychiatry Hum. Dev. 2017, 48, 828–839. [Google Scholar] [CrossRef] [Green Version]
- Bauminger, N.; Kasari, C. Loneliness and friendship in high-functioning children with autism. Child Dev. 2000, 71, 447–456. [Google Scholar]
- Bossaert, G.; Colpin, H.; Pijl, S.J.; Petry, K. Loneliness among students with special educational needs in mainstream seventh grade. Res. Dev. Disabil. 2012, 33, 1888–1897. [Google Scholar] [CrossRef] [Green Version]
- Bauminger, N.; Shulman, C.; Agam, G. Peer interaction and loneliness in high-functioning children with autism. J. Autism Dev. Disord. 2003, 33, 489–507. [Google Scholar] [CrossRef]
- Lasgaard, M.; Nielsen, A.; Eriksen, M.E.; Goossens, L. Loneliness and social support in adolescent boys with autism spectrum disorders. J. Autism Dev. Disord. 2010, 40, 218–226. [Google Scholar] [CrossRef]
- Locke, J.; Ishijima, E.H.; Kasari, C.; London, N. Loneliness, friendship quality and the social networks of adolescents with high-functioning autism in an inclusive school setting. J. Res. Spec. Educ. Needs 2010, 10, 74–81. [Google Scholar] [CrossRef]
- Poulsen, A.A.; Ziviani, J.M.; Cuskelly, M.; Smith, R. Boys with developmental coordination disorder: Loneliness and team sports participation. Am. J. Occup. Ther. Off. Publ. Am. Occup. Ther. Assoc. 2007, 61, 451–462. [Google Scholar]
- Poulsen, A.A.; Ziviani, J.M.; Johnson, H.; Cuskelly, M. Loneliness and life satisfaction of boys with developmental coordination disorder: The impact of leisure participation and perceived freedom in leisure. Hum. Mov. Sci. 2008, 27, 325–343. [Google Scholar] [CrossRef]
- Al-Yagon, M. Perceived Close Relationships With Parents, Teachers, and Peers: Predictors of Social, Emotional, and Behavioral Features in Adolescents With LD or Comorbid LD and ADHD. J. Learn. Disabil. 2016, 49, 597–615. [Google Scholar] [CrossRef]
- Karpov, Y.V. Development Through the Lifespan. In Vygotsky’s Educational Theory in Cultural Context; Kozulin, A., Gindis, B., Miller, S.M., Ageyev, V.S., Eds.; Cambridge University Press: Cambridge, UK, 2003; pp. 138–155. [Google Scholar] [CrossRef]
- Parker, J.G.; Asher, S.R. Peer relations and later personal adjustment: Are low-accepted children at risk? Psychol. Bull. 1987, 102, 357–389. [Google Scholar] [CrossRef]
- Rieber, R.W.; Carton, A.S. The Collected Works of L.S. Vygotsky: The Fundamentals of Defectology (Abnormal Psychology and Learning Disabilities); Springer: Boston, MA, USA, 1993. [Google Scholar] [CrossRef]
- Ong, A.D.; Uchino, B.N.; Wethington, E. Loneliness and Health in Older Adults: A Mini-Review and Synthesis. Gerontology 2016, 62, 443–449. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Peters, M.D.J.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for conducting systematic scoping reviews. Int. J. Evid.-Based Healthc. 2015, 13. [Google Scholar]
- Sirriyeh, R.; Lawton, R.; Gardner, P.; Armitage, G. Reviewing studies with diverse designs: The development and evaluation of a new tool. J. Eval. Clin. Pract. 2012, 18, 746–752. [Google Scholar] [CrossRef]
- Zach, S.; Yazdi-Ugav, O.; Zeev, A. Academic achievements, behavioral problems, and loneliness as predictors of social skills among students with and without learning disorders. Sch. Psychol. Int. 2016, 37, 378–396. [Google Scholar] [CrossRef]
- Valås, H. Students with learning disabilities and low-achieving students: Peer acceptance, loneliness, self-esteem, and depression. Soc. Psychol. Educ. Int. J. 1999, 3, 173–192. [Google Scholar] [CrossRef]
- Lackaye, T.; Margalit, M. Self-Efficacy, Loneliness, Effort, and Hope: Developmental Differences in the Experiences of Students with Learning Disabilities and Their Non-Learning Disabled Peers at Two Age Groups. Learn. Disabil. A Contemp. J. 2008, 6, 1–20. [Google Scholar]
- Idan, O.; Margalit, M. Socioemotional self-perceptions, family climate, and hopeful thinking among students with learning disabilities and typically achieving students from the same classes. J. Learn. Disabil. 2014, 47, 136–152. [Google Scholar] [CrossRef]
- Becker, S.P. Social Information Processing, Comorbid Mental Health Symptoms, and Peer Isolation among Children with Attention-Deficit/Hyperactivity Disorder; ProQuest Information & Learning; Miami University: Oxford, OH, USA, 2015. [Google Scholar]
- Asher, S.R.; Hymel, S.; Renshaw, P.D. Loneliness in Children. Child Dev. 1984, 55, 1456–1464. [Google Scholar] [CrossRef]
- Dovgan, K.N.; Mazurek, M.O. Relations among activity participation, friendship, and internalizing problems in children with autism spectrum disorder. Autism 2019, 23, 750–758. [Google Scholar] [CrossRef]
- White, S.W.; Roberson-Nay, R. Anxiety, social deficits, and loneliness in youth with autism spectrum disorders. J. Autism Dev. Disord. 2009, 39, 1006–1013. [Google Scholar] [CrossRef]
- Whitehouse, A.J.; Durkin, K.; Jaquet, E.; Ziatas, K. Friendship, loneliness and depression in adolescents with Asperger’s Syndrome. J. Adolesc. 2009, 32, 309–322. [Google Scholar] [CrossRef]
- Taylor, J.L.; Adams, R.E.; Bishop, S.L. Social participation and its relation to internalizing symptoms among youth with autism spectrum disorder as they transition from high school. Autism Res. 2017, 10, 663–672. [Google Scholar] [CrossRef]
- Hedley, D.; Uljarevic, M.; Foley, K.R.; Richdale, A.; Trollor, J. Risk and protective factors underlying depression and suicidal ideation in Autism Spectrum Disorder. Depress. Anxiety 2018, 35, 648–657. [Google Scholar] [CrossRef]
- Tillinger, M. The Influence of Friends and Family on Well-Being for Children and Adolescents with Developmental Disabilities; ProQuest Information & Learning; Boston College: Boston, MA, USA, 2014. [Google Scholar]
- Hauser-Cram, P.; Warfield, M.E.; Shonkoff, J.P.; Krauss, M.W., III. The Early Intervention Collaborative Study: Study Design and Methodology. Monogr. Soc. Res. Child Dev. 2001, 66, 22–53. [Google Scholar] [CrossRef]
- Tekinarslan, I.C.; Kucuker, S. Examination of the Psychometric Properties of the Children’s Loneliness Scale for Students with and without Special Needs in Inclusive Classrooms. Kuram Uygul. Egit. Bilimleri 2015, 15, 709. [Google Scholar]
- Ladd, G.W.; Profilet, S.M. The Child Behavior Scale: A teacher-report measure of young children’s aggressive, withdrawn, and prosocial behaviors. Dev. Psychol. 1996, 32, 1008–1024. [Google Scholar] [CrossRef]
- Ladd, G.W.; Herald-Brown, S.L.; Andrews, R.K. The Child Behavior Scale (CBS) revisited: A longitudinal evaluation of CBS subscales with children, preadolescents, and adolescents. Psychol. Assess. 2009, 21, 325–339. [Google Scholar] [CrossRef]
- Achenbach, T.M.; Rescorla, L. Manual for the ASEBA School-Age Forms & Profiles: An Integrated System of Multi-Informant Assessment; ASEBA: Burlington, VT, USA, 2001. [Google Scholar]
- Tehrani-Doost, M.; Shahrivar, Z.; Pakbaz, B.; Rezaie, A.; Ahmadi, F. Normative data and psychometric properties of the child behavior checklist and teacher rating form in an Iranian community sample. Iran. J. Pediatr. 2011, 21, 331–342. [Google Scholar]
- Jones, W.H. Loneliness and social exclusion. J. Soc. Clin. Psychol. 1990, 9, 214–220. [Google Scholar] [CrossRef]
- Leary, M.R. Responses to social exclusion—Social anxiety, jealousy, loneliness, depression, and low self-esteem. J. Soc. Clin. Psychol. 1990, 9, 221–229. [Google Scholar] [CrossRef]
- Mazurek, M.O. Loneliness, friendship, and well-being in adults with autism spectrum disorders. Autism 2014, 18, 223–232. [Google Scholar] [CrossRef]
- Cassidy, S.; Bradley, P.; Robinson, J.; Allison, C.; McHugh, M.; Baron-Cohen, S. Suicidal ideation and suicide plans or attempts in adults with Asperger’s syndrome attending a specialist diagnostic clinic: A clinical cohort study. Lancet Psychiatry 2014, 1, 142–147. [Google Scholar] [CrossRef] [Green Version]
- Lasgaard, M.; Goossens, L.; Elklit, A. Loneliness, depressive symptomatology, and suicide ideation in adolescence: Cross-sectional and longitudinal analyses. J. Abnorm. Child. Psychol. 2011, 39, 137–150. [Google Scholar] [CrossRef]
- Loades, M.E.; Chatburn, E.; Higson-Sweeney, N.; Reynolds, S.; Shafran, R.; Brigden, A.; Linney, C.; McManus, M.N.; Borwick, C.; Crawley, E. Rapid Systematic Review: The Impact of Social Isolation and Loneliness on the Mental Health of Children and Adolescents in the Context of COVID-19. J. Am. Acad. Child Adolesc. Psychiatry 2020. [Google Scholar] [CrossRef]
- Calati, R.; Ferrari, C.; Brittner, M.; Oasi, O.; Olié, E.; Carvalho, A.F.; Courtet, P. Suicidal thoughts and behaviors and social isolation: A narrative review of the literature. J. Affect. Disord. 2019, 245, 653–667. [Google Scholar] [CrossRef]
- Hymel, S.; Rubin, K.H.; Rowden, L.; LeMare, L. Children’s Peer Relationships: Longitudinal Prediction of Internalizing and Externalizing Problems from Middle to Late Childhood. Child Dev. 1990, 61, 2004–2021. [Google Scholar] [CrossRef]
- Marryat, L.; Thompson, L.; Minnis, H.; Wilson, P. Associations between social isolation, pro-social behaviour and emotional development in preschool aged children: A population based survey of kindergarten staff. BMC Psychol. 2014, 2. [Google Scholar] [CrossRef] [Green Version]
- Benner, A.D. Latino adolescents’ loneliness, academic performance, and the buffering nature of friendships. J. Youth Adolesc. 2011, 40, 556–567. [Google Scholar] [CrossRef] [Green Version]
- Sadeghi Bahmani, D.; Faraji, R.; Faraji, P.; Holsboer-Trachsler, E. Depression and loneliness did not affect academic achievement among university students. Eur. Psychiatry 2017, 41, S541. [Google Scholar] [CrossRef]
- Griswold, D.E.; Barnhill, G.P.; Myles, B.S.; Hagiwara, T.; Simpson, R.L. Asperger Syndrome and Academic Achievement. Focus Autism Other Dev. Disabil. 2002, 17, 94–102. [Google Scholar] [CrossRef]
- Turner, S.; Alborz, A. Academic attainments of children with Down’s syndrome: A longitudinal study. Br. J. Educ. Psychol. 2003, 73, 563–583. [Google Scholar] [CrossRef]
- Turner, S.; Alborz, A.; Gayle, V. Predictors of academic attainments of young people with Down’s syndrome. J. Intellect. Disabil. Res. 2008, 52, 380–392. [Google Scholar] [CrossRef] [Green Version]
- Venturini, E.; Parsons, T.D. Virtual Environments for Assessment of Social Exclusion in Autism: A Systematic Review. Rev. J. Autism Dev. Disord. 2018, 5, 408–421. [Google Scholar] [CrossRef]
- Peristeri, E.; Tsimpli, I.; Williams, K. Ostracism effects in children and adults with high functioning autism. In International Psychological Applications Conference and Trends Proceedings (InPact); Pracana, C., Ed.; World Institute for Advanced Research and Science: Lisbon, Portugal, 2014; pp. 62–67. [Google Scholar]
- Chandrasekhar, T.; Sikich, L. Challenges in the diagnosis and treatment of depression in autism spectrum disorders across the lifespan. Dialogues Clin. Neurosci. 2015, 17, 219–227. [Google Scholar]
- Matthews, N.L.; Orr, B.C.; Warriner, K.; DeCarlo, M.; Sorensen, M.; Laflin, J.; Smith, C.J. Exploring the effectiveness of a peer-mediated model of the PEERS curriculum: A pilot randomized control trial. J. Autism Dev. Disord. 2018, 48, 2458–2475. [Google Scholar] [CrossRef]
- Matthews, T.; Danese, A.; Wertz, J.; Ambler, A.; Kelly, M.; Diver, A.; Caspi, A.; Moffitt, T.E.; Arseneault, L. Social isolation and mental health at primary and secondary school entry: A longitudinal cohort study. J. Am. Acad. Child Adolesc. Psychiatry 2015, 54, 225–232. [Google Scholar] [CrossRef]
- Elmose, M.; Lasgaard, M. Loneliness and social support in adolescent boys with attention deficit hyperactivity disorder in a special education setting. J. Child Fam. Stud. 2017, 26, 2900–2907. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study | Country | Design | Sample Size (N, Female) | Age Range (Mean) | Demographics | Diagnosis | Outcomes Measured | Measurement Tools | Key Findings |
|---|---|---|---|---|---|---|---|---|---|
| Zach, Yazdi-Ugav, Zeev. (2016) [32] | Israel | Cross-sectional | 733 (374 females) | 6.04–13.72 years (8.82) | General education class in 2 Public schools, grade 1–5 in Israel. LD: +2 SD below average achievement in standardized tests and IQ 85–115 | LD, TD | 1. Social skills 2. Social dissatisfaction | 1. Elementary school Social Skills Rating System (SSRS)-T form - Hebrew Adaptation, completed by teacher and includes 3 domains: social skills, problem behaviours, and academic competence. Loneliness was measured with a modified version of the Loneliness and Social Dissatisfaction questionnaire by Asher. | - Learning disorders and loneliness did not contribute to the explanation of the females’ social skills variance. In boys, loneliness can explain their social skills variance. |
| ValÅs (1999) [33] | Norway | Cross-sectional | 1434 (728 females) | 10–16 years (not reported) | 552 4th grade, 511 7th grade, 371 9th grade from 128 classes across 49 schools in Norway in 1996. | LD, low-achieving | 1. Peer acceptance 2. Self-esteem Depression | 1. Sociometric question referred to the hypothetical situation: “Imagine the school will form new classes and you can decide who goes into which classes. Which students in your grade would you like to have in your new class?” 2. A scale modified from the Self-Description Questionnaire SDQ II 3. Scale modelled after Kovacs’ 1985 instrument that assesses affective, cognitive, motivational, and somatic symptoms of depression. Loneliness was measured with the Loneliness and Social Dissatisfaction Questionnaire by Asher (modified version). | - Pearson correlations were significant between loneliness and the following: self-esteem (r = −0.251), depression (r = 0.312) in all participants. Students with LD compared with non-LD and non low-achieving students were less accepted among peers, were more lonely, and had lower self-esteem. |
| Lackaye & Margalit (2008) [34] | Israel | Cross-sectional | 280 (140 females) | 2 age groups: 7th grade and 10th grade | From 10 schools in Israel. LD students: IQ 85–120 | LD and non-LD | 1. Numerical grades for mathematics and history 2. Specific academic self-efficacy 3. General academic self-efficacy 4. Hope 5. Effort | 1. Grade reports 2. The Hebrew adaptation of the Specific Academic Self-Efficacy Scale 3. The Hebrew adaptation of the General Academic Self-Efficacy Scale 4. The Hebrew adaptation of The Children’s Hope Scale 5. Adaptation of the Meltzer scale for effort Loneliness was measured with the Hebrew adaptation of the Loneliness and Social Dissatisfaction Questionnaire from Asher | Loneliness is statistically significantly correlated with: academic self-efficacy (r = −0.35), history (r = 0.20), and hope (r = −0.42). |
| Idan & Margalit (2014) [35] | Israel | Cross-sectional | 856 (396 females) | 15–18 years (not reported) | Public High school students from seven high schools in Central Israel (5 located in predominantly middle class districts, 2 located in predominantly lower class districts) LD students: IQ 85–120, achievement scores at least one standard deviation | LD and non-LD | 1. Sense of coherence 2. Basic psychological needs (autonomy, competence, relatedness) 3. Family climate (cohesiveness, adaptability) 4. Hope 5. Effort 6. Academic self efficacy Students’ achievements | 1. Sense of coherence scale 2. Basic psychological needs scale 3. FACES III (family adaptability and cohesion evaluation scale) 4. Hebrew adaptation of the children’s hope scale 5. Effort scale 6. Hebrew adaptation of the academic self-efficacy scale 7. Students’ numerical grades Loneliness was measured with the Hebrew adaptation of the Loneliness Scale from Asher. | - In the LD group, there was a statistically significant negative correlation between loneliness and the following measures (spearman correlation in bracket): sense of coherence (−0.43), autonomy/competence (−0.42), relatedness (−0.64), family cohesion (−0.18). A positive correlation with self-efficacy English (0.25), Loneliness contributed negatively to hope (−0.42). |
| Al-Yagon (2016) [24] | Israel | 3 groups Cross-sectional assessment | 280 (154 females) | 15–17 years (15.94) | Grade 10/11 public high schools in urban Israel. Parents: mainly married full time workers with a university degree. | LD, LD + ADHD, TD | 1. Adolescents’ (ado) perceptions of security in parent-child relationship. 2. Ados’ perceptions of their homeroom teacher as an attachment figure. 3. Ados’ perception of their relationship with their very best friend. 4. Ados’ view of their own affects. 5. Emotional and behavioural problems among youth | 1. Attachment security style scale (answered by teen) 2. Children’s Appraisal of Teacher as a Secure Base Scale. 3. Friendship Quality Questionnaire. 4. Affect scale. 5. Externalizing/Internalizing Syndrome scales from the standardized Youth Self-Report Version for Age 11–18 Loneliness was measured with (i) the Peer-Network Loneliness and (ii) the Peer-Dyadic Loneliness Scale. | Ado with comorbid LD + ADHD: - significant correlation between peer network loneliness and: ado-mother attachment (r = −0.31), ado-father attachment (r = −0.27), teacher’s availability (r = −0.21), teacher’s rejection (r = 0.25), friendship quality (r = −0.47), positive affect (r = −0.47), negative affect (r = 0.39), internalizing behaviours (r = 0.57). - significant correlation between peer-dyadic loneliness and: adolescent mother attachment (r = −0.22), friendship quality (−0.55), positive affect (r = −0.30). Ado with LD only: - significant correlation between peer network loneliness and: ado-mother attachment (r = −0.38), ado-father attachment (r = −0.25), friendship quality (−0.41), positive affect (r = −0.4), negative affect (r = 0.35), externalizing behaviours (r = 0.28), internalizing behaviours (r = 0.45). - significant correlation between peer dyadic loneliness and: ado mother attachment (r = −0.25), friendship quality (r = −0.49), positive affect (r = −0.37), negative affect (r = 0.27), externalizing behaviour (r = 0.33), internalizing behaviour (r = 0.47) |
| Becker (2015) [36] | United States | Cross-sectional | 112 (39 females) | 7–12 years (8.79) | 76% non-Hispanic white, 17% African American, 5% Hispanic, 2% Asian, 1% Native American. 9% annual family income >$20,000, 34% $20,001–50,000, 21% $50,001–80,000, 36% <$80,000 | ADHD-I or ADHD-C | 1. Academic achievement 2. Intelligence 3. Social Information Processing attribution biases (internal and external attributions) 4. oppositional defiant/conduct disorder (ODD/CD) symptoms 5. Anxiety symptoms 6. Positive illusory bias 7. Aggression 8. Perceived social acceptance 9. Peer isolation | 1. Wechsler Individual Achievement Test 2. The Kaufman Brief Intelligence Test Second Edition 3. Externalizing-relevant vignettes (responses coded as negative internal, negative external, or neutral attributions) and internalizing-relevant vignettes (Children’s Evaluation of Everyday Social Encounters Questionnaire) 4. The Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children, Vanderbilt ADHD Diagnostic Rating Scale 5. The Revised Child Anxiety & Depression Scales 6. Self-Perception Profile for Children (SPPC) 7. Dodge and Coie’s (1987) measure of aggressive behaviors 8. The Child Behavior Scale Loneliness was measured with the Loneliness Questionnaire (Asher et al., 1984) [37]. | - Peer exclusion/withdrawal not significantly correlated with child depressive symptoms or anxiety symptoms. - ODD/CD symptoms were significantly associated with peer exclusion (r = 0.26, p = 0.005). - Negative internal attribution bias had a significant negative association with peer withdrawal - Anxiety was negatively associated with perceived social acceptance (β = −0.38, SE = 0.09, p < 0.001) and positively associated with loneliness (β = 0.62, SE = 0.06, p < 0.001). |
| Dovgan & Mazurek (2019) [38] | United States | Cross-sectional, survey | 129 (18 females) | 6–18 years (10.86) | 40.3% scored IQ less than 70 | ASD | 1. Adaptive Behaviour 2. Childhood emotional & behavioural problems 3. Internalizing & externalizing symptoms 4. Participation in sports, hobbies and clubs, total activities 5. Friendships 6. Intelligence (IQ) | 1. Vineland Adaptive Behaviour Scales 2. The Child Behavior Checklist. 3. Early Years Differential Ability Scales, School-Age Differential Ability Scales, Wechsler Abbreviated Scale of Intelligence or Mullen Scales of Early Learning Social participation/isolation was measured by the Child Behaviour Checklist. | - Internalizing problems were not significantly correlated with the number of friends (rs = 0.010, p = 0.914) or with the number of total activities (r = 0.037, p = 0.678). |
| White & Roberson-nay (2009) [39] | United States | Cross-sectional | 20 (2 females) | 7–14 years (12.08) | 95% attended public regular education schools. 14 received special education services, 8 received speech/language therapy, 5 received social skills training interventions. 65% on medication | Clinical diagnoses of ASD including autistic disorder, PDD-NOS, or AS | 1. Prosocial index and social initiative index 2. Anxiety 3. Social competence, emotional and behavioral problems | 1. Social Communication Questionnaire 2. Social Responsiveness Scale 3. Social Competence Inventory 4. Multidimensional Anxiety Scale for Children 5. Child Behavior Checklist Loneliness was measured with the Loneliness Questionnaire by Asher. | - The high-anxiety group self-reported more social loneliness than their less anxious peers (t = 2.57, p < 0.05). - Social and global loneliness scores were significantly correlated with social anxiety (r = 0.59, p = 0.01) and (r = 0.50, p = 0.04), respectively. |
| Whitehouse et al. (2009) [40] | Australia | Cross-sectional | 70 (13 females) | AS group: 12–17 years (14, 2 mos) TD group: 13–16 years (14, 4 mos) | Attending mainstream secondary schools in one of three states in Australia: Western Australia, New South Wales, and Queensland. | Asperger’s syndrome, TD | 1. Friendship Depressive symptom | 1. Friendship Quality Questionnaire and Friendship Motivation Questionnaire 2. Centre for Epidemiological Studies Depression Scale Children’s Version Loneliness was measured with the De Jong-Gierveld Loneliness Scale. | - Loneliness significantly mediated the association between the conflict/betrayal subscale (p < 0.01) and levels of depressive symptoms in the AS group (p < 0.001), which was the only significant predictor of depression. |
| Lounds Taylor, Adams, Bishop (2017) [41] | United States | Longitudinal | 36 (6 females) | 17–22 years (18.71) | 88.9% white non-Hispanic IQ range 40–147 standard score Avg 85.33 (SD25.65) Schooling: 63.9% regular public/magnet school, 8.3% regular private school, 11.1% school that only serves students with disabilities, 13.9% home schooled, 2.8% other All youth living with parents Parents: 32 mothers and 4 fathers, age 38–59. 69.4% married, 69.4% post- secondary degree, 30.6% post-bachelor’s degree Avg annual income $85,000, 25% <$50,000 | ASD | Internalizing symptoms | 1. Adult behaviour checklist Social Participation was measured by the National Survey of Families and Households, modified to be appropriate for adolescents and adults | - The correlation between earlier unstructured social participation and later internalizing symptoms was −0.26. |
| Hedley et al. (2018) [42] | Australia | Cross-sectional, survey | 185 (92 females) | 14–80 years (37.11) | Employment: 49.7% employed (part-time/full-time). Education: 7.2% Current secondary, 3.8% Some secondary, 9.2% completed secondary, 21.1% certificate or diploma, 27.6% Bachelor’s degree, 18.9% Post graduate degree, 11.9% other/not reported. Living Conditions: 31.9% w/parents, 2.2% relatives, 6.5% Others, 20.5% alone, 34.1% couples, 4.9% other | ASD | 1. Social support 2. Major and subthreshold depressive disorder and suicidal ideation | 1. Social Support Questionnaire-Shortened Version (SSQ-6) 2. Patient Health Questionnaire (PHQ) Loneliness was measured with the University of California Los Angeles Loneliness Scale-Short Form | - Loneliness was negatively correlated with social support satisfaction/number (𝛽 = –0.47, p < 0.001), but positively correlated with depression (𝛽 = 0.24, p = 0.002) and suicidal ideation (b = 0.04; BCa [0.02, 0.06]). Depression predicted suicidal ideation(𝛽 = 0.51, p < 0.001). |
| Tillinger (2013) [43] | United States | Longitudinal data, correlational design | 93 (49 females) | Recruited at less than 24 months old, then home visits were conducted when children were age 1, 2, 3, 5, 10, 18, and 23 years. | 90% Euro-American descent from Massachusetts and New Hampshire. Family avg annual $40,000–45,000. Mothers’ education = avg 13.97 yrs. Child IQ 62.4% lower than one standard deviation below standardized mean, 53.8% lower than two standard deviations below standardized mean. | Down syndrome, motor impairment, or developmental delay of unknown etiology | 1. Child cognitive functioning 2. Autonomy 3. Self-efficacy 4. Behaviour problems 5. Nature of friend relationships at age 18 6. Friendship quality 7. Family satisfaction 8. Adolescent global self-worth 9. Adolescent depressive symptoms | 1. Stanford-Binet Intelligence Scales 2. Arc’s Self Determination Scale–Autonomy Subscale 3. Perceived Self-Efficacy Scale 4. Child Behavior Checklist 5. Multidimensional Scale of Perceived Social Support–Friends Subscale 6. Pictorial Scale of Perceived Competence and Social Acceptance for Young Children 7. Maternal Acceptance Subscale 8. Self-Perception Profile for Learning Disabled Students-Global Self-worth Subscale 9. Center for Epidemiologic Studies Depression Scale Loneliness was measured with the Loneliness and Social Dissatisfaction Questionnaire (Williams & Asher, 1992). | - Age 10 loneliness did not significantly predict friendship quality at age 18. - Age 10 loneliness was found to significantly predict adolescent global self-worth at age 18 (p = 0.008); higher levels of loneliness at age 10 led to lower levels of adolescent global self-worth at age 18. - Age 10 loneliness was found to significantly predict adolescent depressive symptoms at age 18 (p = 0.013); higher levels of loneliness at age 10 led to higher levels of adolescent depressive symptoms at age 18. |
| Criteria | Al-Yagon [24] | Becker [36] | Dovgan & Mazurek [38] | Hedley et al. [42] | Idan & Margalit [35] | Lackaye & Margalit [34] | Lounds Taylor, Adams, Bishop [41] | Tillinger [43] | Valas [33] | White & Robertson-nay [39] | Whitehouse et al. [40] | Zach, Yazdi-Ugav, Zeey [32] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Explicit theoretical framework | 3 | 3 | 3 | 3 | 3 | 2 | 2 | 3 | 3 | 3 | 2 | 2 |
| Statement of aims/objectives in the main body of the report | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 2 |
| Clear description of research setting | 3 | 3 | 3 | 2 | 3 | 3 | 2 | 3 | 3 | 2 | 3 | 3 |
| Evidence of sample size considered in terms of analysis | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 3 | 0 | 0 | 0 | 0 |
| Representative sample of target group of a reasonable size | 2 | 2 | 1 | 3 | 3 | 2 | 1 | 2 | 3 | 1 | 1 | 2 |
| Description of procedure for data collection | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 2 | 2 | 1 |
| Rationale for choice of data collection tool(s) | 2 | 2 | 2 | 3 | 3 | 2 | 2 | 3 | 3 | 2 | 1 | 1 |
| Detailed recruitment data | 3 | 3 | 1 | 3 | 1 | 2 | 2 | 1 | 2 | 2 | 2 | 1 |
| Statistical assessment of reliability and validity of measurement tool(s) (Quantitative only) | 1 | 2 | 1 | 3 | 2 | 2 | 1 | 2 | 2 | 1 | 2 | 2 |
| Fit between stated research question and method of data collection (Quantitative) | 2 | 2 | 2 | 3 | 2 | 1 | 1 | 2 | 2 | 2 | 2 | 1 |
| Fit between stated research question and format and content of data collection tool e.g., interview schedule (Qualitative) | n/a | 2 | 2 | 3 | 3 | 1 | 1 | 1 | 2 | 2 | 2 | 1 |
| Fit between research question and method of analysis | 3 | 3 | 2 | 3 | 2 | 1 | 2 | 3 | 2 | 1 | 1 | 1 |
| Good justification for analytical method selected | 3 | 2 | 2 | 3 | 3 | 2 | 1 | 2 | 2 | 2 | 1 | 1 |
| Assessment of reliability of analytical process (Qualitative only) | n/a | 3 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Evidence of user involvement in design | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Strengths and limitations critically discussed | 3 | 2 | 3 | 3 | 1 | 2 | 2 | 2 | 1 | 1 | 1 | 1 |
| Total score | 31 | 36 | 28 | 38 | 33 | 26 | 24 | 33 | 31 | 24 | 23 | 19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwan, C.; Gitimoghaddam, M.; Collet, J.-P. Effects of Social Isolation and Loneliness in Children with Neurodevelopmental Disabilities: A Scoping Review. Brain Sci. 2020, 10, 786. https://doi.org/10.3390/brainsci10110786
Kwan C, Gitimoghaddam M, Collet J-P. Effects of Social Isolation and Loneliness in Children with Neurodevelopmental Disabilities: A Scoping Review. Brain Sciences. 2020; 10(11):786. https://doi.org/10.3390/brainsci10110786
Chicago/Turabian StyleKwan, Celia, Mojgan Gitimoghaddam, and Jean-Paul Collet. 2020. "Effects of Social Isolation and Loneliness in Children with Neurodevelopmental Disabilities: A Scoping Review" Brain Sciences 10, no. 11: 786. https://doi.org/10.3390/brainsci10110786